
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Diabetes mellitus is a highly prevalent disease in the United States. Adult spinal deformity (ASD) surgery encompasses a wide variety of spinal disorders and is associated with a morbidity rate between 20% and 80%. Considering utilization of spinal surgery will continue to increase, this study investigates the influence of diabetes mellitus on acute postoperative outcomes following elective ASD surgery.
Methods:
The 2010-2014 American College of Surgeon’s National Surgical Quality Improvement Program database was queried using Current Procedural Terminology and International Classification of Diseases (9th Revision) diagnosis codes relevant to ASD surgery. Patients were divided into cohorts based on their diabetic status. Bivariate and multivariate logistic regression analyses were employed to identify which 30-day postoperative outcomes patients are at risk for.
Results:
A total of 5809 patients met the inclusion criteria for the study of which 4553 (84.2%) patients were nondiabetic, 578 (10.7%) patients had non–insulin-dependent diabetes mellitus (NIDDM), and 275 (5.1%) patients had insulin-dependent diabetes mellitus (IDDM). Diabetes status was significantly associated with length of stay ≥5 days (NIDDM: odds ratio [OR] = 1.27, 95% confidence interval [CI] = 1.02-1.58, P = .034; IDDM: OR = 1.55, 95% CI = 1.15-2.09, P = .004), any complication (NIDDM: OR = 1.26, 95% CI = 1.01-1.58, P = .037), urinary tract infection (NIDDM: OR = 1.87, 95% CI = 1.14-3.05, P = .012), and cardiac complications (IDDM: OR = 4.05, 95% CI = 1.72-9.51, P = .001).
Conclusions:
Given the prevalence of diabetes, surgeons will invariably encounter these patients for ASD surgery. The present study identifies the increased risk NIDDM and IDDM patients experience following ASD surgery. Quantification of this increased risk may improve the selection of appropriate surgical candidates, patient risk stratification, and patient postoperative safety.
Introduction
The number of adults in the United States with diabetes mellitus (DM) from 1980 through 2012 has nearly quadrupled from 5.5 million to 21.3 million. 1 –5 The incidence of DM among adults is approximately 1.7 million new cases per year, and if this trend continues, as many as 1 out of every 3 adults in the United States could have DM by 2050. 1,4 Considering both the DM and obesity epidemics in the United States, compounded with overall longer lifespans, the lifetime risk of DM has increased to 40% for US adults. 1 Currently, DM effects between 5.3% and 13.2% of people living in the United States, 6 with approximately 8.1 million people unaware they have DM. 1,2
Adult spinal deformity (ASD) is a complex spinal disorder and encompasses a wide variety of spinal conditions including degenerative scoliosis, adult scoliosis, sagittal and coronal imbalance, and iatrogenic deformity (with or without spinal stenosis). 7,8 Approximately 5 million adults in the United States are disabled to some degree from spine-related disorders. 9 The elderly population, a growing demographic in the United States and much of the Western world, is commonly affected by spinal conditions. 7,9 –11 Additionally, advances in surgery and anesthesia have reduced the physiologic impact of surgery, thus making the option of surgery available to older patients who may have a significant comorbidity burden. 10 Considering these population and medical factors, it is no surprise the annual number of discharges for spinal fusion procedures increased by 137% between 1998 and 2008, and this trend is expected to continue. 12 Choice of spinal deformity treatment is influenced by a variety of factors such as patient variables, location and type of deformity, number of affected levels, and sagittal alignment 9,11,13 and has been associated with morbidity rates between 20% and 80%. 7,14
Postoperative complications following ASD surgery can have significant impact on a patient’s quality of life and can also place a significant burden on the health care system. Previous studies in the orthopedic literature have demonstrated the adverse effect of DM on postoperative outcomes following spinal procedures. 3,6,15 –17 However, a need still exists in the literature as many previous studies have either been small, single-institution investigations or have not delineated between non–insulin-dependent diabetes mellitus (NIDDM) and insulin-dependent diabetes mellitus (IDDM) patients.
The present study utilizes the American College of Surgeon’s National Surgical Quality Improvement Program (ACS-NSQIP) database to analyze the effect of patient diabetes status on 30-day complications following elective ASD surgery. The authors hope that identifying which acute postoperative complications NIDDM and IDDM patients are at risk for may improve appropriate patient selection for surgery, assist physicians in developing risk reductive strategies such as tighter glycemic control, and direct physician postoperative management efforts in order to avoid common complications in diabetic populations.
Materials and Methods
Data Source
This was a retrospective study of prospectively collected data in the 2010-2014 ACS-NSQIP database. ACS-NSQIP data is collected by dedicated clinical abstractors at each institution on more than 150 demographic, preoperative, intraoperative, and 30-day postoperative variables. 18 –22 Over 500 hospitals that vary in size, socioeconomic location, and academic affiliation contributed data to the 2010-2014 ACS-NSQIP database. 18 The success of quality improvement initiatives based on ACS-NSQIP data has been validated in the VA and private sector. 20,23
Inclusion and Exclusion Criteria
The ACS-NSQIP database from 2010 to 2014 was used in this study. Adult patients (≥18 years) undergoing spinal fusion for deformity were identified based on Current Procedural Terminology (CPT) codes 22 800, 22 802, 22 804, 22 808, 22 810, 22 812, 22 818, and 22 819. CPT codes 22 843, 22 844, 22 846, and 22 847 were also included to capture long, multilevel fusion constructs. Patients with CPT codes 22 842 and 22 845 were included if they had an ICD-9 (International Classification of Diseases, 9th Revision) diagnosis for spinal deformity (including 737.1, 737.2, 737.3, 737.4, 737.8, and 737.9). Cases with missing preoperative data; emergency cases; patients with a wound class of 2, 3, or 4; an open wound on their body; current sepsis; current pneumonia; prior surgeries within 30 days; cases requiring cardiopulmonary resuscitation prior to surgery; any patients undergoing a nonelective procedure; or cases with diagnoses of cervical spine, trauma or injury to spine, or neoplasm of spine were excluded in order to reduce the risk of confounding variables.
Variable Definition
Patient demographic variables included sex, age (≤50, 51-60, 61-70, 71-80, and ≥80 years), and race (white, black, Hispanic, and other). Other race included American Indian or Alaska Native, Asian, Native Hawaiian or Pacific Islander, or Unknown/Not Reported. Preoperative variables included obesity (≥30 kg/m2), diabetes (NIDDM or IDDM), current smoking (within 1 year of surgery), dyspnea (≤30 days prior to surgery), functional status prior to surgery (independent or partially/totally dependent ≤30 days prior to surgery), pulmonary comorbidity (ventilator dependent ≤48 hours prior to surgery or history of chronic obstructive pulmonary disease ≤30 days prior to surgery), cardiac comorbidity (use of hypertensive medication or history of chronic heart failure ≤30 days prior to surgery), renal comorbidity (acute renal failure ≤24 hours prior to surgery or dialysis treatment ≤2 weeks prior to surgery), steroid use for chronic condition (≤30 days prior to surgery), ≥10% loss of body weight (in the last 6 months), bleeding disorder (chronic, active condition), preoperative transfusion of ≥1 unit of whole/packed red blood cells (RBCs; ≤72 hours prior to surgery), and American Society of Anesthesiology (ASA) physical status classification (≥3).
Intraoperative variables included operation year (2010-2014), surgery setting (inpatient vs outpatient), fusion length (long fusion is ≥4 levels during an anterior approach and ≥7 levels during a posterior approach), surgical approach (anterior, posterior, or combined), pelvic fixation, osteotomy, operative time (≥4 hours), and total relative value units. Thirty-day-day postoperative outcome variables include mortality, any postoperative complication, length of stay (LOS; ≥5 days), wound complication (superficial or deep surgical site infection, organ space infection, or wound dehiscence), pulmonary complication (pneumonia, unplanned reintubation, or duration of ventilator-assisted respiration ≥48 hours), venous thromboembolism (pulmonary embolism or deep vein thrombosis), renal complication (progressive renal insufficiency or acute renal failure), urinary tract infection (UTI), cardiac complication (cardiac arrest requiring cardiopulmonary resuscitation or myocardial infarction), intra-/postoperative transfusion, sepsis, reoperation (related to initial procedure), and unplanned readmission (related to initial procedure). ACS-NSQIP provides further information on characteristics of variables. 22
Patients were divided into cohorts depending on their diabetes status. Three cohorts were created: nondiabetic, NIDDM, and IDDM. Note, if a patient required both noninsulin and insulin treatment, they were classified as IDDM.
Statistical Analysis
Patients were divided into cohorts based on their diabetes status. A bivariate analysis was performed on patient demographic, preoperative, intraoperative, and postoperative characteristics using Pearson’s χ2 test. Fischer’s exact test was used where appropriate. Multivariate logistic regression models were employed, adjusting for patient demographic and preoperative and intraoperative variables to identify the influence of diabetes on each of the investigated 30-day postoperative complications. Regression models utilized a stepwise entry and removal criteria, set to a significance level of .05. SAS Studio Version 3.4 (SAS Institute Inc, Cary, NC) was used for all statistical analysis.
Results
Study Population
A total of 5809 patients met the inclusion criteria for the study, of which 4553 (84.2%) patients were nondiabetic, 578 (10.7%) patients were NIDDM, and 275 (5.1%) patients were IDDM. The median age was 61 ± 13.5 years.
Nondiabetic patients were more likely to be female, smoke, have an osteotomy, and have operation times ≥4 hours. NIDDM patients were more likely to be obese. IDDM patients were more likely to be black, >80 years of age, partially or totally functionally dependent, cardiac comorbidity, renal comorbidity, use steroids, ASA class ≥3, and long fusion lengths (Table 1).
Distribution of Demographics and Preoperative and Intraoperative Variables for Patients Undergoing Elective Spinal Deformity Surgery by Diabetes Status (N = 5338).a
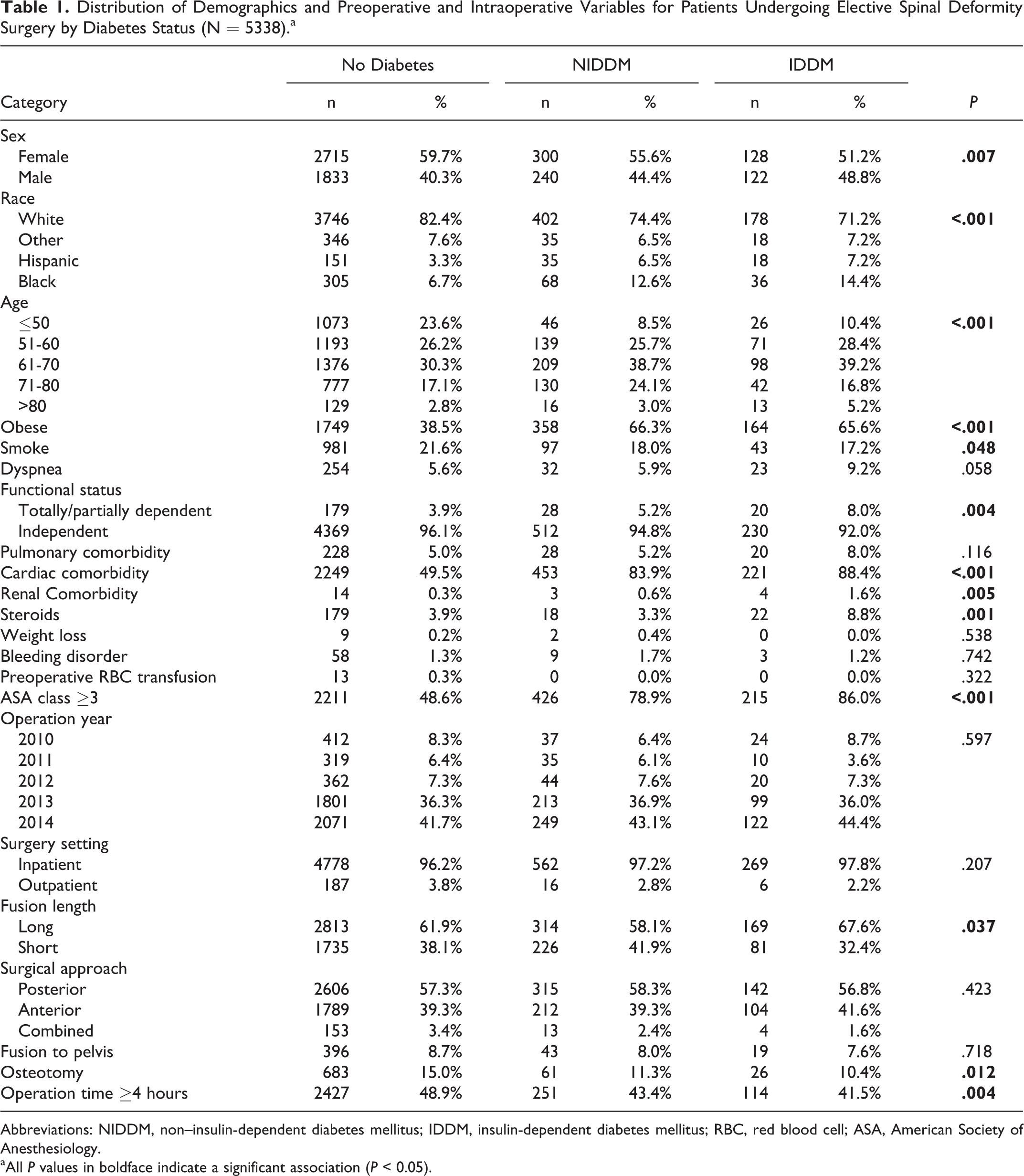
Abbreviations: NIDDM, non–insulin-dependent diabetes mellitus; IDDM, insulin-dependent diabetes mellitus; RBC, red blood cell; ASA, American Society of Anesthesiology. aAll P values in boldface indicate a significant association (P < 0.05).
Bivariate Analysis
Patient cohorts experienced a statistically significant difference in the following 30-day postoperative complications: mortality (nondiabetic: 19, 0.4%; NIDDM: 7, 1.3%; IDDM: 2, 0.8%), wound complications (nondiabetic: 99, 2.2%; NIDDM: 22, 4.1%; IDDM: 5, 2.0%), pulmonary complications (nondiabetic: 109, 2.4%; NIDDM: 20, 3.7%; IDDM: 11, 4.4%), UTI (nondiabetic: 84, 1.8%; NIDDM: 19, 3.5%; IDDM: 5, 2.0%), cardiac complication (nondiabetic: 23, 0.5%; NIDDM: 7, 1.3%; IDDM: 7, 2.8%), reoperation (nondiabetic: 171, 3.8%; NIDDM: 31, 5.7%; IDDM: 15, 6.0%), and unplanned readmission (nondiabetic: 262, 5.8%; NIDDM: 43, 8.0%; IDDM: 27, 10.8%; Table 2).
Distribution of Postsurgical Outcomes for Patients Undergoing Elective Spinal Surgery by Diabetes Status (N = 5338).a
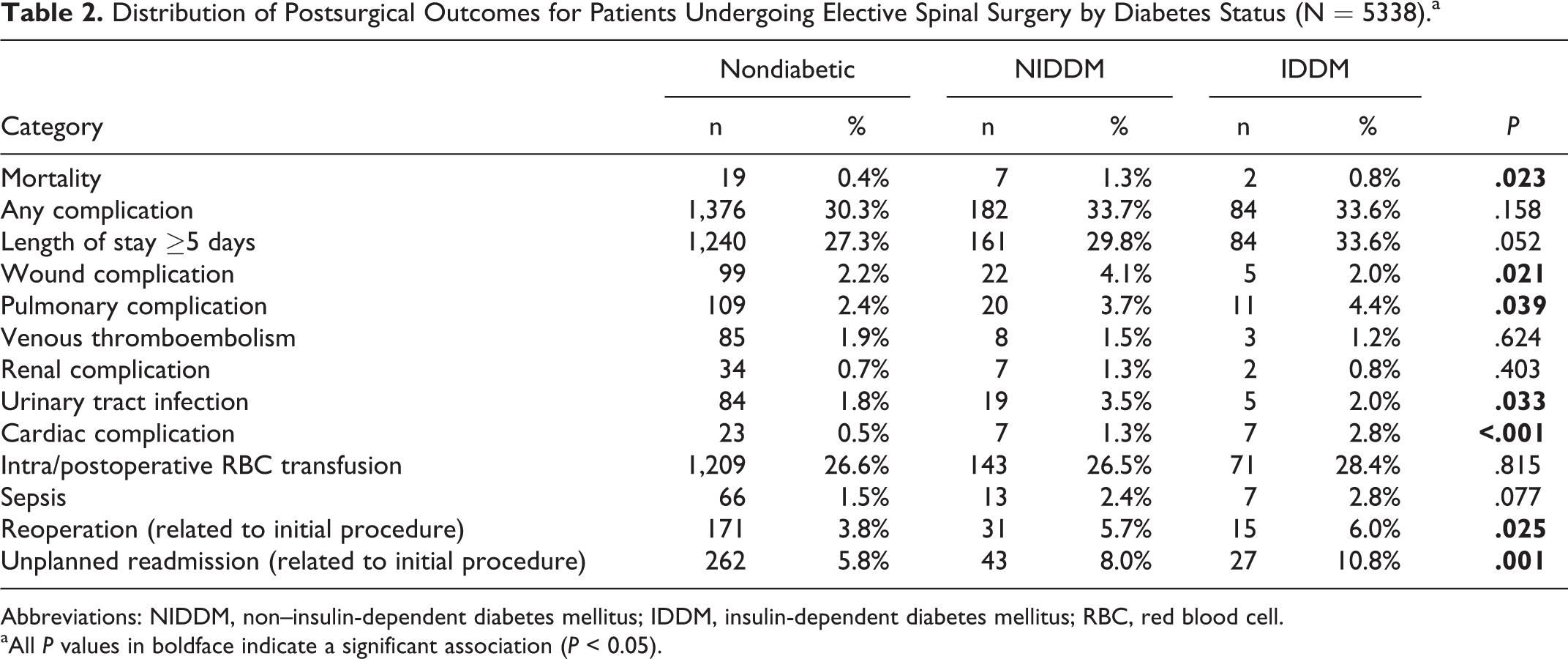
Abbreviations: NIDDM, non–insulin-dependent diabetes mellitus; IDDM, insulin-dependent diabetes mellitus; RBC, red blood cell. aAll P values in boldface indicate a significant association (P < 0.05).
Multivariate Analysis
Multivariate logistic regression analysis revealed diabetes status to be related to several 30-day postoperative complications. Diabetes status was significantly associated with LOS ≥5 days (NIDDM: odds ratio [OR] = 1.27, 95% confidence interval [CI] = 1.02-1.58, P = .034; IDDM: OR = 1.55, 95% CI = 1.15-2.09, P = .004), any complication (NIDDM: OR = 1.26, 95% CI = 1.01-1.58, P = .037; IDDM: 1.27, 95% CI = 0.93-1.74, P = .130), UTI (NIDDM: OR = 1.87, 95% CI = 1.14-3.05, P = .012; IDDM: OR = 0.85, 95% CI = 0.34-2.15, P = 0.737), and cardiac complications (NIDDM: OR = 1.95, 95% CI = 0.83-4.62, P = .127; IDDM: OR = 4.05, 95% CI = 1.72-9.51, P = .001; Table 3).
Thirty-Day Postoperative Outcomes Between Diabetes Cohorts Following Elective ASD Surgery (N = 5809).a
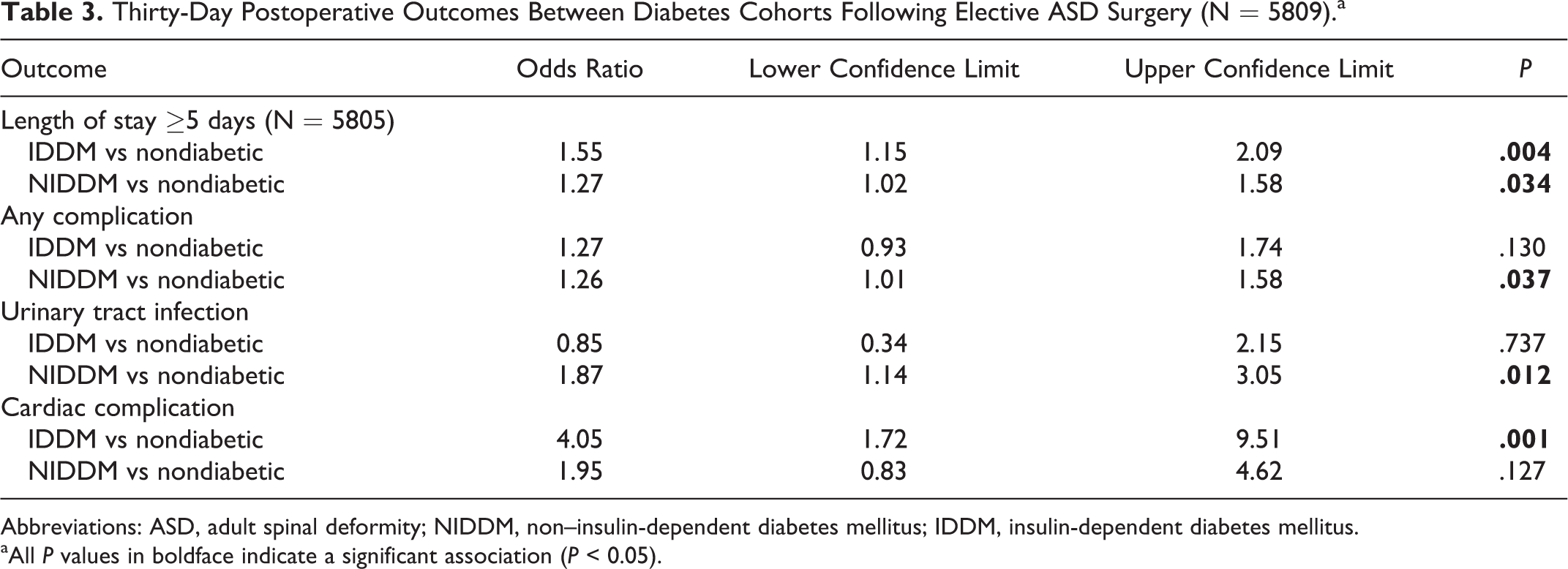
Abbreviations: ASD, adult spinal deformity; NIDDM, non–insulin-dependent diabetes mellitus; IDDM, insulin-dependent diabetes mellitus. aAll P values in boldface indicate a significant association (P < 0.05).
Discussion
This retrospective analysis of the 2010-2014 ACS-NSQIP database found that patients with NIDDM or IDDM were at increased risk for prolonged LOS, any complication, UTI, and cardiac complications following elective ASD surgery. In the study population, 15.8% of the identified patients had DM, a similar rate to a Scoliosis Research Society database study (17.6%) conducted by Shaffrey et al. 24 ACS-NSQIP is a well-established database in the surgical literature and contains risk-adjusted 30-day postoperative complications from over 500 medical centers across the United States. 18 –22,25 The success of quality improvement initiatives based on ACS-NSQIP data has been validated by the decreased mortality rates in the VA system, as well as decreased surgical site infection rates in the private sector. 20,23
Both NIDDM and IDDM patients were at an increased risk for prolonged hospital LOS (≥5 days). LOS following any surgical procedure is of great importance to a patient’s sense of well-being and health care system expenditure. 26,27 At baseline, it costs approximately US$1000 to keep a patient in the hospital per day. 26 –28 Many studies have demonstrated that DM patients experienced longer durations of hospital stay. 2,6,15 Browne et al found that patients with DM experienced a statistically significant increase in hospital LOS following elective lumbar fusion surgery (5.33 days vs 4.96 days, P < .001). 15 Their analysis also revealed that DM patients incurred an additional $1200 inflation-adjusted charges related to their extended hospital stay. 15 In a similar analysis of patients following elective lumbar fusion, Golinvaux et al found both NIDDM and IDDM patients experienced an increased LOS (OR = 1.4 and OR = 1.8, respectively). 6
The current analysis found NIDDM patients were at a 1.26 greater odds of developing any postoperative complication following elective ASD surgery. Considering the systemic nature of DM, patients are often at higher risk for a wide variety of conditions during their postoperative course. 29,30 Notably, our univariate analysis suggests that diabetes (IDDM and NIDDM) is associated with wound complications. However, adjusted multivariable regression analysis reveals that diabetes is not an independent risk factor for wound complications and infection. Infection risk may be related to elevated perioperative glucose level rather than diabetes or the presence or absence of insulin resistance. Olsen and colleagues showed that a preoperative glucose >125 mg/dL or a postoperative glucose >200 mg/dL was associated with higher odds (OR = 3.3) of surgical site infection even in the absence of diabetes. 31 These findings correlate with joint arthroplasty literature, which show elevated preoperative and postoperative glucose on postoperative day 1 are predictors for infection, which was present in patients even without a diagnosis of DM. 32 In addition, on bivariate analysis rates of unplanned reoperation were significantly increased in both NIDDM and IDDM patients, a result supported Puvanesarajah et al, who utilized the PearlDriver database to identify risk factors for reoperation in elderly ASD patients. 33 However, as in our study, on multivariate analysis DM was no longer a significant risk factor for reoperation. 33
Poor glycemic control preoperatively, intraoperatively, or postoperatively has been related to hyperglycemia-induced metabolic abnormalities that contribute to nervous system disorders such as neuropathy, microvascular and macrovascular disease, suppressed immune system due to diminished polymorphonuclear leukocytes, and musculoskeletal changes due to increased collagen cross-linking. 4 Other common conditions associated with DM for patients undergoing orthopedic procedures are wound dehiscence, wound infection, pseudoarthrosis, loss of fracture reduction, hardware and implant failure, myocardial infarction, UTI, ileus, pulmonary embolus, hemorrhage, increased RBC transfusions, increased LOS, and mortality. 4 The level of postoperative glycemic control may affect the occurrence of complications in diabetic patients. 34
NIDDM patients also experienced a 1.87 greater odds of UTI. UTIs are the most common urologic disorder and represent 4% of all outpatient physician visits. 35 A UTI in a diabetic patient is automatically considered a complicated UTI as they experience more frequent and severe UTIs and often have asymptomatic upper track involvement. 36,37 Potential explanations for the increased risk of UTI include glycosuria, impaired immune and leukocyte function, and impaired micturition. 36,37 In the context of joint arthroplasty, Bolognesi et al found patients with DM had a 1.4 greater odds of UTI following either primary total hip arthroplasty or primary total knee arthroplasty. 29 Marchant et al established that patients with either controlled or uncontrolled diabetes were also at risk for increased urinary tract infections (OR = 1.245 and OR = 2.476, respectively) following total joint arthroplasty. 30
IDDM patients were more than 4 times more likely to develop cardiac complications. Diabetes is associated with microvascular and macrovascular disease, which contributes to the development of neuropathy, nephropathy, retinopathy, coronary artery disease, cerebrovascular disease, stroke, peripheral artery disease, and lower extremity infection and amputation. 4,38 Subsequently, diabetic patients have a 2- to 4-fold increase in cardiovascular disease including stroke, coronary artery disease, and hypertension. 38 IDDM patients may be at greater risk of cardiac complications compared to NIDDM patients due to their absolute insulin deficiency and greater potential risk of hypoglycemia-induced arrhythmias. 39
Cho et al performed a matched retrospective cohort analysis of 46 patients (23 NIDDM and 23 control) on single-institution data over a 25-year period. 34 Their analysis concluded there was no difference in minor or major complications between NIDDM and nondiabetic patients. These difference in results may arise for several reasons. The sample of patients analyzed in the present study is much larger, providing greater power to detect differences in postoperative complications. In addition, the present study evaluated both NIDDM and IDDM patients. Finally, the way postoperative complications were defined differs greatly between studies, with Cho et al classifying complications as minor or major while the present study evaluated each complication separately. Mortality, any complication, unplanned readmission, unplanned reoperation, extended LOS, renal complications, and intra-/postoperative RBC transfusion were also only evaluated in the present study. It should be noted that Cho et al excluded patients with less than 2 years of postoperative follow-up, a significantly longer length of follow-up than performed in this study, which may provide for a more accurate detection of postoperative complication rates.
The difference in acute postoperative outcomes between NIDDM and IDDM patients suggests that a binary designation of diabetic versus nondiabetic is inadequate to meaningfully assess outcomes, as these patient populations may be more dissimilar than previously assumed. 6 Additionally, previous studies have evaluated the utility of creating patient cohorts depending on level of glycemic control among diabetic patients. 16,17,30 Future studies may consider creating cohorts depending on NIDDM and IDDM and performing subgroup analysis for level of glycemic control.
There are several limitations for this study. The ACS-NSQIP database classifies cases based on CPT codes. However, differences between procedural techniques, such as type of osteotomy or pelvis fixation, cannot be accounted for using this modality. Additionally, differences in postoperative anticoagulation protocol across institutions as well as Foley catheter placement are potentially confounding variables that are not captured by the ACS-NSQIP database. ACS-NSQIP also significantly overrepresents academic medical centers and therefore may not be fully representative of all US hospitals. Contributing hospital is kept anonymous, limiting the ability to adjust for institution size, patient volume, academic affiliation, and surgeon experience. Additionally, long-term complications are not captured in the ACS-NSQIP database, which only evaluates complications up to 30-days postoperatively, leading to a potential underestimation of risk. ACS-NSQIP does not collect data on patient blood glucose or HbA1c, thus limiting adjustment for well-controlled versus poorly controlled diabetes. Finally, while not a limitation but a necessary distinction, patients were classified as nondiabetic, NIDDM or IDDM, not as nondiabetic, type 1 or type 2 diabetic.
Despite these limitations, this is the first national study to evaluate the effect NIDDM and IDDM have on acute postoperative outcomes following elective ASD surgery. The analysis found NIDDM to be a risk factor for hospital LOS ≥5 days, any complication, and UTI. Additionally, the study found IDDM to be a risk factor for hospital LOS ≥5 days and cardiac complications. The authors hope the results of this study be used by health care teams to improve patient risk stratification and initiate proper safety efforts for these 2 populations of diabetics.
Footnotes
Authors’ Note
This study was qualified as exempt by the Mount Sinai Hospital Institutional Review Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.