
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To compare the incidence of complications in patients undergoing single-level and 2-level lumbar laminectomy in either the inpatient or outpatient settings.
Methods:
Patients who underwent single-level and 2-level lumbar laminectomy were identified in the ACS NSQIP database from the years 2006 to 2015. Independent patient variables were recorded, including demographics and preoperative health characteristics. Logistic regression was used to determine the risk of postoperative complications for both a 1- and 2-level lumbar laminectomy as well as to identify independent risk factors for a complication. Comparisons were made between 2 groups: (1) inpatient and (2) outpatient as determined by billing data.
Results:
A total of 18 076 single- and 2-level lumbar laminectomy cases were identified with 10 743 (59.4%) inpatient procedures and 7333 (40.6%) outpatient procedures. The incidence of any postoperative complication was significantly lower in the outpatient group than in the inpatient group among all cohorts including 1-level lumbar laminectomy (1.9% vs 6.7%), 2-level lumbar laminectomy (3.17% vs 7.38%), as well as in the combined cohort of 1- and 2-level laminectomies (2.47% vs 7.01%). Significant independent risk factors for complications after lumbar laminectomy were identified, including body mass index (BMI) >30 kg/m2, age ≥55 years, a functional status of partially dependent, chronic obstructive pulmonary disease (COPD), chronic steroid use, American Society of Anesthesiologists (ASA) class 3 or 4, and operative time >90 minutes.
Conclusions:
This study reports a lower overall complication rate in the 30-day postoperative period following 1- and 2-level lumbar laminectomy performed in an outpatient versus inpatient setting. Significant risk factors for complications included BMI >30 kg/m2, age ≥55 years, a functional status of partially dependent, COPD, chronic steroid use, ASA class 3 or 4, and operative time >90 minutes.
Keywords
Introduction
Lumbar laminectomy is one of the most commonly performed spinal surgical procedures for the treatment of a wide variety of pathologies. Complication rates and hospital lengths of stays have decreased over time and, in many cases, this procedure is now being performed in the outpatient setting. 1 -4 There are benefits of an inpatient stay after spine surgery, including close monitoring by a physician for any acute postoperative complications such as neurological deficits or surgical wound dehiscence, which may necessitate emergent intervention. On the other hand, outpatient spine surgery has been associated with lower complication rates and lower health care costs. 5 -7 Recently, a number of studies have been published supporting the performance of certain spinal procedures in the outpatient compared with the inpatient setting. 8 -11
To the best of our knowledge, no large studies have examined the difference in complications rates between lumbar laminectomies performed in the inpatient and outpatient settings. The purpose of this study was to compare the incidence of complications in patients undergoing single- and 2-level lumbar laminectomy in either the inpatient or outpatient settings. We queried the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database to identify all single- and 2-level lumbar laminectomy cases performed between 2006 and 2015. We hypothesized that there would be a significantly lower 30-day complication rate when the procedure was performed in an outpatient setting as compared to those performed in an inpatient setting.
Materials and Methods
The ACS NSQIP database provides surgical outcomes data from over 400 participating hospitals throughout the United States. 9 Perioperative data, including patient demographics, preoperative comorbidities, and operative variables are collected prospectively by trained, on-site, surgical clinical reviewers and postoperative 30-day outcomes across 21 categories of morbidity and mortality are recorded. 9 Data collection continues for 30 days regardless of date of discharge or inpatient status. Data quality is ensured with routine auditing with an overall interrater disagreement rate reported to be approximately 2%. 12
Patients who underwent single- and 2-level lumbar laminectomy were identified in the ACS NSQIP database from the years 2006 to 2015 using the Current Procedural Terminology (CPT) codes 63 047 and 63 048 as the primary procedural code. Patients who underwent 2-level lumbar laminectomy were identified by using the CPT codes 63 047 and 63 048 as secondary procedural codes. Patients were excluded if they had more than 2 laminectomy codes (63 047 or 63 048) or any other CPT codes that were not directly associated with the primary laminectomy codes. Cases with any evidence of fusion were excluded from the study. Independent patient variables were recorded including demographics and preoperative health characteristics. Patient demographics included age and sex. Preoperative health characteristics included body mass index (BMI), World Health Organization (WHO) obesity classification, American Society of Anesthesiologists (ASA) class, functional status (independence), smoking status, and comorbidities. BMI was calculated for each patient using their recorded height and weight and this was then used to stratify patients based on the WHO classification for obesity. 13 Comorbidities included were diabetes, dyspnea, chronic obstructive pulmonary disease (COPD), ascites, congestive heart failure (CHF), hypertension, renal failure, use of steroids, and cancer. Inpatient vs. outpatient status was determined based on hospital billing defined in the NSQIP database.
Postoperative endpoints included death, pulmonary complications (pneumonia, intubation, or ventilator requirement), deep vein thrombosis (DVT) or pulmonary embolism (PE), wound complications (superficial wound infection, deep surgical site infection, organ space surgical site infection, or dehiscence), sepsis, or septic shock, cardiac complication (cardiac arrest or myocardial infarction), return to the operating room within 30 days, blood transfusions (intra- or postoperative), or urinary tract infection (UTI). Major complications were defined as any septic, cardiac, or pulmonary complications as well as DVT, PE, return to the operating room, and death. Minor complications were defined as any wound complications, UTI, or blood transfusions.
Differences in demographics and comorbidities between the inpatient and outpatient groups were analyzed using an independent t test for continuous variables or Pearson’s chi-square test for categorical variables. Given that the decision to perform a laminectomy in either an in- or outpatient setting may be partially dependent on the presence of covariates, propensity scores were calculated. Univariate logistic regression was used to identify predictors of treatment (in- vs outpatient). Age, BMI, diabetes, smoking, dyspnea, functional status, CHF, steroid use, disseminated cancer, ASA class, and level of laminectomy (1 vs 2) were all found to be associated with treatment and were therefore used to generate propensity scores. To assess the quality of the matching, the comparison of demographics and comorbidities between the inpatient and outpatient groups was repeated. Following propensity score matching, univariate logistic regression models were constructed to identify potential predictors of morbidity. Logistic regression was then carried out on the entire cohort (unadjusted) and matched sample (adjusted) to determine the risk of postoperative complications for the entire group and for with patients grouped according to the level lumbar laminectomy (1 vs 2). Variables that were predictive at P < .10 were considered in the multivariate model. In addition, variables with a known association with morbidity, for example, smoking, were also considered in the multivariate model. A multivariate logistic regression model was created using the matched sample to identify independent risk factors for a complication. Results are reported as odds ratio with corresponding 95% confidence intervals. A P value of <.05 was considered statistically significant. All statistical analysis was performed using Stata 15 (StataCorp, 2017, Stata Statistical Software: Release 15, College Station, TX).
Results
A total of 18 076 single- and 2-level lumbar laminectomy cases were identified with 10 743 (59.4%) inpatient procedures and 7333 (40.6%) outpatient procedures. The proportion of outpatient surgery increased exponentially over time from 2006 to 2015 whereas the proportion of inpatient surgery increased linearly to the point where the proportion of outpatient surgery exceeded that of inpatient surgery in 2015 (Figure 1). Patients who underwent outpatient surgery were younger and had lower obesity classifications (all unadjusted P < .001). In addition, patients who underwent outpatient surgery had lower rates of diabetes, dyspnea, CHF, hypertension, steroid use, and cancer when compared with patients undergoing inpatient surgery. They also had higher rates of smoking and functional independence as compared with patients undergoing inpatient surgery. More ASA class 1 and 2 patients underwent outpatient surgery whereas more ASA class 3 and 4 patients underwent inpatient surgery. Propensity score matching eliminated statistically significant differences between the groups with respect to age, BMI, smoking, dyspnea, functional status, CHF, steroid use, and disseminated cancer. Differences between the groups in the proportion of patients with diabetes, renal failure, ASA class, and level of laminectomy were reduced with the propensity matching however the adjusted p values remained statistically significant. To account for these differences, these variables were considered in the multivariate model (Table 1).
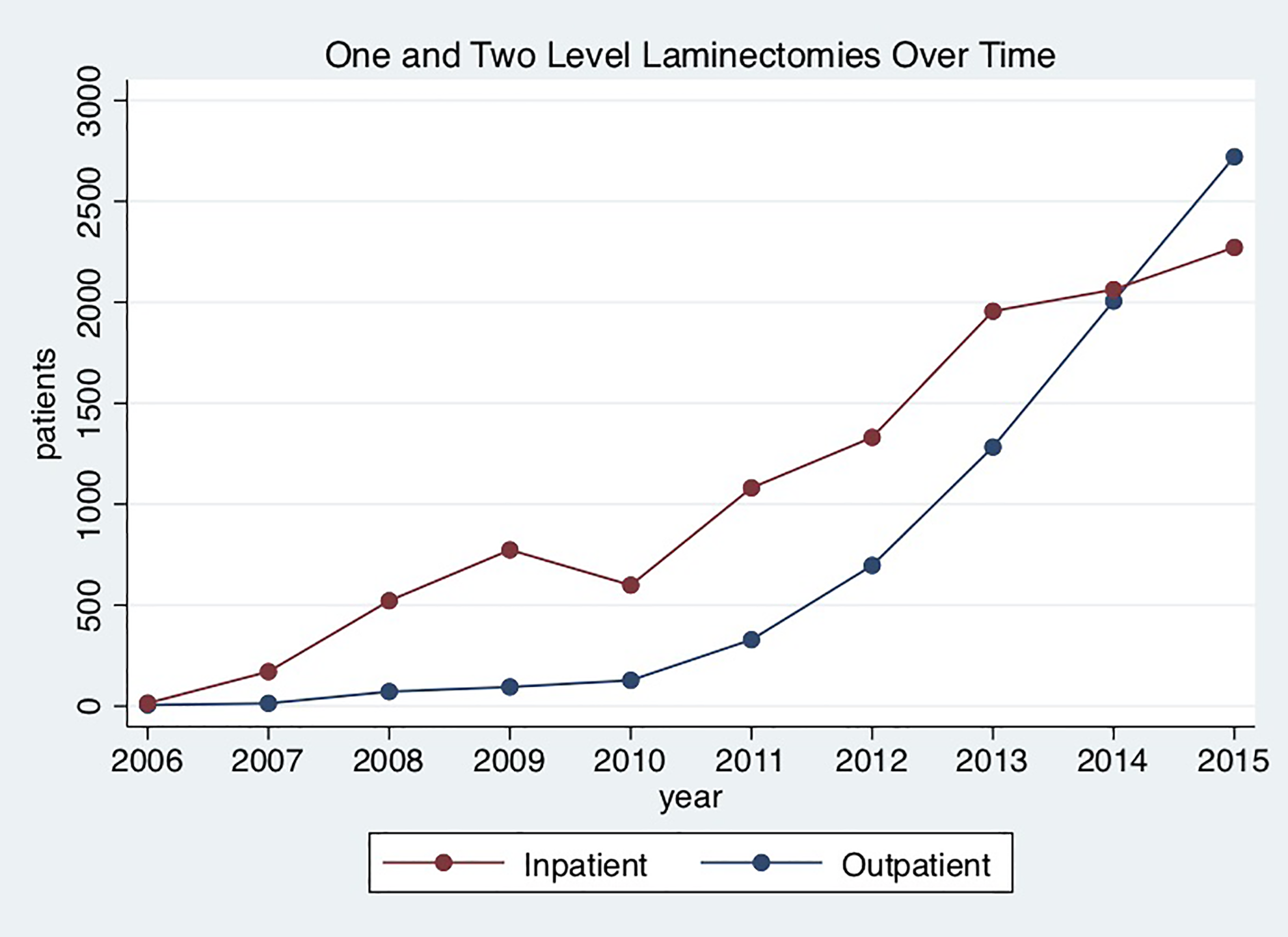
Single- and 2-level lumbar laminectomies performed in the inpatient and outpatient settings over the study time frame from 2006 to 2015. The number of inpatient procedures exceeded that of outpatient procedures throughout this time period until the year 2015 when more single- and 2-level lumbar laminectomies were performed in the outpatient setting than in the inpatient setting.
Patient Demographics and Comorbidities With Propensity-Adjusted P Values.
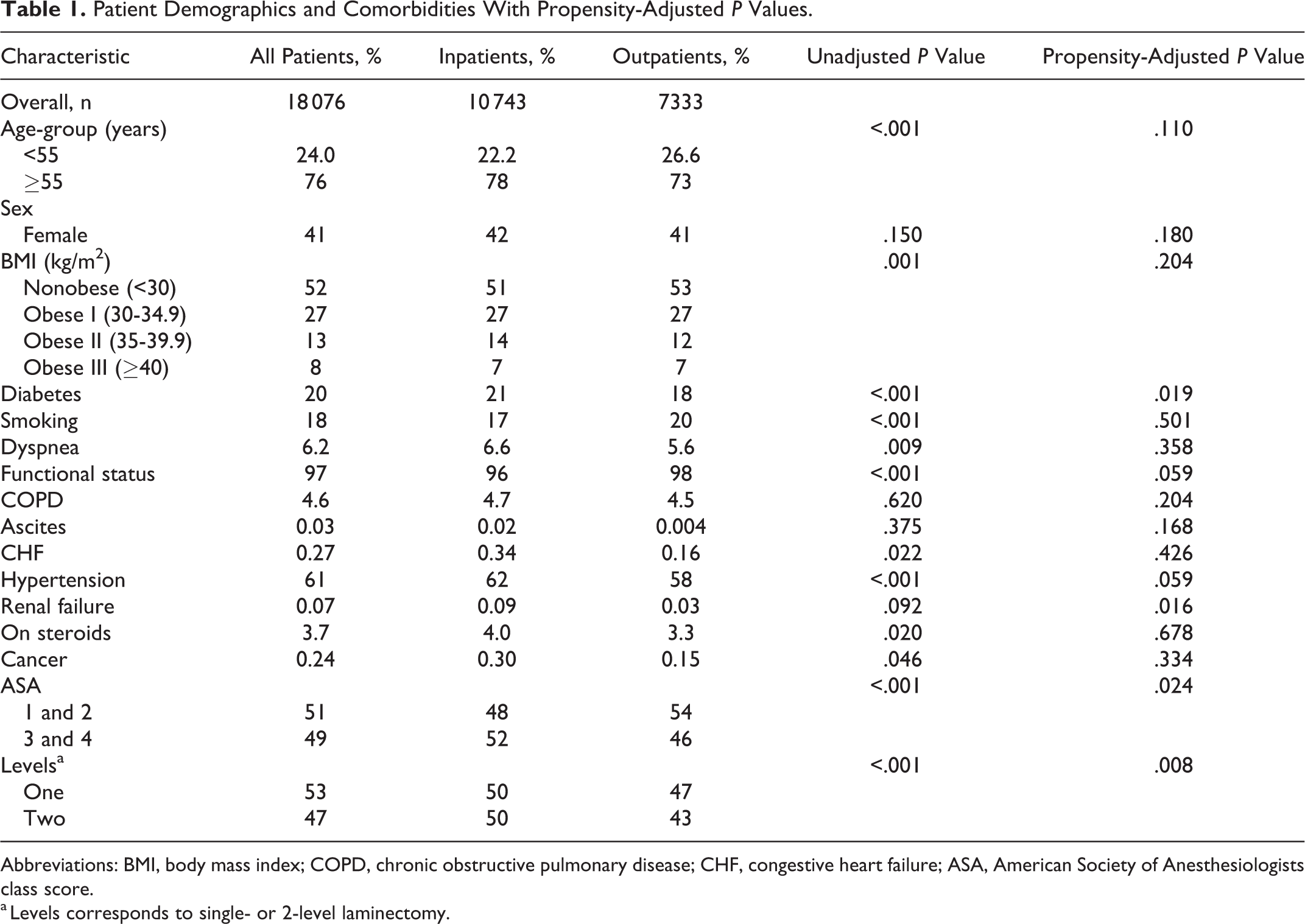
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; ASA, American Society of Anesthesiologists class score.
a Levels corresponds to single- or 2-level laminectomy.
Among single-level lumbar laminectomy cases, the incidence of any postoperative complication was significantly lower in the outpatient group than in the inpatient group (1.9% vs 6.7%) with a propensity-adjusted odds ratio (OR) of 0.28, 95% confidence interval (CI) 0.22 to 0.36, P < .001. Other postoperative endpoints that were found to be significantly less likely in the outpatient cohort included any major complication (0.90% vs 3.75%, OR 0.24, 95% CI 0.17-0.35, P < .001), any pulmonary complication (0.15% vs 0.93%, OR 0.16, 95% CI 0.07-0.37, P < .001), thromboembolic event including DVT or PE (0.27% vs 0.71%, OR 0.37, 95% CI 0.19-0.75, P = .006), sepsis or septic shock (0.19% vs 0.88%, OR 0.22, 95% CI 0.10-0.49, P < .001), any cardiac complication (0.05% vs 0.40%, OR 0.11, 95% CI 0.03-0.47, P = .003), return to the operating room (0.24% vs 1.72%, OR 0.15, 95% CI 0.08-0.30, P < .001), blood transfusion (0.12% vs 1.91%, OR 0.06, 95% CI 0.02-0.15, P < .001), and UTI (0.29% vs 1.52%, OR 0.17, 95% CI 0.09-0.31, P < .001) (Table 2).
Unadjusted and Propensity Adjusted, Unmatched and Matched, Complication Rates Between Inpatient and Outpatient Single-level Lumbar Laminectomy Groups.
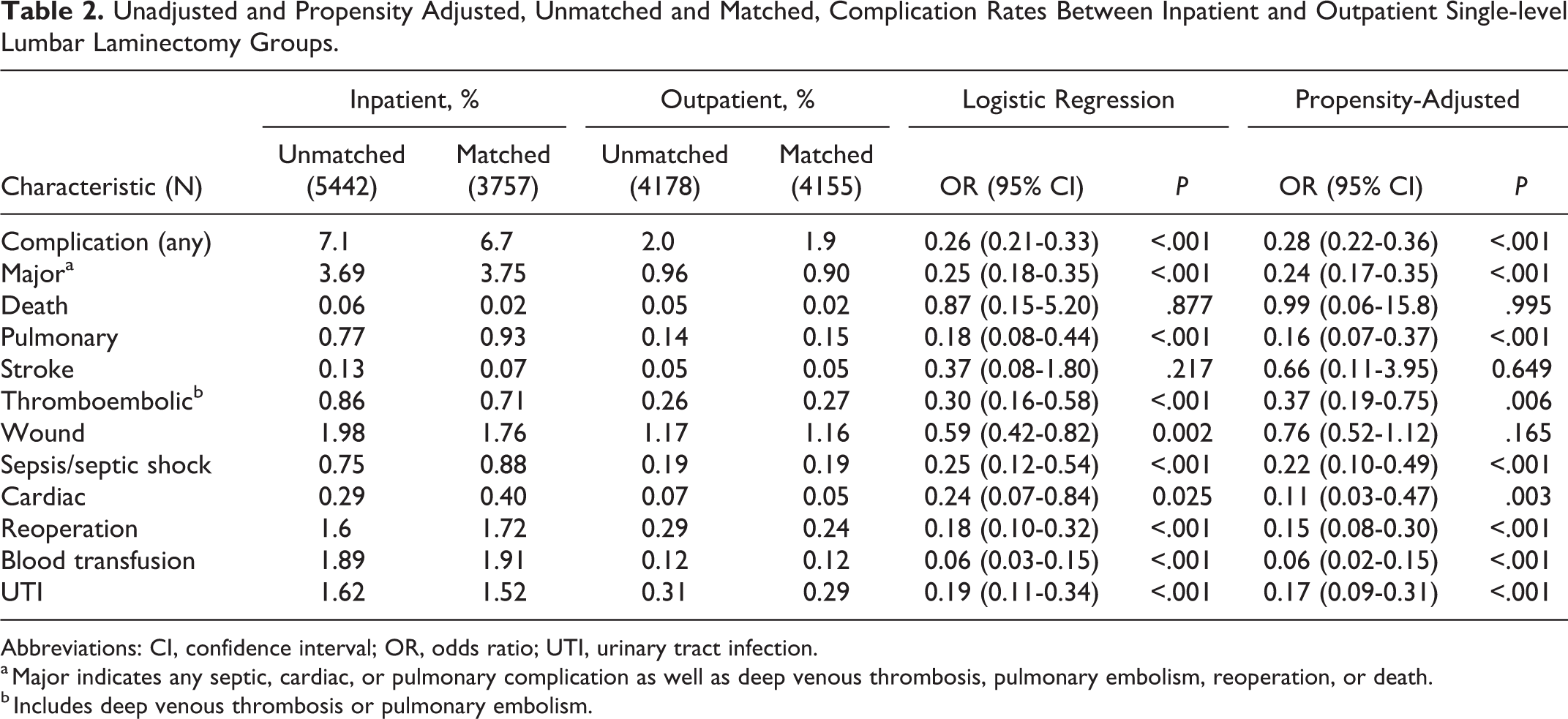
Abbreviations: CI, confidence interval; OR, odds ratio; UTI, urinary tract infection.
a Major indicates any septic, cardiac, or pulmonary complication as well as deep venous thrombosis, pulmonary embolism, reoperation, or death.
b Includes deep venous thrombosis or pulmonary embolism.
Among 2-level lumbar laminectomy cases, the incidence of any postoperative complication was once again, significantly lower in the outpatient group compared with the inpatient group (3.17% vs 7.38%, OR 0.42, 95% CI 0.33-0.54, P < .001). Other postoperative endpoints that were found to be significantly less likely in the outpatient cohort included any major complication (1.59% vs 3.22%, OR 0.52, 95% CI 0.37-0.73, P < .001), wound complications (1.62% vs 2.27%, OR 0.66, 95% CI 0.46-0.94, P = .021), sepsis or septic shock (0.29% vs 0.85%, OR 0.36, 95% CI 0.17-0.78, P = .009), return to the operating room (0.44% vs 1.04%, OR 0.43, 95% CI 0.23-0.80, P = .008), blood transfusion (0.16% vs 2.32%, OR 0.07, 95% CI 0.03-0.18, P < .001), and UTI (0.67% vs 1.42%, OR 0.56, 95% CI 0.33-0.95, P = 0.032). Other study outcomes trended toward lower incidences of complications in the outpatient cohort but did not reach statistical significance (Table 3).
Unadjusted and Propensity Adjusted, Unmatched and Matched, Complication Rates Between Inpatient and Outpatient 2-Level Lumbar Laminectomy Groups.
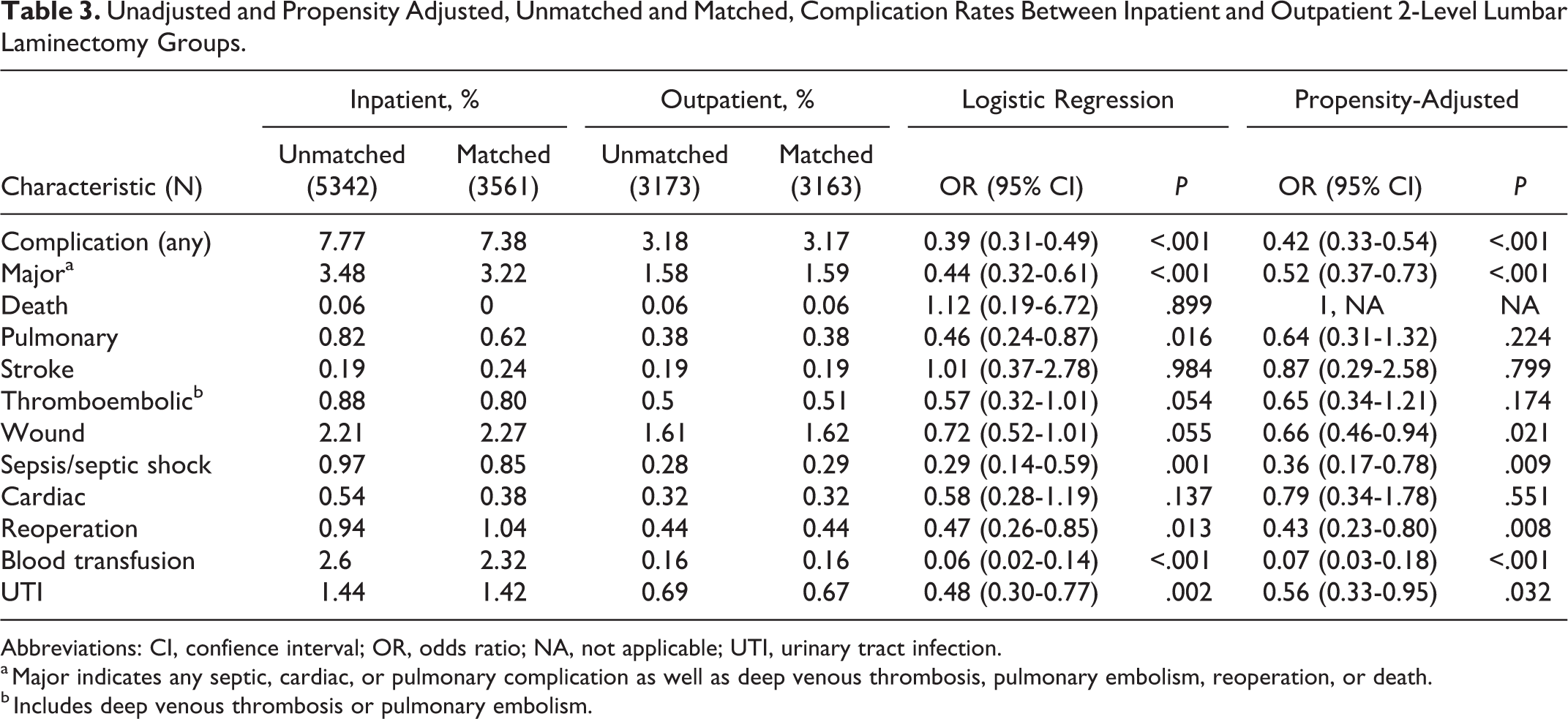
Abbreviations: CI, confience interval; OR, odds ratio; NA, not applicable; UTI, urinary tract infection.
a Major indicates any septic, cardiac, or pulmonary complication as well as deep venous thrombosis, pulmonary embolism, reoperation, or death.
b Includes deep venous thrombosis or pulmonary embolism.
When both 1- and 2-level laminectomy cohorts were combined, the incidence of any postoperative complication remained significantly lower in the outpatient group compared with the inpatient group (2.47% vs 7.01%, OR 0.34, 95% CI 0.29-0.41, P < .001). Other postoperative endpoints that were found to be significantly less likely in the outpatient cohort included any major complication (1.19% vs 3.51%, OR 0.38, 95% CI 0.30-0.49, P < .001), pulmonary (0.25% vs 0.82%, OR 0.30, 95% CI 0.17-0.52, P < .001), thromboembolic event including DVT or PE (0.37% vs 0.67%, OR 0.50, 95% CI 0.31-0.79, P = .003), wound complications (1.36% vs 1.99%, OR 0.70, 95% CI 0.54-0.91, P = .008), sepsis or septic shock (0.23% vs 0.87%, OR 0.28, 95% CI 0.16-0.48, P < .001), cardiac (0.16% vs 0.39%, OR 0.38, 95% CI 0.20-0.75, P = .005), return to the operating room (0.33% vs 1.41%, OR 0.24, 95% CI 0.16-0.38, P < .001), blood transfusion (0.14% vs 2.10%, OR of 0.07, 95% CI 0.03-0.12, P < .001), and UTI (0.45% vs 1.47%, OR 0.31, 95% CI 0.21-0.45, P < .001). Other study outcomes trended toward lower incidences of complications in the outpatient cohort but did not reach statistical significance (Table 4).
Unadjusted and Propensity Adjusted, Unmatched and Matched, Complication Rates Between Inpatient and Outpatient Combined (Single- and 2-level) Lumbar Laminectomy Groups.
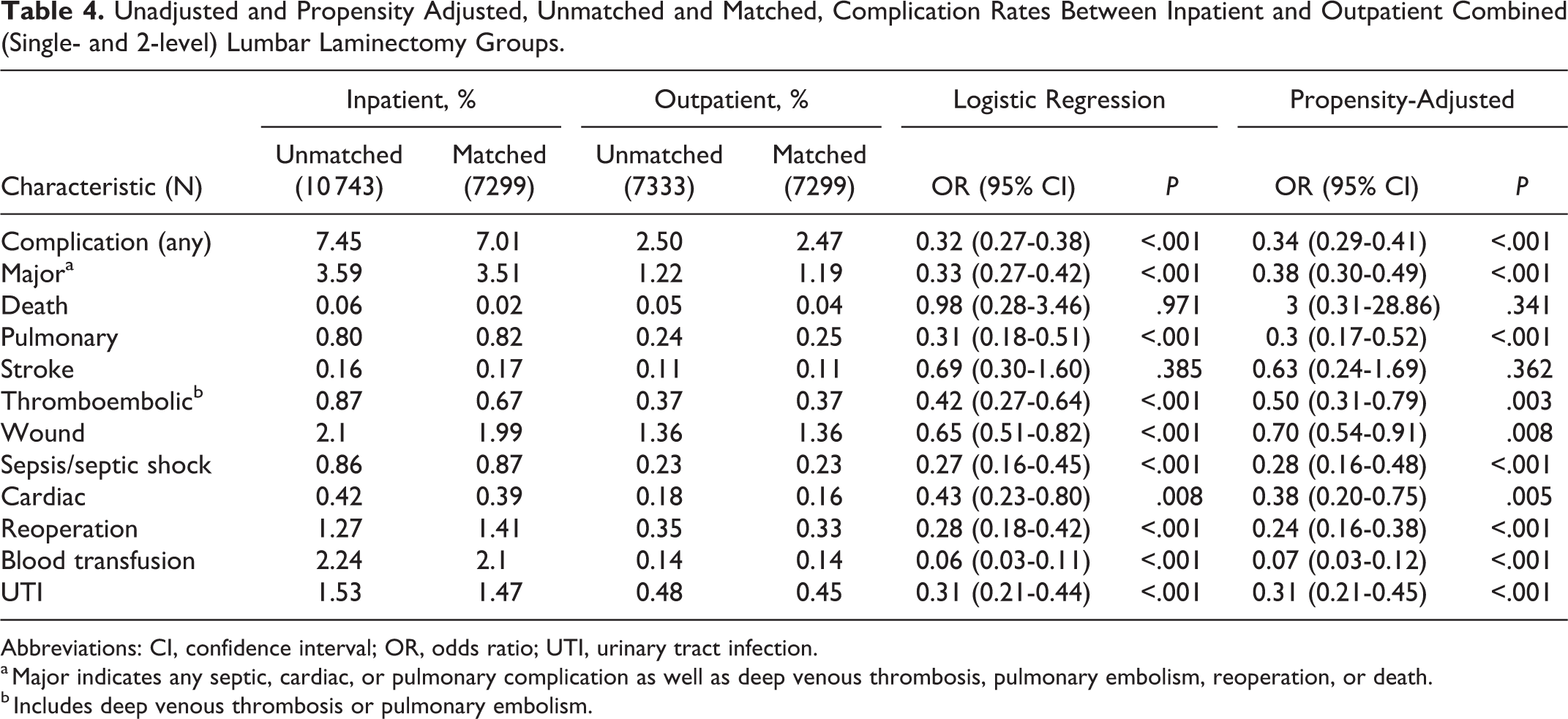
Abbreviations: CI, confidence interval; OR, odds ratio; UTI, urinary tract infection.
a Major indicates any septic, cardiac, or pulmonary complication as well as deep venous thrombosis, pulmonary embolism, reoperation, or death.
b Includes deep venous thrombosis or pulmonary embolism.
Significant independent risk factors for complications after lumbar laminectomy were identified using multivariate logistic regression. Demographic variables that were found to be risk factors included BMI >30 kg/m2 (OR 1.23, 95% CI 1.02-1.49, P = .027), age ≥55 years (OR 1.28, 95% CI 1.01-1.61, P = .041), and a functional status of partially dependent (OR 2.36, 95% CI 1.34-4.18, P = .003). Comorbidities that were found to be independent risk factors included COPD (OR 1.59, 95% CI 1.10-2.29, P = .013), chronic steroid use (OR 3.38, 95% CI 2.39-4.79, P < .001), and ASA class 3 or 4 (OR 1.74, 95% CI 1.43-2.12, P < .001). Operative time >90 minutes was found to be an independent risk factor for complications as well (OR 1.86, 95% CI 1.50-2.30, P < .001). A factor that was found to be protective was performance of the procedure in the outpatient setting (OR 0.40, 95% CI 0.32-0.50, P < .001) (Table 5).
Independent Risk Factors for Any 30-day Complication After Lumbar Laminectomy as Defined by Multivariable Logistic Regression.
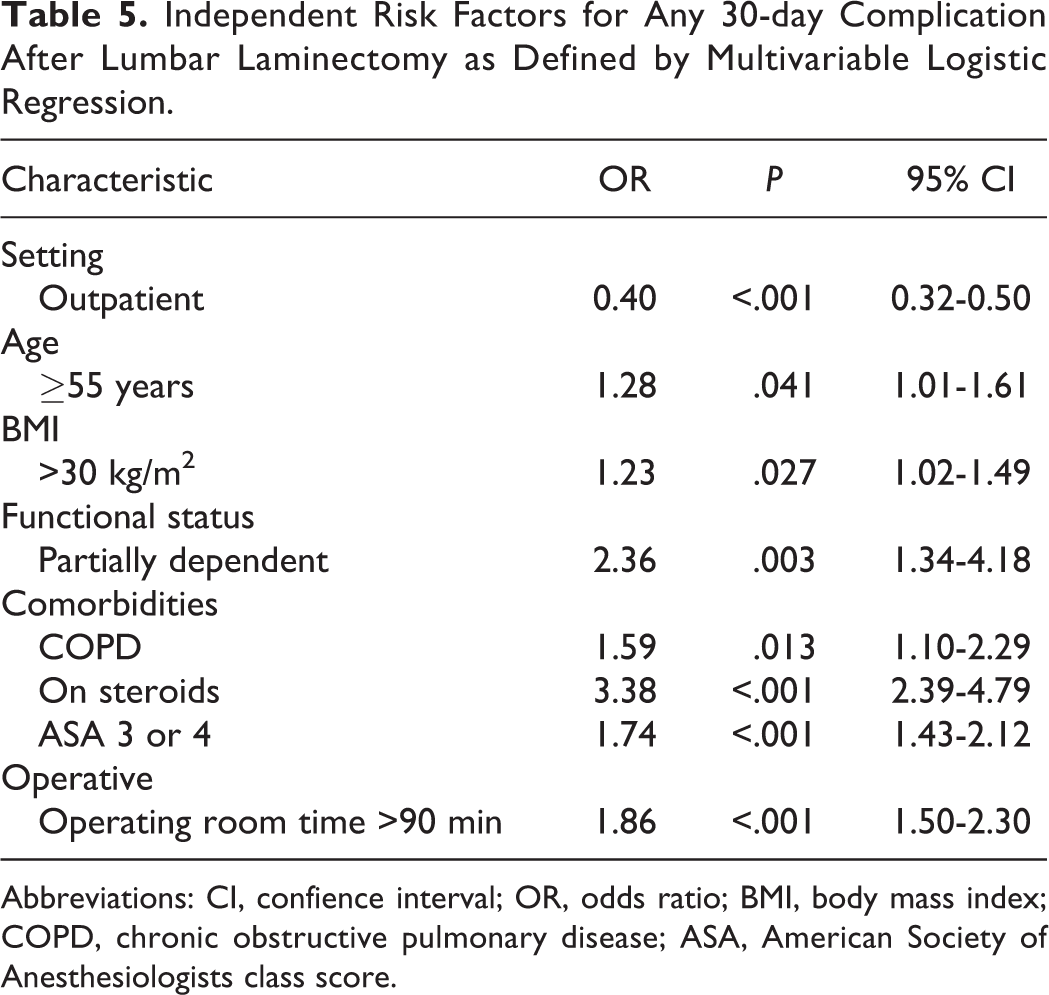
Abbreviations: CI, confience interval; OR, odds ratio; BMI, body mass index; COPD, chronic obstructive pulmonary disease; ASA, American Society of Anesthesiologists class score.
Discussion
An expanding body of literature exists demonstrating the increasing prevalence and safety of outpatient spine surgery. 1 -11 Despite the growing interest in performing spine procedures in the outpatient setting, concerns remain regarding the safety of this approach. 14,15 In this study, we have shown that outpatient single- and 2-level lumbar laminectomies are associated with lower overall perioperative complication rates when compared with the procedure performed in the inpatient setting.
By analyzing a large prospective multicenter database, we identified a cohort of 18 076 patients who underwent single- and 2-level lumbar laminectomies from the years 2006 to 2015. When matched, we found that amongst the single-level laminectomy cases, the overall risk of developing any 30-day postoperative complication was 6.7% in the inpatient group versus only 1.9% in the outpatient group. Among the 2-level laminectomy cases, the overall risk of developing any 30-day postoperative complication was 7.38% versus only 3.17% in the outpatient group. When the 2 cohorts were combined, these results persisted with an overall risk of developing any 30-day postoperative complication of 7.01% in the inpatient group versus only 2.47% in the outpatient group. It is true that in this study, outpatients were younger, less obese, and had fewer comorbidities. While the difference in complication rates between the inpatient and outpatient cohorts could be attributed to the differences in the baseline comorbidity burden, age, and, obesity profile between the 2 cohorts, the significant difference in complication rates persisted after propensity score adjustment suggesting that this may only be partially responsible for these findings. Interestingly, the proportion of outpatient surgery increased exponentially over the years 2006 to 2015 with the proportion of outpatient surgery finally exceeding that of inpatient surgery beginning in 2015. This was noted despite the fact that the overall health of the population as indicated by ASA and comorbidities remained relatively unchanged. These results suggest that not only does lumbar laminectomy performed in the outpatient setting have no association with increased morbidity relative to the inpatient setting, but that it may potentially be safer to perform this procedure on an outpatient basis. Our findings appear to be consistent with other recent studies in the literature comparing spine surgery performed in the inpatient and outpatient settings.
Pugely et al 8 compared the incidence of complications in patients undergoing single-level lumbar discectomy between the inpatient and outpatient settings. Using the NSQIP database, they analyzed 4310 patients and found that the overall complication rates were higher in the inpatient cohort than in the outpatient cohort (5.4% vs 3.5%). 8 They hypothesized that outpatients may be more likely to mobilize postoperatively, have decreased rates of urinary catheterization, and less exposure to pathogens seen in the hospital setting. 8
Fu et al 9 compared the complication rates between inpatient and outpatient 1- and 2-level anterior cervical discectomy and fusion (ACDF) cases in NSQIP from 2011 to 2014. Among the 2-level cases, they found that the overall complication rates were higher in the inpatient cohort than in the outpatient cohort (3.94% vs 1.47%). 9 They also reported a similar finding in the single-level cases (4.05% vs 1.01% overall complication rate in inpatient vs outpatient setting). 9 They noted that while the comorbidity burden between the cohorts was likely to be at least partially responsible for these findings, the difference in complication rates persisted after propensity score adjustment suggesting that outpatient surgery provides a protective effect against hospital-associated complications. 9
In this study, we also identified independent risk factors of any complication after lumbar laminectomy. These risk factors included BMI > 30 kg/m2, age ≥55 years, COPD, steroid use, ASA class 3 or 4, and an operative time >90 minutes. Surgery in the outpatient setting was found to be protective against complications (OR 0.40, 95% CI 0.32-0.50, P < .001). These results could help to determine appropriate candidates for surgery in the outpatient setting. These findings were in line with other studies in the literature as well.
Baswues et al 16 looked at patients who underwent lumbar laminectomy in the NSQIP database between 2011 and 2012 to identify factors associated with increased postoperative length of stay (LOS) and readmission. They found that increased age, BMI, ASA class 3 or 4, and a preoperative hematocrit of less than 36 were all independent risk factors of increased LOS. 16 Increased age, BMI, ASA class 3 or 4, and steroid use were risk factors for readmission. 16 Fu et al 9 identified Charlson Comorbidity Index 4 or greater, ASA class 3 or greater, chronic steroid use, hypertension, male sex, and BMI >30 kg/m2 as independent risk factors for any postdischarge complication after ACDF in their NSQIP study. Pugely et al 8 found that age >70 years, diabetes, previous wound infection, transfusion, and operative time >150 minutes were all independent risk factors of any complication after lumbar discectomy.
Although the NSQIP database does not include cost data, the cost of inpatient versus outpatient spine surgery has been reported in the literature. Silvers et al 17 reported an estimated annual cost savings of over $100 million dollars with the performance of ACDF in the outpatient setting in 1996. With increasing performance of this procedure in the outpatient setting in more recent years, there has been a projected increase in the cost savings as well. 18,19 Bekelis et al 20 reported a lower cost of lumbar discectomy performed in the outpatient versus inpatient setting ($13 107 vs $29 906). Purger et al 21 reported a significantly lower overall cost with ACDF performed in the outpatient setting compared with inpatient setting when accounting for the initial procedure as well as all 90-day charges related to complications, readmissions, and reoperations within that time frame ($33 362 vs $74 667). While there is a relative lack of comparative cost data on outpatient versus inpatient lumbar laminectomy in the literature, the available evidence for other spine procedures suggests that the performance of this procedure in the outpatient setting could result in substantial cost savings.
Despite the fact that outpatient lumbar laminectomy appears to be safe, there is a concern that the diagnosis and treatment of certain complications could be delayed. Helseth et al 5 reported on a series of 1449 patients who underwent cervical and lumbar spine surgery in the outpatient setting. Postoperative hematomas were found in 9 of 1449 patients (0.6%), 2 after cervical and 7 after lumbar surgery. Eight of the 9 patients were discovered immediately after surgery and treated with clot removal prior to discharge home the day of surgery. The final patient underwent a single-level lumbar discectomy and woke up with acute abdominal pain due to a retroperitoneal hematoma diagnosed on computed tomography scan. He was transfused 2 units of packed red blood cells and fully recovered without further surgery. 5 Best and Sasso 1 reported on 1 patient of 263 (0.38%) who returned to the hospital the same day after discharge from outpatient lumbar decompression with a symptomatic dural tear. In addition, they reported that the only other complication that occurred in patients who left the same day was an incisional infection (3/263 patients, 1.1%) discovered within a week following the procedure. 1 In all these instances, the diagnosis was made expediently; however, it is possible that a delay in treatment could occur if these patients were discharged home and did not present for urgent evaluation. Thus, it is important that patients being considered for outpatient surgery be educated with regard to the symptoms of potential early complications and counseleld to present for evaluation immediately. In addition, outpatient surgery should be recommended with significant caution for patients who will not have expedient access to a physician postoperatively.
There were several weaknesses inherent to this study. The NSQIP database uses hospital billing data to determine inpatient and outpatient status, which may not accurately reflect the actual length of stay postoperatively. In addition, we identified single- and 2-level lumbar laminectomy cases using CPT codes and as there are a number of different ways to code for single- and 2-level decompression, it is possible that we did not capture all of these cases within the database. Furthermore, this approach relies on the accuracy of the coding for the procedure so it is possible that cases other than a single- or 2-level laminectomy may have been included (eg, discectomy). Another shortcoming of this study with regard to the use of the NSQIP database is the fact that the database only tracks postoperative complications up to the 30 days after the procedure, thus, complications occurring after this timeframe would have been missed. In addition, the NSQIP database also does not include patient satisfaction surveys, which would have provided information with regard to patient preference for surgery in the inpatient versus outpatient setting. Another weakness of this study with regard to the use of the NSQIP database is that we were unable to determine potential instances where a patient may have switched over from the outpatient cohort to the inpatient cohort. This may occur if there are intraoperative complications which necessitate an inpatient level of care. Unfortunately, this data is not available in the NSQIP database and thus could potentially increase the complication rate of the inpatient cohort while decreasing the complication rate of the outpatient cohort. In the literature, there is a relatively low occurrence of this. Three patients (0.2%) required admission to the hospital on the day of surgery due to complications in Helseth et al 5 series of 1449 patients who underwent outpatient cervical and lumbar spine surgery. Best and Sasso 1 reported a 3.8% rate of patients requiring perioperative inpatient admission after outpatient lumbar decompression was performed in their series of 233 patients and noted that the most common reason for admission was pain control. Sivaganesan et al, 22 in their review of the literature on spine surgery performed at ambulatory surgery centers, found an incidence of hospital transfer averaging less than 2% among numerous studies.
Another factor that may have affected the results of our study were potential differences in surgical technique used in the inpatient versus outpatient setting. Unfortunately, we were unable to account for minimally invasive surgery (MIS) versus open approaches for laminectomy as we were only able to screen for the procedure using CPT codes in the NSQIP database and there are no separate CPT codes for MIS techniques. This would be relevant in that there is a trend in the literature for shorter postoperative recovery time, shorter time to mobilization, and decreased postoperative pain with MIS techniques for spine surgery. 23 -25 Despite these differences in recovery, there was no difference in complication rates based on surgical technique, and thus it is unlikely to impact the findings of this study. In addition, differences in postoperative pain management between inpatient and outpatient cohorts could have impacted the observed results in that opioid use is associated with adverse effects including gastrointestinal dysfunction, respiratory depression, and urinary retention. 26 Furthermore, postoperative pain has been shown to be a common cause for unplanned 30-day readmission as well as increased length of postoperative hospital stay. 27 Importantly, without an adequate pain control regimen, patients undergoing laminectomy in the outpatient setting would require hospitalization for pain control (as previously noted). 1 Multimodal pain management regimens have been shown to allow for improved pain control with decreased use of opiods and their associated adverse effects. 26,27 Unfortunately, methods of postoperative pain management were not available for review in the NSQIP database and if a difference existed between the inpatient and outpatient cohorts, this may have played a role in the observed complication rate.
The strengths of the NSQIP database include prospective data collected on a large number of patients included over multiple centers in the United States allowing for high-powered analysis with greater generalizability. 12 In addition, trained, on-site, surgical clinical reviewers collect the perioperative data in the NSQIP database, which increases the reliability and sensitivity of the database for the assessment of postoperative complications when compared with other databases. 12
Other weaknesses of this study include the possibility of selection bias. The outpatient cohort was younger, less obese, and had fewer comorbidities (Table 1) compared with the inpatient cohort which could be at least partially responsible for the increased complication rate seen in the inpatient cohort. 28 -31 In addition, NSQIP data is collected prospectively and, as such, patients are not randomized, which could also introduce bias. Despite these weaknesses, the significant difference in complication rates between the 2 cohorts persisted after propensity-matched analysis, which has been shown in other studies to approach the statistical power of a randomized study. 32
In conclusion, this study demonstrated that single- and 2-level lumbar laminectomy performed in the outpatient setting did not confer an increased 30-day risk of complications when compared with the procedures performed in the inpatient setting. In fact, performance of these procedures in the outpatient setting appeared to be associated with a lower overall complication rate in the 30-day postoperative period. In addition, this study identified multiple independent risk factors for any complication following lumbar laminectomy. This data suggests that outpatient lumbar laminectomy is a viable and potentially safer option than inpatient lumbar laminectomy in appropriately selected patients. Future studies are needed assessing patient satisfaction and perception of outpatient versus inpatient surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.