
Abstract
Study Design:
Retrospective cohort study and systematic review.
Objectives:
Endoscopic decompression offers a minimally invasive alternative to traditional, open laminectomy. However, comparison of these surgical techniques has been largely limited to small, single-center studies. In this study, we perform the first international, multicenter comparison of both with regard to their associated rates of mortality, complications, readmissions, and reoperations.
Methods:
The 2017 American College of Surgeons’ National Surgical Quality Improvement Program (ACS-NSQIP) database, containing data from over 650 hospitals internationally, was queried to evaluate the effect of endoscopic guidance on adverse events. Operative time, length of stay, readmission and reoperation rates, as well as the incidence of peri- and postoperative complications, were compared between endoscopic and open groups. The PubMed/MEDLINE database was queried for studies comparing the techniques.
Results:
A total of 10 726 single-level lumbar decompression patients were identified and included in this study, 34 (0.32%) of whom were operated upon endoscopically. Apart from 2 (5.88%) readmissions, among which only 1 was unplanned, there were no reported surgical complications within the endoscopic group. The mean length of stay for these patients was 0.86 ± 1.44 days, with procedures lasting an average of 91.89 ± 46.72 minutes. However, these endpoints did not differ significantly from the open group. On literature review, 16 studies met the inclusion criteria, and largely consisted of single-center, retrospective analyses.
Conclusions:
Endoscopically guided approaches to single-level lumbar decompression did not reduce the incidence of adverse events, length of stay or operative time, perhaps due to advances among certain nonendoscopic techniques, such as microsurgery.
Introduction
Lumbar spinal stenosis is the most common indication for back surgery in adults older than 65 years and is characterized by the narrowing of the spinal canal with subsequent impingement upon neural structures by surrounding bone and soft tissue. 1 –3 The pathophysiologic development of stenosis is complex and multifactorial, most commonly resulting from degenerative changes to spinal structures, including hypertrophy of the ligamentum flavum, bulging of the intervertebral disc, and facet joint arthropathy. 2 Clinically, this often manifests in the fifth and sixth decades of life as generalized lower back pain, radicular leg pain, and/or sensorimotor deficits in the lower extremities. 3 –5
Open lumbar laminectomy has long been considered the conventional surgical intervention for decompression of lumbar stenosis. 1,2,6 However, this technique involves extensive muscle dissection and detachment in order to adequately exposure and resect posterior spinal elements, consequently resulting in potentially significant blood loss, postoperative pain, and generalized weakness. 2,6 Additionally, disruption of patients’ native anatomy due to paraspinous soft tissue injury and removal of midline ligaments can lead to significant pain and muscular atrophy. 7 Thus, the performance of microendoscopic procedures has surged in recent years, in an effort to provide adequate decompression through smaller incisions while preserving midline musculotendinous structures and soft tissues. 1,6,7 More specifically, 2 “portal” incisions are rendered laterally—one for the endoscope and the other for instruments, with additional portals added per subsequent vertebral level. 8 However, concrete evidence supporting the use of these minimally invasive, endoscopic techniques over traditional, simple open laminectomy without instrumentation remains to be seen. Relatively few studies have directly compared surgical outcomes, operative metrics, complications, readmissions, and reoperations between endoscopic and nonendoscopic decompression, and those that have tend to be underpowered. Here, we conduct the first international, multi-institutional comparison of these 2 techniques with regard to their associated adverse events, operative time, length of stay, readmissions, and reoperations.
Methods
Patient Selection
A retrospective cohort analysis was conducted using de-identified patient-level data queried from the American College of Surgeons’ National Surgical Quality Improvement Program (ACS-NSQIP, or simply NSQIP) database for the 2017 calendar year. The program contains data from over 680 hospitals across at least 14 countries around the world. 9 –11 Only 2017 data was utilized due to the fact that a new Current Procedural Terminology (CPT) code for endoscopic lumbar decompression—62380—was introduced during that year, allowing us to differentiate between endoscopic and “open” (simple nonendoscopic) approaches, with the latter categorized under the code 63030. 12 Patients whose primary CPT code was either of the 2 aforementioned were included in our study, and separated into endoscopic and nonendoscopic groups accordingly.
Data Acquisition
All relevant baseline patient characteristics provided by NSQIP were collected, including age, sex, race/ethnicity, height, weight, admission status (ie, outpatient vs inpatient), primary diagnosis (ie, disc disease, osteophytes, ligamentum flavum hypertrophy, etc), and past history of comorbidities such as diabetes, smoking, chronic obstructive pulmonary disease (COPD), congestive heart failure, hypertension, renal failure requiring dialysis, disseminated cancer, open wound/wound infection, chronic steroid use, ventilator dependence, bleeding disorders, preoperative blood transfusions, sepsis, and significant weight loss. The endpoints of our study were 30-day reported reoperation, readmission, death, and surgical complications, as well as total length of hospital stay and operative time. Complications recorded by NSQIP include surgical site infection, wound disruption, unplanned intubation, prolonged ventilator support, renal insufficiency, pneumonia, pulmonary embolism, deep vein thrombosis, urinary tract infection, myocardial infection, cardiac arrest, bleeding requiring transfusion, and sepsis. Reasons for readmission were also collected and categorized.
Statistical Analysis
Chi-square and Student t tests were performed to assess the effect of endoscope use on categorical and numerical variables respectively, and to detect significant baseline differences, if any, between endoscopic and open groups. Baseline variables (eg, age, sex, race, comorbidities), as well as primary listed diagnosis (indicating cause of lumbar stenosis, eg, idiopathic, degenerative, ligamentum flavum hypertrophy, etc), were then factored into a multivariate analysis using propensity score matching in order to assess 2-tailed P values for primary endpoints (ie, death, reoperation, readmission, complications, length of stay, and operative time). Statistical significance was set at P < .05, and analysis was performed using SPSS (IBM Corporation, Armonk, NY).
Systematic Review
A search of the PubMed/MEDLINE database was then conducted in order to compare the findings of our study with those of existing literature on the efficacy and complications of endoscopic decompression of the spine in relation to open surgical approaches. Search queries included the phases “endoscopic versus open lumbar laminectomy,” “endoscopic versus open lumbar decompression,” and “endoscopic versus open lumbar foraminotomy.” Articles comparing the 2 aforementioned techniques, regardless of study design, were included in our analysis. Systematic reviews found in the query process were also perused for citations and other mentions of individual articles comparing endoscopic and nonendoscopic techniques, which were subsequently included in our analysis as well.
Results
Demographics and Comorbidities
A total of 10 726 patients were identified, with 34 (0.32%) having undergone endoscopic decompression. There was a slight male preponderance in both endoscopic and nonendoscopic groups (55.9% and 56.4% respectively), and an average age of approximately 52 years (52.51 ± 15.01 and 51.92 ± 15.93 years, respectively). However, this data was not significantly different between the 2 groups. Furthermore, apart from the prevalence of COPD (8.82% vs 2.37%) at baseline, comorbidities were also no different between the cohorts. The full sum of demographic and comorbidity data is listed in Table 1.
Patient Characteristics at Baseline.
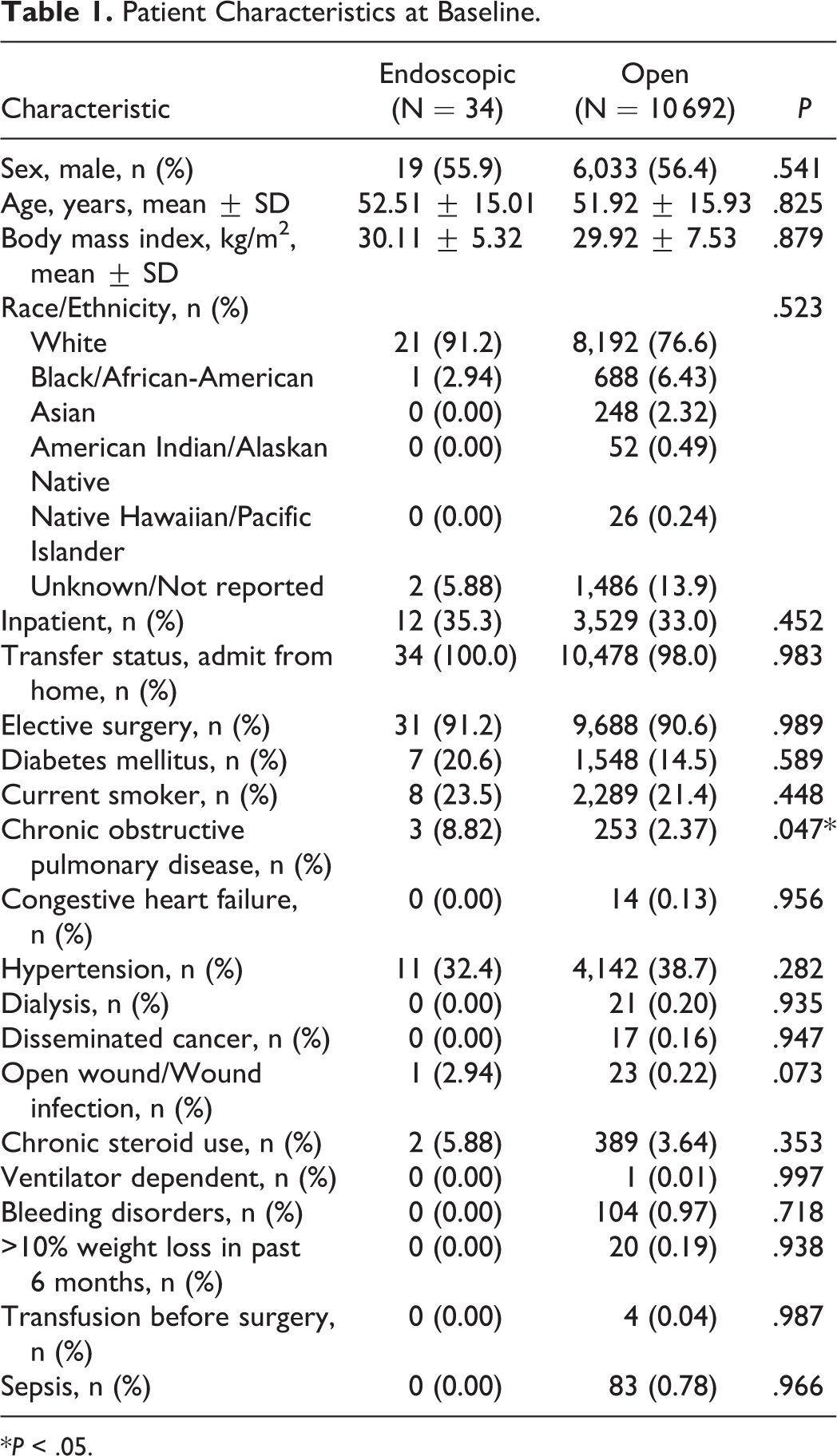
*P < .05.
Adverse Events and Operative Data
Following propensity score matching to control for preoperative patient characteristics, the incidence of perioperative and 30-day postoperative complications in the resulting equally sized endoscopic and open decompression groups is summarized in Table 2. There were no deaths, reoperations or complications reported for those patients operated upon endoscopically. However, these figures were not significantly lower than those of the open decompression group, where the mortality rate was also 0%, and only 2.94% of patients returned to the operating room (P = 1.000).
Adverse Events, 30-Day, Following Endoscopic Versus Open Lumbar Laminectomy, Propensity Score Matched.
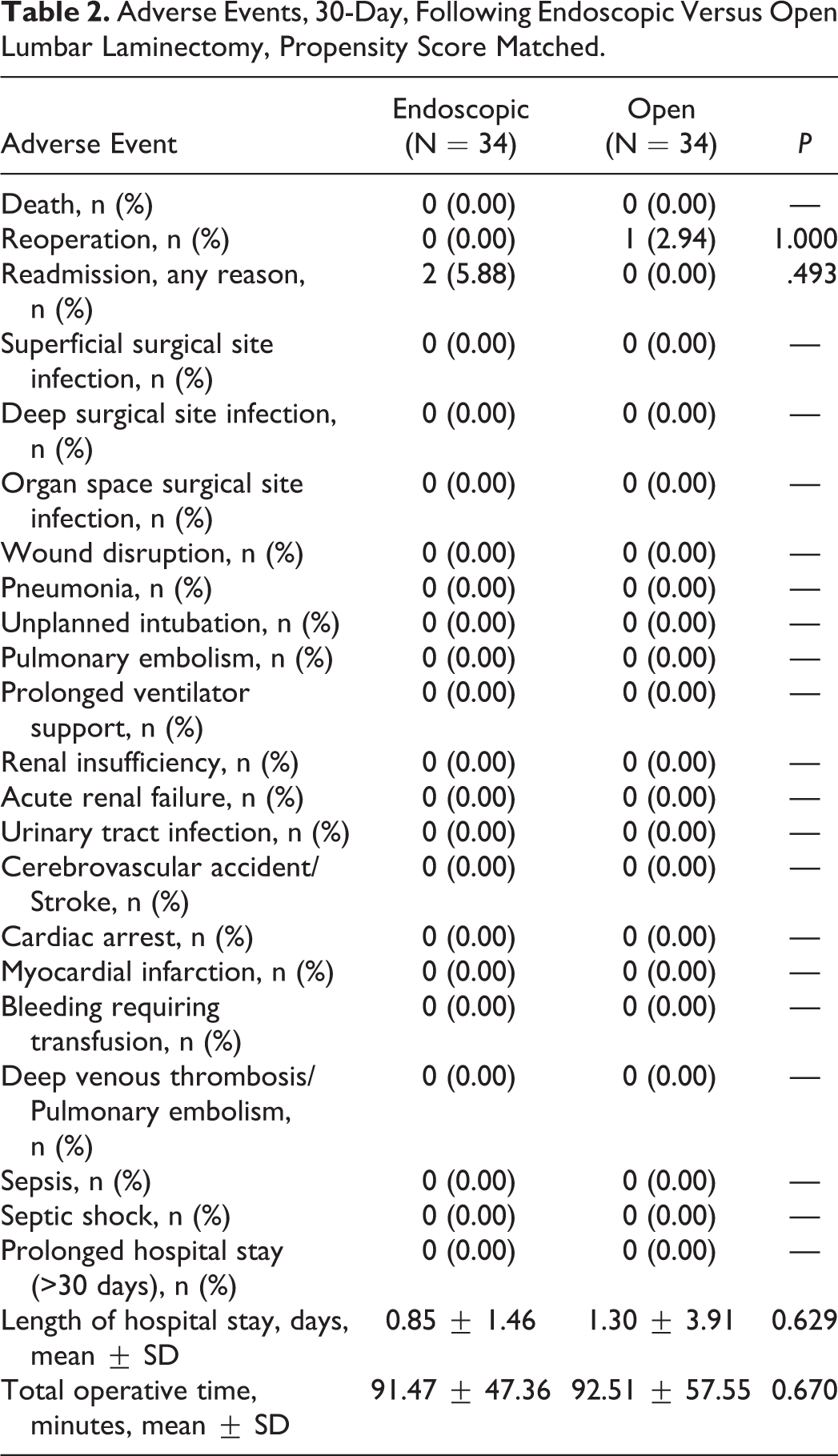
The average endoscopically guided surgery lasted 91.47 ± 47.36 minutes, whereas open operations had a mean operative time of 92.51 ± 57.55 minutes. In addition, the average length of stay among endoscopic patients was 0.85 ± 1.46 days, with no prolonged hospitalization (>30 days) reported, compared with 1.30 ± 3.91 days, with 5 (0.05%) cases of prolonged hospitalization. Two (5.88%) patients in the endoscopic group were later readmitted to the hospital, compared with 0 (0.00%) from the matched nonendoscopic group. Nonetheless, similar to other endpoints, this particular difference was also not statistically significant.
Reasons for the readmission of patients are detailed in Table 3. The only readmission in the endoscopic patient group that was related to the initial surgery was due to atelectasis. In the corresponding nonendoscopic group, the most common reasons for readmission were surgical site infection (14.2%), postprocedural pain (6.34%), postprocedural hematoma (6.04%), and venous thromboses/pulmonary emboli (5.74%).
Reasons for Readmission Within 30 Days.
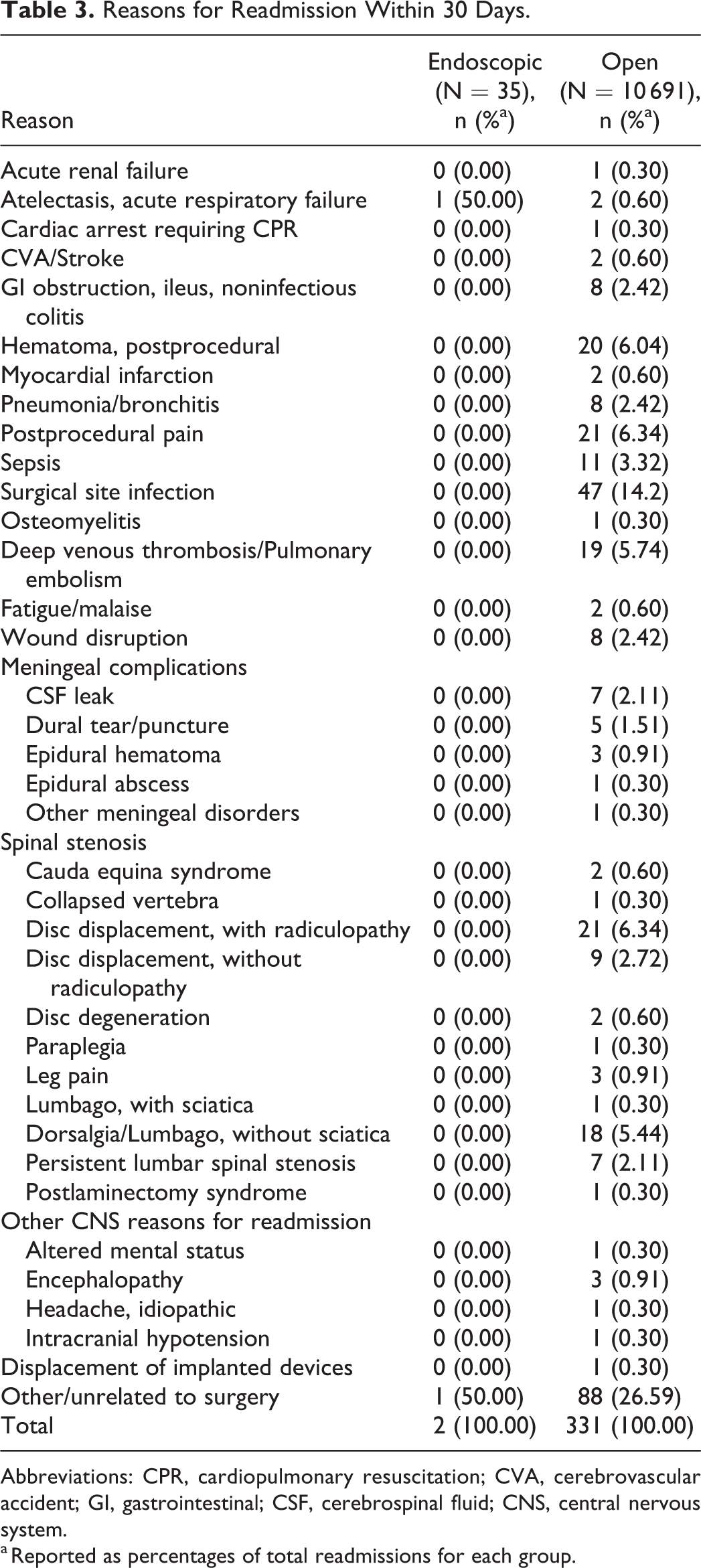
Abbreviations: CPR, cardiopulmonary resuscitation; CVA, cerebrovascular accident; GI, gastrointestinal; CSF, cerebrospinal fluid; CNS, central nervous system.
a Reported as percentages of total readmissions for each group.
Discussion
Decompression serves as a principal surgical technique for the treatment of low back pain secondary to spinal stenosis. Currently, endoscopic and open decompression involving laminectomy, and often facetectomy and foraminotomy, are utilized to alleviate pressure on the impinged cord. 3 While endoscopic decompression is less invasive and does not require dissection of much of the overlying midline muscular and soft tissue, open techniques still remain far more prevalent. In this multinational, multi-institutional retrospective analysis, comparison of these 2 approaches for single-level lumbar decompression showed no significant discrepancy in mortality, reoperations, surgical complications, operative time, length of stay and readmissions, even after controlling for preoperative risk factors. These findings concur with existing literature in some respects, while standing in stark contrast in others.
Demographics and Comorbidities
The average age of the patients in our study cohort was approximately 52 years that is, patients are younger in comparison with other studies assessing surgical decompression of lumbar stenosis, whose patients are largely in the sixth decade of life. 13 –17 The endoscopic decompression group in this study differed significantly from the open decompression group in one comorbidity—COPD—wherein patients in the former were nearly 4 times more likely to present with a past medical history. This is significant due to an established association between the presence of chronic lung disease and rates of postoperative complications among patients undergoing surgical decompression. 18 However, subsequent propensity score matching accounted for COPD history as a variable to be controlled for, among other baseline factors, and was still unable to uncover a significant difference in adverse events between the 2 groups.
Surgical Complications and Other Adverse Events
The vast majority of available literature regarding complications and adverse events associated with endoscopic decompressions are limited to single-center populations or are noncomparative studies. 6,19,20 To the best of our knowledge, only one previous study—Oichi et al (2018) 15 —has explored this topic on a multi-institutional level, utilizing a Japanese national inpatient database. However, the study’s homogeneous population limits its external validity and generalizability, especially considering the fact that many risk factors for spinal stenosis (eg, obesity) are much less prevalent in Japan. 21,22 Furthermore, certain countries (in this case, Japan) may have incorporated endoscopic techniques into their institutions earlier or later in comparison to other countries. Because of the significant learning curve associated with these newer techniques, this may, in turn, result in discrepancies in operative time and adverse events as a direct result of technique experience and relative comfort levels. 23,24 Thus, a multinational analysis such ours would theoretically be better able to control for these factors.
The study concluded that patients who underwent endoscopic decompression were less likely to experience post-operative complications and surgical site infections, and had a shorter length of stay. 15 A meta-analysis of existing single-center studies on the topic concurred with Oichi et al 15 in its result of shorter hospital stays, while supporting the results of our study in finding similar rates of reoperation, wound infections and other surgical complications. 6 It also noted that endoscope utilization did not reduce operative time, but actually increased it, which differs with the conclusion of our study that the 2 techniques had a similar operative time.
Regarding surgical site infections and other surgical complications (eg, bleeding requiring transfusion), the lack of discrepancy between endoscopic and open groups in this regard may be due to several distinct factors. First, with single-level decompressions, the difference between the size of an incision with an open surgical approach and the sum of the smaller individual incisions required for endoscopic placement may not be significant. In addition, the introduction of microscopes and percutaneous guidance technologies into the neurosurgical suite may further reduce the size of incisions in so-called “mini-open” procedures, which may be included within the open decompression patient group. It follows that microscopes and other nonendoscopic guidance may be present for the entire duration of an “open” procedure, or merely a specific portion of it. Although we are unable to distinguish between these less invasive subsets of surgeries with more traditional approaches using CPT codes and other fields availed by the NSQIP database, it is certain that all procedures coded as being endoscopically guided in our cohort are indeed entirely minimally invasive in nature. Thus, the results of this study are able to speak to the merits, or lack thereof, of utilizing endoscopes as a form of assisted visualization, and the risk profile in doing so from the standpoint of patient mortality and adverse events.
Review of the Literature
Our systematic review of the available literature yielded 16 unique articles published between 2006 and 2018, which included 4 retrospective analyzes, 4 systematic reviews and meta-analyzes, 3 retrospective cohorts, 1 prospective observational study/cohort, 1 prospective randomized study, 1 literature review, 1 meta-analysis, and 1 retrospective case series.
The conclusions of the included studies seemed to converge on a consensus regarding a number of advantages associated with use of an endoscopic approach for decompression of lumbar spinal stenosis. Two publications concluded that use of endoscopy was associated with a shorter time to return to work and functional recovery over open decompression technique (weighted mean difference [WMD] = −15.45; 1.1 ± 1.1 weeks vs 5.4 ± 2.1 weeks; P < .05) for patients. 23,24 Isolated noteworthy findings also included superior preservation of paraspinal muscle cross sectional area (increased 9.9% ± 14.4% vs decreased 5.4% ± 10.6%) and decreased postoperative delirium (1.1% vs 2.3%, P = .010), infection rates (0.5% vs 1.6%, P = .004), slip progression, and need of supportive services following discharge (absolute difference 19%, P = .063). 15,16,25,26 Despite the reported benefits of endoscopic decompression, however, percutaneous endoscopic lumbar discectomy has also been found to be associated with higher rates of incomplete decompression (odds ratio 3.08, P < .05). 23
Nevertheless, there were several controversies found in existing literature relating to endoscopic versus nonendoscopic approaches. Two studies claimed that endoscopic intervention was associated with decreased blood loss (WMD = −31.86, P < .001; 139.8 mL vs 62.0 mL, P = .013), while another concluded that such a difference in blood loss was actually negligible with no clinical significance. 6,16,27 One study discussed how endoscopic interventions significantly lower complication rates (1.0% vs 2.8%, P < .001) compared to open approaches. 15 Meanwhile, three articles discussed no significant difference between both techniques. 23,28,29 Two studies reported shorter operative times (WMD = −12.83, P = .04; 48.66 ± 6.45 minutes vs 53.71 ± 8.49 minutes, P = .009) for endoscopic procedures, 27,29 contrary to what another study discussed in there being no significant difference in operation duration. 23 Several articles found endoscopic methods to be superior with regard to the attenuation of pain assessed by a visual analogue scale score, functional outcomes assessed by an Oswestry Disability Index score, and incidence of reoperation. 23,28,29
A summary of the literature included in our review, their respective study designs, and conclusions therein, are outlined in Table 4. Taken together, the available literature surrounding this topic seems to suggest that endoscopy may be associated with lower rates of certain short-term postoperative complications, but at the potential cost of increased revision and reoperation rates. Thus, the results of our study seem to stand in contrast to this general consensus, yet these findings should be considered in the context of potential limitations to our methodology, as outlined below.
Summary of Literature Review: Endoscopic Versus Nonendoscopic Decompression.
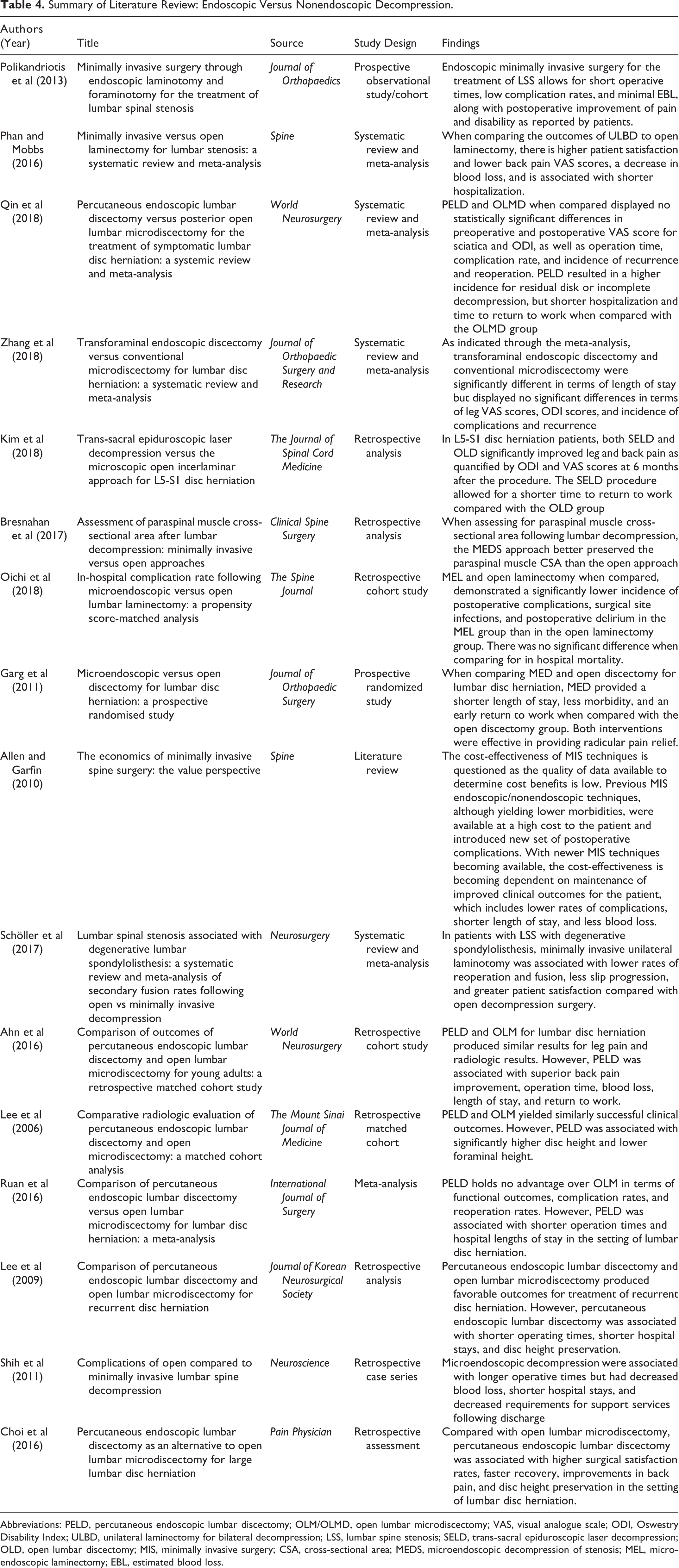
Abbreviations: PELD, percutaneous endoscopic lumbar discectomy; OLM/OLMD, open lumbar microdiscectomy; VAS, visual analogue scale; ODI, Oswestry Disability Index; ULBD, unilateral laminectomy for bilateral decompression; LSS, lumbar spine stenosis; SELD, trans-sacral epiduroscopic laser decompression; OLD, open lumbar discectomy; MIS, minimally invasive surgery; CSA, cross-sectional area; MEDS, microendoscopic decompression of stenosis; MEL, microendoscopic laminectomy; EBL, estimated blood loss.
Limitations
There are several limitations to this study. First and foremost is the small number of endoscopic patients (N = 34), which affects statistical power and type I error rates. On a larger scale, the small group size may indicate a lack of comfort or training with endoscopes, a relatively newer technology with a significant learning curve, as discussed in the previous subsection. 30,31 Because selection of surgical technique is largely up to the discretion of individual surgeons, the low rate of adverse events seen in this group may be the result of self-selection on the part of practitioners more comfortable with endoscopic utilization. Other study limitations relate to the NSQIP database itself, in that it does not include functional outcomes, particularly from a neurological standpoint (e.g. Oswestry Disability Index or visual analogue scale scores), and that it does not track adverse events beyond a 30-day window, which impacts our ability to assess long-term patient outcomes. Thus, we would caution against overextrapolating the results of this study to render a definitive judgement on the relative efficacy of endoscopic versus nonendoscopic lumbar laminectomy techniques. Rather, our findings provide a much-needed “snapshot” in time of the rates of mortality and complications associated with these procedures, particularly because of the fact that several of our results contrasted directly with those found in existing literature. Furthermore, our results and subsequent conclusions reflect the need for future, prospective studies on this topic.
Conclusion
Endoscopic guidance in decompression of the lumbar spine does not improve or exacerbate the incidence of mortality, reoperation, readmission, or other adverse events, not does it affect operative time and total length of hospital stay. Further studies within a higher level of evidence, particularly those of a prospective nature, are needed in order to reconcile differences that exist within this study and among the existing literature, and to more accurately assess the impact of endoscopic decompression techniques on patient outcomes and complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.