
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Reported incidences and complications of heterotopic ossification (HO) after using recombinant human bone morphogenetic protein–2 (rhBMP-2) in transforaminal lumbar interbody fusion (TLIF) have been inconclusive. This study was designed to evaluate both incidences of radiologic and symptomatic HO in a large series of TLIFs using rhBMP-2.
Methods:
A total of 996 disc levels in 927 consecutive TLIF patients were retrospectively evaluated at 6-month postoperative follow-up in a single surgical practice. Subjects were separated into the BMP group and the control group. Operative reports, pre- and postoperative medical records were reviewed. Computed tomography (CT) scans were analyzed and graded independently for ossification at each disc level of TLIF.
Results:
A total of 933 disc levels were in the BMP group, and 63 were in the control group. Six-month fusion rate of interbody was 92.5% in the BMP group, which was significantly higher in contrast to 71.4% in the control group (P < .001). The incidence of radiologic HO in the BMP group was 13.5%, which was significantly higher than 1.6% in the control group (P = .006). After controlling for basic demographics and comorbidities, the presence of radiologic HO was significantly associated with the use of rhBMP-2 (P = .026). However, only one case in the BMP group (0.11%) developed a symptomatic HO (mild-medium left buttock pain, treated nonsurgically) involving left foramen of L5-S1.
Conclusions:
rhBMP-2 can be safely used in TLIF with regard to HO. There was a low rate of radiologic HO and minimal symptomatic HO, with high fusion rates at 6 months postoperative.
Keywords
Introduction
As an osteoinductive growth factor, recombinant human bone morphogenetic protein–2 (rhBMP-2) has been broadly used in anterior, lateral, posterolateral, transforaminal, and posterior lumbar interbody fusion procedures since the early 2000s. 1 -4 In certain series, it has been shown to yield excellent fusion rates over 92% to 100%, with few complications. 3 -8 Other series, however, have noted BMP-related complications such as postoperative radiculitis, vertebral osteolysis, infection, and heterotopic ossification. 9 -12
Because of the osteoinductive nature of BMP, heterotopic ossification (HO; also known as ectopic bone formation), which is defined as excess bone formation outside the intended fusion area, is a potentially serious complication. 13 -15 Previous studies involving rhBMP-2 use in transforaminal lumbar interbody fusion (TLIF) reported an increased rate of HO in the epidural or foraminal area, but no clinical consequences (eg, new reported/reoccurred back or leg pain, or numbness) resulted. 6,16 In contrast, other studies reported rhBMP-2 cases with significant HO and clinical symptoms of neural compression, with a few of those cases requiring revision surgery to remove the HO. 12,17,18
Overall, reported incidences and clinical complications of HO after using rhBMP-2 in TLIF have been limited, inconclusive and occasionally, contradictory. Therefore, the purpose of this study was to evaluate both the radiologic and clinical incidence of HO in a large series of TLIFs using rhBMP-2.
Methods
Study Design
The study was approved by the review board of the institution involved. This is a retrospective cohort study including 927 consecutive adult patients with a total of 996 disc levels undergoing TLIF performed by a single surgeon between January 1, 2007 and June 30, 2017. A total of 1104 patients with TLIF were initially reviewed. In all, 177 patients were excluded due to lack of postoperative computed tomography (CT) scan, previous attempt for fusion at the involved level, or undergoing surgery for nondegenerative diseases (eg, trauma, infection, or tumor). A total of 927 included patients were separated into 2 groups based on whether rhBMP-2 was used for the interbody fusion: the BMP group and the control group. Bilateral segmental pedicle screw-rod fixation was used in each case. A single polyetheretherketone interbody cage was placed through a unilateral transforaminal approach. In the BMP group, rhBMP-2 was administrated in the mixture with local bone graft and packed in the cage. Care was taken to avoid placement of the collagen sponge anywhere near the posterior annulus. Being a retrospective study, the exact dosing varied depending on the number of levels being fused. However, in general, the equivalent of one-eighth (about 1 mg of rhBMP-2) of a medium kit of INFUSE (Medtronic) was placed inside the cage, and one-eighth was mixed with local bone and placed anterior to the cage in the disc space. In control group, either local bone graft or iliac crest bone graft was applied without the use of BMP. Medical records including operative reports, pre- and postoperative clinical notes, and routine lumbar CT scans (high-resolution axial with sagittal and coronal reconstruction) at 6-month postoperative follow-up were retrospectively and independently reviewed.
Radiographic Evaluation
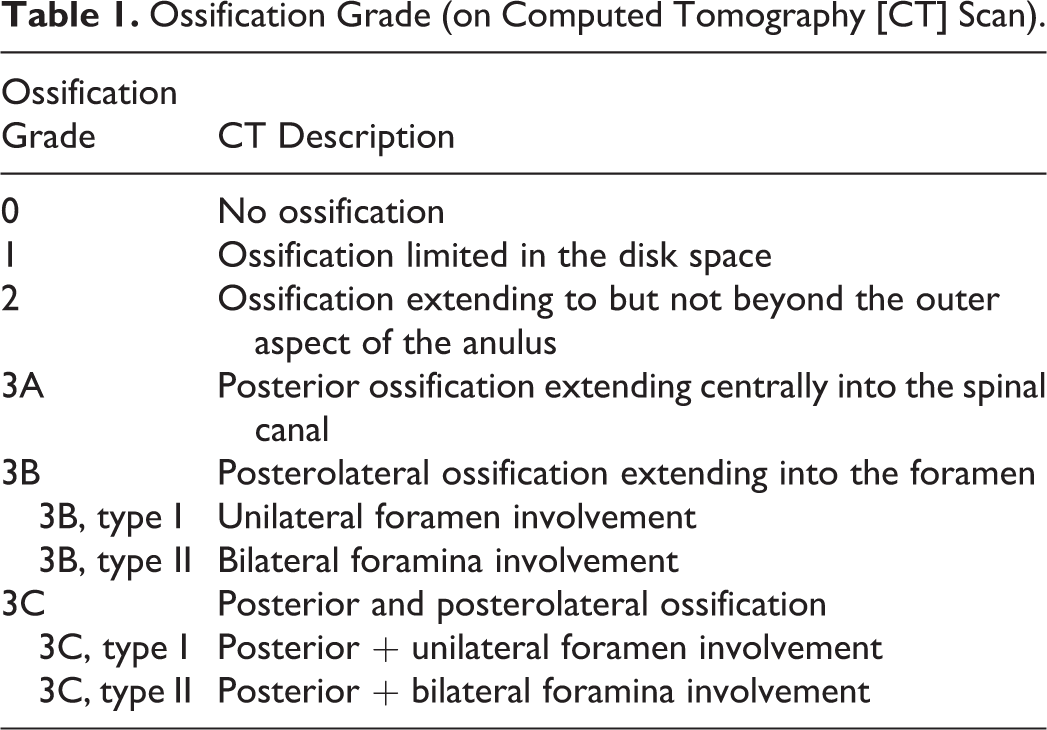
Both fusion and ossification at each disc level undergoing TLIF were evaluated independently by 2 reviewers on postoperative CT at 6-month follow-up. Fusion was assessed by the bridging bone continuity as previously described. 16,19,20 Ossification at the operated level was rated based on a grading system (Table 1 and Figure 1) modified from previous studies 6,16 to fully cover all possible types of ossification. Grades 3A, B, and C all indicate radiologic HO according to its definition. The rates of each grade were compared between the BMP and control groups. In addition, the rates of HO among each operated disc level were compared in the BMP group.
Ossification Grade (on Computed Tomography [CT] Scan).
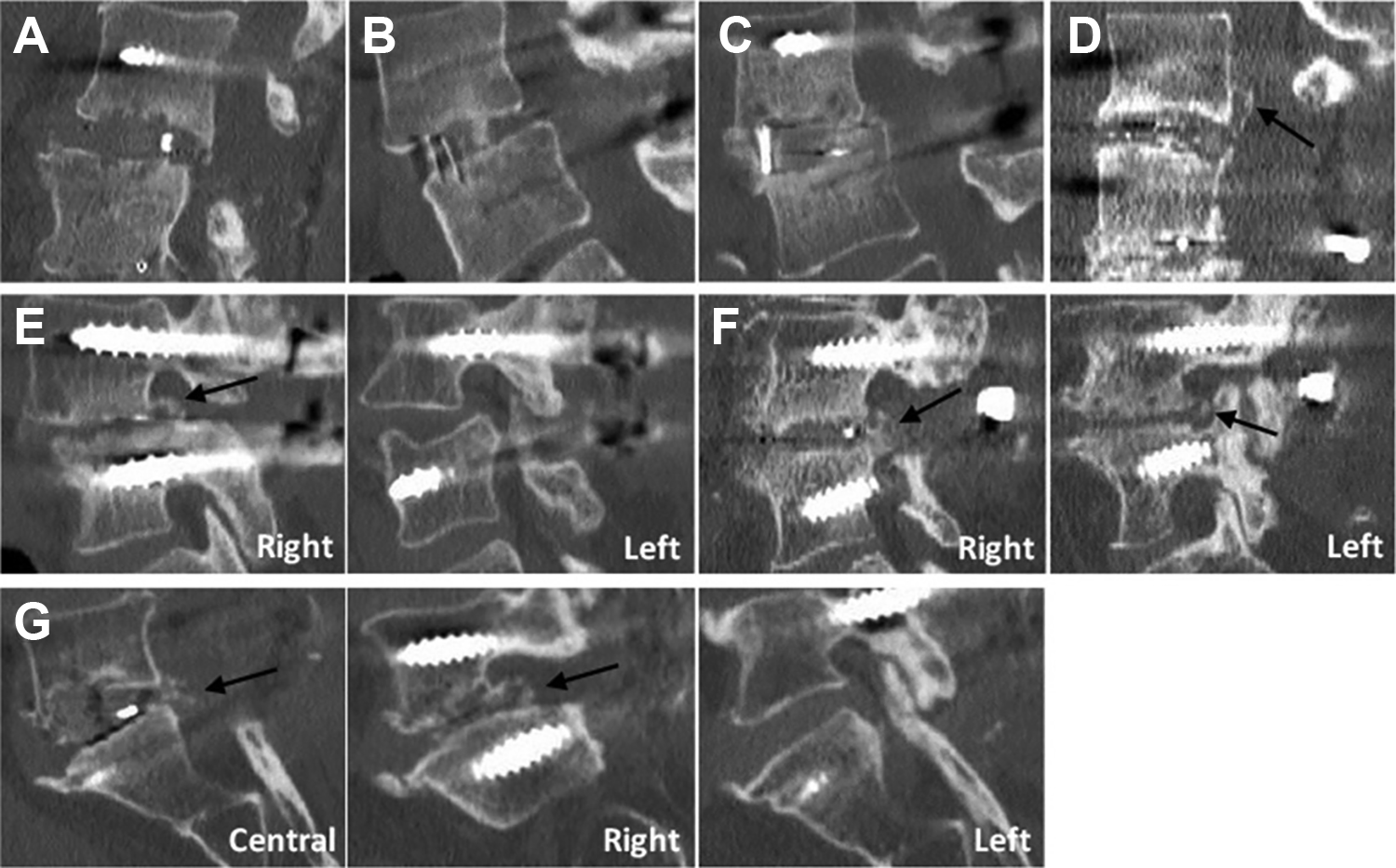
Examples of ossification grades at the sagittal view. (a) Grade 0, no apparent ossification; (b) Grade 1, ossification limited in the disk space; (c) Grade 2, ossification extending to but not beyond the outer aspect of the anulus; (d) Grade 3A, posterior ossification extending centrally into the spinal canal; (e) Grade 3B, type I, posterolateral ossification extending into unilateral foramen (right, black arrow); (f) Grade 3B, type II, posterolateral ossification extending into bilateral foramina (black arrow); (g) Grade 3C, type I, posterior (central, black arrow) and posterolateral (right, black arrow) ossification. No Grade 3C, type II was observed in this study.
Clinical Evaluation
Pre- and postoperative medical records were reviewed for visual analogue pains scores, and clinical complications potentially associated with HO. These complications included any newly reported or recurrent lumbar symptoms (eg, back or leg pain), or physical findings of nerve root compression. The management of clinical complications due to HO was also reviewed.
Statistical Analyses
All statistical analyses were performed using IBM SPSS Statistics 22 (IBM Corp, Armonk, NY, USA). Results were reported as the mean ± standard error of the mean where applicable. Comparison of categorical variables between BMP and control groups was analyzed with Fisher’s exact test or chi-square test. The association between the presence of HO and the use of BMP was determined by univariate logistic regression that controlled for patient demographics and comorbidities. Rates of HO among each operated disc level (from T12-L1 to L5-S1) in BMP group were also compared and analyzed by Fisher’s exact test. P < .05 was considered significant throughout this study.
Results
Patient Data
A total of 927 patients with a mean age of 63.8 years (range, 20-88 years; 59.0% female) were included, 859 patients with single-level TLIF, 67 with 2-level TLIF, and 1 with 3-level TLIF. Mean clinical and CT follow-up was 185 days (range, 104-300 days). A total of 996 operated disc levels were investigated, with 933 levels in the BMP group and 63 levels (40 with local bone graft, and 23 with iliac crest bone graft) in the control group (Tables 2 and 3).
Patient Demographics.

Abbreviations: BMI, body mass index; BMP, bone morphogenetic protein.
Surgical Disc Level Information.

Abbreviation: BMP, bone morphogenetic protein.
Fusion and HO Evaluation on 6-Month CT
The fusion of interbody was assessed directly from a routine 6-month CT. A total of 863 of 933 (92.5%) disc levels in BMP group were successfully fused, in contrast to 45 of 63 (71.4%) fused in control group. A statistically significant difference in the rate of interbody fusion was shown between the 2 groups (P < .001).
As shown in Table 4, compared with the control group, ossification in the BMP group was composed of significantly less grade 1, but more grade 2 and grade 3 (HO, 13.5%). In the BMP group, 72 disc levels were grade 3B type I, 4 were grade 3B type II; all 12 disc levels of grade 3C were type I. After controlling for basic demographics and comorbidities (Table 5), the presence of HO on CT was significantly associated with the use of BMP.
Comparison of Ossification Grade at the Level of TLIF on CT Scan.

Abbreviations: BMP, bone morphogenetic protein; CT, computed tomography; TLIF, transforaminal lumbar interbody fusion.
aAll grade 3 indicates the presence of heterotopic ossification.
Univariate Logistic Regression for Association With the Presence of HO.

Abbreviations: BMI, body mass index; BMP, bone morphogenetic protein; CI, confidence interval; HO, heterotopic ossification; OR, odds ratio.
aValues in boldface indicate significance at P < .05.
For HO in BMP group, grade 3B (posterolateral HO into the foramen) was most commonly observed compared with grade 3A and 3C (P < .001). In addition, there is no significant difference among the rate of HO at each operated disc level from T12-L1 to L5-S1 (Table 6, P = .228).
Rate of HO at Each Disc Level in the BMP Group.

Clinical Outcomes
Average preoperative pain score was 6.6 ± 2.0, which significantly reduced to 0.5 ± 0.9 at postoperative 6-month follow-up (P < .001). Only 1 case (male patient, age 67 years) in BMP group (1/933, 0.11%) developed symptomatic HO. This patient had HO at L5-S1 and complained of a recurrent mild-medium left buttock pain which recurred at 2 months postoperative but remained less than preoperative. It was treated nonsurgically without further progression. No patients in the control group had symptomatic HO.
Discussion
In this study, we evaluated the rate of radiologic and symptomatic HO associated with TLIF using rhBMP-2 in a large series. Although radiologic HO was significantly more common in the BMP group versus control, with 13.5% of operated levels displaying HO on CT scan at 6-month follow up, symptomatic HO was very rare, occurring in only 1 of 933 (0.11%) operated levels. The risk of radiologic HO also did not vary by spinal level, although the vast majority of cases were performed from L3-S1. On the basis of these findings, we conclude that rhBMP-2 can be safely used in TLIF with relatively low risk of radiologic HO and very little risk of symptomatic HO.
Since rhBMP-2 was introduced in the early 2000s, the possibility of postoperative HO has been a concern due to its potent osteoinductive nature. However, the actual rate of HO remains unclear. An early series in 2004 by Haid et al 6 reported 75% (23 of 32) of patients receiving rhBMP-2 for posterior lumbar interbody fusion (PLIF) developed HO on CT scan at 6-month follow up, compared with 13% (4 of 31) of those receiving iliac crest bone graft. In that series, no symptomatic HO was observed. Later studies by Mummaneni et al 7 and Villavicencio et al 8 both reported a zero rate of HO in patients undergoing TLIF with rhBMP-2, although different surgical techniques were used, including the application of a physical barrier. In contrast to studies reporting no symptomatic HO, Wong et al 17 described 5 patients with symptomatic HO 8.4 months after PLIF or TLIF with rhBMP-2. Three of the 5 patients underwent revision surgery with the removal of HO that resulted in moderate improvement in radiculopathy. Potential risk factors postulated by the authors for symptomatic HO included hematoma or sterile fluid collections in the area of the decompression, wound irrigation after BMP insertion, and drains placed deep to the fascia. Rihn et al 10 reported a 2.3% (2 of 86) rate of symptomatic HO (postoperative radiculitis) in patients undergoing single-level TLIF with rhBMP-2 at 29.4-month follow-up. In that series, 1 patient underwent revision surgery with improvement of radiculitis.
A major strength of this study is its very large sample size. To our knowledge, the current study represents one of the largest series on this subject to date. All patients were also evaluated postoperatively with CT scan, which provides a level of detail for evaluating HO in the lumbar spine that far surpasses x-rays alone. 21 Because the existing ossification grading systems in the literature 6,16 did not fully cover all possible types of HO we have observed in the clinic, we also utilized a modified ossification grading system to address this issue. Additionally, all surgical cases were performed by a single surgeon, eliminating variation in surgical technique among cases.
There are limitations to the present study besides a retrospective design. First, the CT scans were obtained at 6 months postoperative, because that is when we evaluate patients clinically for the presence of fusion before allowing for an increase in activities. As such, it is possible that findings may differ with longer-term follow-up. However, the literature demonstrates that HO usually occurs within the first 6-month period, with progressive bone maturation then taking place after the initial formation of bone mass. 22,23 Cipriano et al 23 also reported that the time to HO presentation typically occurs at about 2 months postneurologic injury, but admittedly can range from 2 weeks to 12 months postinjury.
A second limitation is that the dose of rhBMP-2 was not standardized in this retrospective series. We estimate that the average dose of rhBMP-2 used within the disc space was 2-3 mg, which is on the low end of the spectrum reported in the literature, which varies from 2 to 12 mg per level. 13 We believe that the lower dose used in our cases contributes to the lower rates of HO observed in the BMP group. In addition, our surgical technique avoided placement of the collagen sponge containing rhBMP-2 near the posterior annular defect. The rhBMP-2 sponge was placed as anteriorly as possible within the disc space in order to avoid contact with the posterior annulus. Of note, a physical barrier was not used in these procedures. If the rhBMP-2 were applied near the annulus, we suspect there would be a higher rate of both radiologic and symptomatic HO. Therefore, we believe that the safe use of rhBMP-2 in TLIF is technique dependent. We believe that the low rates of symptomatic and radiologic HO observed are due to a combined result of limiting the concentration of rhBMP-2, and a surgical technique that ensures that the rhBMP-2 sponge does not contact the posterior annulus.
Conclusion
In conclusion, rhBMP-2 can be used safely in TLIF with regard to HO. There was a low rate of radiologic HO and minimal symptomatic HO, with high fusion rates at 6 months postoperative. Careful attention to dose and placement of the rhBMP-2 sponge anteriorly (away from the posterior annular defect) are likely important factors in limiting HO formation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John M. Rhee, MD: Dr. Rhee reports personal fees from Medtronic, personal fees from Stryker spine, personal fees from Biomet Spine, personal fees from Zimmer, personal fees from Wolters-Kluwer, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.