
Abstract
Study Design
Narrative review.
Objective
To provide an overview on the diagnosis, natural history, and nonoperative and operative management of ossification of the posterior longitudinal ligament (OPLL). OPLL is a multifactorial condition caused by ectopic hyperostosis and calcification of the posterior longitudinal ligament. Familial inheritance and genetic factors have been implicated in the etiology of OPLL. The cervical spine is most commonly affected followed by the thoracic spine. The clinical manifestations range from asymptomatic to myelopathy or myeloradiculopathy.
Methods
Using PubMed, studies published prior to October 2014 with the keywords “OPLL, etiology”; “OPLL, genetics”; “OPLL, spinal cord injury”; “OPLL, natural history”; “OPLL, non-surgical management”; OPLL, surgical management”; “OPLL, surgical complications” were evaluated.
Results
The review addresses the etiology, epidemiology, classification, clinical presentation, imaging findings, and nonoperative and operative management of OPLL. Complications associated with surgical management of OPLL are also discussed.
Conclusions
OPLL commonly presents with myelopathy and radiculopathy. Spine providers should consider OPLL in their differential diagnosis and when reviewing images. If surgical intervention is pursued, imaging-based measurements and findings can help in choosing an anterior versus posterior surgical approach.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is a hyperostotic condition that results in ectopic calcification of the posterior longitudinal ligament. 1 Although most of the studies on OPLL are from East Asia, OPLL can be encountered in any patient population. We performed this review to update spine surgeons on the current state of the art on the etiology, diagnosis, and management of OPLL. PubMed was used to conduct electronic searches for studies published prior to October 2014 with the following key works: “OPLL, etiology”; “OPLL, genetics”; “OPLL, spinal cord injury”; “OPLL, natural history”; “OPLL, non-surgical management”; OPLL, surgical management”; “OPLL, surgical complications.”
Etiology
The pathogenesis of OPLL is poorly understood. Some have suggested it is a variant of diffuse idiopathic skeletal hyperostosis. 2 A multifactorial etiology has been suggested due to associations with both genetic and environmental factors. 3 Familial inheritance (genes including BMP4, BMP9, and COL6A1) has been associated with the development of OPLL. 3 , 4 , 5 A recent genomewide association study comparing 1,130 patients with OPLL and 7,135 controls found six loci to be more frequent in patients with OPLL than controls. 6 HAO1A was the gene most commonly associated with OPLL in this study. It is a gene commonly expressed in the liver and pancreas. Further analysis of the loci indicates HAO1, RSPO2, and CCDC91 may promote OPLL via endochondral ossification. Meanwhile, the genes RSPH9 and STK38L may promote OPLL via membranous ossification. There are no other known systemic manifestations of OPLL, although some studies have noted increased bone mineral density in patients with OPLL. 7
Classification
The most common classification of cervical OPLL is from the Investigation Committee on OPLL of the Japanese Ministry of Health and Welfare. A lateral radiograph is used to classify OPLL into four subtypes: continuous, segmental, mixed, and localized or other.8 The continuous type is an ossified mass that spans several vertebral bodies and the intervening disk spaces (Fig. 1). The segmental type involves ossification behind each vertebral body (Fig. 2). The mixed type is a mixture of both continuous and segmental types. The localized or other type has been described as a variant pattern such that the ossification is localized to the intervertebral disk space without involvement of the vertebral body. The mixed and continuous types are most frequently associated with progression to myelopathy. A recent study of ligamentum flavum taken from patients undergoing surgery for cervical OPLL revealed differences in osteogenic differentiation based upon the classification of OPLL. Increased bone morphogenetic protein-2 (BMP-2) expression was noted in continuous and mixed types in comparison with less BMP-2 expression in the segmental and other types. 9 Additional studies are needed to determine if the increased BMP-2 expression in the continuous and mixed types of OPLL can result in future progression of OPLL even after decompression surgery.
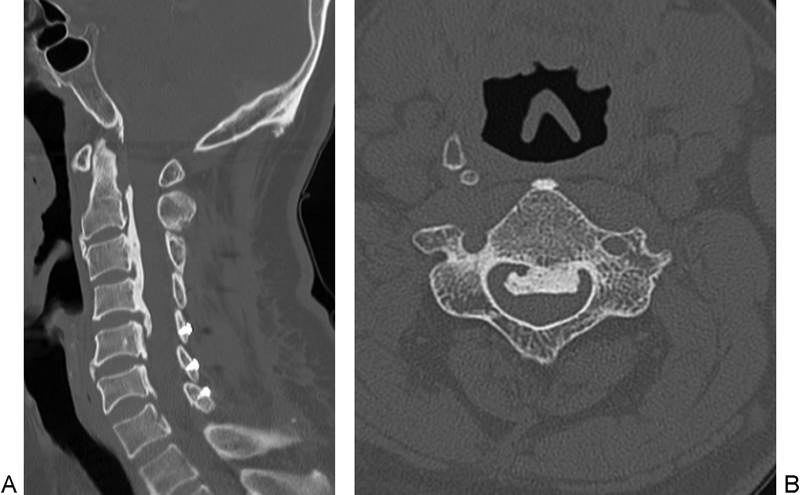
(A) Sagittal computed tomography (CT) demonstrating continuous ossification of the posterior longitudinal ligament (OPLL) from C2 to C4. (B) Axial CT of C3 vertebral body demonstrating a continuous OPLL.
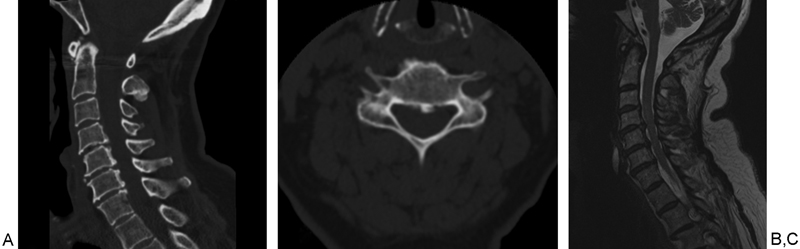
(A) Sagittal computed tomography (CT) demonstrating segmental ossification of the posterior longitudinal ligament (OPLL) at C5 and C6. (B) Axial CT demonstrating segmental OPLL. (C) Sagittal T2-weighted magnetic resonance imaging demonstrating the segmental OPLL at C5 and C6.
OPLL of the thoracic spine is further subclassified as flat or beak type (Fig. 3). The beak type is a segmental OPLL with a sharp protrusion behind the disk space. 10 The flat type is either continuous or mixed OPLL with a flat shape.
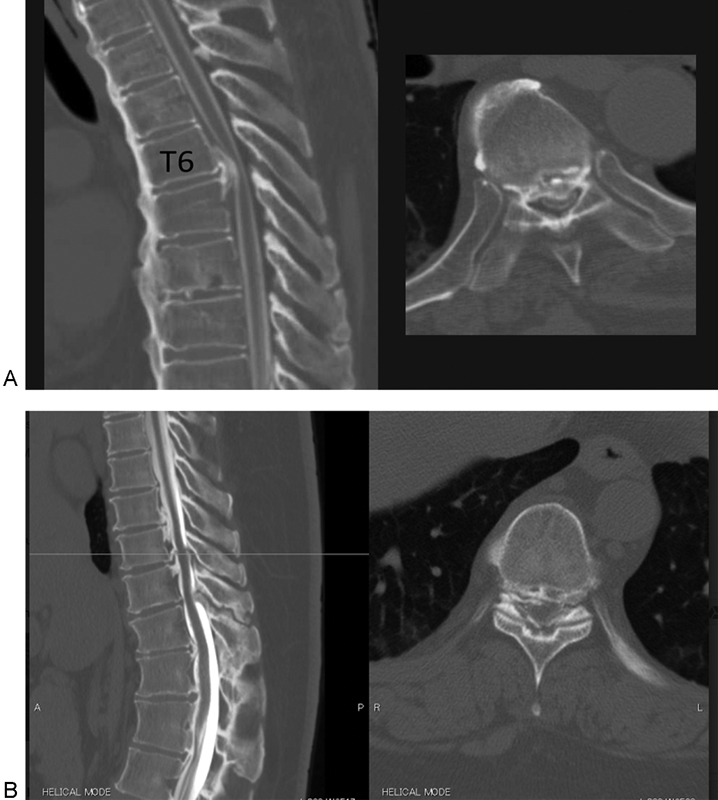
(A) Sagittal and axial computed tomography (CT) of the thoracic spine demonstrating beak ossification of the posterior longitudinal ligament (OPLL) in a patient with diffuse idiopathic skeletal hyperostosis. (B) Sagittal and axial CT of the thoracic spine demonstrating flat OPLL. (Images courtesy of Hideki Murakami, MD, Kanazawa University, Kanazawa, Japan.)
Epidemiology
OPLL is traditionally thought to be more common in Japan with a prevalence of 2 to 4% as compared with 0.01 to 2% in non-Asian populations.11 Among patients with myelopathy, the prevalence of OPLL is 27% in Japan and 20 to 23% in the United States. 12 OPLL commonly presents in the fifth or sixth decade, and a male-to-female ratio of 2:1 has been reported. 13 OPLL of the cervical spine is more common than thoracic OPLL, which was confirmed in a survey of 1,058 patients with OPLL, of whom 3.2% demonstrated involvement of the cervical spine and 0.8%, the thoracic spine. 14
Clinical Presentation
A careful history and physical are important in diagnosing OPLL. Although 5% of diagnosed patients are asymptomatic, varying degrees of neurologic symptoms can be present including both radiculopathy and myelopathy. 14 Myelopathy is caused by a decrease in the space available for the spinal cord due to the OPLL. The severity of myelopathy symptoms may be exacerbated by coexisting congenital cervical stenosis. Patients with myelopathy often give a history of changes in balance and fine motor skills (worsening handwriting, difficulty buttoning buttons). As myelopathy progresses, patients may require ambulatory aids or a wheelchair. During the physical examination, the clinician should assess both the Rhomberg and tandem gait tests to identify early signs of gait or balance dysfunction. Brisk reflexes as well as clonus may be present in the upper and lower extremities. Pathologic reflexes such as Hoffman reflex and the inverted radial reflex suggest an upper motor neuron lesion. A hyperactive scapulohumeral reflex can be seen with cord compression above C3. 15 Dysdiadochokinesia or difficulty with rapid supination and pronation of the hand can be found in myelopathy. In some cases of OPLL, the patient may complain of radicular symptoms and may demonstrate radicular signs such as a positive Spurling test.
The rate of progression of symptoms in OPLL has been linked to the age at presentation. Presentation in the fourth decade or younger is associated with progressively symptomatic OPLL and subsequent myelopathy. Presentation in the fifth and sixth decades is less frequently associated with progression to myelopathy. 16 , 17 , 18
Spinal Cord Injury and OPLL
OPLL and the subsequent cervical stenosis can predispose to spinal cord injury (SCI) following minor trauma (Fig. 4). In a series of 106 patients with OPLL and cervical SCI, 88.7% (94/106) suffered a central cord syndrome and did not have a concurrent fracture. 19 The average age was 66 years and the most common mechanism was a fall (74%). Only 25% of the patients were previously aware that they had OPLL. In a smaller series of patients (n = 28) with OPLL and cervical SCI, the average age was 63 years and 61% were due to a ground-level fall. 20 Eight patients had a continuous type of OPLL, 6 had a mixed type, and 14 had a segmental type. The authors noted that in the group with continuous OPLL, SCI occurred at the caudal end of the OPLL analogous to an ankylosed spine. In the segmental OPLL group, SCI occurred most commonly at the disk level. With segmental OPLL, a hyperextension mechanism can cause compression of the spinal cord and subsequent SCI.
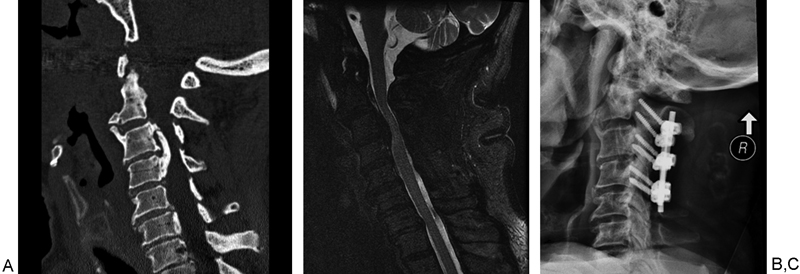
An 82-year-old-man involved in a motor vehicle collision presented with left upper and lower extremity weakness. (A) Sagittal computed tomography demonstrated a mixed type of ossification of the posterior longitudinal ligament (OPLL; continuous at C3–C4 and segmental at C5). (B) Sagittal T2 fat-suppressed sequence demonstrated cord signal change predominantly on the left side. (C) The patient underwent an urgent laminectomy of C3 to C4 with instrumented posterior spinal fusion C2 to C4.
Risk factors for OPLL and SCI were recently reported in a study comparing 34 patients with OPLL and SCI to 32 patients with OPLL and cervical myelopathy. 21 Ground-level falls (79%) were the most common risk factor. The OPLL and SCI group was significantly older than the OPLL and cervical myelopathy group (71.5 versus 63.3 years, p < 0.02). Ossification of the anterior longitudinal ligament demonstrated by CT was present in 56% of the OPLL and SCI group, whereas only 22% of the OPLL and cervical myelopathy group had ossification of the anterior longitudinal ligament (p < 0.002). Thus, patients with OPLL and SCI tend to be older and have ossification of the anterior longitudinal ligament.
Imaging Diagnosis
Radiographs are helpful in the diagnosis of OPLL, particularly when located in the cervical region. However, low inter- and intraobserver reliability for diagnosing OPLL with radiographs has been demonstrated as compared with computed tomography (CT). 22 CT scan sagittal sequences can help classify the type of OPLL and have been associated with higher intraobserver reliability than radiographs. 22 The axial sequences localize the lesion to a central or paracentral location, which can aid in the preoperative planning. Some groups have used three-dimensional CT to quantify the volume of OPLL as well as for classification purposes. 23
Dural ossification can be detected using a bone window on CT scans. Dural defects are associated with the nonsegmental type of OPLL. 5 The double-layer and single-layer signs on CT indicate OPLL penetration into the dura. The single-layer sign describes a mass of uniformly hyperdense OPLL. 24 The double-layer sign describes anterior and posterior rims of hyperdense regions separated by a hypodense area. 24 The double-layer sign is more predictive of a dural defect than the single-layer sign. 24 , 25 , 26 Magnetic resonance imaging (MRI) is useful in detecting myelomalacia as a result of compression from OPLL as well as detecting the extent of spinal cord compression. MRI is also useful to assess for foraminal stenosis that could be contributing to radiculopathy.
Radiographic Risk Factors for Symptomatic Progression
Occupancy ratio, defined as the anterior-to-posterior ratio of the OPLL to the spinal canal, can be calculated on lateral radiographs or CT sagittal images (Fig. 5A). A ratio of 30 to 60% is predictive of the development of myelopathy. 27 , 28 Studies found that 100% of patient with occupancy ratio > 60% developed myelopathy. 29 , 30 In addition, OPLL fragments on axial CT that were more laterally deviated resulted in higher rates of myelopathy as compared with those that were centrally based. 29 The space available for cord is measured by subtracting the anterior to posterior distance of the OPLL from the spinal canal. A space available for cord of 6 to 9 mm has also been associated with the development of myelopathy. 30
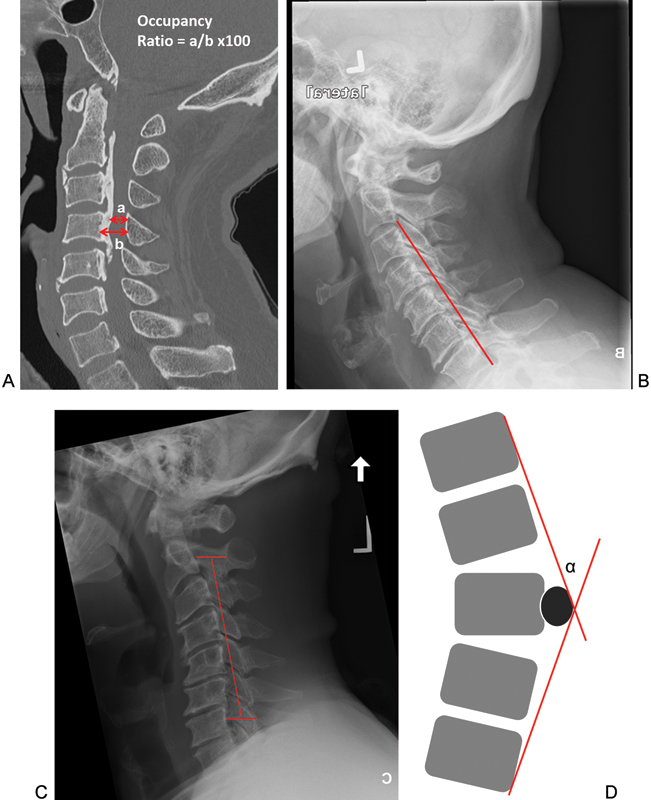
Measurements used in surgical planning of ossification of the posterior longitudinal ligament (OPLL). (A) Occupancy ratio can be calculated to decide on an anterior versus posterior decompression . It is calculated by dividing a (distance between largest width of OPLL to posterior spinal canal) by b (spinal canal diameter) and multiplying by 100. Anterior decompression is recommended with a ratio of 60% and higher. (B). Effective lordosis measured by a line from the dorsal-caudal aspect of the C2 vertebral body to the dorsal-caudal aspect of C7. Effective lordosis is maintained in this case because no ventral structures such OPLL, vertebral body, or osteophytes are dorsal to the line. This patient would be a candidate for a posterior-based surgery. (C) The K-line on the lateral radiographs connects the midpoints of the spinal canal at C2 and C7. In K-line-positive cases, the OPLL is ventral to the line and in K-line-negative cases, the OPLL is dorsal to the line. In K-line-positive cases, a posterior approach is recommended. (D) Ossification-kyphosis angle (α) is measured on sagittal thoracic magnetic resonance imaging by drawing a Cobb angle from the cranial vertebrae to the caudal vertebrae that span the planned decompression site and centered over the largest OPLL fragment. An ossification-kyphosis angle > 23 degrees should undergo an anterior decompression.
When myelomalacia is present on MRI along with an occupancy ratio ≥60%, an anterior decompression approach has been associated with improved surgical outcomes in comparison with laminoplasty. 31 Dynamic CT has also been introduced in the evaluation of cervical OPLL. In 107 patients with myelopathy, OPLL, and pre-existing kyphotic alignment, extension resulted in increased narrowing at levels that were already stenosed, and flexion led to further spinal cord compression. 32
Management
Nonoperative Management of Cervical OPLL
Nonoperative management of OPLL with cervical involvement includes observation, and if radicular symptoms are present, physical therapy and oral analgesics are options. Pham et al reviewed 11 studies with 480 patients with OPLL treated nonoperatively. 33 They concluded that patients without myelopathy are likely to remain progression-free, and patients with myelopathy have a high rate of progression. Therefore, prophylactic surgery is not recommended for patients without myelopathy. A cohort study by Matsunaga et al prospectively evaluated 450 patients and using Kaplan-Meier analysis predicted that 71% of patients would remain free of myelopathy at 30 years. 34 In this cohort, the average age of presentation was 59.6 years and 72.6 years at latest follow-up. Most were men (319; 71%). The most important risk factor for developing myelopathy was canal stenosis > 60%.
Operative Management of Cervical OPLL
In a multicenter study of 4,589 patients undergoing cervical spine surgery, 5% of the surgeries were performed in patients with OPLL. 35 Operative management of OPLL with cervical involvement is reserved for patients with progressive myelopathy and myeloradiculopathy that has not responded to nonoperative treatment. Patients presenting with SCI in the setting of trauma and OPLL are also surgical candidates for decompression and stabilization (Fig. 4). Choices for surgical management include anterior, posterior, and circumferential approaches. Along with clinical findings, radiologic findings are important in deciding the optimal surgical approach. 36 A straight line drawn from the posterior-inferior aspect of the C2 vertebral body to C7 is used to assess effective lordosis (Fig. 5B). If osteophytes and hypertrophic calcification are present behind this line, then effective lordosis is lost and an anterior approach is advised. 37 The K-line is an important radiographic marker to assess lordosis (Fig. 5C). A K-line is formed with a line drawn from the midpoint of the C2 spinal canal to the midpoint of the spinal canal at C7. K-line-positive patients have OPLL anterior to this line. A posterior approach is recommended for these patients. For K-line-negative patients, an anterior approach can be pursued. 38 The occupancy ratio is also important in deciding between an anterior versus posterior approach. In patients with occupancy ratio > 60% who underwent laminoplasty, there was significantly less (p < 0.03) improvement in neurologic recovery rate and Japanese Orthopaedic Association scores compared with those who underwent an anterior approach. 39
Operative Techniques: Anterior Approach
Anterior approaches can include corpectomy and fusion or anterior cervical diskectomy and fusion. Corpectomy is associated with greater neurologic recovery especially with stenosis greater than 50% but can be complicated by dural tears. 40 The anterior floating decompression method minimizes the chance of cerebrospinal fluid (CSF) leak by allowing the OPLL to stay attached to the dura, which in turn allows the OPLL to migrate anteriorly after decompression. The method is recommended in patients with an occupancy ratio of 60% or higher. 27 , 28 When performing one-level or multilevel corpectomies for the anterior floating method, a minimum of 20 mm of transverse decompression is needed, and the OPLL should be thinned to 5 mm or less. The OPLL is next transected horizontally at its cranial and caudal margins followed by transecting the lateral margin that adheres to the vertebral body, which allows the OPLL to be released and “float.” A minimum of 2 to 3 mm of space between the OPLL and the lateral edge of the vertebral body is needed to allow the OPLL to float. 27 Reconstruction can be performed with fibula strut allograft, iliac crest autograft, or cage depending on the surgeon. A recent long-term follow-up of patients with an occupancy ratio of 60% undergoing an anterior-based decompression (n = 12) or a posterior decompression (n = 15) noted significantly better outcomes (p < 0.04) in the anterior group. 41 Complications rates were similar between the two groups.
Operative Techniques: Posterior Approach
Posterior surgical approaches include laminoplasty, laminectomy, and laminectomy and fusion. A positive K-line (OPLL ventral to this line) is a radiographic indication for performing a posterior-based decompression. 38 When choosing the level of decompression, in addition to the segments affected with OPLL, one may consider decompressing above and below the OPLL-affected levels to prevent spinal cord kinking as the spinal cord drifts posteriorly. Laminoplasty is indicated with a neutral cervical spine alignment and/or kyphosis up to 13 degrees. The open-door or French-door techniques of laminoplasty can be performed, and plates, sutures, or bone graft can be used to maintain the lamina open. Laminoplasty can provide adequate decompression but OPLL may progress in over 70% of patients. 42 Factors associated with OPLL progression were younger age at surgery and mixed and continuous types of OPLL. However, only 2 of the 41 (4.9%) patients with OPLL progression developed neurologic changes. Axial neck pain is a postoperative concern of laminoplasty. Recent modifications such as avoiding laminoplasty at C3 and C7 have led to a decrease in postlaminoplasty neck pain. Factors associated with successful surgical outcomes for patients with OPLL undergoing laminoplasty include occupancy ratio < 60%, preoperative morbidity for less than 1 year, younger age, and a smaller area of T2 cord signal change. 43 Laminectomy alone is not routinely recommended for OPLL due to the high rate of postlaminectomy kyphosis that can develop. Laminectomy with instrumented fusion can prevent postsurgical kyphosis but may be associated with higher rates of nerve root palsy. Eighty-three patients undergoing posterior laminectomy and fusion for OPLL demonstrated significant improvements in JOA scores at latest follow-up (p < 0.01). 44 Nerve root palsy included 7 cases at C5, 2 at C6, and 1 at C7. The authors noted that patients who developed a nerve root palsy had increased cervical lordosis, 13.5 degrees compared with 3.9 degrees in the rest of the cohort.
Operative Approach: Combined Anterior-Posterior
Circumferential decompression for OPLL is limited to cases with significant preoperative kyphosis. There have been limited reports of circumferential surgery for OPLL. In a series of 12 patients with multilevel OPLL and spinal cord signal change, multilevel open-door laminoplasty was performed followed by anterior corpectomy at the most stenotic level. 45 The laminoplasty was performed first to allow the spinal cord to drift back and decrease the risk associated with anterior-based decompression. 45 If corpectomy of two or more levels is performed, then a posterior-based instrumentation and fusion should also be performed to minimize the risk of graft or cage complications.
Complications following Surgical Management of Cervical OPLL
Surgical complications are a particular concern in patients with OPLL. In a review of 27 studies with a total 1,558 patients undergoing surgery for OPLL, the complication rate was 21.8%. 40 CSF leaks (5.1%), implant complications (3.5%), and hoarseness, dyspnea, and dysphagia (0.3%) were more common with anterior approaches. C5 nerve palsy (4.2%) and axial pain (3.5%) were more common with posterior approaches. 40 In a single-institution study of 1,994 patients undergoing cervical spine surgery, a 1% prevalence of CSF leak was noted. In this series, patients with OPLL were 13.7 times more likely to have a CSF leak compared with patients without OPLL. 46 Pseudarthrosis had a frequency of 3 to 6% for a one-level corpectomy and 17 to 30% for three-level anterior fusions. 47 , 48 , 49 Intraoperative neuromonitoring consisting of transcranial motor evoked potentials and somatosensory evoked potentials may be useful in increasing the safety of operating on the myelopathic spine with OPLL.
Thoracic OPLL
Nonoperative Management of Thoracic OPLL
Thoracic OPLL is rare, and symptoms of myelopathy are more severe than in cervical OPLL due to the narrow canal, rigidity of the thoracic spine, tenuous blood supply, and inability of the spinal cord to withstand much compression. Surgical intervention is usually indicated due to the severity of clinical presentation.
Operative Management of Thoracic OPLL
Surgical options for thoracic OPLL include laminoplasty, laminectomy and fusion, anterior decompression through a posterior approach (transpedicular, costotransversectomy), and circumferential decompression via staged anterior and posterior approaches. The ossification-kyphosis angle is an MRI-based measurement that can assist in planning for an anterior versus posterior approach for thoracic OPLL (Fig. 5D). 50 On a sagittal MRI, it is the angle formed by the line connecting the most cranial vertebral body of the decompression site to the maximum prominence of the OPLL and the most caudal vertebral body of the decompression site to the maximum prominence of the OPLL. An ossification-kyphosis angle of 23 degrees is a critical point for effective posterior decompression. With an angle greater than 23 degrees, an anterior decompression is recommended. 50
Intraoperative ultrasound has been used by some surgeons to determine adequacy of decompression for thoracic OPLL. An echo-free space between the OPLL and anterior portion of the spinal cord can be determined from an intraoperative ultrasound. A positive echo-free space is a good indicator of adequate decompression. 51 An ossification kyphosis angle that is less than 23 degrees correlates with an echo-free space. 51
Posterior Decompression
For posterior-based procedures, a laminoplasty is recommended for flat OPLL and posterior decompression and fusion is recommended for a beak type. 9 For upper thoracic OPLL, a dorsal shift of the spinal cord can be expected by posterior decompression alone and laminoplasty. 52 Using an intraoperative ultrasound, the adequacy of decompression can be evaluated. One can look for an echo-free space anterior to the spinal cord after filling the extradural space with physiologic saline. 50 , 51
Posterior-based decompression and fusion via transpedicular or costotransversectomy approaches are options for thoracic OPLL. In 18 patients in whom intraoperative ultrasound was used to assess the adequacy of decompression via laminectomy, 12 were deemed not to have adequate decompression. 53 These 12 patients underwent transpedicular decompressions successfully with one neurologic deficit and two durotomies. Kato et al described their posterior-based transpedicular decompression and ligation of bilateral thoracic nerve roots to perform decompression for thoracic OPLL. 54 The ligation of the nerve roots allowed for better visualization of the OPLL and manipulation of the dura to aid in its removal, which was followed by instrumentation and fusion. 54 The advantages of this technique are better visualization and better kyphosis correction along with the benefits of an all-posterior approach. However, there is a risk of potential disruption of blood supply to the spinal cord. This approach is recommended for three consecutive levels or less. Neuromonitoring is recommended with this approach, and some groups clamp the nerve roots prior to nerve root ligation to ensure there is no change in spinal cord neuromonitoring. 55
Anterior and Posterior Decompression
Circumferential decompression in two stages is also an option for severe thoracic OPLL. In a series of 15 patients, 11 had posterior-based decompression followed by an anterior approach. Initially, a transpedicular approach is created to create “gutters” adjacent to the dura. 56 This technique frees the lateral edges of the OPLL and allows for removal of the OPLL during the anterior approach. A trans-sternal approach can be used for T2 and above, and a thoracotomy for T3 and below. The remaining OPLL can be removed via this approach, and anterior column reconstruction is performed depending on the extent of the corpectomy. There were three cases of CSF leak with this approach and one case of neurologic deterioration in a beak OPLL.
Surgical Outcomes
Baaj et al reviewed 16 published case series on thoracic OPLL with a total of 460 patients. 57 The authors concluded that there was no significant difference in outcomes in regards to surgical approaches. However, patients with instrumented fusion had better outcomes as there was a decreased rate of progressive kyphosis postoperatively. CSF leaks were noted in 22.1% of cases (34 patients), and 11.7% (18 patients) had neurologic deterioration. A review of these cases demonstrated that surgeons favored posterior approaches. Anterior and circumferential approaches were technically more demanding and associated with higher complication rates.
Complications following Surgical Management of Thoracic OPLL
The most common complications associated with anterior approaches were CSF leaks. 51 Postoperative kyphotic deformity and postoperative paraparesis were more common with uninstrumented posterior approaches and were managed with instrumentation and fusion. 5 , 53 Beak OPLL has a higher association with neurologic deterioration than the flat type. 9 , 57
Conclusion
OPLL is a multifactorial hyperostosis disorder that leads to ectopic calcification of the posterior longitudinal ligament. OPLL can occur throughout the spine; however, the cervical spine is more commonly affected. There are four types of OPLL based on sagittal CT: segmental, continuous, mixed, and localized or other. OPLL can be asymptomatic or can present with myelopathy or myeloradiculopathy. Imaging studies including radiographs, CT, and MRI can aid in assessment of severity and preoperative planning. For cervical OPLL, an initial trial with nonoperative management should be attempted for patients without myelopathy. Operative intervention is recommended for patients with myelopathy or those who fail conservative management. If the occupancy ratio is greater than 60, there is a high likelihood of myelopathy developing and surgery can potentially be offered in advance. Effective lordosis, K-line measurements, and occupancy ratio calculations can aid in deciding between anterior or posterior cervical approaches for decompression. Durotomies are a common complication during anterior decompressions; however, the floating island technique can be used to minimize CSF leaks. Posterior decompressive procedures such as laminoplasty or laminectomy and fusion can also be of used if lordosis of the cervical spine is maintained and in K-line-positive patients with occupancy ratio < 60%. Axial neck pain and C5 nerve root palsy are common complications of posterior-based approaches. Although rare, thoracic OPLL is more severe than cervical OPLL and usually requires operative intervention. The ossification kyphosis angle can be used to determine surgical approach. Decompression can be achieved via posterior-based approaches as well as anterior approaches. Posterior upper thoracic OPLL decompressions supplemented with instrumentation are associated with the best outcomes.
Disclosures
Rasheed Abiola, none
Paul Rubery, none
Addisu Mesfin, none