
Abstract
Study Design:
Retrospective review of prospectively collected spinal surgery and transfusion databases.
Objectives:
To evaluate the efficacy of a care pathway developed at our institution since 2003 with a focus on reducing the need for blood transfusions in children undergoing scoliosis correction surgery. The care pathway includes nurse-led clinics facilitating preoperative hemoglobin optimization, intraoperative cell salvage, the use of tranexamic acid, and a transfusion criteria awareness program.
Methods:
Retrospective review of our institution’s prospectively recorded spinal surgery and transfusion databases including all cases of scoliosis surgery in patients 18 years and younger between 2001 and 2015.
Results:
A total of 1039 procedures were included in the analysis. Overall, 24.4% of patients received a transfusion. The proportion of patients transfused was 89.2% in 2001-2003, 39.6% in 2004-2006, 16.5% in 2007-2009, 15.6% in 2010-2012, and 20.1% in 2013-2015. The volume of blood products transfused in those undergoing transfusion was 9.1 units in 2001-2003, 4.8 units in 2004-2006, 5.0 units in 2007-2009, 2.3 units in 2010-2012, and 2.1 units in 2013-2015. A multivariate logistic regression demonstrated adjusted odds ratios for the probability of receiving any transfusion of 5.45 (95% confidence interval 3.62-8.11) for patients with neuromuscular diagnoses and 11.17 (5.02-24.86) for those undergoing combined anterior and posterior surgical approach.
Conclusions:
We have demonstrated over a 15-year period that the introduction of a multifaceted, multidisciplinary pathway can dramatically and sustainably reduce the need for blood transfusions and their attendant risks in pediatric scoliosis surgery. This data lends weight to the adoption of such a care pathway in pediatric scoliosis surgery.
Introduction
Pediatric scoliosis surgery for both idiopathic and neuromuscular curves has historically been associated with large volumes of perioperative blood loss. 1 Scoliosis surgery can involve prolonged operative times with often extensive soft tissue dissection and bone cutting. 2 Historically up to 59% of children undergoing scoliosis surgery have received allogenic blood transfusions in the perioperative period. 3 Though the risk of transmission of blood borne viruses such as human immune deficiency virus and hepatitis C virus have decreased significantly with the increased security of the blood supply, 4 other risks of allogenic blood transfusion remain. Transfusion induced immunomodulation can increase the risk of postoperative infection. 5 Transfusion-related acute lung injury and mistransfusion, though rare, are associated with significant morbidity and mortality. 6 Allogenic blood transfusion is a costly treatment both financially (the cost in the UK National Health Service of a unit of red blood cells has increased from £78 in 2000 to £125 in 2011) and in the utilization of a scarce resource. 7,8
Multiple interventions have been employed to reduce the need for allogenic blood transfusions in scoliosis surgery. 9 These can be divided into preoperative interventions, including hemoglobin optimization (using hematinics and erythropoietin) and autologous blood donation. Intraoperative interventions include hypotensive anesthesia, cell salvage and retransfusion, antifibrinolytic administration 2 and appropriate surgical techniques. Postoperative interventions include acceptance of lower hemoglobin levels without triggering transfusion. 7
Since 2001, our unit has adopted a multifaceted, multidisciplinary blood conservation integrated care pathway program involving the introduction of some of these techniques with the objective to reduce allogenic blood transfusion rates. The goal of our study was to review the allogenic transfusion rates and transfusion volumes over the 15-year period since the introduction of the care pathway and analyze factors associated with an increased risk of transfusion.
Methods
Our pediatric spinal surgery service began in 2000 and covers a tertiary referral population of 4.5 million. Initially, the service was run by 2 surgeons: 1 with 3 years prior experience and 1 new into practice. Since 2000, the service has included 6 different surgeons and currently employs 3 surgeons. Beginning in 2003, we developed a multifaceted program aiming to reduce allogenic blood transfusion rates in children undergoing scoliosis surgery (Figures 1 and 2). In 2003, cell salvage and aprotonin administration were introduced for all scoliosis surgeries. In 2007, a nurse-led optimization clinic was introduced to review all preoperative patients with hematinics and erythropoietin administered as required to meet a target preoperative hemoglobin level of 125 g/L. This target was chosen based on a previous local review that identified this cutoff as predictive of the need for postoperative transfusion. 10 In 2007, because of safety concerns, aprotonin usage was stopped and replaced with tranexamic acid. Intravenous tranexamic acid has since been used with a present dosage regime of a loading dose of 30 mg/kg followed by a 1 mg/kg/h infusion continued until skin closure. All patients receive moderate hypotensive anesthesia 11 and appropriate positioning to reduce abdominal compression, including the usage of a Jackson table. A transfusion awareness program was developed in 2009 to educate all health care professionals about strategies to minimize perioperative blood transfusion. Transfusion triggers were introduced in 2009: A postoperative hemoglobin threshold of 80 g/L in patients with clinical symptoms of anemia is used to consider transfusion and 70 g/L in those without clinical symptoms. Any decision to transfuse a patient must be made by a senior decision maker (consultant surgeon or anesthetist).
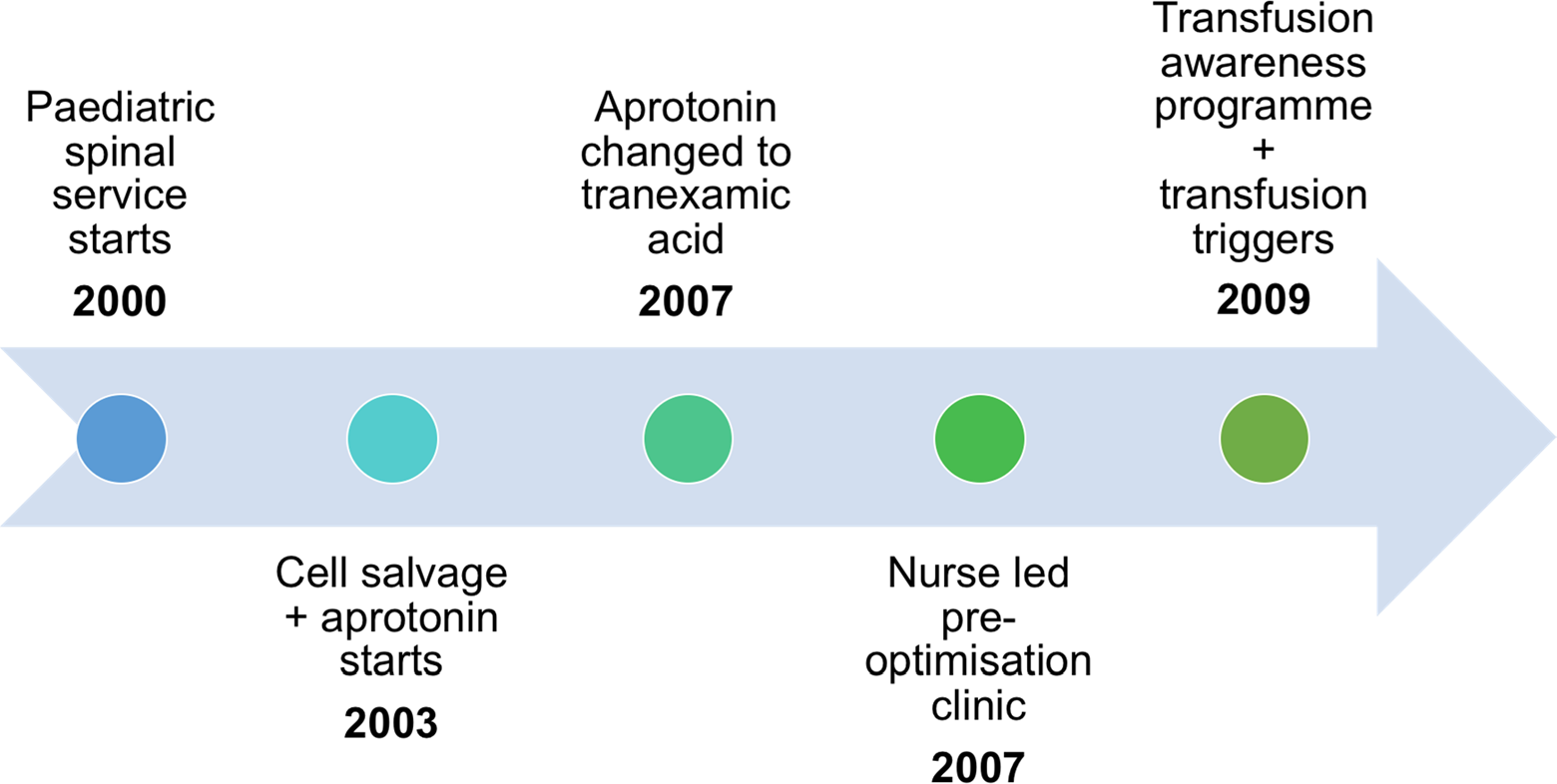
Summary of transfusion reduction interventions.
Timeline for transfusion reduction interventions.
Our institution maintains a prospectively recorded spinal surgery database and transfusion department database. A retrospective review was undertaken of both databases to include all patients aged 18 years or younger undergoing scoliosis correction surgery between January 2001 and December 2015. Six surgeons undertook the procedures with surgical techniques evolving throughout the 15-year period. All patients underwent wide facetectomies, less than 5% underwent osteotomies, and less than 5% had postoperative wound drains (routine usage stopped in 2004).
Data analyzed included patients’ demographics, underlying diagnosis, surgical approach, preoperative and lowest postoperative hemoglobin within 7 days of surgery, transfusion rates, and volumes of red blood cells and other blood products transfused. The 15-year period studied was divided into five 3-year periods for the purposes of comparison and analysis.
The collected data were analyzed using STATA version 14.0. 12 Univariate and multivariate logistic regressions were performed to identify associations between variables yielding odds ratios (OR), adjusted OR, 95% confidence intervals (CI), and P values. Trend (P trend) was calculated using linear regression. All tests were 2-sided, with a P value of less than .05 indicating statistical significance.
Results
Between January 2001 and December 2015, a total of 1039 scoliosis correction procedures were performed (Table 1). The median age at surgery was 14.0 years (interquartile range 13-16). Of these, 705 (67.9%) patients were female and 334 (32.2%) were male. Overall, 629 (61.1%) procedures were for idiopathic scoliosis, 400 (38.9%) for scoliosis associated with underlying neuromuscular diagnoses (NMS). The posterior approach was used in 797 cases (80.3%), anterior in 125 (12.6%), combined anterior and posterior (including staged) in 71 (7.2%).
Baseline Characteristics of the Cohort (n = 1039).
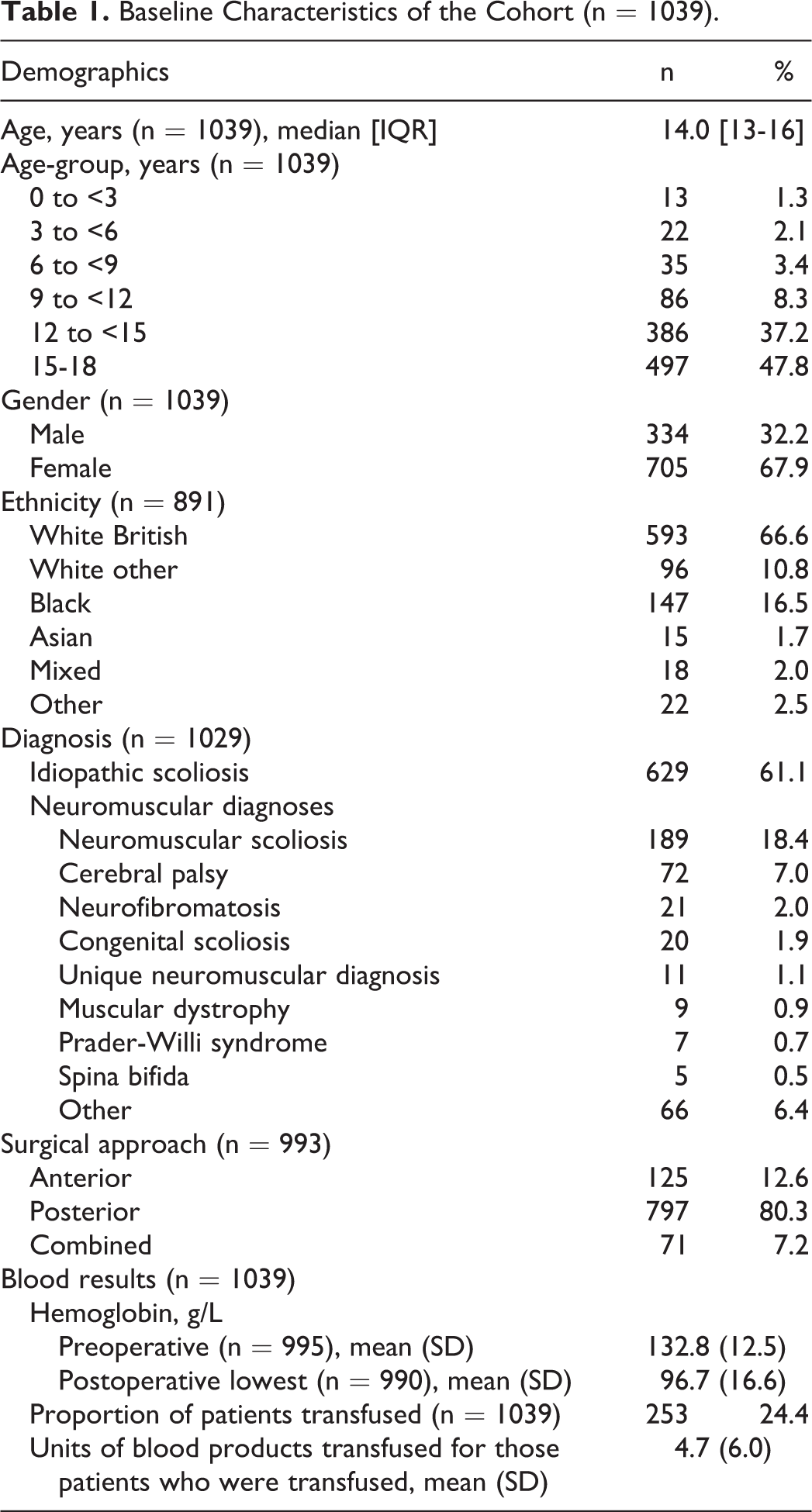
Overall, 253 patients (24.4%) received a blood transfusion with a mean transfusion volume of 4.7 units (SD 6.0). Full demographics of the cohort can be found in Table 1. Mean (SD in parentheses) preoperative hemoglobin was 133.8 g/L (13.5) in 2001-2003, 135.4 g/L (12.8) in 2004-2006, 132.5 g/L (12.9) in 2007-2009, 131.9 g/L (13.1) in 2010-2012, and 132.7 g/L (11.4) in 2013-2015.
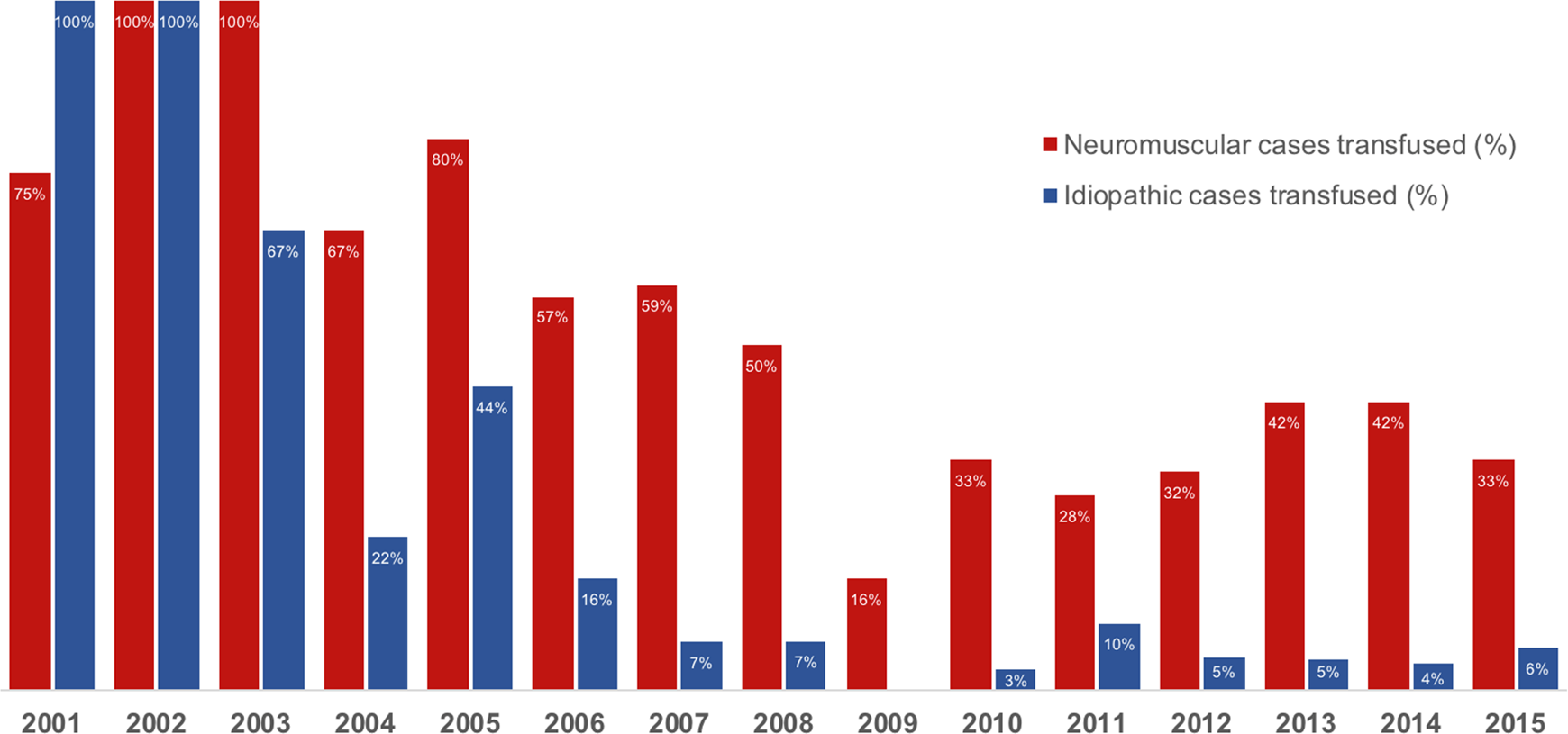
The proportion of patients transfused was 89.2% in 2001-2003, 39.6% in 2004-2006, 16.5% in 2007-2009, 15.6% in 2010-2012, and 20.1% in 2013-2015 (Table 2). Figure 3 demonstrates the proportion of patients transfused per year by diagnostic category. The volume of blood products transfused in those undergoing transfusion was 9.1 units in 2001-2003, 4.8 units in 2004-2006, 5.0 units in 2007-2009, 2.3 units in 2010-2012, and 2.1 units in 2013-2015.
Demography, Surgical Approach, and Proportion of Patients Receiving a Transfusion From 2001 to 2015 in 3-Year Periods.
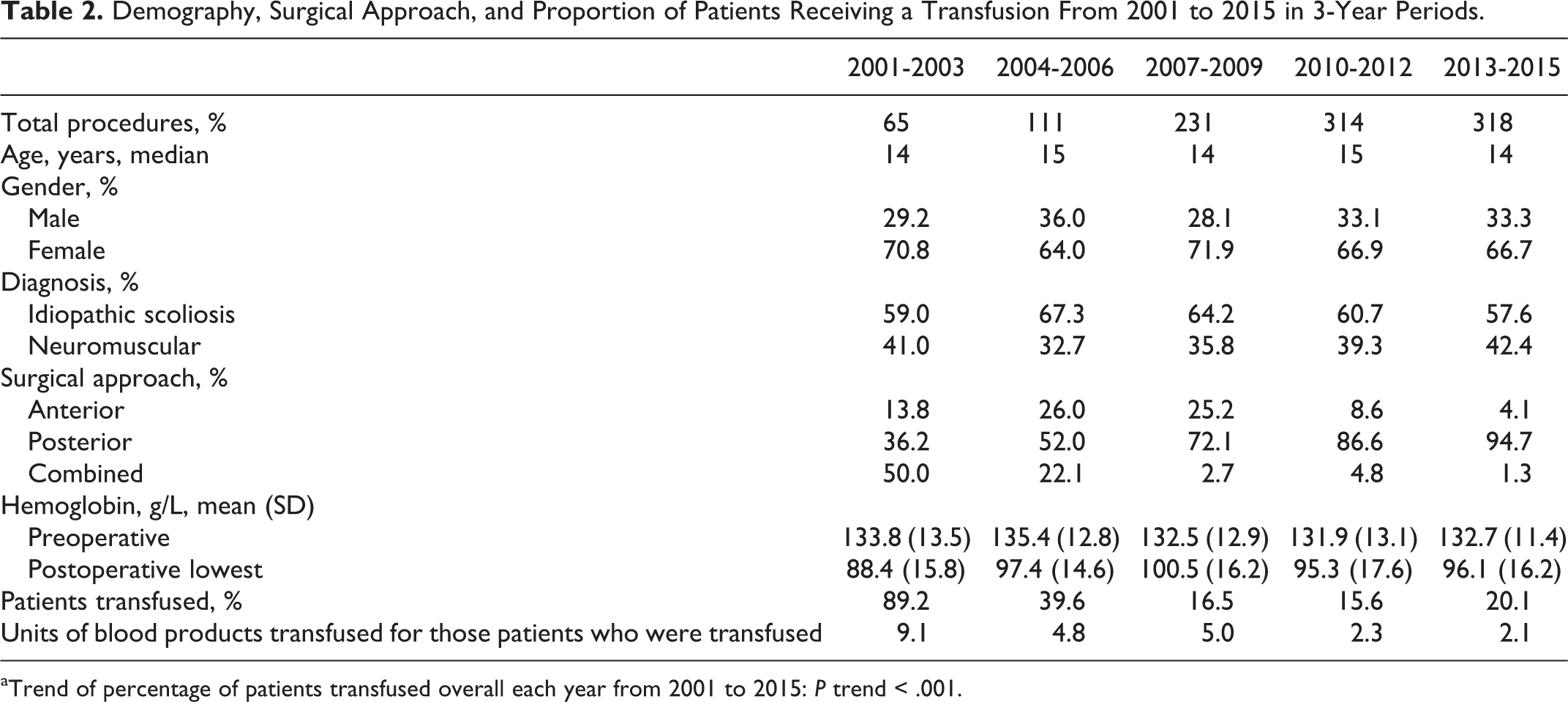
aTrend of percentage of patients transfused overall each year from 2001 to 2015: P trend < .001.
Proportion of patients transfused per year by diagnostic category, 2001-2015.
Age, female gender, “white other” ethnicity, neuromuscular diagnoses, and nonanterior surgical approach were significantly associated with an increased likelihood of transfusion in the univariate model (Table 3). After adjustment, “white other” ethnicity remained associated. Black ethnicity was also associated with an increased likelihood of blood transfusion in the multivariate model.
Univariate and Multivariate Logistic Regression of Demographic and Surgical Characteristics Associated With the Probability of Receiving Any Blood Transfusion Between 2001 and 2015.
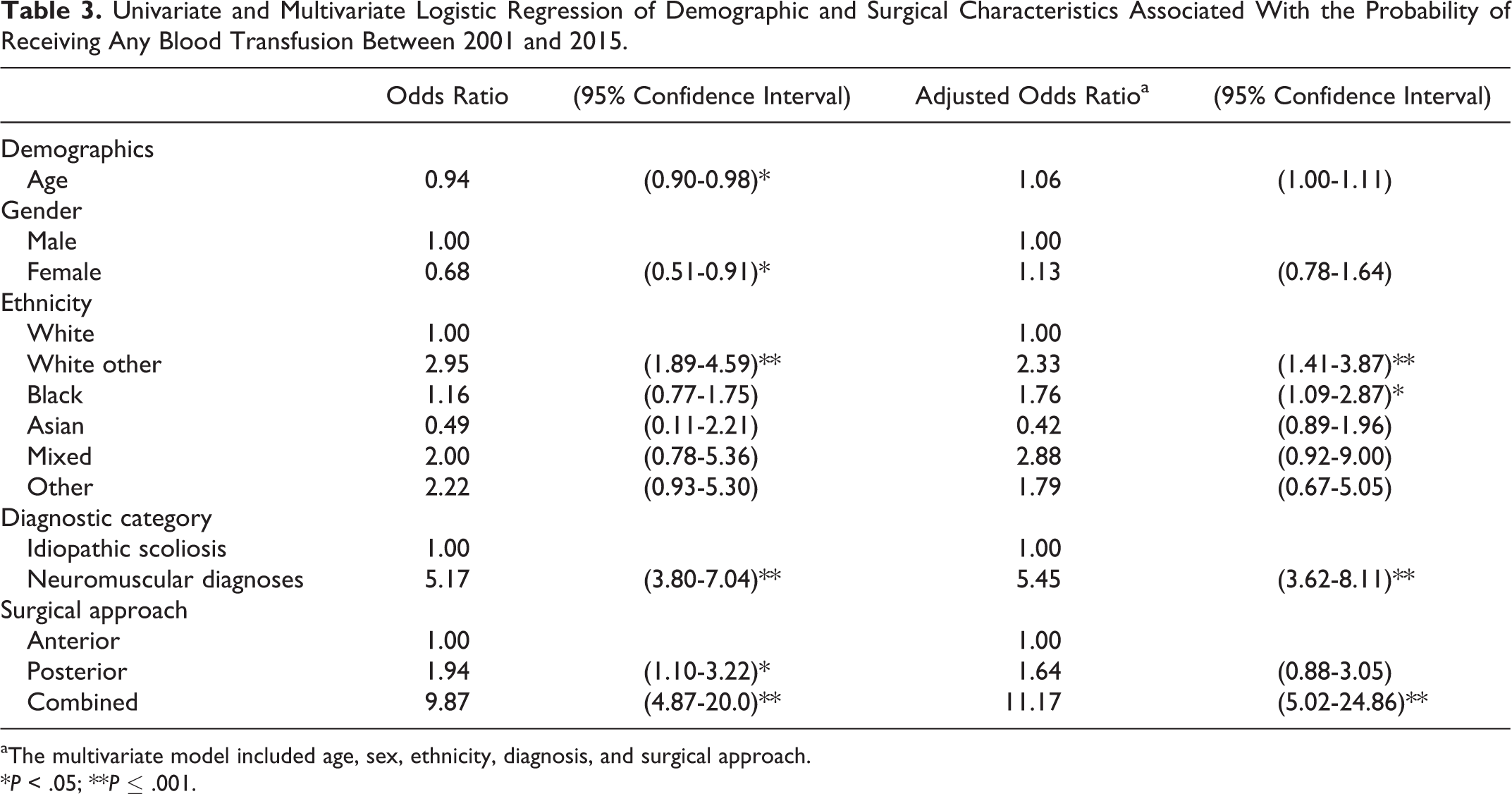
aThe multivariate model included age, sex, ethnicity, diagnosis, and surgical approach.
*P < .05; **P ≤ .001.
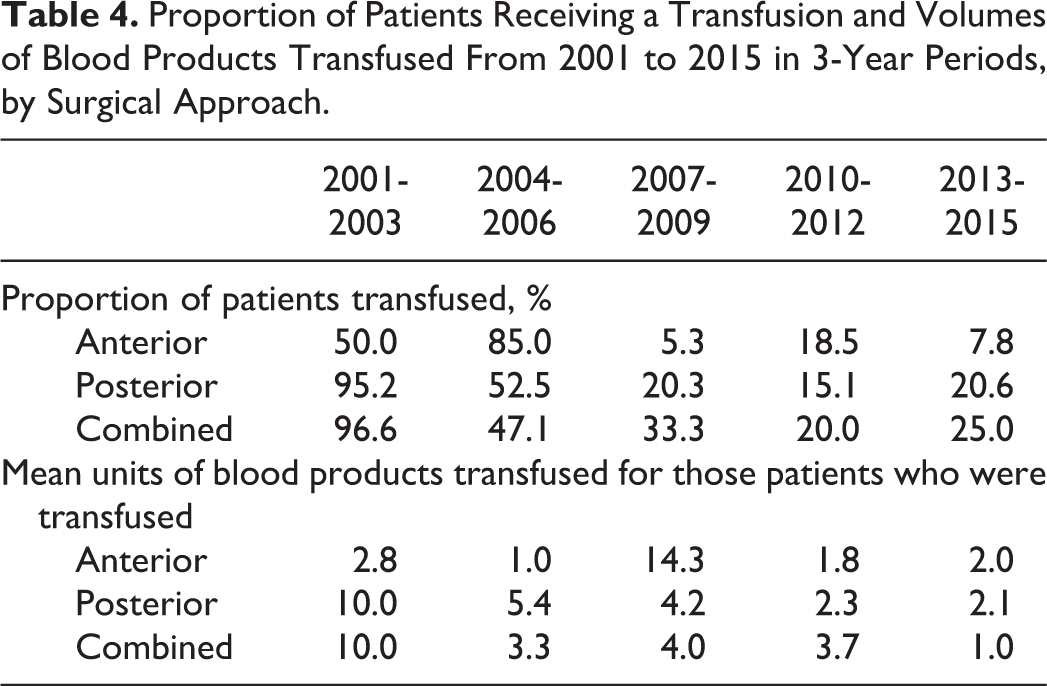
Patients undergoing procedures for neuromuscular diagnoses were approximately 5 times more likely to receive a blood transfusion in both the univariate and multivariate regressions (adjusted OR 5.45, 95% CI 3.62-8.11). Posterior approach was associated with higher transfusion likelihood but this association was not significant in the multivariate model. Combined surgical approach was associated with an approximately 10-fold likelihood of transfusion before and after adjustment (adjusted OR 11.17, 95% CI 5.02-24.86). Sub group analysis by surgical approach demonstrated a downward trend in proportion transfused and mean volume transfused across all approaches between 2001-2003 and 2013-2015 (Table 4).
Proportion of Patients Receiving a Transfusion and Volumes of Blood Products Transfused From 2001 to 2015 in 3-Year Periods, by Surgical Approach.

Descriptive analysis and univariate regression of the diagnoses demonstrated that unique neuromuscular diagnoses, cerebral palsy, neuromuscular scoliosis, and congenital scoliosis were strongly associated with an increased likelihood of transfusion (Table 5); additionally, all patients (n = 4) with muscular dystrophy received a transfusion.
Univariate Logistic Regression of Diagnosis and the Proportion of Patients Receiving Any Blood Transfusion Between 2001 and 2015.
*P < .05; **P ≤ .001.
Discussion
The aim of our study was to determine whether our unit’s allogenic blood transfusion rate had reduced following the introduction of a blood conserving integrated care pathway for children undergoing scoliosis surgery. We report a significant reduction in allogenic transfusion rates from approximately 90% of patients receiving a transfusion at the start of the program to approximately 20% most recently. Several reports exist in the literature regarding reducing allogenic blood transfusion rates with the use of various blood conservation techniques in small cohorts. Verma et al 13 reported on the introduction of a blood transfusion reduction policy resulting in an allogenic transfusion rate of 5% in 38 patients with adolescent idiopathic scoliosis (AIS). Berney et al 14 reported a reduction from a 56% allogenic transfusion rate to a 0% transfusion rate in an AIS cohort of 56 patients with the usage of tranexamic acid. Hassan et al 15 reported in 2011 on their 2-year experience with 104 patients with blood conservation measures similar to ours and report a 36% transfusion rate in NMS and 1.7% in AIS. 15 To our knowledge, our study is the first to evaluate a blood conservation program in a large cohort (>1000 patients).
We note an especially marked reduction in transfusion rates in patients with AIS. Blood loss is known to be considerably higher in patients with NMS as compared with AIS. 1 Shaipro et al 16 reported a 75% and 94% transfusion rate in patients with Duchenne muscular dystrophy undergoing scoliosis surgery with and without tranexamic acid, respectively. Meert et al 3 reported an overall allogenic transfusion rate of 59% in a mixed scoliosis cohort of 107 patients with underlying neuromuscular disease a predictor of increased transfusion requirements. We report a reduction from 96.0% in 2001-2003 to 39.6% in 2013-2015 in NMS patients compared with 86.1% in 2001-2003 to 4.9% in 2013-2015 in AIS patients. These results are broadly similar to those reported by Hassan et al. 15 In 2013-2015, we note an increase in the transfusion rate for NMS patients from 30.9% to 39.6%, while in the same time period, the rate for AIS patients continued to decline from 5.8% to 4.9%. This could be due to an increasingly challenging surgical caseload with surgical intervention being undertaken in patients not previously considered surgical candidates.
Our integrated care pathway includes a range of interventions, all aimed at reducing allogenic blood transfusion rates. The cumulative effect of all the interventions is seen in our results; establishing specifically which are responsible for the benefits seen is not possible in a retrospective study. The greatest reduction in transfusion rate was seen between 2001-2003 and 2004-2006, which followed the introduction of aprotonin and cell salvage. These results suggest that aprotonin (later tranexamic acid) and cell salvage may be particularly effective in reducing transfusion rates. There is an extensive evidence base for the benefits of tranexamic acid in reducing intraoperative blood loss. 16 -21 A recent meta-analysis by Yuan et al 2 demonstrated a significant reduction in total blood loss after scoliosis surgery with tranexamic acid (though no reduction in the need for transfusion). The optimal dosing of intravenous tranexamic acid remains unclear. Grant et al 22 found a trend toward reduced transfusion requirements in a small pediatric scoliosis cohort using high dose (20 mg/kg loading dose, 10 mg/kg/h infusion) as opposed to lower dose (10 mg/kg loading dose, 1 mg/kg/h infusion). There may be a role for topical tranexamic acid administration—a recent systematic review found limited though promising evidence for reducing blood loss in spinal surgery. 23
Evidence for the benefits of cell saver usage in scoliosis surgery remains unclear. A Cochrane systematic review in 2010 demonstrated cell saver usage to reduce allogenic transfusion rates though this was in adults and included elective cardiac surgery as well as other nonspinal orthopedic procedures. 24 There are conflicting reports of the benefits in terms of reducing allogenic blood transfusion requirements with cell saver usage. 25 -29 The usage of a low transfusion threshold has been shown to result in a significant reduction in risk of blood transfusion with no evidence of an increase in associated morbidity and mortality. 30
We have not adopted the usage of autologous blood transfusion in our integrated care pathway. Concerns remain about the risk of transmission of bacterial infection 31 and the evidence remains conflicted as to its role in reducing allogenic transfusion. 32,33
Limitations
The limitations of the study are typical of those expected in retrospective studies. The quality of the data is reliant on that recorded prospectively in the databases and some demographic data were incomplete in our dataset. There is no simultaneous control group as all patients were enrolled in the blood conservation integrated care pathway. It is not possible to control for potential confounders such as improved surgical technique and decreased operative time as surgical experience developed over the period studied.
Conclusion
Our study shows that using simple blood conservation methods can dramatically and sustainably reduce the need for allogenic blood transfusions and their attendant risks and costs in pediatric scoliosis surgery. These results lend weight to the adoption of such measures in pediatric scoliosis surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.