
Abstract
Study Design
Systematic review and meta-analysis.
OBJECTIVESSurgical decompression alone for patients with neurogenic leg pain in the setting of degenerative lumbar scoliosis (DLS) and stenosis is commonly performed, however, there is no summary of evidence for outcomes.
Methods
A systematic search of English language medical literature databases was performed for studies describing outcomes of decompression alone in DLS, defined as Cobb angle >10˚, and 2-year minimum follow-up. Three outcomes were examined: 1) Cobb angle progression, 2) reoperation rate, and 3) ODI and overall satisfaction. Data were pooled and weighted averages were calculated to summarize available evidence.
Results
Across 15 studies included in the final analysis, 586 patients were examined. Average preoperative and postoperative Cobb angles were 17.6˚ (Range: 12.7 - 25˚) and 18.0 (range 14.1 - 25˚), respectively. Average change in Cobb angle was an increase of 1.8˚. Overall rate of reoperation ranged from 3 to 33% with an average of 9.7%. Average ODI before surgery, after surgery, and change in scores were 56.4%, 27.2%, and an improvement of 29% respectively. Average from 8 studies that reported patient satisfaction was 71.2%.
Conclusions
Current literature on decompression alone in the setting of DLS is sparse and is not high quality, limited to patients with small magnitude of lumbar coronal Cobb angle, and heterogenous in the type of procedure performed. Based on available evidence, select patients with DLS who undergo decompression alone had minimal progression of Cobb angle, relatively low reoperation rate, and favorable patient-reported outcomes.
Introduction
Degenerative lumbar scoliosis (DLS) is a prevalent condition amongst the growing elderly population. 1 Unlike idiopathic scoliosis, DLS is characterized by a mid-lumbar curve with minimal compensatory thoracic curve, hypolordosis, rotatory deformity at the apex, coronal/sagittal subluxation, and stenosis. 2 Radiculopathy and neurogenic claudication in the setting of DLS are common due to the presence of both central, lateral recess, and foraminal stenosis. 3 Significant variability in radiological findings, presenting symptoms, and a heterogeneous patient population creates controversy on the best strategies to manage the condition.4,5
Surgical management options include decompression alone, decompression with limited fusion, and decompression with multilevel fusion for the goal of scoliosis correction. 6 The use of decompression alone for radiculopathy or neurogenic claudication in the setting of DLS with stenosis is controversial.7–9 Proponents of limited surgical intervention through simple decompression alone, cite advantages in select patients, particularly in the elderly and frail. 10 Opponents of this approach suggest that if a scoliotic deformity contributes to the clinical presentation then fusion is necessary to adequately decompress the neural elements and prevent the progression of deformity.8,9 Although decompression alone procedures may limit upfront costs, a failure to stop the progression of deformity may lead to revision surgeries and increased costs long-term. 11
This systematic review and meta-analysis assesses the functional and radiological outcomes of decompression alone in patients with DLS.
Materials and Methods
Literature Search Strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed for the present systematic review. Electronic searches were performed using Ovid Medline, PubMed, Cochrane Central Register of Controlled Trials (CCTR), Cochrane Database of Systematic Reviews (CDSR), and Database of Abstracts of Review of Effectiveness (DARE), from their dates of inception to February 2021. The final search string was: “lumbar scoliosis” OR “degenerative scoliosis” OR “adult spinal deformity” AND “decompression.” The reference lists of all retrieved articles were reviewed for further identification of potentially relevant studies.
Eligibility Criteria
All studies undergoing full-text screening were included if the following criteria were met: (1) published prior to February, 2021; (2) peer-reviewed, original, and written in the English language or full-English translation available; (3) reported on clinical and/or radiographic outcomes of lumbar decompression alone in patients with de novo or degenerative lumbar scoliosis, defined as Cobb angle >10˚, no known history of adolescent idiopathic scoliosis, and with 2 year minimum follow-up; (4) format of a randomized controlled trial, nonrandomized trial, case series (≥ 2 patients), case-control study, or cohort study. Abstracts, case reports, conference presentations, editorials, reviews, and expert opinions were excluded. No ethics approval was required for this study with all data obtained from a review of the literature.
Data Extraction
Abstracts were screened by 2 reviewers, ME and JS, using the inclusion and exclusion criteria stated above. In cases of disagreement, a third independent reviewer was involved to make the final decision. The inclusion and exclusion of studies was performed according to the latest version of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Statement (www.prisma-statement.org). The bias of each study was evaluated with the criteria recommended by the Cochrane Back Review Group, and studies were considered to have an overall low risk of bias when at least 6 of the individual criteria were determined to have a low risk of bias. 12
Levels of evidence were assigned based on the North American Spine Society guidelines. Three outcomes were examined: (1) radiological Cobb angle progression, (2) reoperation rate including the need for fusion, and (3) patient-reported outcome measures including Oswestry Disability Index (ODI), Visual Analog Scale (VAS) for leg and back pain, and overall satisfaction. Data were pooled to summarize the available evidence. A qualitative review of risk factors for progression of scoliosis after decompression was performed.
Statistical Analysis
Weighted means were calculated for demographic variables, spinal measurements, and outcome measures. Studies were weighted according to their reported sample size. Calculations were performed using Python 3.8.3 and the publicly available package Pandas 1.0.5.
Results:
Search results are summarized in the PRISMA flow diagram shown in Figure 1. Our search returned 483 results from the search of online databases. Two additional references were added after the bibliography review of included studies. After the removal of 217 duplicates, 266 records were screened for eligibility based on title and abstract. After screening, 39 full-text versions of the remaining studies were collected and further assessed for eligibility. Of these 39 studies, 15 were found to meet inclusion criteria for analysis. Of the 24 articles excluded, 12 were review articles offering expert opinion, 4 had insufficient follow-up time, and 8 did not separate outcome results for patients that did or did not have degenerative lumbar scoliosis or from patients that underwent fusion. PRISMA Diagram.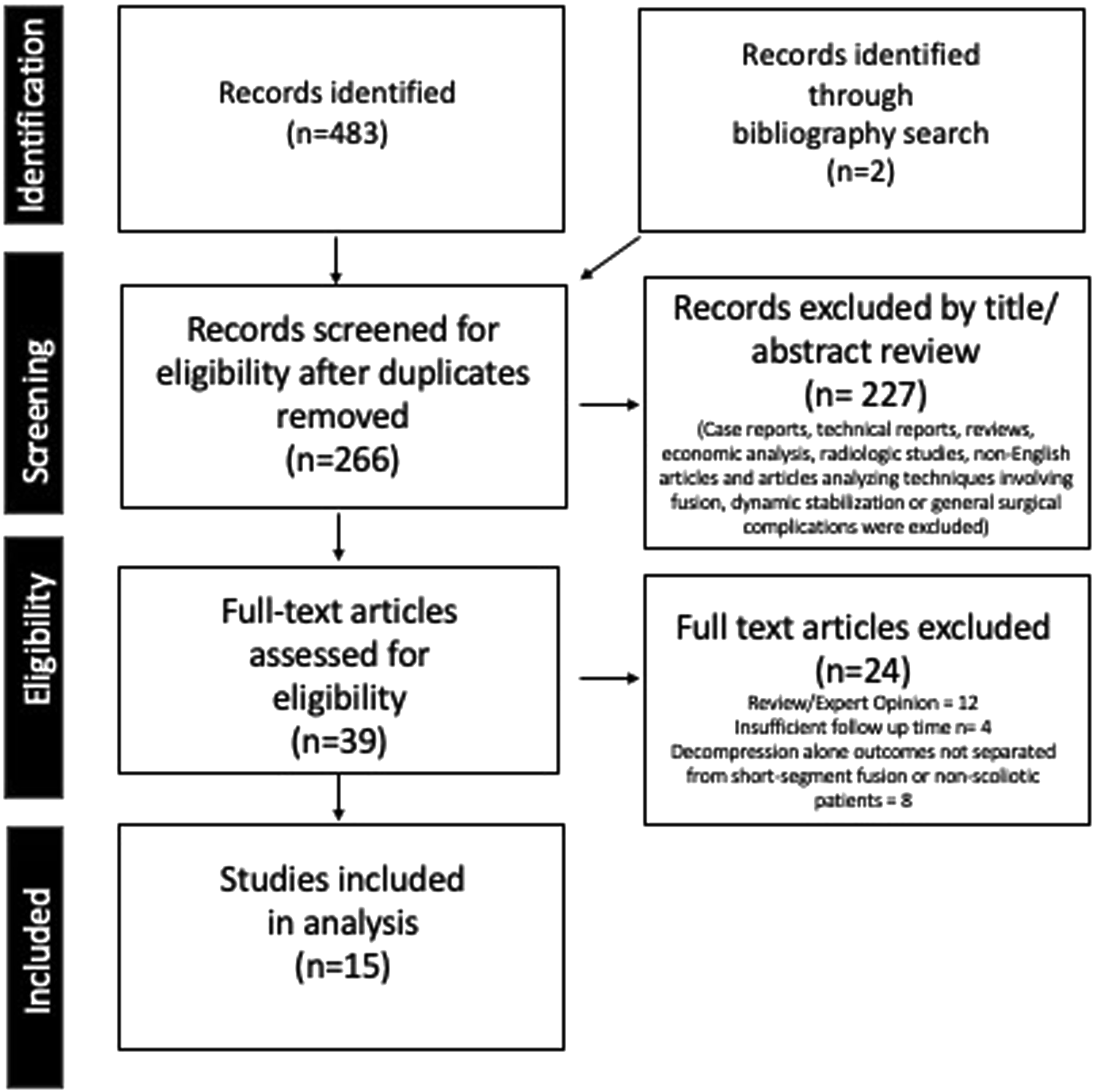
Included Studies and Patient Demographics
Included studies and level of evidence.
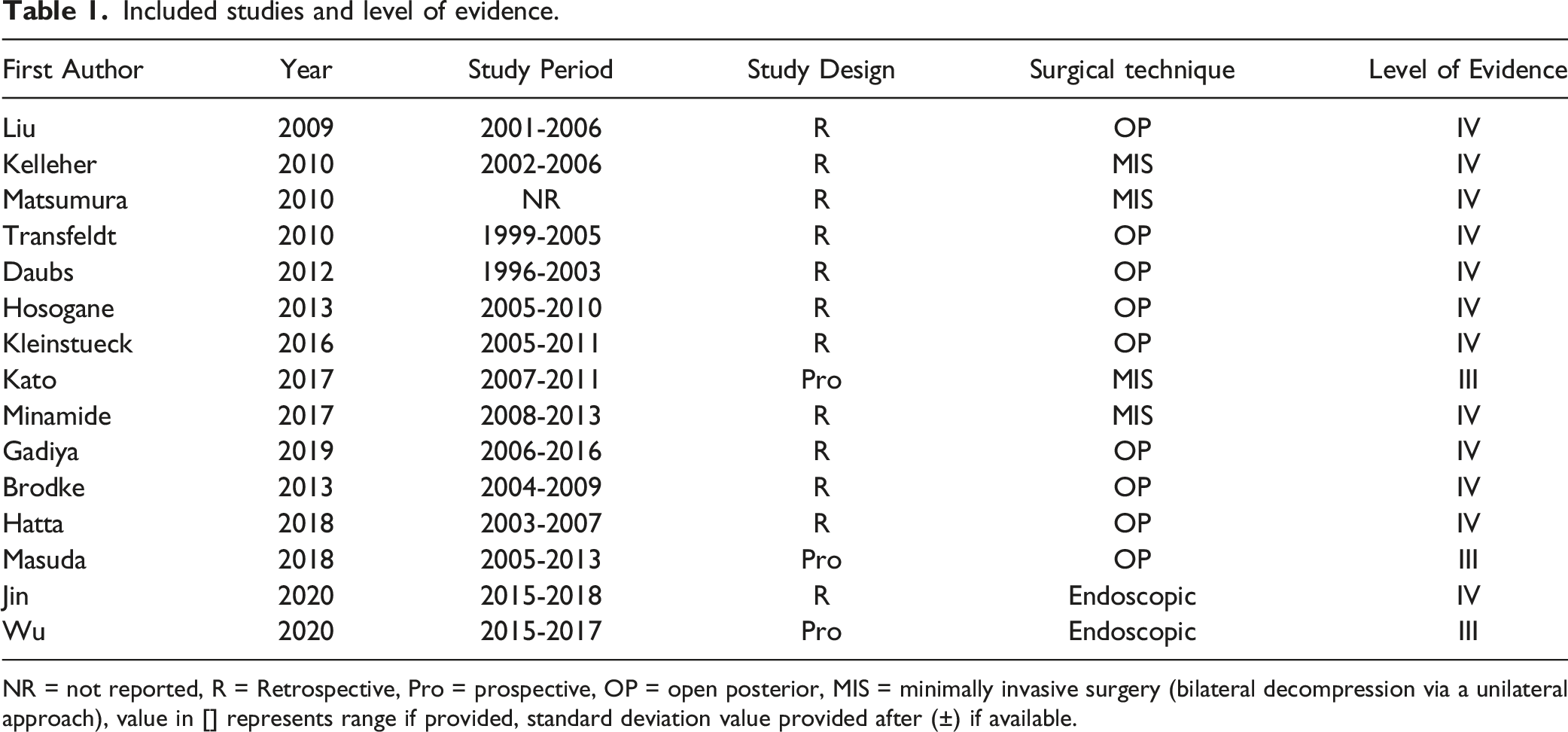
NR = not reported, R = Retrospective, Pro = prospective, OP = open posterior, MIS = minimally invasive surgery (bilateral decompression via a unilateral approach), value in [] represents range if provided, standard deviation value provided after (±) if available.
Patient Demographics.
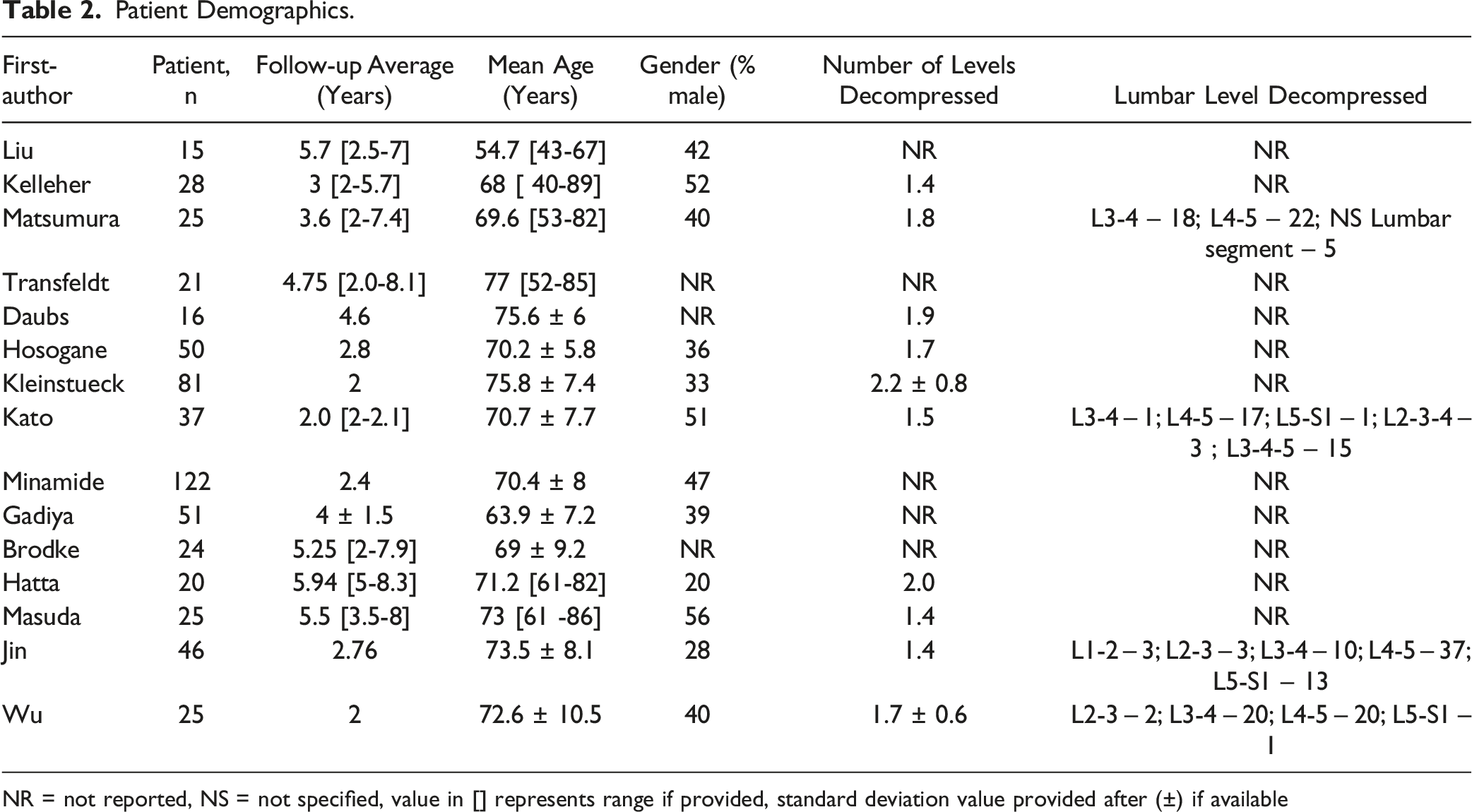
NR = not reported, NS = not specified, value in [] represents range if provided, standard deviation value provided after (±) if available
Radiographic Outcomes
Radiographic Outcomes
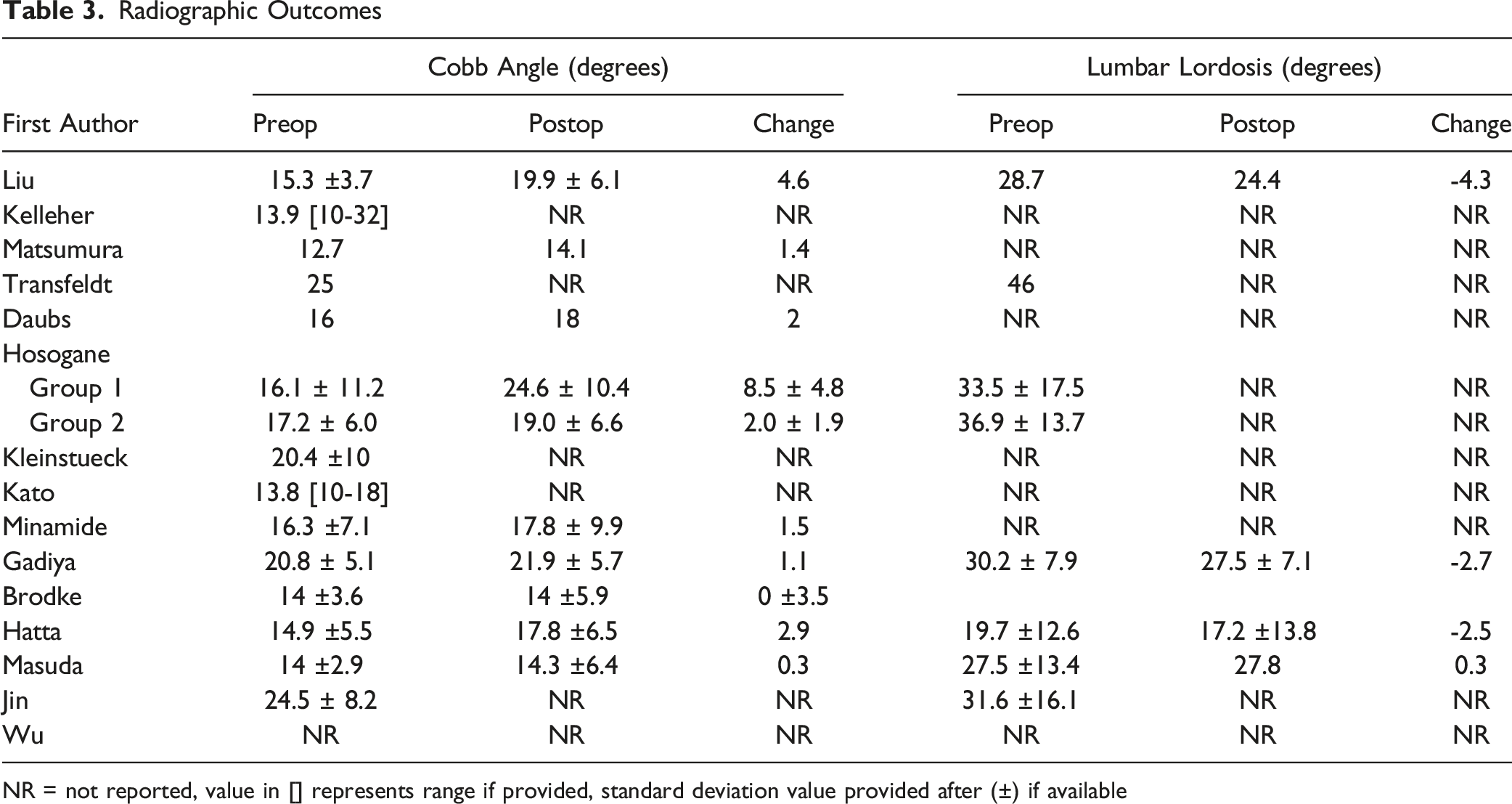
NR = not reported, value in [] represents range if provided, standard deviation value provided after (±) if available
Four of the included studies reported preoperative and postoperative lumbar lordosis with or without describing pelvic incidence whereas 3 studies included only preoperative values.14,20,24,25 The average pre-operative lordosis was 32.0 degrees and post-operative lordosis was 25.2 degrees. The average change in lumbar lordosis was a negative (-) 2.2 degrees. Among the studies that included the lumbar lordosis, the average follow-up period was 4.9 years.
Clinical Outcomes
Clinical Outcomes
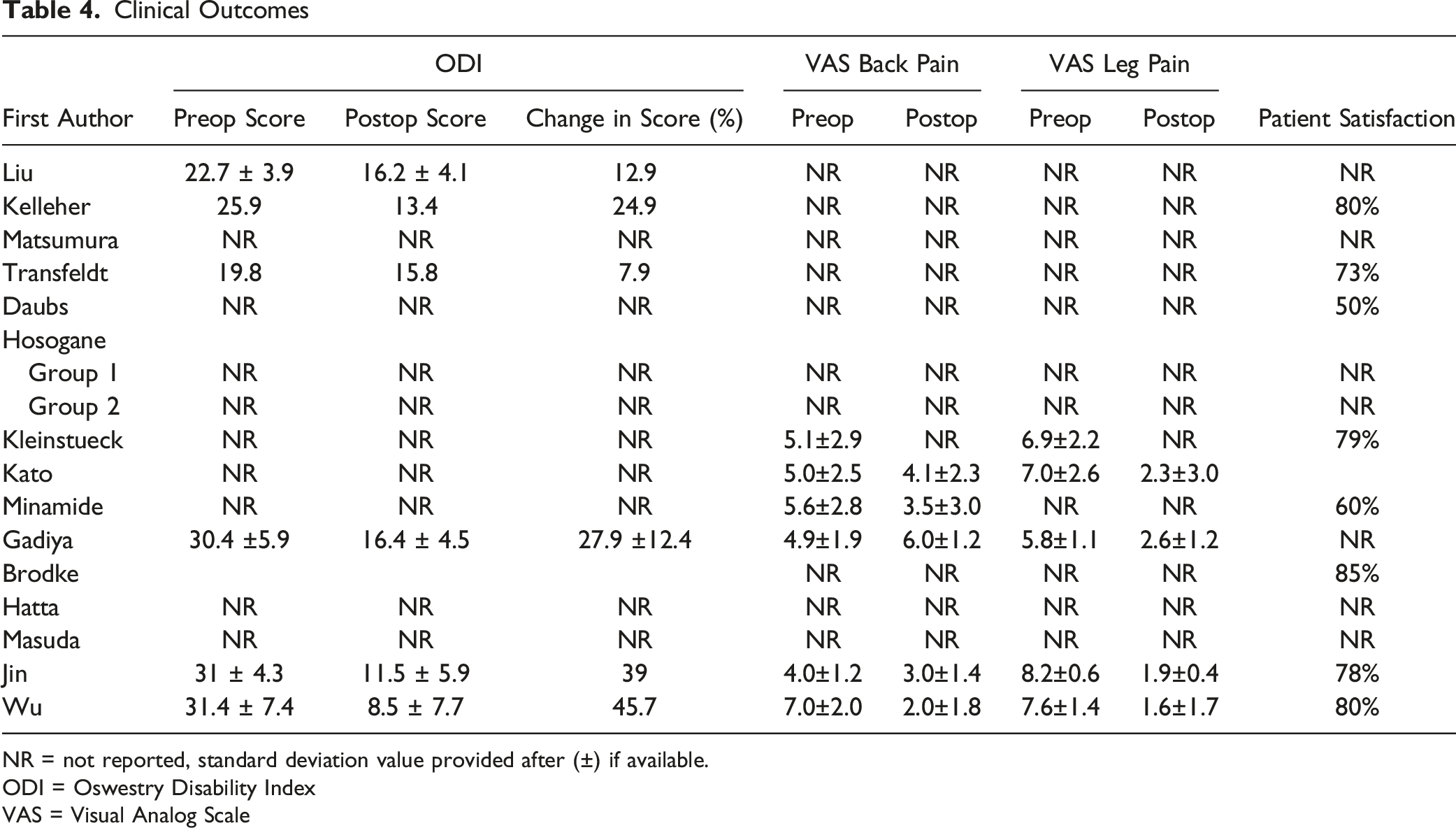
NR = not reported, standard deviation value provided after (±) if available.
ODI = Oswestry Disability Index
VAS = Visual Analog Scale
Complication and Revision Rates
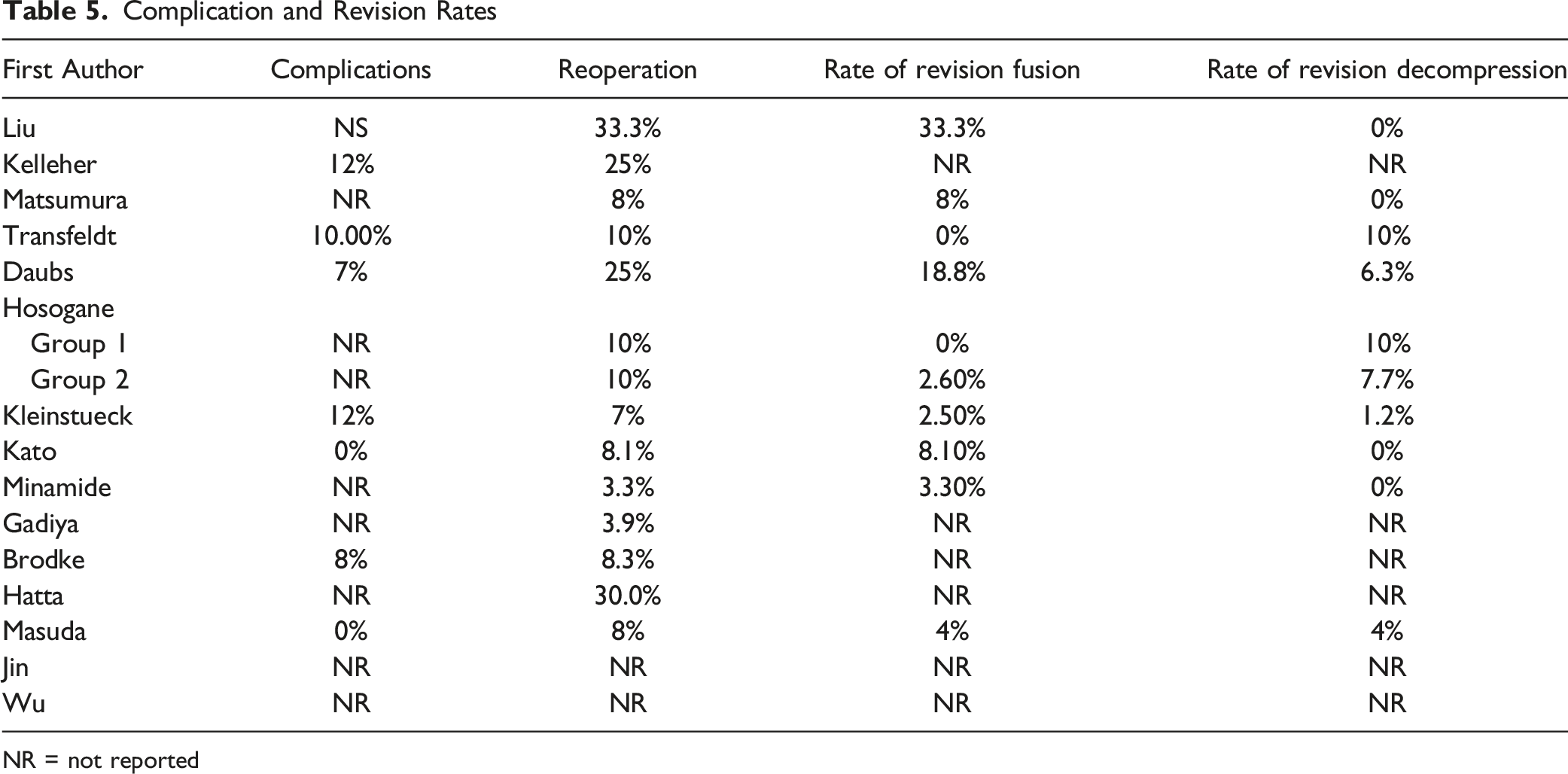
NR = not reported
Risk Factors for Progression of Scoliosis and Revision Surgery or Poor Outcomes
Four studies further specified risk factors for Cobb angle progression, revision surgery, and poor outcomes. Matsumura et al reported 2 patients requiring additional fusion, of which 1 was due to poor facet preservation leading to curve progression. 17 They further postulated that the approach side may influence facet preservation, and when using the convex approach there was around 80% of the facet preserved and no curve progression. In contrast, the concave approach led to approximately 50% facet preservation, which may have led to curve progression and poor clinical outcome in the 2 reported patients. Conversely, Hosogane et al found that Cobb angle progression did not affect outcomes. They compared patients that demonstrated Cobb angle progression over 5 degrees (Group 1) and no progression (Group 2), and reported equal rates of reoperation of 10% for both groups. 23
Hosogane et al also performed analysis of 15 variables to determine risk factors for progression of the lumbar curve, including vertebral osteophyte on the concave or convex side, decompression method (fenestration vs laminectomy vs spinous process splitting), age, disc degeneration, L-5 tilt angle, follow-up period, decompression level, apical vertebral rotation, Cobb angle at decompression level, lumbar lordosis, T10-L2 sagittal angle, rotatory subluxation >5mm, Cobb angle of main curve, pelvic tilt angle, and spondylolisthesis >5mm. 23 However, in both their univariate and multivariate logistic regression analysis no variable reached statistical significance.
Minamide et al found that patients with preoperative Cobb angle over 20 degrees were more likely to have curve progression more than 5 degrees than patients with preoperative Cobb angle less than 20 degrees (40 vs 15%, P < .05) as well as a higher rate of additional fusion (13 vs 1%, P < .05). 19 They also evaluated risk factors for poor outcomes based on Japanese Orthopaedic Association (JOA) score, and demonstrated that gender, preoperative severe lumbar coronal Cobb angle (mean; 29.6 ± 7.9º), increased preoperative pelvic tilt (mean; 28.3 ± 11.5 º) and preoperative mismatch of pelvic incidence minus lumbar lordosis (mean; 35.5 ± 21.2 º) were significant (P < .05).
Transfeldt et al performed a logistic regression analysis for probable risk factors for less than successful outcomes and demonstrated 2 significant factors, a sacrum to curve apex fusion, and a positive sagittal malalignment greater than 4.0 cm after surgery. 16 Rotatory olisthesis was not found to be a significant factor.
Discussion
Degenerative lumbar scoliosis with associated stenosis remains a challenging spinal pathology without a standard surgical treatment algorithm based on high-quality evidence. 28 This is due to limited evidence as the majority of studies (12 out of 15) included in this systematic review were retrospective case series, level IV evidence. In addition, the complexity of the pathology along with a highly variable amount of patient comorbidities, functional status, and both surgeon and patient preferences add to the convolution of decision making for surgery. 6 An increasing number of complex reconstructive surgery being performed for DLS has raised concerns about the high rate of complications and revision surgery as well as the higher total cost, especially in elderly patients. 29 Limiting surgical morbidity to the least invasive approach via decompressing areas of stenosis alone has become favored in select patient populations. 30 However, the durability of this approach has not yet received a full appraisal of the literature. 31 In this systematic review, for the first time the radiographic and clinical outcomes of decompression alone in the setting of DLS over an average 3-year period are described.
Radiographically, the degree of scoliosis as measured by Cobb angle progressed at a rate of approximately 2 degrees per 2-year follow-up after surgery. This rate is equivalent to the rate of progression seen with natural history as reported by Pritchett and Bortell of an average 3 degrees per year over a 5 year period. 32 Of note, the patient population in their study had a higher average preoperative Cobb angle of 24 degrees compared with the weighted mean of 17.6 degrees seen across the selected studies presented here. Thus, among the well-selected patients included in the above publications, with mild to moderate degenerative lumbar curves, there was a low magnitude of progression following decompression alone. Although mild hypolordosis and positive sagittal malalignment were present among the included patients, this finding did not significantly worsen in the reported results following decompression alone. Buckland et al demonstrated patients with DLS permit mild to moderate sagittal malalignment without recruiting compensatory mechanisms to achieve neural decompression, however ultimately the drive for upright posture becomes the priority seen by the adoption of increased pelvic tilt. 33
Current trends include finding minimally invasive surgery (MIS) alternatives for DLS.34,35 A prior meta-analyses focusing on MIS approaches to DLS by Dangelmajer et al compared twelve studies in the MIS group, including 8 studies utilizing extreme lateral interbody fusion (XLIF) and 4 studies utilizing decompression alone, against thirty-five studies in the open surgery and fusion group with or without osteotomy. 36 Another meta-analysis by Wang et al also compared various surgical treatments for DLS, including 9 studies that performed decompression alone. 37 3 of these studies, however, incorporated dynamic stabilization instrumentation as part of the decompression alone group. Thus, both systematic reviews did not yield more than 6 studies that performed decompression alone because of a limited search and broad comparisons. As such, this current systematic review builds upon the previous works by adjusting a focus solely to assessing the outcomes of the least invasive approach available – decompression alone.
Previous studies favored fusion for patients with DLS due to the perceived high revision rate for decompression alone. 8 There is, however, also a high rate of complications and revision surgery following short-segment fusion or full curve correction with the reported incidence varying between studies.38,39 Reoperation risk from a large prospective multicenter adult spinal deformity database report a 17% risk of reoperation, including instrumentation failure as the most common reason for a return to surgery. 40 Pellise et al recently analyzed the 2 largest multicenter data sets available, and, even with significant improvements in surgeon experience and medical management, the most recent 2 year major complication rate was 23% and reintervention rate was 16%. 41 Clearly, the patients in this study have a greater degree of spinal deformity and are not readily comparable to the patients represented in this systematic review. However, trends in the improvement of quality metrics coincided with trends in decreased surgical invasiveness, including a decrease in mean number of fused segments, pelvic fixation, and three-column osteotomies. Similarly, Deyo et al found in a retrospective cohort analysis of Medicare claims of procedures performed for older patients with spinal stenosis trends of increasing frequency of complex fusions and decreasing frequency of decompression alone were associated with a rise in major complications, 30-day mortality, and costs. 42 As such, further work must be done to identify appropriate cases for decompression alone in DLS, and to compare effectiveness to more complex and potentially higher risk short-segment fusion or full curve corrections.
Brodke et al provided a direct comparison between laminectomy without fusion vs laminectomy and fusion by excluding patients from the study if the deformity precluded the option for either treatment. 27 The radiographical parameters varied minimally with mean preoperative Cobb angle of 14 degrees for both groups. Their results demonstrate that laminectomy and fusion had a higher rate of reoperation due to symptomatic adjacent segment pathology, whereas laminectomy alone had the highest rate of progression free survival. Thus, when considering surgical options there must be an analysis between the rate of re-developing stenotic symptoms or instability in decompression alone vs the rate of pseudarthrosis and adjacent segment complications in fusion procedures. Additionally, proceeding to full curve correction is less invasive following previous decompression alone than after a previous in-situ short-segment fusion. 43
Studies that included patients treated by all 3 methods were specifically described as distinct patient populations not intended for direct comparison.16,18,26 This current review is therefore unable to decide which surgical technique is best for DLS, however demonstrates that decompression alone is an effective intervention in the well selected patient groups represented herein. Mummaneni et al presented an updated 4-level treatment algorithm, the MISDEF2 algorithm, to aid spine surgeons in fitting patients into specific criteria. 44 Glassman et al also presented appropriate use criteria for lumbar degenerative scoliosis. 45 Both papers provide a more thorough overview of the decision-making process to select an appropriate level of intervention given the patient’s primary symptoms and radiographic findings. However, both papers relied on panels of experts that methodically determined appropriateness of an intervention for a specific clinical scenario. Our results after a systematic review of the literature offers further evidence-based support for these expert recommendations. It is important to note smaller deformities with small coronal Cobb angle less than 20 degrees and normal sagittal alignment are a common presentation seen in clinical practice. Yet, the decision to offer decompression alone for these patients is primarily based off expert opinion and has not been well studied, as demonstrated by the low level of evidence available. Thus, most importantly this systematic review demonstrates a need for these patients with mild to moderate DLS to be enrolled in large, multicenter prospective comparison studies with greater follow-up periods.
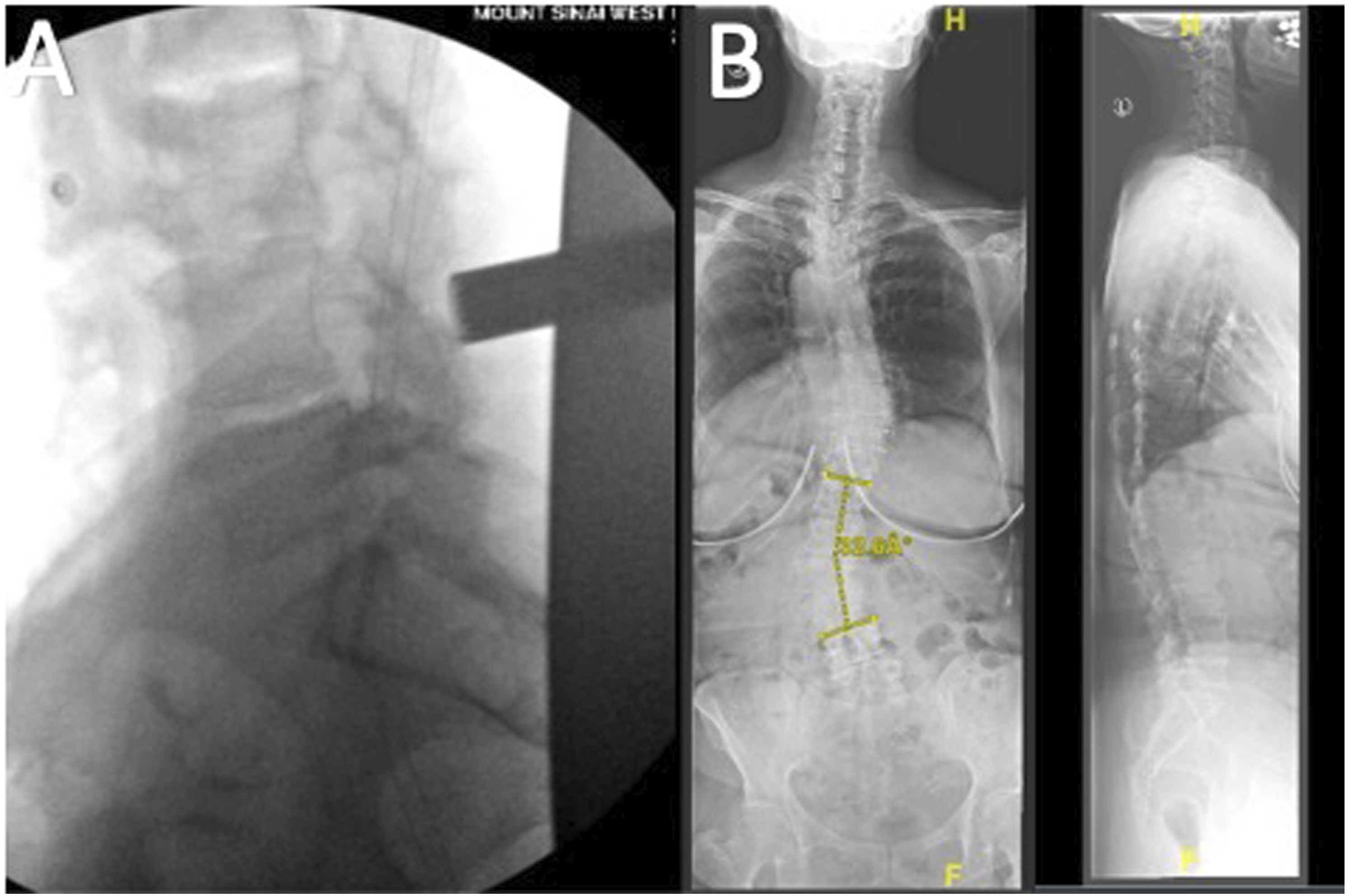
Risk factors for poor patient-reported outcomes included preoperative severe lumbar coronal Cobb angle (mean; 29.6 ± 7.9º), increased preoperative pelvic tilt (mean 28.3) preoperative mismatch of pelvic incidence minus lumbar lordosis (mean 35.5), and poor facet preservation (approximately 50%) on the approach side of the concavity.17,19 However, a patient that falls outside these parameters is represented in Figure 2 with a severe T12-L4 curve of 33 degrees but relatively balanced without significant coronal offset or sagittal malalignment. Figure 3 demonstrates a MIS decompression with follow-up full-length x-rays demonstrating a stable deformity. Faraj et al performed a systematic review of prognostic factors for curve progression in DLS, and found that the majority of prognostic factors were limited, conflicting, or inconsistent.
46
As such, the authors demonstrated that many of these risk factors may not be directly applicable to an individual patient. Thus, shared decision making with the patient and considering their chief complaints and goals of surgery are paramount. Studies that measured the intensity of leg to back pain demonstrated the importance of an absence of severe back pain (VAS <8), as predominant axial back pain is strongly correlated with potential instability or sagittal imbalance.13,15,22,25 Further work may define more strict criteria based on the ratio of leg pain to back pain. A 68 year-old woman presenting with primarily left greater than right radiating leg pain due to cranial disc extrusion and spinal stenosis at L4-5 seen on sagittal T2-weighted MRI (A), axial cuts shown at the level behind the L4 body and L4-5 disc space, respectively (B & C), and a severe T12-L4 curve of 33 degrees on standing AP lumbar x-ray (D). demonstrates a minimally invasive tubular decompression (A) with 1-year follow-up full-length AP and Lateral x-rays (B) demonstrating a stable deformity without progression.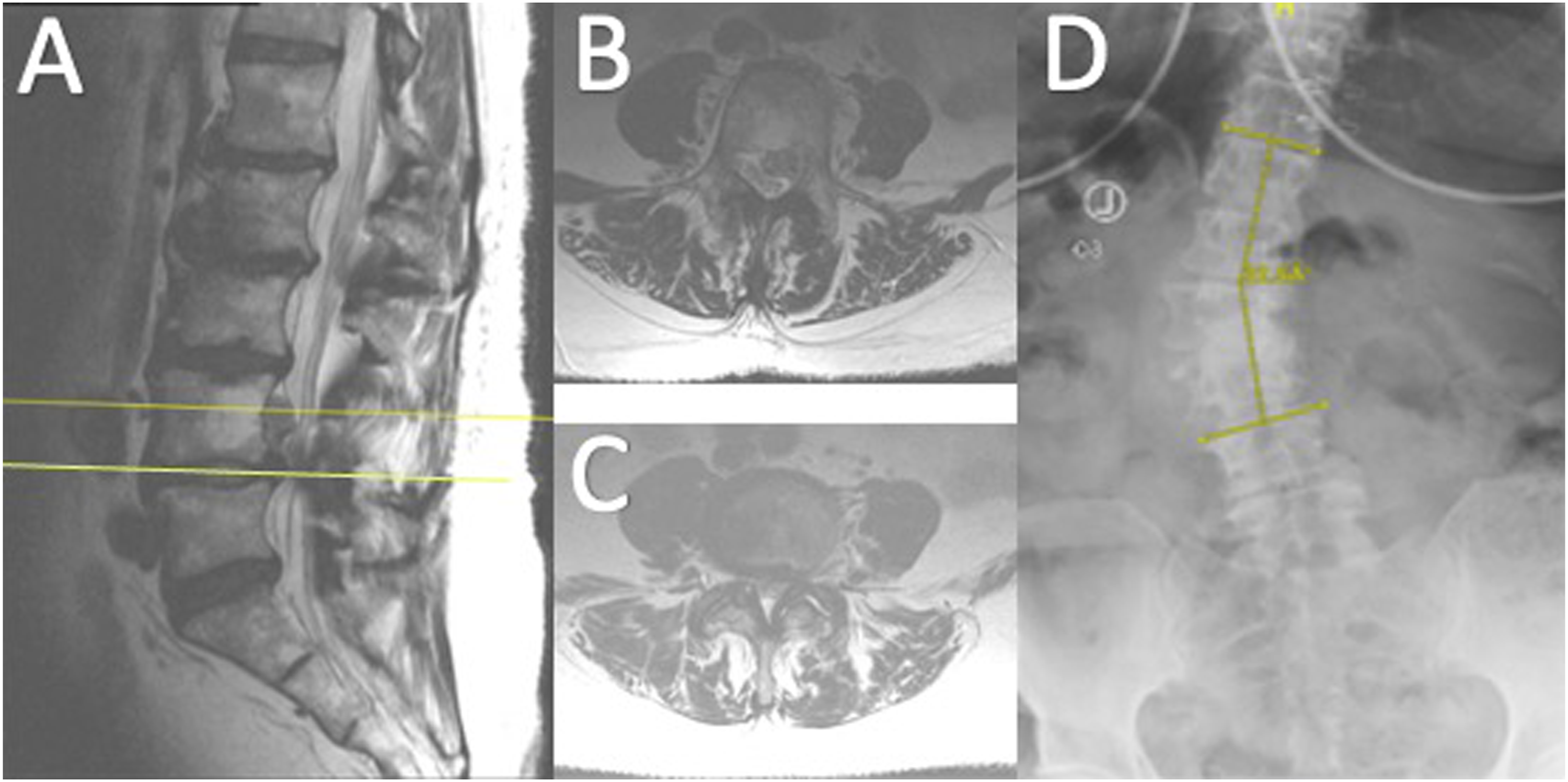
Other factors to consider are foraminal stenosis due to severe disc wedging resulting from approximation of the pedicles will be better suited via interbody fusion allowing for indirect decompression in the cranial-caudal dimension. In addition, the finding of a mobile spondylolisthesis coexisting with DLS is a contraindication to decompression alone and necessitates at least a limited fusion. 14 Phan et al demonstrated that these patients with mild DLS and focal deformities or instability may be more amenable to a short vs long segment fusion. 47
As the number of older and elderly patients with DLS increases so does the prevalence of osteoporosis in spinal surgery.48,49 Decreased bone mineral density was previously thought to be a significant risk factor for progression seen in the natural history of DLS, with regional malalignment resulting in asymmetric compression fractures and accelerating the progression of deformity.50,51 However, recent studies have demonstrated no correlation between bone mineral density and curve progression in DLS, including both measurements on dual-energy x-ray absorptiometry scans and Hounsfield units.46,52–54 Osteoporosis and bone mineral density have, on the other hand, consistently demonstrated to be a major risk factor for instrumentation failure and proximal junctional failure.55–58 Unfortunately, none of the current studies listed herein are stratified by bone mineral density measurements, and thus no conclusions can be made regarding its effect on decompression alone in DLS. This is a major potential area of study.
Limitations
Limitations of this study include the inability to directly compare results between decompression alone, short-segment, and long-segment fusions. While several reports include patients treated by all 3 methods, they were specifically described as different patient populations not meant for comparison. The ability to provide a meta-analysis comparing outcomes was thus limited by the methods of the included papers.
The other main limitation to this analysis is the low level of evidence in all the included studies, and the indications for decompression alone, the surgical techniques, and outcome measures varied significantly. Thus, the reported case series are susceptible to bias in their results. It is also difficult to draw final conclusions from small sample sizes which was made more complex by heterogeneity of levels, approach side at the convexity vs concavity, limited radiographic follow-up, and no standard reported outcome measures. Importantly, lumbar lordosis and pelvic tilt were poorly reported, and it is not known if the decompressions were primarily in the fractional curve or at the concavity of the mid-lumbar curve. However, all studies reported decompressions only in the lumbar spine, and not remote from the degenerative lumbar scoliosis.
Duration of follow-up was another profound limitation, particularly in DLS where the natural history is slow and greater time intervals are needed. The longest average follow-up period was shy of 6 years, and the minimum was 2-year follow-up. If significant destabilization after decompression alone occurred presumably deterioration will be seen within the first 2 years. However, if the durability of a procedure is under analysis, then future studies with long-term follow-up of 10-years is required.
Additionally, while all included studies report only patients with adult degenerative, or de novo, scoliosis were included, it is possible that some patients were actually untreated adolescent idiopathic scoliosis (AIS) with superimposed degenerative changes. This is an important factor since DLS and adult progression of AIS are distinct in their treatment and prognosis. However, patients with adult progression of AIS are typically easy to differentiate by the presence of higher degrees of curvature and younger age of presentation. The included patients reported by each study demonstrated lesser degrees of curvature and older age making this possible confounding factor less likely.
While the analysis is limited to compiling the available data for decompression alone for DLS, it provides for the first time a compilation of the literature regarding the radiographic and clinical outcomes of decompression alone in the setting of DLS over an average 3-year period. This results in a consistent demonstration of a relatively low rate of deformity progression and need for revision surgery in carefully selected patients. Perhaps most compelling to advocate for a decompression only approach in these case series is to reflect its already accepted use in current clinical practices. In addition, risk factors for Cobb angle progression, revision surgery, and poor outcomes revealed in the included studies represent important considerations for clinical evaluation and for future study. The weighted averages described herein may provide a baseline, but most importantly demonstrates a need for future large, multicenter prospective comparison studies with greater follow-up periods.
Conclusions
Current literature on decompression alone in the setting of DLS is sparse and is not high quality, limited to patients with small magnitude of lumbar coronal Cobb angle, and heterogenous in the type of procedure performed. Based on available evidence, well-selected patients with DLS who undergo decompression alone had minimal progression of Cobb angle, relatively low reoperation rate, and favorable patient-reported outcomes. A low complication rate and durable outcomes may be expected for selected patients with predominant symptoms related to stenosis in the presence of mild degenerative scoliosis, but further study is needed.
Supplemental Material
Supplemental Material - Decompression Alone in the Setting of Adult Degenerative Lumbar Scoliosis and Stenosis: A Systematic Review and Meta-Analysis
Supplemental Material for Decompression Alone in the Setting of Adult Degenerative Lumbar Scoliosis and Stenosis: A Systematic Review and Meta-Analysis by Murray Echt, Rafael De la Garza Ramos, Eric Geng, Ula Isleem, Julia Schwarz, Steven Girdler, Andrew Platt, Adewale A Bakare, Richard G. Fessler, and Samuel K Cho in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Richard Fessler receives consulting fees from DePuy-Synthes and Benvenue. Dr. Samuel Cho receives consulting fees from Globus, Zimmer, and Medtronic. The other authors have no conflict of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.