
Abstract
Study Design
A retrospective radiologic study.
Objectives
To identify age-associated changes in T1 slope (T1S) and C7 slope (C7S), as well as the difference between T1S and C7S (△, which was defined as T1S minus C7S) and to explore the cervical morphology that C7S can be the most accurate alternative for the invisible T1S.
Methods
625 asymptomatic Chinese volunteers received cervical lateral radiographs from August 2021 to May 2022. Occipito-C2 angle (O-C2), C2-7 angle (C2-7), cranial arch, caudal arch, C7S, and T1S were examined. Thereafter, the △ was established. The correlations among T1S, C7S, △ and other cervical sagittal parameters, and between age and other cervical sagittal parameters were evaluated with the Pearson correlation coefficient analysis. Then, analysis of variance (ANOVA) was conducted to compare variations in cervical sagittal parameters among volunteers aged 40 to 59 years, 60 to 64 years, 65 to 69 years, 70 to 74 years, and ≥75 years of age, and among volunteers with 1 lordotic morphology, 2 lordotic morphology, straight morphology, kyphotic morphology, 1 sigmoid morphology, and 2 sigmoid morphology. Linear regression modeling of the correlation between C7S and T1S in various cervical alignment patterns was then established.
Results
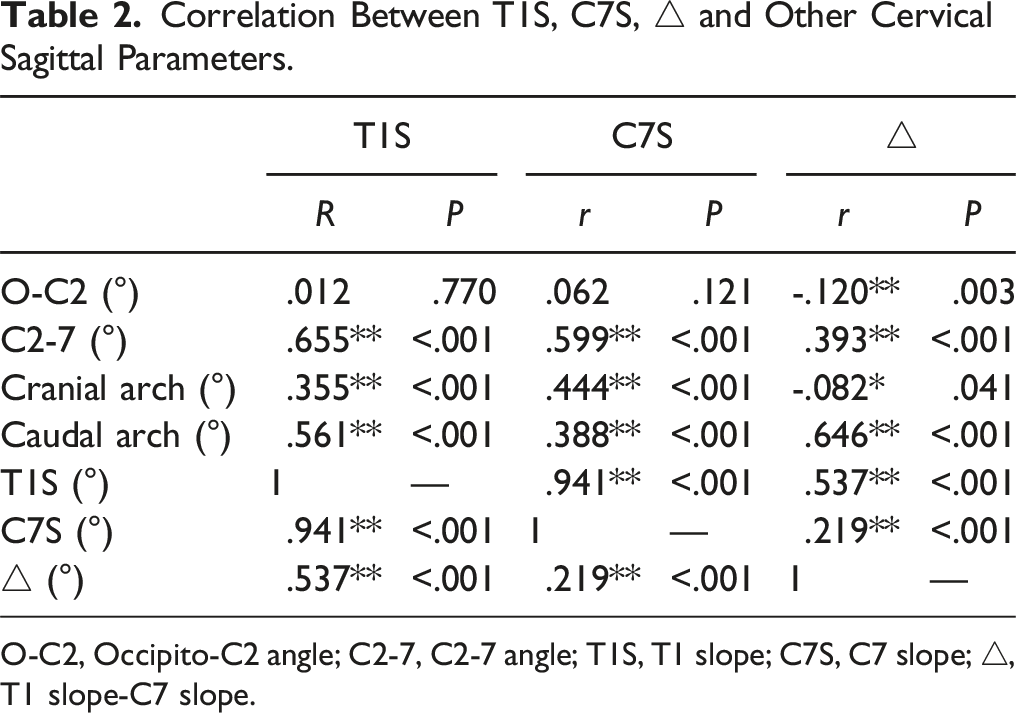
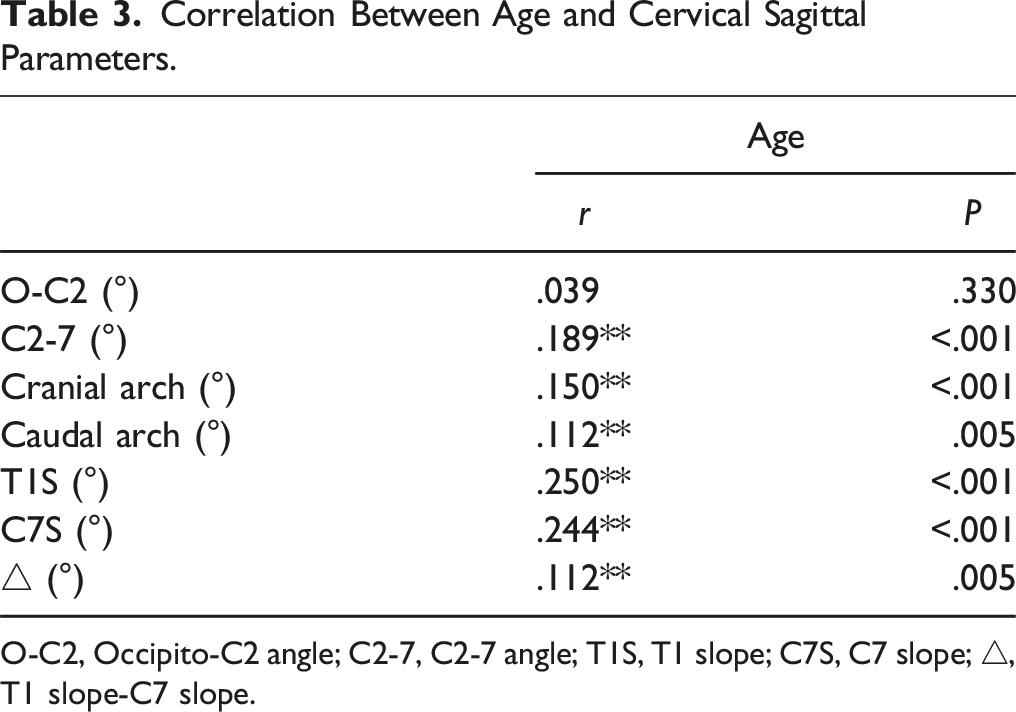
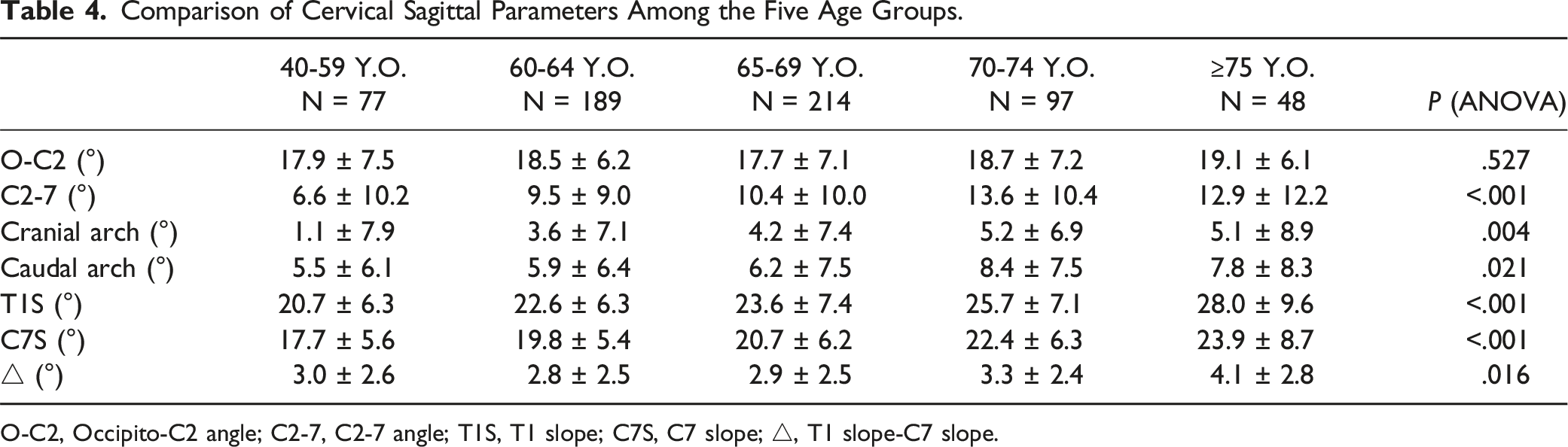
△ had the strongest correlation with caudal arch (r = .646), and weakest correlation with cranial arch (r = -.082). Age was significantly correlated with T1S (r = .250), C7S (r = .244), and △ (r = .112). Among them, △ was stable until 74 years after which it showed an elevation from 3.3° in the group 70-74 years to 4.1° in the group over 75 years. Moreover, there was marked variation between T1S and C7S at 1 lordotic, 2 lordotic, straight and 2 sigmoid alignment patterns, but no difference was seen between T1S and C7S at kyphotic and 1 sigmoid alignment patterns.
Conclusions
There was a progressive increase in T1S, C7S, and △ with age. Linear regression equations for accurate prediction of T1S were developed based on the C7S in 1 lordotic, 2 lordotic, straight and 2 sigmoid alignment patterns. C7S may be a reliable proxy for T1S in kyphotic and 1 sigmoid alignment patterns.
Introduction
T1 slope (T1S) was the angle between the horizontal line and the superior endplate of the T1 vertebra. As the foundation of the head and cervical spine, T1S can not only reflect the regional balance of cervical spine, but also reflect the association between the whole spine and the cervical spine. 1 Additionally, T1S can predict the outcome of cervical surgery2-8 and is closely associated with the degenerative changes of sagittal alignment.9,10 Despite its significance, accurately quantifying T1S on radiographs is often limited due to poor visibility, resulting from high shoulder positioning or obesity, 11 with visibility of T1S ranging from 11% to 30% in plain lateral radiographs. 12 Therefore, several studies attempt to replace lateral radiographs with computed tomography (CT) or magnetic resonance imaging (MRI).13,14 However, the economic cost and the influence of supine posture on cervical alignment limit the generalizability and accuracy of MRI and CT in evaluating T1S. 15
Findings from recent investigations showed that measuring C7 slope (C7S) instead of blurry T1S,16-19 but it does not imply that C7S is equivalent to T1S. Despite C7S shows the potential to be a good substitute marker, the difference between C7S and true T1S (△) can lead to substantial errors when formulating standards for cervical deformity correction. Furthermore, both C7S and T1S show an age-dependent increase.20-23 It remains uncertain whether △ also varies with age. The potential association between △ and age presents a challenge to the development of an equation for predicting T1S based on C7S.
Rather than focusing on age, observing substitutability of C7S for T1S in line with various cervical morphologies can offer more direct insights. Cervical morphologies exhibit significant alterations in asymptomatic individuals, eg, lordosis, straight, sigmoid, and kyphosis. 24 Kyphosis, previously deemed pathological, has been found in asymptomatic subjects presenting regional or global kyphosis. 25 Moreover, the cervical spine with sigmoid alignment is gradually excavated and represents a certain proportion in the normal population.26,27 Despite these findings, it is still unknown whether C7S can accurately replace T1S in various cervical morphologies.
To fill the academic gap, we aimed at assessing age-associated changes in T1S and C7S, the difference between T1S and C7S based on different age subgroups and to determine in which cervical morphology C7S can best accurately replace T1S in a large radiographic data for 625 healthy volunteers.
Materials and Methods
The institutional review board of our institution (approval number: 2018014) permitted this study. A total of 1250 Chinese volunteers over 18 years were recruited in the Beijing town health screening program between August 2021 and May 2022. All the volunteers were fully informed about the purposes, methods, and risks of the study and then signed the written informed consents before the enrollment. The inclusion criteria were volunteers with free of apparent symptoms of neck pain (Neck Disability Index, NDI <10) in previous 6 months.
28
The exclusion criteria were volunteers with histories of brain or cervical surgery and sensory or motor disorders-related symptoms (including numbness, motor weakness, clumsiness, as well as gait disturbance). Pregnant women and volunteers with lateral cervical radiographs without clearly visible superior C7 endplate, inferior C7 endplate, and superior T1 endplate were also excluded. Finally, 625 volunteers (150 males and 475 females) were recruited in the study. The detailed flowchart is shown in Figure 1. Volunteers selection flowchart.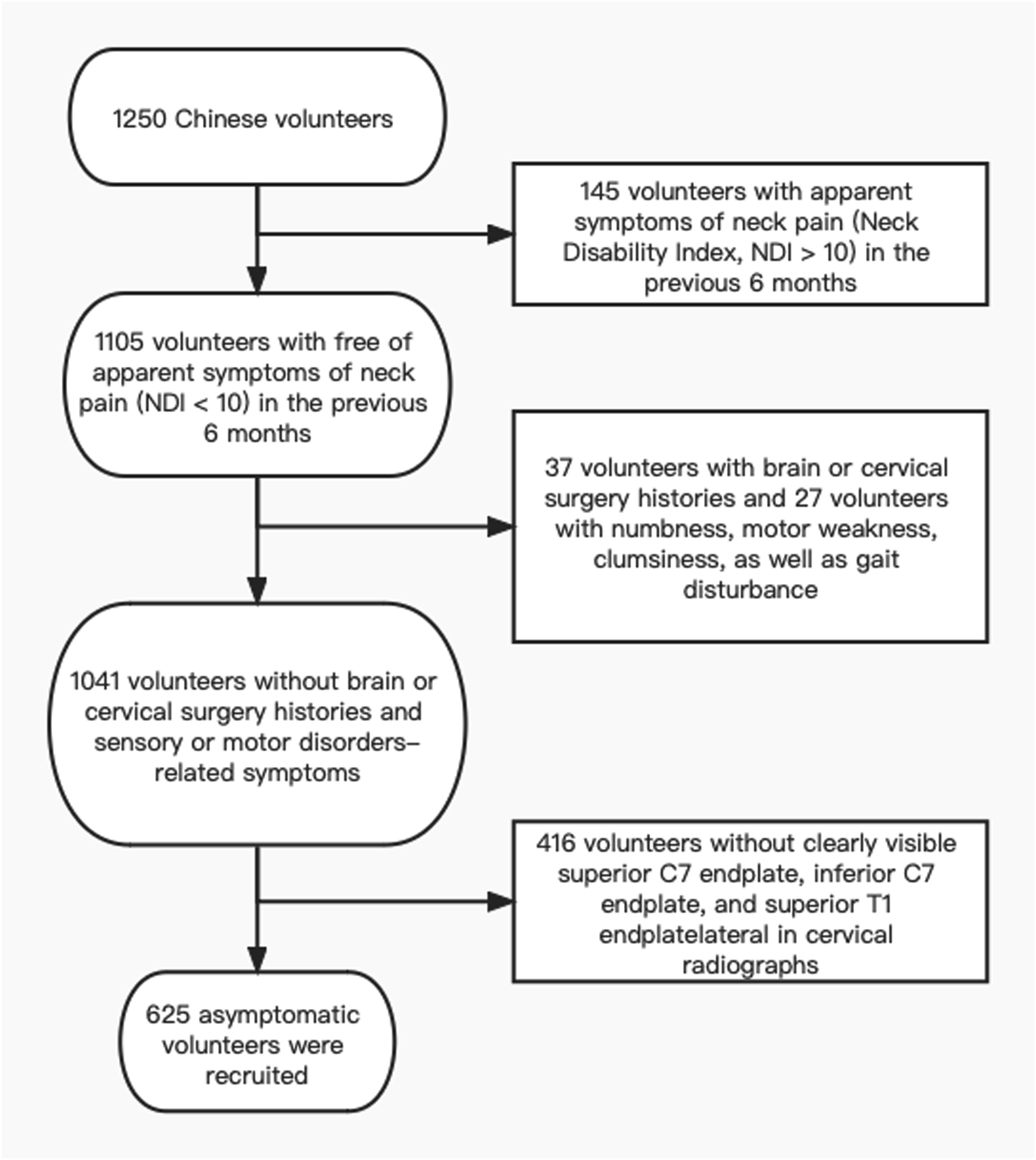
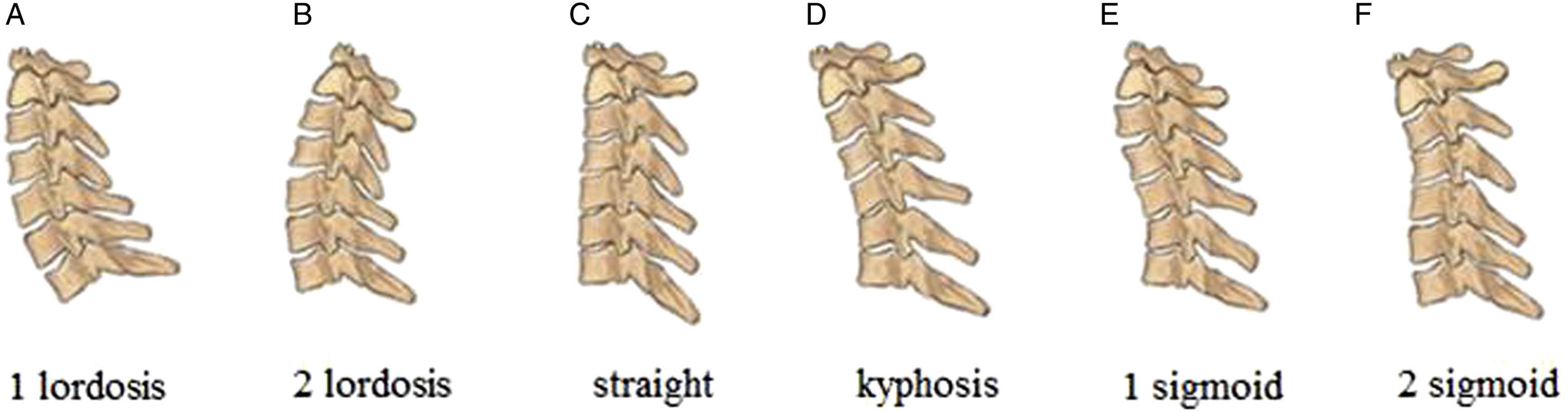
Under the guidance of a professional radiologist, all volunteers underwent standard lateral cervical spine radiography while in neutral relaxed positions with horizontal gaze. The film-tube distance was 180 cm. Lateral X-ray images were acquired while volunteers were standing and in upright positions with their fingers resting on their clavicles and shoulders at a 45° forward position to alleviate the measurement errors in cervical alignment associated with the head movement. Cervical morphologies were grouped into lordotic, straight, kyphotic and sigmoid alignment patterns.24,27,29 We subdivided the lower cervical alignment into cranial and caudal arches on the basis of cervical apex (or inflexion point in sigmoid alignment pattern) and further supplemented the cervical morphologies. Cervical 1 lordotic alignment was artificially defined as cranial arch that is smaller relative to the caudal arch and the 2 lordotic alignment was artificially defined as cranial arch that is larger than caudal arch. Lordotic cranial arch with kyphotic caudal arch was defined as a 1 sigmoid alignment, and kyphotic cranial arch with lordotic caudal arch was defined as a 2 sigmoid alignment (Figure 2A-F).
30
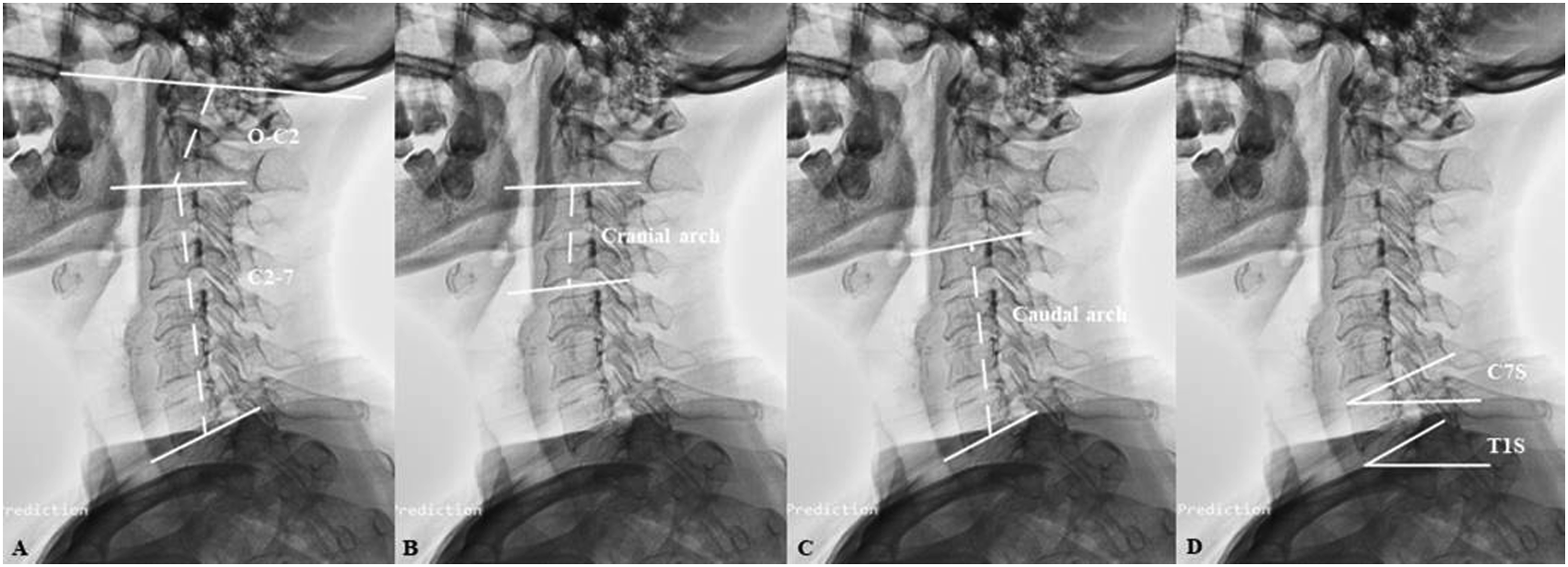
Cervical sagittal parameters were evaluated: • Occipito-C2 angle (O-C2): the angle between the McGregor line and inferior aspect of the axis; • C2-7 angle (C2-7): the angle between the inferior aspect of the axis and vertebral body C7; • Cranial arch: the angle between the inferior endplate of the axis and cervical apex (inflexion point in sigmoid alignment); • Caudal arch: the angle between the inferior endplate of vertebral body C7 and the superior endplate of cervical apex (inflexion point in sigmoid alignment); • T1S: the angle between the horizontal line and superior endplate of vertebral body T1; • C7S: the angle between the horizontal line and superior endplate of vertebral body C7; • △: the value of T1S minus C7S (Figure 3A-D). Six morphologic variations of cervical alignments (A)-(F): 1 lordotic pattern (A), 2 lordotic pattern (B), straight pattern (C), kyphotic pattern (D), 1 sigmoid pattern (E), and 2 sigmoid pattern (F). Radiographic measurements of cervical sagittal alignment: O-C2, Occipito-C2 angle; C2-7, C2-7 angle (A), Cranial arch (B), Caudal arch (C), and C7S, C7 slope, T1S, T1 slope (D).
Negative value was defined as kyphotic angle whereas a positive value was defined as lordotic angle. The inter- and intra-observer variations of cervical sagittal parameters were determined via reliability statistics by intra-class correlation coefficient (ICC) from values of angles of 625 volunteers as measured by two independent observers. The mean intra- and inter-observer ICCs were .93 and .92 in O-C2 angles, .91 and .95 in C2-7 angles, .86 and .89 in cranial arch, .88 and .90 in caudal arch, .94 and .95 in T1S, .92 and .94 in C7S, respectively.
Data were presented as mean ± standard deviation (SD). The SPSS software 20.0 (SPSS Inc., Chicago, IL) was used for analyses. Pearson correlation analysis was used to determine the associations between T1S, C7S, △ and other cervical sagittal parameters. The relationship between cervical sagittal parameters and age was also evaluated by Pearson correlation coefficient. Based on age, subjects were divided into 5 groups: 40-59-year-old (Y.O.) (N = 77), 60-64 Y.O. (N = 189), 65-69 Y.O. (N = 214), 70-74 Y.O. (N = 97) and ≥75 Y.O. (N = 48)). Subjects were then classified into 6 groups on the basis of cervical morphology: 1 lordotic alignment (N = 244), 2 lordotic alignment (N = 124), straight alignment (N = 134), kyphotic alignment (N = 37), 1 sigmoid alignment (N = 28), and 2 sigmoid alignment (N = 58). Differences in cervical sagittal parameters among the 5 age groups and 6 cervical morphologies were determined by one-way analysis of variance (ANOVA). Afterwards, Tukey’s or Dunnett’s post hoc test was adopted, aiming at further comparing the mean differences among multiple groups based on age and morphology. Linear regression modeling of the correlation in various cervical alignment patterns were then performed by R statistical computing software (www.R-project.org). The threshold for significance was P < .05.
Results
Cervical Sagittal Parameters in Healthy Volunteers.
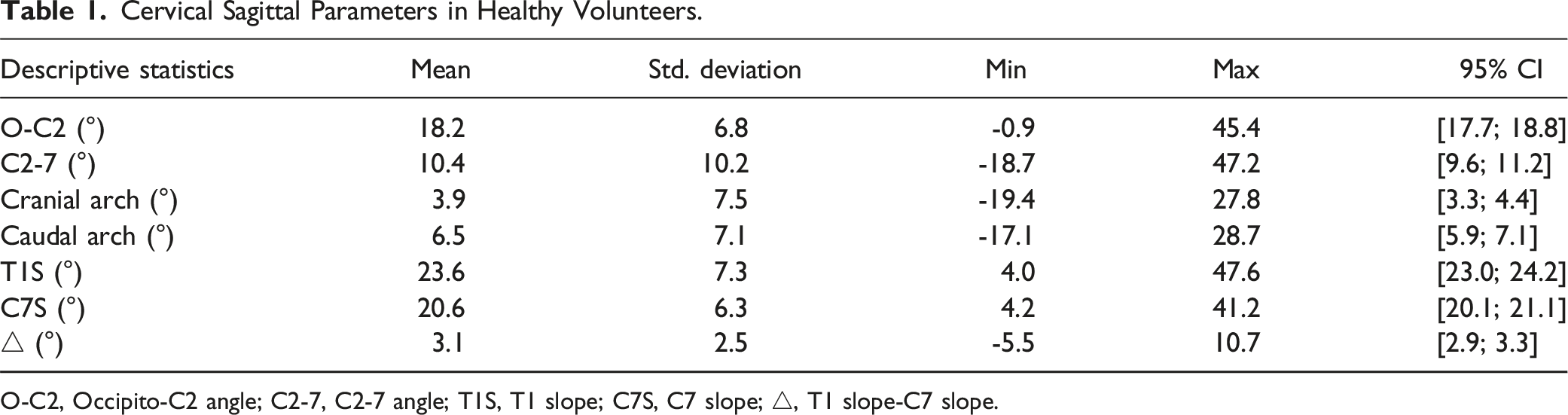
O-C2, Occipito-C2 angle; C2-7, C2-7 angle; T1S, T1 slope; C7S, C7 slope; △, T1 slope-C7 slope.
Correlation Between T1S, C7S, △ and Other Cervical Sagittal Parameters.
O-C2, Occipito-C2 angle; C2-7, C2-7 angle; T1S, T1 slope; C7S, C7 slope; △, T1 slope-C7 slope.
Correlation Between Age and Cervical Sagittal Parameters.
O-C2, Occipito-C2 angle; C2-7, C2-7 angle; T1S, T1 slope; C7S, C7 slope; △, T1 slope-C7 slope.
Comparison of Cervical Sagittal Parameters Among the Five Age Groups.
O-C2, Occipito-C2 angle; C2-7, C2-7 angle; T1S, T1 slope; C7S, C7 slope; △, T1 slope-C7 slope.
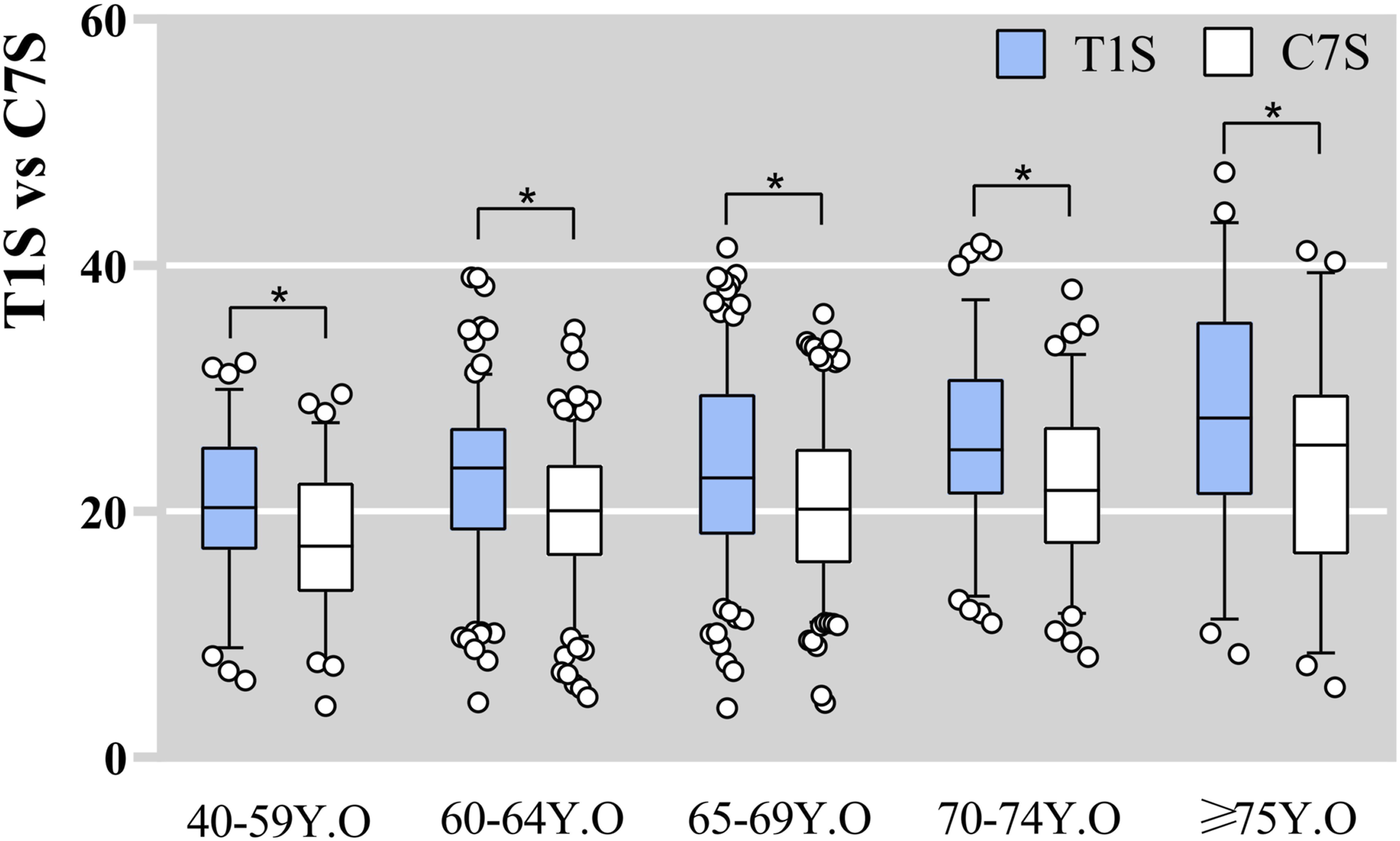
Box-plot distribution of T1S and C7S based on age. *P < .05.
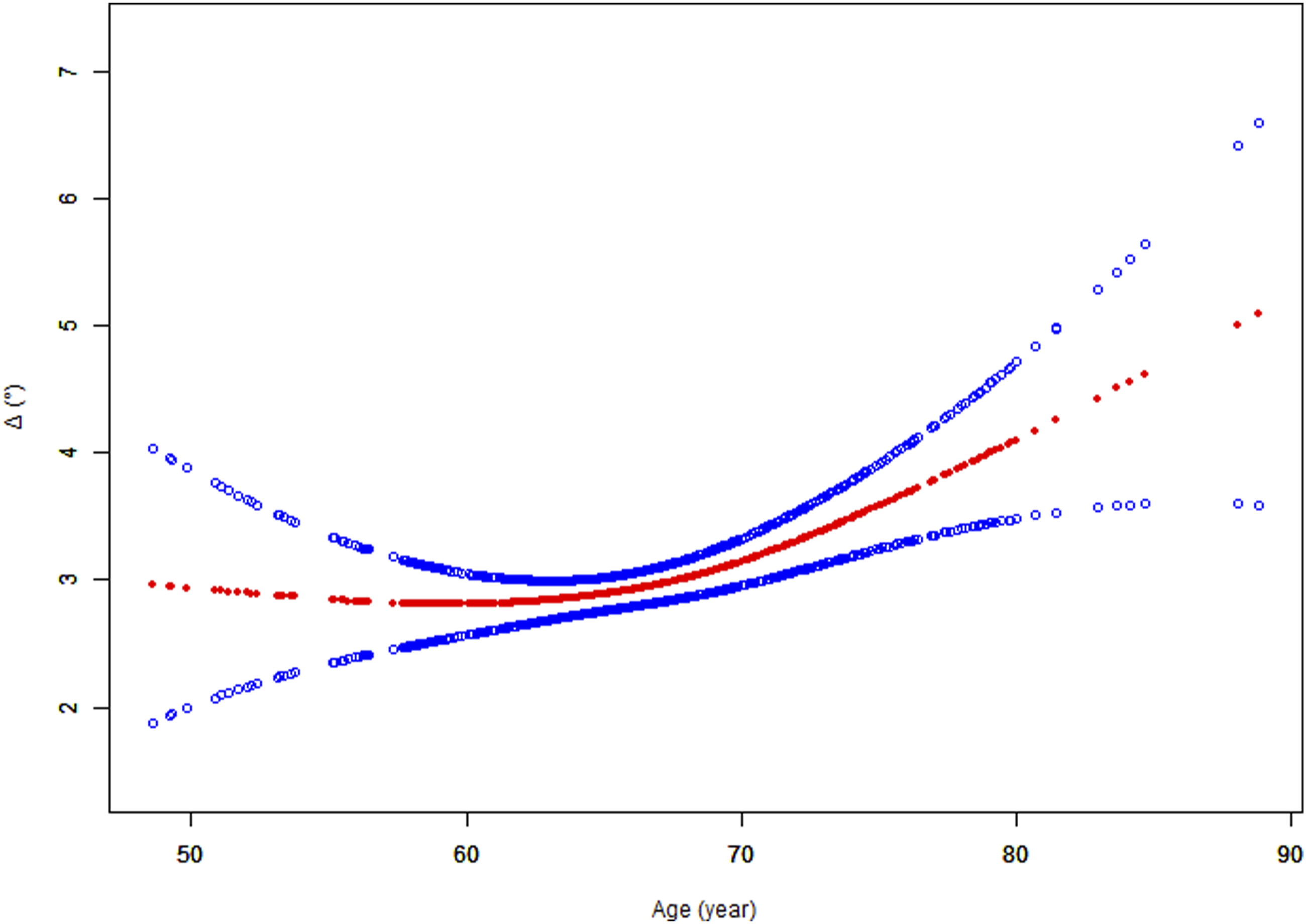
The association between age and △. The solid red line denotes the smooth curve fit between variables. Blue bands denote the 95% confidence interval (CI) from the fit.
Comparison of Cervical Sagittal Parameters Among the Six Cervical Morphology Groups.
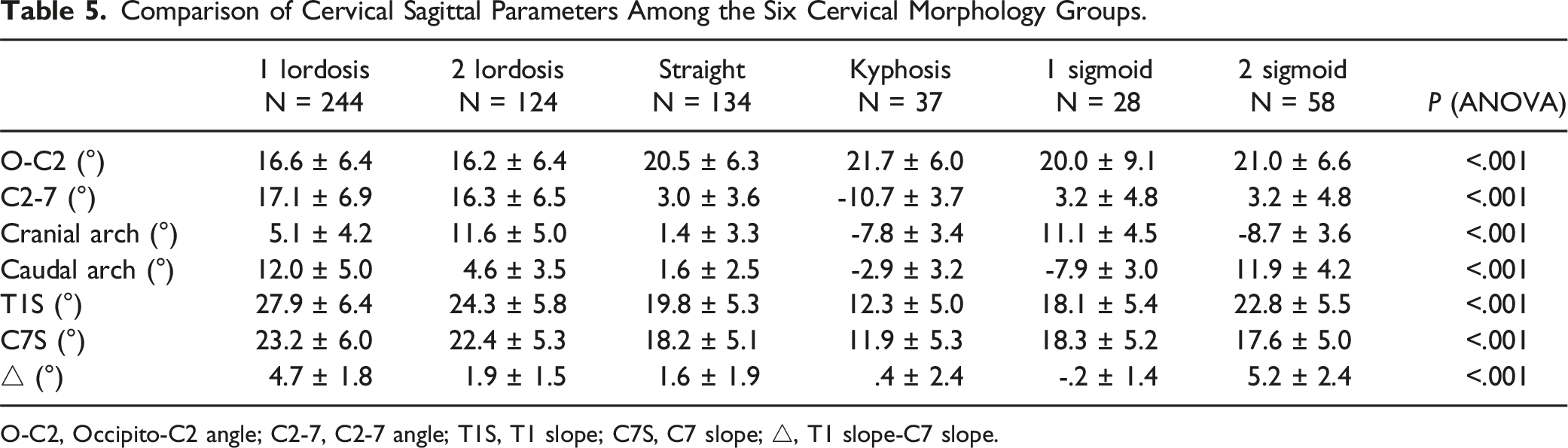
O-C2, Occipito-C2 angle; C2-7, C2-7 angle; T1S, T1 slope; C7S, C7 slope; △, T1 slope-C7 slope.
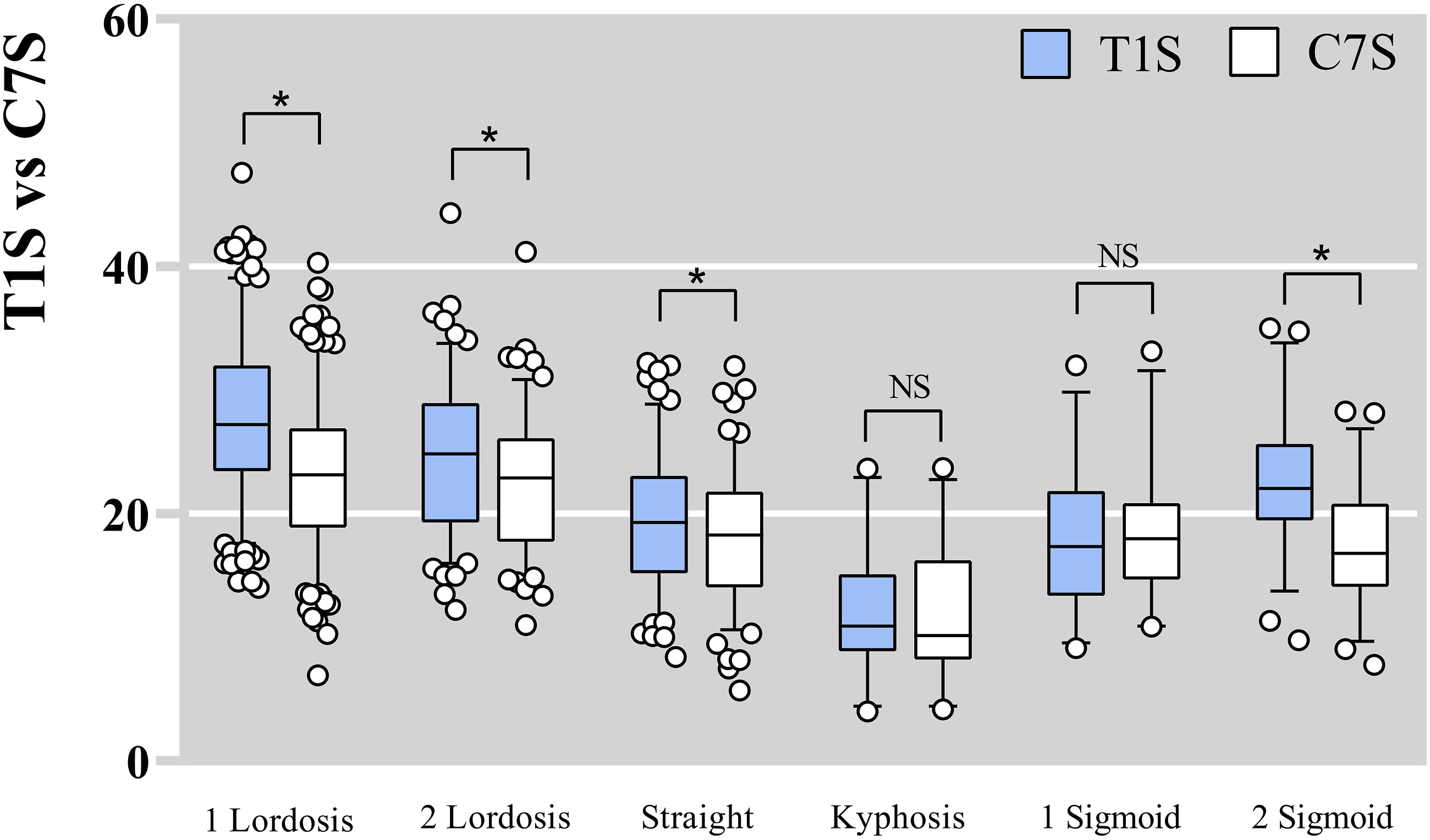
Box-plot distribution of T1S and C7S based on cervical alignment patterns. *P < .05.
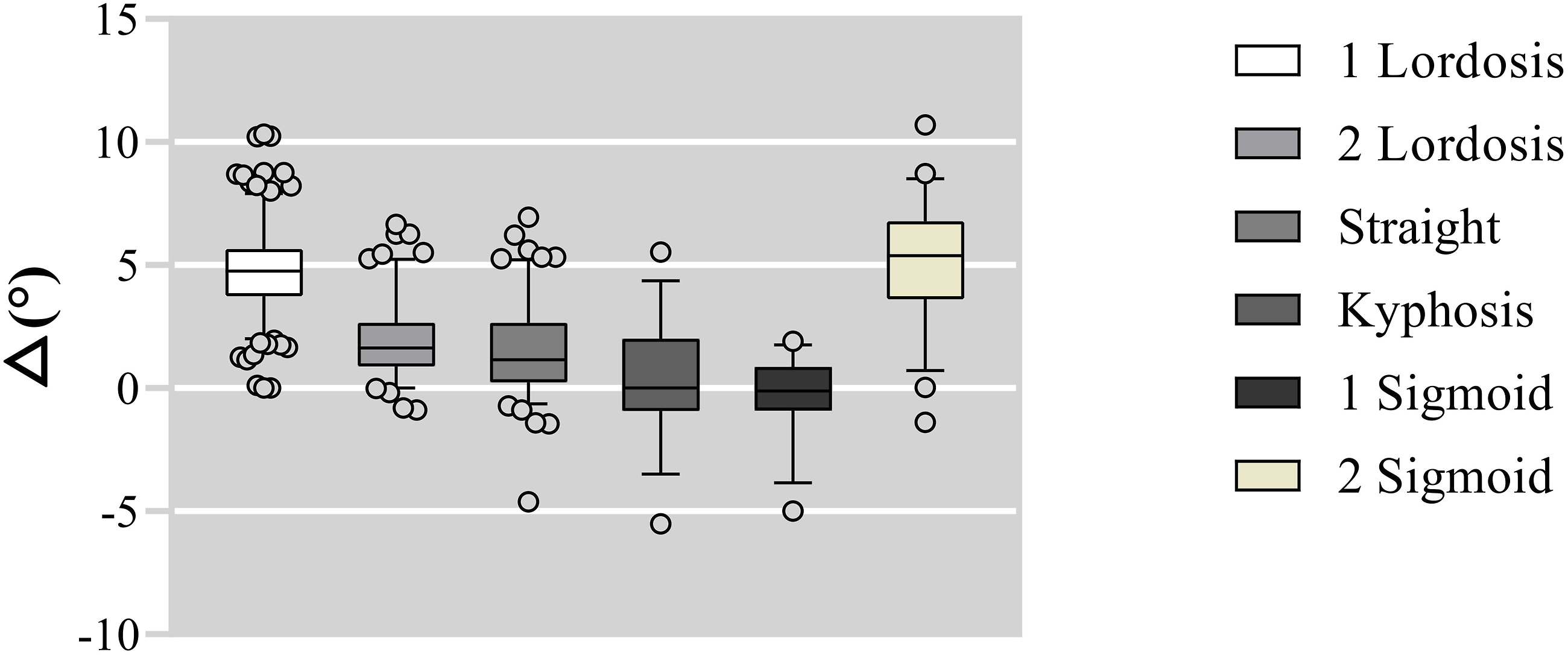
Box-plot distribution of △based on cervical alignment patterns. *P < .05.
Linear regression modeling of the correlation between C7S and T1S in 1 lordotic alignment disclosed that T1S = 4.10 + (1.02 × C7S), R2 = .92 (Figure 8A). Correlation between T1S and C7S based on linear regression equation in 1 lordotic pattern (A), in 2 lordotic pattern (B), straight pattern (C), and 2 sigmoid pattern (D). Linear regression represented (black line) with 95% CI limits (dark gray) and 95% prediction limits (light gray).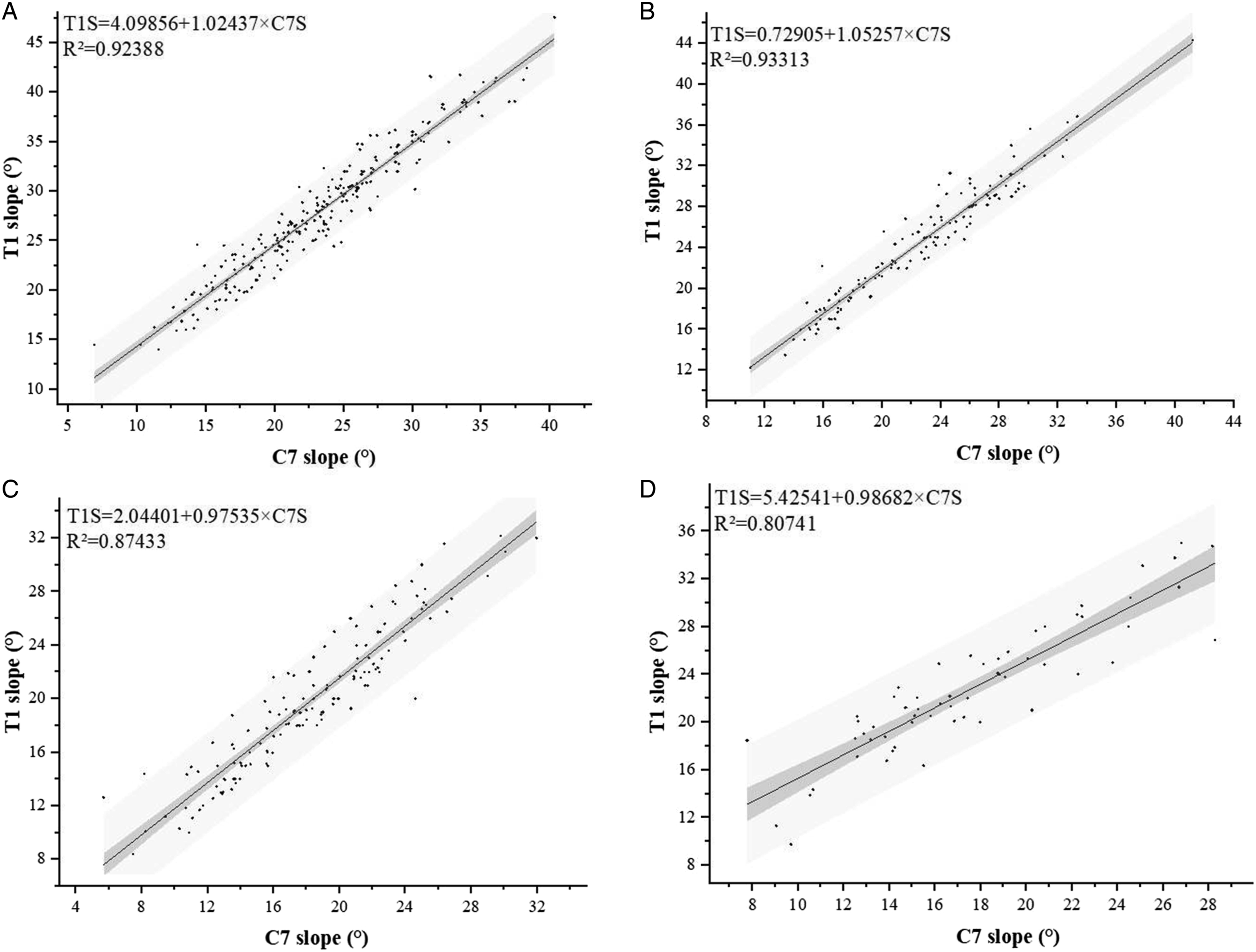
Linear regression modeling of the correlation between C7S and T1S in 2 lordotic alignment disclosed that T1S = .73 + (1.05 × C7S), R2 = .93 (Figure 8B).
Linear regression modeling of the correlation between C7S and T1S in straight alignment disclosed that T1S = 2.04 + (.98 × C7S), R2 = .87 (Figure 8C).
Linear regression modeling of the correlation between C7S and T1S in 2 sigmoid alignment disclosed that T1S = 5.43 + (.99 × C7S), R2 = .81 (Figure 8D).
Discussion
In this study, we sub-grouped healthy volunteers by age and cervical morphology, measured sagittal alignments of cervical spine and found that T1S, C7S, and △ exhibited a significant and progressive increase during aging. Furthermore, T1S and C7S showed marked differences at 1 lordotic, 2 lordotic, straight and 2 sigmoid alignment patterns, but no difference between T1S and C7S at kyphotic and 1 sigmoid alignment patterns. This showed that C7S can be measured and used to directly substitute for an invisible T1S in the above two cervical alignment patterns. Linear regression model that could predict T1S accurately based on the C7S in the remaining four cervical alignment patterns were developed, and it revealed marked differences between T1S and C7S. The strengths of the current study is that we can intuitively judge the substitutability of C7S for T1S according to the cervical alignment patterns, without considering the age-related changes in △.
The Clinical Significance and Evaluation Challenges of T1S
Since Knott first reported T1S in 2010, 1 several publications focused on T1S have been reported. In terms of global sagittal balance, T1S showed a significant positive correlation with cervical lordosis (CL) and thoracic kyphosis (TK).31-33 Yang et al 34 established the following formula through examining the global spinal alignment in healthy volunteers: T1S = .6 × maxTK −.2 × maxLumbar lordosis (LL) + 8, which implies that T1S not only predicts the amount of CL required to maintain the regional balance of the center of head gravity, but also varies with the overall spinal alignment determined by TK and LL. In terms of clinical guidance, Zhang et al 8 confirmed that preoperatively elevated T1S was associated with the loss of CL after laminoplasty. Oe et al 6 found that preoperative T1S >40° was the correction failure risk factor for patients with adult spinal deformity. In addition, Park et al 7 concluded that preoperative low T1S can predict adjacent segment disease development after anterior cervical surgery. In terms of symptom evaluation, Oe et al 35 found that T1S >40° in asymptomatic volunteers had negative effects on EuroQol 5 Dimension (EQ-5D) score, while Iyer et al 36 confirmed that preoperative T1S is an independent predictor of preoperative neck disability index (NDI). However, current result confirmed that T1S was invisible on the lateral cervical scans, since anatomical structures such as acromioclavicular joint or thick thoracic trunks. Although X-ray measurement of T1S can be substituted by CT and MRI, images obtained in the supine position do not represent physiologic alignment, which make the measurement results not very accurate.15,37
The Potential of C7S as a Substitute for T1S
Considering that T1 vertebral body is not always visible clearly on cervical radiography, a large number of studies attempt to identify parameters which can substitute T1 upper endplate. Wang et al38-41 reported a strong correlation between spino-cranial angle (SCA) and T1S and verified the value of SCA in evaluating cervical sagittal balance. In addition, C7S as the adjacent cervical sagittal parameter of T1S has been widely concerned in recent years. Nunez-Pereira et al 17 found that the C7S showed the strongest association with T1S and was significantly correlated with CL. Current results are in line with this finding, demonstrating that both C7S and T1S showed a strong correlation with C2-7, cranial arch, and caudal arch. Collectively, we concluded that C7S may be a robust parameter for evaluating cervical sagittal balance with the potential to substitute T1S. To obtain accurate measurement of T1S, researchers have created linear regression models to predict T1S based on the C7S.12,14,16-19 Tamai et al 14 demonstrated a close correlation between the upper C7S and T1S (C7S = .8821 × T1S − .5449, R2 = .8183), and between lower C7S and T1S (C7S = .9335 × T1S – 1.6833, R2 = .84) by linear regression analysis in cervical patients. Ye et al 19 also confirmed linear regression equation between the upper C7S and T1S (T1S = .87 × C7S + 7.21, R2 = .82), and between lower C7S and T1S (T1S = .87 × C7S + 7.60, R2 = .81) in asymptomatic healthy subjects. However, given that C7S and T1S increased with age,20-23 it can cause marked errors while using the formula to predict T1S via C7S, if age affects the difference between them.
Age-Related Differences Between C7S and T1S and Predictive Modeling Based on Cervical Alignment Patterns
Recently, Inoue et al 42 showed that the normal value and extension ROM of C7S and T1S markedly increased with age in asymptomatic individuals. Our results are congruent with these findings. Further examination demonstrated that T1S was markedly larger than C7S across all age-groups, and △ still exhibited significant differences across all ages, especially above 75 years old. This implied that it is inappropriate to accurately predict T1S based on C7S without factoring in the age-related parameter. Thus, we propose a novel perspective for calculating T1S on a radiograph by examining differences in cervical alignment patterns. This study indicated there were significant variations between C7S and T1S in 1 lordotic, 2 lordotic, straight and 2 sigmoid alignment patterns. Notably, the average value of △ was 4.7° and 5.2°, respectively in 1 lordotic and 2 sigmoid alignment patterns. Both were remarkably larger than other cervical morphotypes. Of note, no significant difference was noted between C7S and T1S in kyphotic and 1 sigmoid alignment patterns. Considering that there is the strongest positive correlation between △ and the caudal arch, we speculated that this may be related to the negative value of the caudal arch in kyphotic and 1 sigmoid alignment patterns, which causing a smaller △. Thus, it is feasible to directly measure C7S in kyphotic and 1 sigmoid alignment patterns when T1S was not visible. For the remaining four cervical alignment patterns, T1S can be predicted by linear regression model.
Limitations
This study has various limitations. First, we only used data from Chinese volunteers, most of whom are female (76%). Moreover, there is no occupational data, which may have affected cervical alignment patterns. However, the dataset that was generated in this study was large enough for majority of the evaluations. Second, we only included asymptomatic subjects without cervical radiculopathy (CR) or cervical spondylotic myelopathy (CSM), which may cause changes in the cervical curvature, especially in elderly patients. Studies should assess the visibility of C7S or T1S on radiographs in CR or CSM patients, as this may limit the utility of C7S or T1S in assessment of postoperative cervical sagittal balance. However, our results could describe the true parameters that did not affected by clinical symptoms. Third, global sagittal alignment parameters in whole-spine standing radiographs were not included. Despite these limitations, our findings form the basis for accurately predicting T1S.
Conclusion
This study explored the association between C7S and T1S in terms of age and cervical alignment patterns. In the correlation analysis, △ showed a strong correlation with caudal arch. T1S, C7S, and △ exhibited a progressive increase with age. Linear regression equations were established to accurately predict T1S based on the C7S in 1 lordotic, 2 lordotic, straight and 2 sigmoid alignment patterns. C7S can be directly used as a reliable proxy for T1S in kyphotic and 1 sigmoid alignment patterns. The strengths of the current study include the ability to intuitively judge the substitutability of C7S for T1S according to the cervical alignment patterns, without considering the age-related changes in △.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key Research and Development Program of China (No.2020YFC2004900), National Natural Science Foundation of China (H0608), Natural Science Foundation of China (No.81672201, 81871794) and Beijing Hospitals Authorit’Ascent Plan (No.DFL20190802).