
Abstract
Study Design:
Retrospective cohort.
Objective:
To understand which patient and surgical factors are predictive of an increased odds of undergoing an admission and a prolonged stay >2 days in an intensive care unit (ICU) following corrective surgery for pediatric deformity.
Methods:
The 2016 American College of Surgeons–National Surgical Quality Improvement Program (ACS-NSQIP) Pediatric Spinal Fusion Procedure Targeted database records, merged with original 2016 ACS-NSQIP Pediatric file variables, were used for this study. Univariate and multivariate analyses were used to identify independent risk factors associated with admission, as well as a prolonged length of stay in the ICU following surgery.
Results:
A total of 1398 (39.5%) patients required an ICU admission following the procedure—out of whom 416 (29.8%) stayed for more than 2 days. Following adjusted analysis, patient and surgical factors independently associated with an ICU admission were black/African American versus white race, anterior fusion, combined fusion, nonidiopathic scoliosis, preoperative ventilator dependence, asthma, having structural pulmonary abnormality, developmental delay, having a neuromuscular disorder, requiring nutritional support and a total operative time >270 minutes. The only significant factors associated with a prolonged length of ICU stay >2 days were preoperative ventilator dependence, nutritional support requirement, and undergoing anterior or combined fusion.
Conclusions:
This study is the first of its kind to identify significant patient- and procedure-level factors associated with an ICU admission, and also explores predictors for a prolonged stay in the ICU. Surgeons can use this data to preoperatively counsel families and ensure postoperative course of care is appropriately planned ahead of time.
Introduction
Pediatric spinal deformities are often complex cases that pose a major challenging task for an orthopedic/spine surgeon. While conservative treatment remains the initial sought-out management for these conditions, a significant proportion of patient ultimately end up requiring corrective surgery, in the form of spinal fusions, to alleviate the quality of life. With an overall increase in the number of spinal fusions being performed for management of pediatric scoliotic conditions, 1,2 as well as a marked inflation over time in overall hospital cost/charges for pediatric spinal fusions, 3 there has been a renewed interest in identifying patient- and hospital-level factors that may be modified to reduce the overall cost burden of the surgery.
Because of the prolonged operative time and the need for adequate and appropriate pain control in the acute postoperative period, a certain subset of pediatric deformity patients often require intensive care unit (ICU) admission/stay following surgery. ICU stays can be costly, 4 and as the current health care system moves toward a widespread adoption of value-based approaches aimed to increasing the quality of care while controlling unnecessary health care resource utilization, 5 there is a need for identification of risk factors that may predispose patients to a prolonged ICU stay following surgery for pediatric spinal deformity.
Using a national surgical dataset of patients undergoing pediatric spinal fusions, the current study aims to understand 2 major objectives: (1) identification of patient- and operative-level risk factors associated with an ICU admission following surgery for pediatric deformity and (2) risk factors associated with a prolonged ICU stay of more than 2 days following spinal fusion.
Materials and Methods
Database
In 2016, the American College of Surgeons–National Surgical Quality Improvement (ACS-NSQIP) released a Pediatric Spinal Fusion Procedure Targeted Database. The Spinal Fusion Procedure Targeted dataset is an enhanced subset of the larger ACS-NSQIP database and contains granular clinical information relevant to pediatric spinal fusions (CPT-22800, CPT-22802, CPT-22804, CPT-22808, CPT-22810, and CPT-22812). Complete details of the Spinal Fusion Procedure Targeted dataset can be found elsewhere. 6 Using unique case IDs, the 2016 ACS-NSQIP Pediatric Spinal Fusion Procedure Targeted dataset was merged with the larger 2016 ACS-NSQIP Pediatric database to retrieve a complete list of variables that could be analyzed as part of the study. The ACS-NSQIP Pediatric Spinal Fusion Procedure Targeted dataset defines the length of stay in the ICU as any part of a 24-hour period that a patient spends in the ICU as defined by the program’s hospital acuity definition on level of care. Any units that do not deliver ICU level of care under the hospital’s definition of ICU would not qualify as ICU admission in the database.
To identify patient- and procedure-level characteristics of patients being admitted to the ICU, the study cohort was divided into 2 major groups for further analysis: (1) those who were admitted to ICU following surgery versus (2) those who were not admitted to an ICU following surgery. To analyze predictors/risk factors associated with a prolonged ICU stay, a separate subgroup analysis was carried out between (1) patients staying in ICU for more than 2 days versus (2) patients staying in the ICU for 1 to 2 days. The cutoff for a prolonged length of stay of more than 2 days, was chosen arbitrarily based on clinical fact that most pediatric deformity patients who get admitted to the ICU stay for around 1 to 2 days.
Statistical Analysis
Univariate analyses, using Pearson chi-square tests, were used to assess for unadjusted associations between clinical characteristics of the study population and ICU admissions. Similar unadjusted univariate comparisons were also carried out to identify significant associations between patient/clinical characteristics and a prolonged ICU stay. All variables with a P value <.1 were added into a multivariate logistic regression model to identify independent predictors associated with an ICU admission, as well as prolonged ICU stay, following a pediatric spinal deformity operation. To prevent multicollinearity in our regression models, we ran collinearity diagnostics to retrieve variance inflation factors (VIF) for variables. A VIF ≥ 2.5 was set as the cutoff for dropping variables from regression model. None of our variables had a VIF ≥ 2.5 and were therefore retained in the final model. For all statistical purposes, a P value of less than .05 was considered significant. All statistical analyses were performed using SPSSv24 (IBM, Armonk, NY).
Results
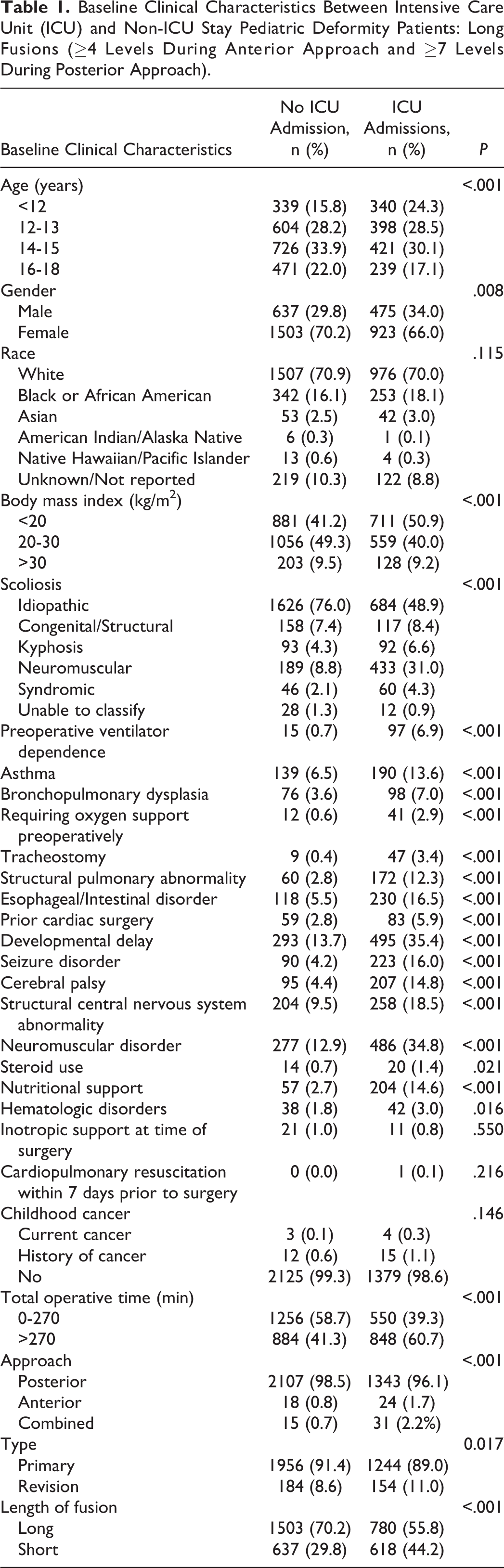
A total of 1398 (39.5%) patients required an ICU admission following spinal fusion for pediatric deformity (Table 1).
Baseline Clinical Characteristics Between Intensive Care Unit (ICU) and Non-ICU Stay Pediatric Deformity Patients: Long Fusions (≥4 Levels During Anterior Approach and ≥7 Levels During Posterior Approach).
Independent Risk Factors for an ICU Admission
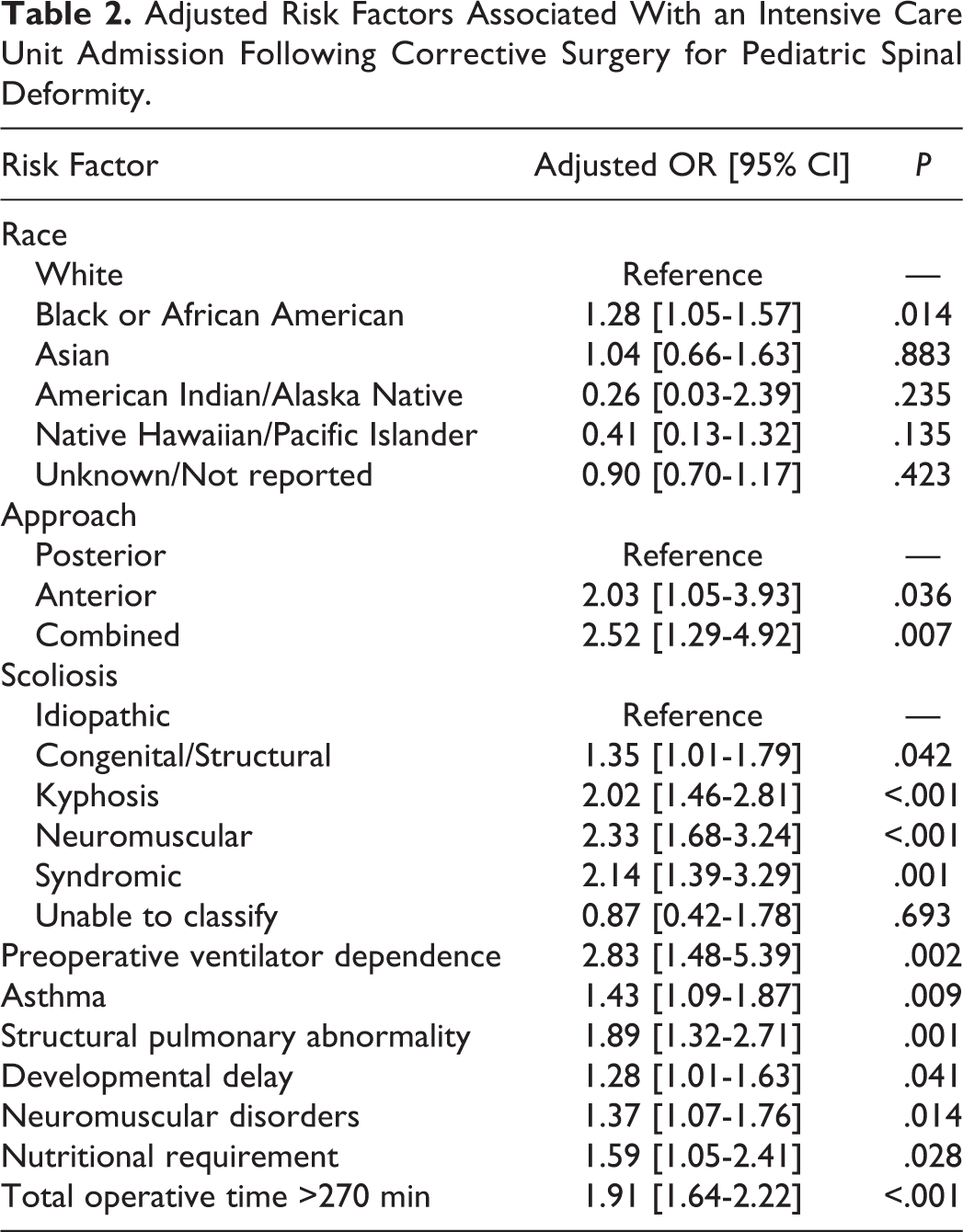
Following adjustment in a multivariate logistic regression model, independent predictors associated with an ICU admission following surgery were black/African American race versus white (odds ratio [OR] 1.28 [95% CI 1.05-1.57]; P = .014), undergoing an anterior-only versus posterior-only fusion (OR 2.03 [95% CI 1.05-3.93]; P = .036), undergoing a combined/anterior-posterior versus posterior-only fusion (OR 2.52 [95% CI 1.29-4.92]; P = .007), having congenital/structural scoliosis (OR 1.35 [95% CI 1.01-1.79]; P = .042), kyphosis (OR 2.02 [95% CI 1.46-2.81]; P < .001), neuromuscular scoliosis (OR 2.33 [95% CI 1.68-3.24]; P < .001) or syndromic scoliosis (OR 2.14 [95% CI 1.39-3.29]; P = .001), being preoperatively ventilator dependent (OR 2.83 [95% CI 1.48-5.39]; P = .002), having asthma (OR 1.43 [95% CI 1.09-1.87]; P = .009), having a structural pulmonary abnormality (OR 1.89 [95% CI 1.32-2.71]; P = .001), diagnosis of developmental delay (OR 1.28 [95% CI 1.01-1.63]; P = .041), concurrent neuromuscular disorder (OR 1.37 [95% CI 1.07-1.76]; P = .014), requiring nutritional support (OR 1.59 [95% CI 1.05-2.41]; P = .028), and a total operative time >270 minutes (OR 1.91 [95% CI 1.64-2.22]; P < .001) (Table 2).
Adjusted Risk Factors Associated With an Intensive Care Unit Admission Following Corrective Surgery for Pediatric Spinal Deformity.
Predictors of a Prolonged ICU Stay >2 Days
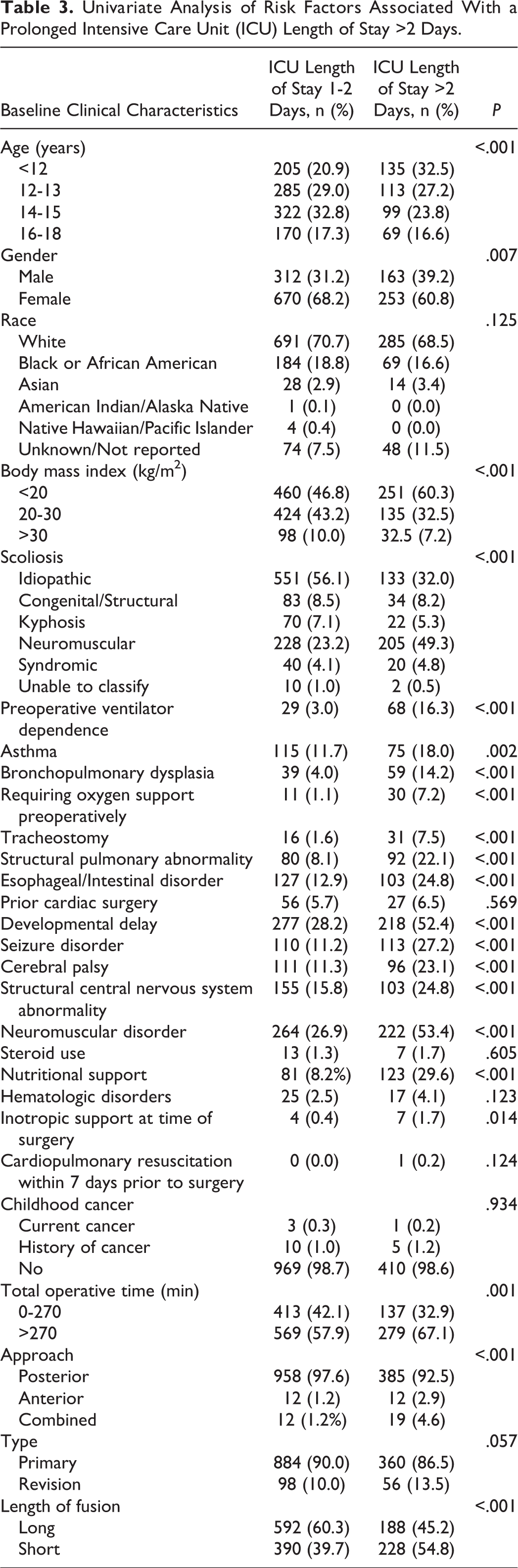
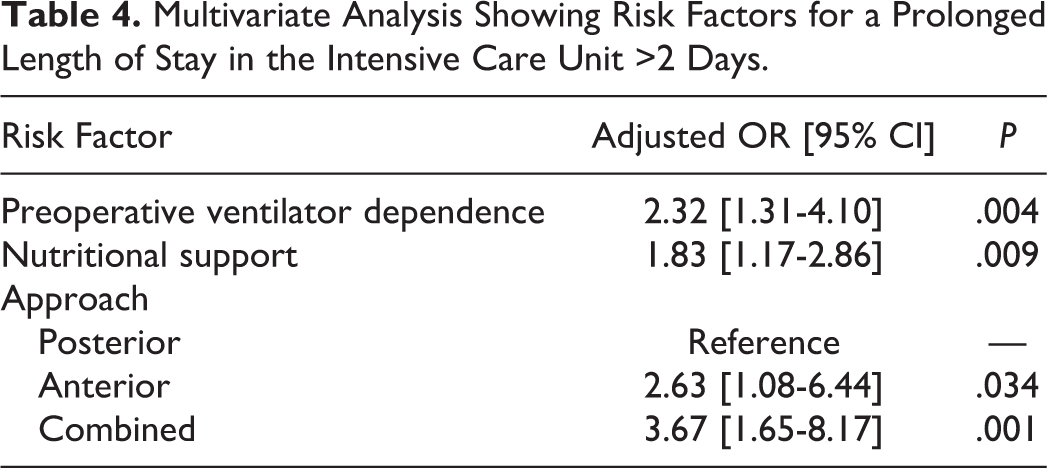
A total of 416 patients (29.8% of ICU patients) stayed for more than 2 days. Unadjusted analyses of patient- and procedure-level characteristics associated with a prolonged ICU stay >2 days can be seen in Table 3. Following adjustment in multivariate regression, independent risk factors associated with a prolonged ICU stay >2 days were preoperative ventilator dependence (OR 2.32; P = .004), nutritional support requirement (OR 1.83; P = .009), and undergoing anterior (OR 2.63; P = .034) or combined (OR 3.67; P = .001) fusion (Table 4).
Univariate Analysis of Risk Factors Associated With a Prolonged Intensive Care Unit (ICU) Length of Stay >2 Days.
Multivariate Analysis Showing Risk Factors for a Prolonged Length of Stay in the Intensive Care Unit >2 Days.
Discussion
As evidenced in our findings, nearly 40% of pediatric deformity patients are admitted to the ICU following a spinal fusion procedure with nearly 30% of these patients staying for more than 2 days. Providers can use this data to not only understand the patient population who would require an ICU stay but also launch optimization strategies aimed at minimizing the need for a prolonged ICU stay, reduce the hospital length of stay and subsequently curb costs associated with unnecessary health care resource utilization.
Among patient-level factors, we noted that race/ethnicity and higher comorbidity burden influenced the need for an ICU stay following spinal fusion for pediatric deformity. Notably, children of black/African American ethnicity, as compared with white/Caucasian, were more likely to be admitted to an ICU. This finding is similar to previously reported observations by Silber et al, 7 showing that black patients, as compared with white patients, were more likely to have an ICU use. Among other factors, patients with a concomitant neuromuscular disorder, asthma, preoperative ventilator dependency, structural pulmonary abnormality were more likely to be admitted to an ICU following the surgery. Neuromuscular disorders are known to interfere with routine respiratory mechanisms. 8,9 Furthermore, pediatric patients are at marked risk of developing hypoventilation after an invasive surgery such as a complex spinal fusion for pediatric deformity. Given the latter, it is likely that providers may be cautious and would prefer having pediatric deformity patients with existing neuromuscular disorders to be admitted to an ICU, so that appropriate resources are available to immediately optimize and/or mechanically ventilate the patient if a scenario may arise. Concurrent pulmonary comorbidities such as asthma, preoperative ventilator dependence and having a structural pulmonary abnormality may also influence a provider’s choice in the same way.
Our results also found that patients with developmental delay were more likely to be admitted to an ICU. Given that these patients are complex, and require higher acuity care, this finding is not surprising. However, it is imperative to highlight that recent literature has shown that pediatric individuals with developmental delay are at higher risk of developing delirium. 10 Enhanced care pathways aimed at optimizing outcomes for patients with developmental delay may be an effective way of mitigating the need for an ICU admission while maintaining the quality of care. Anterior-only and/or combined fusions are largely invasive procedures, as compared to posterior-only fusions, and have been shown to be associated with significant morbidity in adults 11,12 and pediatric patients. 13,14 It is likely that the invasiveness of the approach may guide the choice of an ICU admission in these patients. We also noted that performing spinal fusions on all types of nonidiopathic scoliosis was also associated with higher odds of ICU admission, and it is probable that the higher comorbidity burden seen in congenital/neuromuscular/syndromic scoliotic types may be playing a role. In addition, the varying complexity and/or invasiveness of the spinal fusion employed in different types of scoliosis may also be responsible for the higher odds of ICU admissions seen in these high-risk patients. Last, spinal fusions exceeding an operative time of more than 270 minutes was associated with higher risk of ICU admission. Increasing operative time has been shown to be associated with poor 30-day outcomes in adult spinal deformity surgery. 15 -17 An increasing operative time may be considered a proxy of case-complexity or the occurrence of certain intraoperative complications thus requiring these patients to continued care in a high-acuity surveillance environment such as in the ICU.
While the aforementioned factors were associated with an ICU admission, it is important to relate that the only significant predictors for a prolonged ICU stay of more than 2 days were preoperative ventilator dependence, nutritional support, and undergoing an anterior and/or combined fusion. These results support the fact that most patients only stay in the ICU for a short time, and the equipment of other alternative acuity-care level units (where overhead charges and/or costs are not high) with appropriate care providers would be an effective way for reducing costs associated with ICU stay. Construction of enhanced care pathways, involving preoperative optimization in patients requiring nutritional support, for instance, would also be an operational approach toward avoiding needless prolonged ICU stays. It is important to consider that appropriate selection of patients and enhancing perioperative pain protocols 18 may significantly alleviate the usage and costs associated with an ICU admission. This is particularly essential in the cases of invasive anterior and/or combined fusions where pain may be higher as compared to conventional posterior fusions. Abu-Kishk et al 19 conducted a retrospective single institution review of children undergoing primary scoliosis surgery and concluded that, similar to our findings, young, healthy idiopathic scoliosis children undergoing posterior fusions could be successfully managed in regular wards in the acute postoperative period. While the study also went on to discover that the use of long-acting opioids was associated with increased odds of ICU admission, the lack of adjunct anesthetic/pain protocols and/or granular clinical data with regard to anesthetic medications in the NSQIP dataset prevents us from analyzing this possible aspect. The NSQIP dataset also lacks differentiation between other postoperative care units such as high-acuity units, high-dependency units, and/or general wards. It is also vital to deliberate that while the NSQIP dataset takes into account a number of comorbidity and surgical-related variables, it still lacks clinical data about the severity of scoliosis and radiographic parameters such as the Cobb’s angle, which may be useful in including as part of the analysis.
Conclusion
Despite the limitations, the study is the first of its kind to use a relatively large sample size from a national validated surgical dataset of pediatric spinal fusions and identify a number of patient- and operative-level risk factors associated with an ICU admission and a prolonged ICU stay. Nearly 70% of ICU patients stayed for fewer than 2 days. Identification and/or risk stratification of individuals in this group can allow providers and care-givers to tailor and construct suitable care pathways, aimed at optimizing the outcome of these high-risk patients in a routine surgical ward setting, rather than having these patients undergo care in an expensive high-acuity setting such as the ICU. Meaningfully, the only patients who would ultimately require a prolonged intensive care and/or may benefit from an ICU admission were those with preoperative ventilator dependence, nutritional support requirement, or undergoing an anterior/combined fusion.
Footnotes
Authors’ Note
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS-NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.