
Abstract
Study Design:
Systematic review.
Objective:
To review, critically appraise, and synthesize evidence on use of cell therapy for intervertebral disc repair.
Methods:
A systematic search of PubMed/MEDLINE was conducted for literature published through October 31, 2018 and EMBASE and ClinicalTrials.gov databases through April 13, 2018 comparing allogenic or autologous cell therapy for intervertebral disc (IVD) repair in the lumbar or cervical spine. In the absence of comparative studies, case series of ≥10 patients were considered.
Results:
From 1039 potentially relevant citations, 8 studies across 10 publications on IVD cell therapies in the lumbar spine met the inclusion criteria. All studies were small and primarily case series. For allogenic cell sources, no difference in function or pain between mesenchymal cell treatment and sham were reported in 1 small randomized controlled trial; 1 small case series reported improved function and pain relative to baseline but it was unclear if the change was clinically significant. Similarly for autologous cell sources, limited data across case series suggest pain and function may be improved relative to baseline; whether the changes were clinically significant was not clear. Safety data was sparse and poorly reported. The need for subsequent surgery was reported in 3 case-series studies ranging from 6% to 80%.
Conclusions:
The overall strength of evidence for efficacy and safety of cell therapy for lumbar IVD repair was very low primarily due to substantial risk of bias, small sample sizes and lack of a comparator intervention. Methodologically sound studies comparing cell therapies to other treatments are needed.
Introduction
Intervertebral disc (IVD) degeneration is a complex and multifactorial process, influenced by genetic, nutritional, and mechanical factors. 1 As the degeneration cascade progresses, production of pro-inflammatory molecules such as tumor necrosis factor–α and interleukins increases. Furthermore, endplate calcification impairs nutrient flow and exacerbates the hypoxic acidic environment. Together, nutrient deprivation and inflammatory environment accelerate the cell death within nucleus pulposus. 2 -5 Consequently, levels of proteoglycans and other extracellular matrix proteins decrease leading to disc desiccation and progressive instability. 6 IVD degeneration is considered as one of the major underlying causes of low back pain. 7,8 In addition, degeneration of IVD contributes to other disc pathologies such as disc herniation, spondylolisthesis, spinal canal stenosis, or facet joint syndrome. 9,10
Spine fusions are one of the most common surgical approaches for discogenic back pain with the clinical success rate ranging from 50% to 70%. 11,12 Although existing surgical treatments provide better pain relief than the nonsurgical interventions 13,14 they do not address the biology of disc degeneration namely high pro-inflammatory cytokine levels or the inherent loss of nucleus pulposus cells. In addition, studies have shown surgery may lead to increased biomechanical stress and onset of degenerative cascade of adjacent segments. 15,16
Among the biological disc repair therapies, cell therapy has gained interest as it offers a disc regenerative potential, while being minimally invasive. A cell therapy approach aims to address disc inflammation by inhibiting aberrant cytokine production; disc rehydration and height restoration by initiating matrix anabolism, repopulating and stimulating the native cells. Various cell types have been used for IVD regeneration including disc cells, notochordal cells or stem cells. 17 Mesenchymal stem cells (MSCs) have immunomodulatory functions and ability to differentiate into cartilage, therefore, are considered as a potentially ideal cell source for IVD regeneration. 18 Previous studies have shown that MSCs isolated from bone marrow and adipose tissue can differentiate into a nucleus pulposus–like phenotype. 18 -20 Co-culture experiments of MSCs with nucleus pulposus cells have shown nucleus pulposus cells proliferation and MSCs differentiation into chondrogenic cells. 21,22 Preclinical studies with cell therapy have demonstrated promising results in animal models. 23 -26 Transplanted MSCs have been shown to restore normal disc environment by inducing production of extracellular matrix proteins, including aggrecan and other proteoglycans, and type I and II collagen. 18,25,27 Some studies have also reported preservation of disc height and water content through MSCs application. 25,26,28 Another pilot trial in humans with MSCs of autologous origin has indicated feasibility, safety, and improvement in clinical outcomes, including improved water content. 29 Contrarily, Haufe amd Mork 30 showed that regenerative effect of intradiscal hematopoietic stem cell injection does not correlate with reduced pain, and thus does not offer clinically improved outcomes. Additionally, osteophyte formation by cell leakage was reported with MSC implantation. 31
Although cell therapy promises a greater potential for intervertebral disc regeneration, strong clinical evidence is lacking. Furthermore, questions concerning safety, long-term complications, efficacy in heterogeneous patient population, and cost-effectiveness of the procedure have not been addressed. The aim of this study was to systematically review, critically appraise, and synthesize evidence on use of cell therapy for intervertebral disc repair.
Materials and Methods
The methods for this systematic review followed accepted standards for systematic review/comparative effectiveness reviews for rigor, quality, and transparency including those described by the Agency for Healthcare Research and Quality (AHRQ), IOM Standards for Systematic Reviews, and the PCORI Methods Guide. 32 -34
Electronic Literature Search
A systematic search of PubMed/MEDLINE was conducted for literature published through October 31 and through April 13, 2018 for EMBASE and ClinicalTrials.gov databases. Only studies in humans with abstracts written in English were considered for inclusion, with no other limits placed on the search. A priori inclusion and exclusion criteria are detailed in Appendix A (available online). Briefly, we sought to identify comparative studies of stem cell use versus conservative care, other disc-preserving injection treatments or surgical intervention in persons with cervical or lumbar degenerative disc disease or disc prolapse. In the absence of comparative studies, case series with ≥10 patients were considered. The search strategy included use of controlled vocabulary (MeSH terms) and key words (Appendix A). Bibliographies of included studies and relevant systematic reviews were reviewed to identify pertinent studies. Citations were dual reviewed for inclusion at both title/abstract and full text stages. ClincalTrials.gov was searched to identify studies that may have new publications.
Data Extraction
In addition to results, data abstraction included patient characteristics, demographics, lifestyle choices (eg, smoking), comorbidities (eg, obesity), cointerventions (eg, pharmaceutical, physical therapy, etc) intervention and comparator details (eg, spinal levels treated, use of anesthetic, cell preparation and concentration, delivery, etc).
Individual Study Quality
Each included study was independently assessed for risk of bias and methodological quality by 2 reviewers (ACS, AF) using preset criteria based on criteria and methods delineated in the Cochrane Handbook for Systematic Reviews of Interventions, The Journal of Bone and Joint Surgery, 35 and the AHRQ with adaptations focusing on criteria associated with methodological quality. 32,36 Economic studies were evaluated according to The Quality of Health Economic Studies (QHES) instrument developed by Ofman et al. 37 Where feasible, the focus was on studies with the least potential for bias and the fewest limitations. Risk of bias assessments are detailed in Appendix B.
Data Analysis
For continuous measures from randomized controlled trials (RCTs), mean differences and corresponding confidence intervals were calculated with unpaired t tests used for statistical testing. Statistical testing was not performed for observational studies. Risk ratios were calculated for dichotomous outcomes from RCTs if differences between groups were or approached statistical significance using the Rothman EpiSheet. 38 For continuous outcomes; mean differences were calculated and 2-sample t tests done, if appropriate, using Graphpad Software. 39 Study design, heterogeneity across studies and variation in reporting precluded the pooling of data.
Overall Quality (Strength) of Body of Evidence
For the primary outcomes of function and pain and for adverse events, the overall strength of evidence across included studies was assessed using the precepts outlined the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) working group and recommendations made by the AHRQ.
32,40
-42
The overall quality of evidence was based on studies at least risk for bias. In determining the quality (strength) of a body of evidence regarding a given outcome, the overall quality may be downgraded 1 or 2 levels based on the following domains: (1) risk of bias due to study limitations, (2) consistency (heterogeneity) of results, (3) directness of evidence (eg, hard clinical outcomes), (4) precision of effect size estimates (eg, width of confidence intervals), and (5) publication or reporting bias. Publication and reporting bias are difficult to assess, particularly with fewer than 10 RCTs.
32
Publication bias was unknown in all studies and thus this domain was eliminated from the strength of evidence tables. The initial quality of the overall body of evidence begins as “High” for RCTs and “Low” for observational studies. The body of evidence for methodologically strong observational studies may be upgraded 1 or 2 levels if there are no downgrades in the primary domains above and one or more of the following are met: (1) large magnitude of effect, (2) Dose-response gradient, and (3) all plausible biases would decrease the magnitude of an apparent effect. The final overall quality (strength) of the body of literature expresses the confidence in the estimate of effect and the impact that further research may have on the results as follows: High—High confidence that the evidence reflects the true effect. Further research is very unlikely to change our confidence in the estimate of effect. Moderate—Moderate confidence that the evidence reflects the true effect. Further research may change our confidence in the estimate of effect and may change the estimate. Low—Low confidence that the evidence reflects the true effect. Further research is likely to change the confidence in the estimate of effect and likely to change the estimate. Very low—Very little confidence that the evidence reflect the true effect; the true effect is likely to be substantially different than the estimated effect. In addition, this rating may be used if there is no evidence or it is not possible to estimate an effect.
Results
Study Selection
From 1039 potentially relevant citations identified, 1027 were excluded based on title and/or abstract review; twelve studies, all in the lumbar spine, were selected for full-text review (Figure 1). Eight studies (from 10 publications) met the inclusion criteria, including 1 RCT (N = 24), 1 preliminary report from an ongoing phase I pilot RCT describing safety results (N = 24), 5 case series (7 publications) (N = 10-26), and 1 single-arm registry study (N = 33). 29,30,43 -50 Additionally, 10 ongoing clinical trials were identified (Appendix C). No additional studies were identified from hand searching bibliographies of included studies or identified systematic reviews.
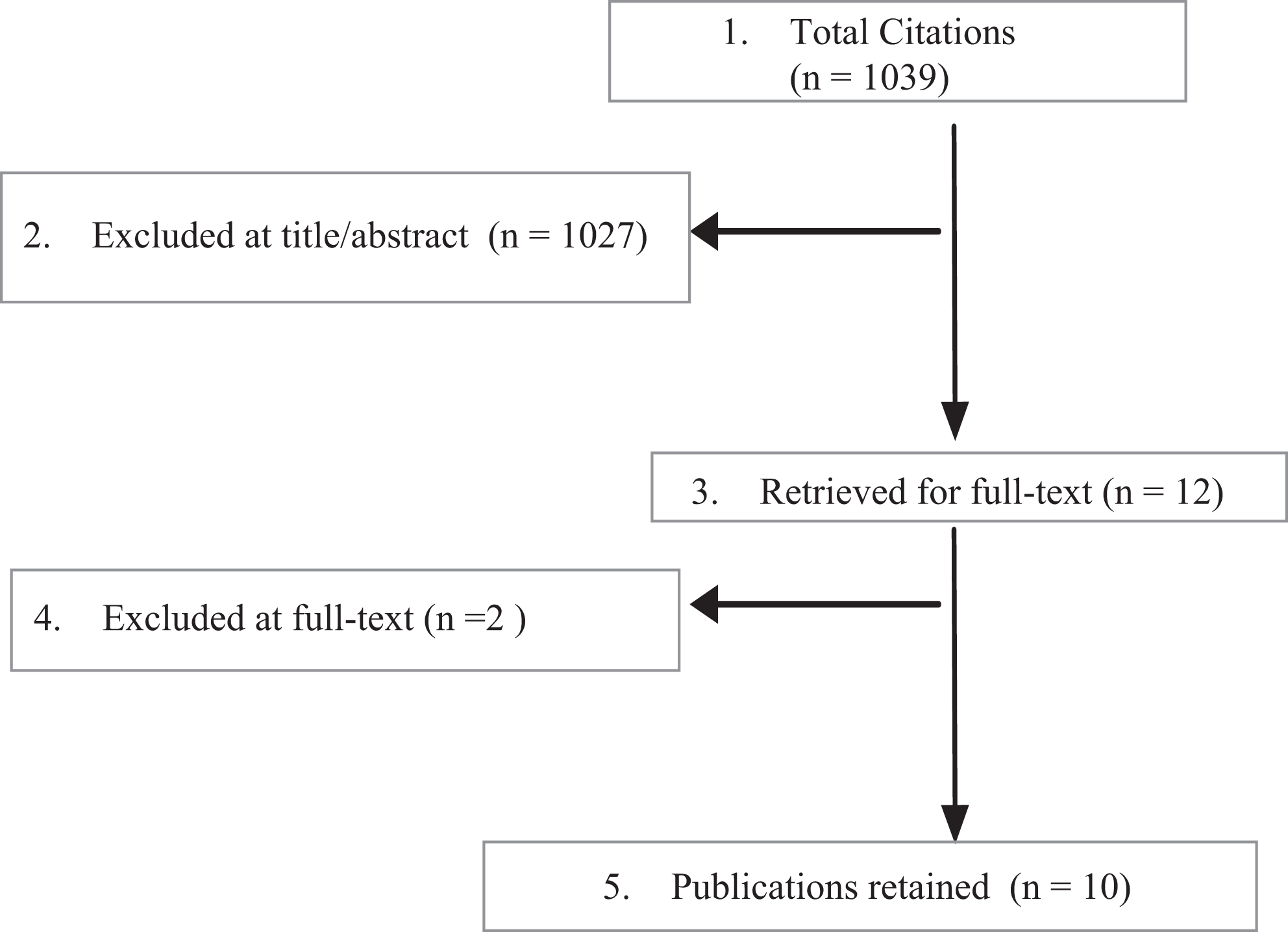
Flowchart showing results of literature search.
No studies of cell-based therapy for cervical IVD repair were identified.
Both RCTs were considered at moderately high risk of bias. All case series were considered at high risk of bias. Methodological concerns included potential for selection bias (failure to describe patient selection methods and/or number of eligible patients and/or loss to follow-up) and lack of blinded outcomes assessment for patient-reported outcomes (Appendix B).
Key Question 1: Effectiveness of Cell Therapy
Across included studies, populations were predominately male with mean ages of approximately 40 years who had failed previous conservative care. Two studies of allogenic cell sources 44,46 and 5 studies (7 publications) of autologous cell sources provided data on effectiveness. 29,30,43,45,47 -49 Table 1 summarizes the pathologies, prior treatments, and levels treated. Details of cell preparation, sources and intervention specifics are found in the abstraction tables (Appendix D). Results and tables for primary outcomes (function, pain) are reported below; results for secondary outcomes are found in Appendix E.
Summary of Pathologies, Prior and Concurrent Treatment, and Spinal Levels Treated.
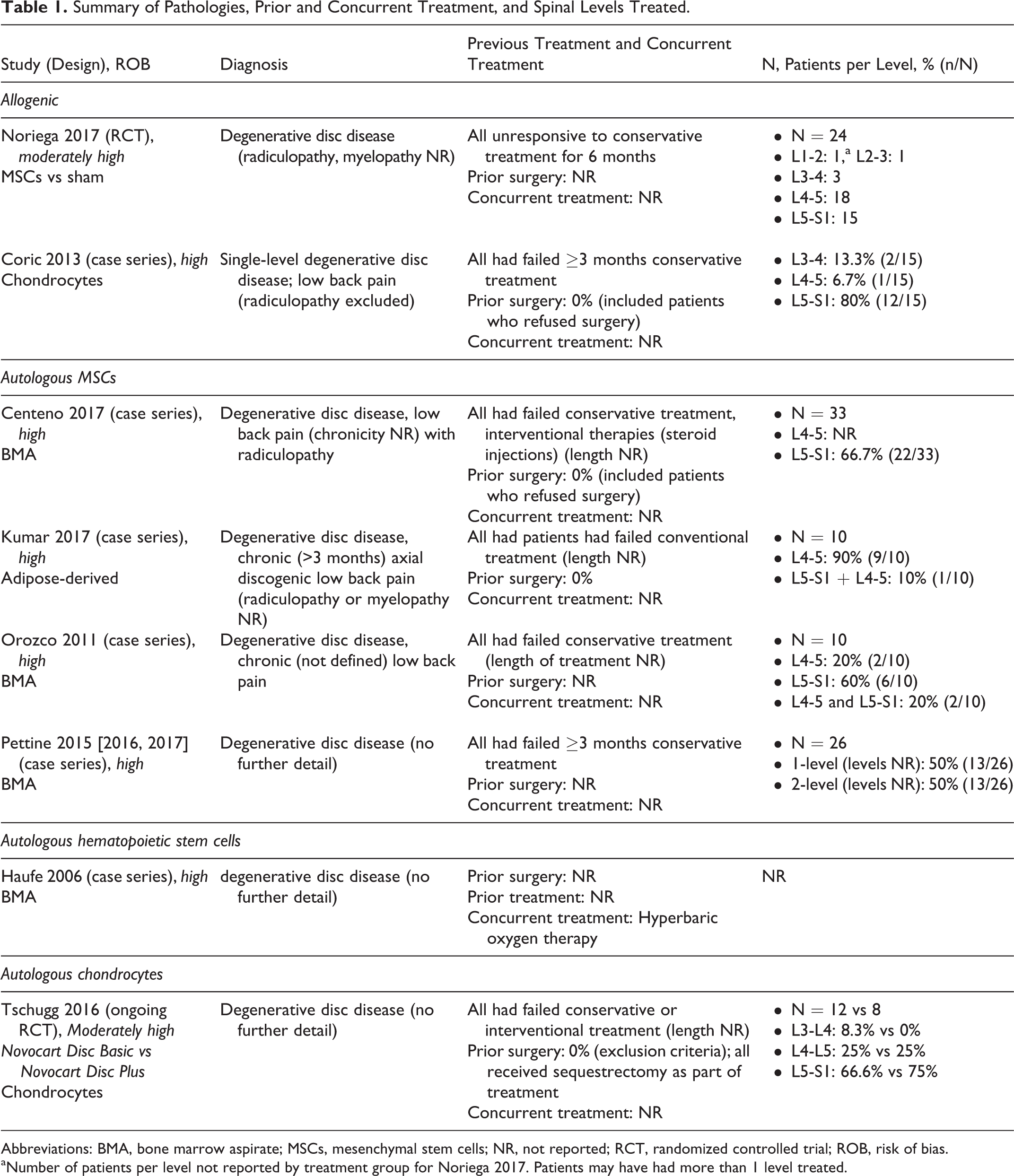
Abbreviations: BMA, bone marrow aspirate; MSCs, mesenchymal stem cells; NR, not reported; RCT, randomized controlled trial; ROB, risk of bias.
aNumber of patients per level not reported by treatment group for Noriega 2017. Patients may have had more than 1 level treated.
Allogenic Cell Sources: Lumbar Spine
One small RCT (N = 24) at moderately high risk of bias comparing expanded allogenic MSC from healthy donors (intradiscal injection of 25 × 106 cells per segment under local anesthesia) compared with sham injection of 2 mL of 1% mepivacaine into the paravertebral musculature was identified. Patients had chronic low back pain and degerative disc disease at 1 or 2 levels and had failed a minimum of 6 months conservative care. 46 L4-L5 and L5-S1 were the most common levels treated. No differences between allogenic MSC and sham treatment were seen for function based on Oswestry Disability Index (ODI), visual analogue scale (VAS)–pain, Short Form–36 (SF-36) Mental Component Score (MCS) or Physical Component Score (PCS) at any time frame, which may in part be due to small sample size (Table 2 and Appendix E). Similarly, there was no statistical difference between treatment groups in disc height decrease. Authors reported improved function and pain compared with baseline in the MSC group at 3, 6, and 12 months; again, no differences between treatment groups were noted.
Summary of Primary Outcomes (RCT and Case Series): Expanded Allogenic Cells for IVD Repair.
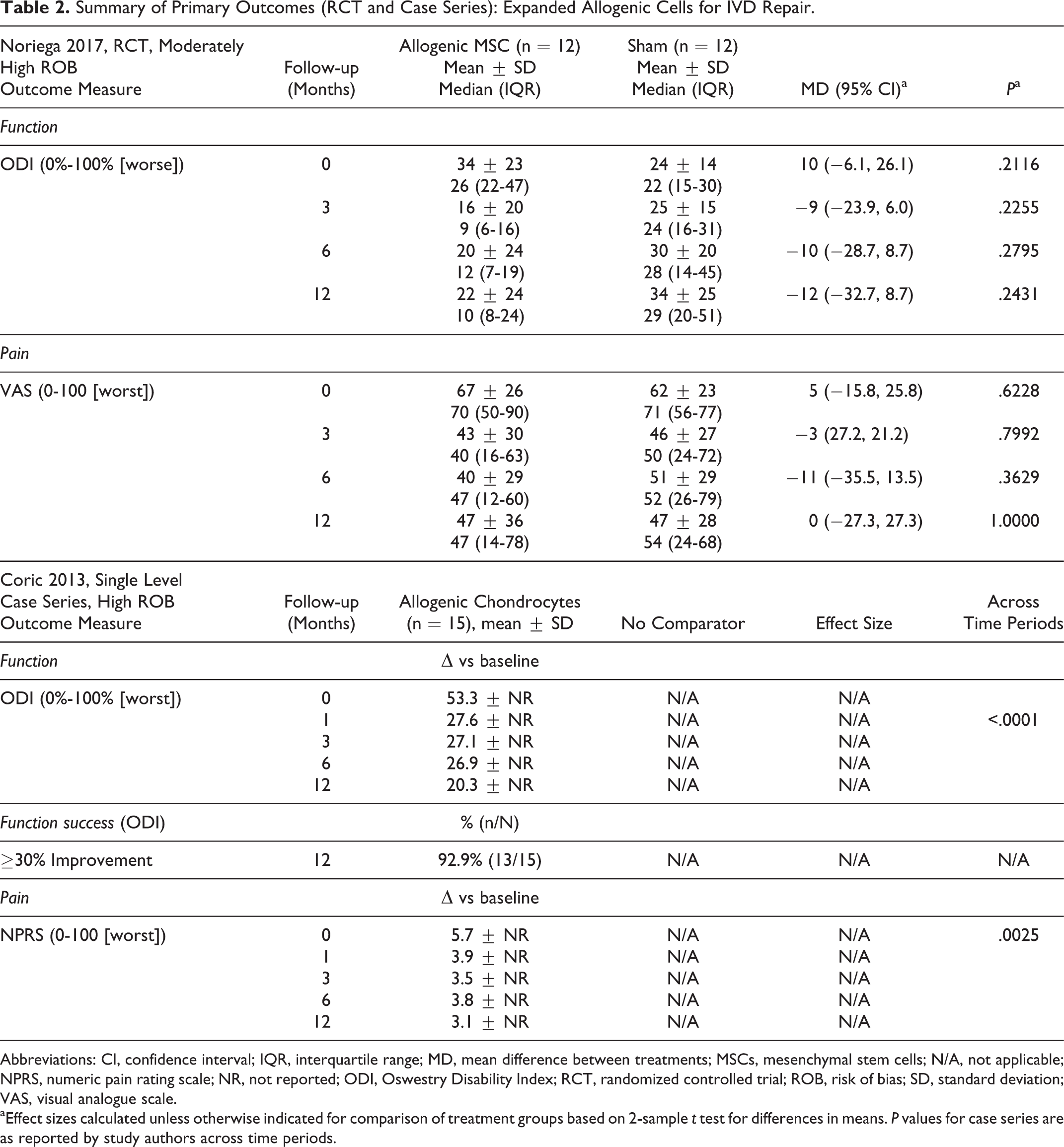
Abbreviations: CI, confidence interval; IQR, interquartile range; MD, mean difference between treatments; MSCs, mesenchymal stem cells; N/A, not applicable; NPRS, numeric pain rating scale; NR, not reported; ODI, Oswestry Disability Index; RCT, randomized controlled trial; ROB, risk of bias; SD, standard deviation; VAS, visual analogue scale.
aEffect sizes calculated unless otherwise indicated for comparison of treatment groups based on 2-sample t test for differences in means. P values for case series are as reported by study authors across time periods.
One small (N = 15) prospective case series (high risk of bias) using expanded, allogenic, cryopreserved juvenile chondrocytes (∼107cells/mL in a fibrin carrier) from cadaveric articular surfaces for single level intervention was also identified. 44 Local anesthetic was used for all procedures. Allogenic chondrocyte implantation improved ODI and VAS scores (Table 2) and SF-36 PCS through 12 months but not SF-36 MCS compared with baseline values (Appendix D1). Functional success and improvement in disc contour or height on magneric resonance imaging (definitions not provided) was achieved by the majority of patients (Appendix Tables D).
Autologous Cell Sources: Lumbar Spine
All data was from 5 small case series (N = 10-33) considered to be at high risk of bias (Table 1). Three series used MSC from bone marrow aspirate (BMA) 29,43,47 -49 ; one combined MCS from adipose tissue with hyaluronic acid 45 and one used hematopoietic cells from BMA 30 (Appendix Tables D).
At 3, 6, and 12 months, 3 of the 5 series reported improved function based on mean ODI scores compared with baseline scores 29,45,48 ; however, one study reported no difference from baseline on the m-SANE (modified single assessment numeric evaluation) measure at any time frame. 43 The percent reduction in ODI compared with baseline was likely clinically significant (>55%) at all time frames in 1 study 48 and a majority of patients achieved success (variably defined) in 2 other studies (Table 3). 43,45 Variability around mean estimates is poorly reported or very large in most instances, making conclusions regarding estimate precision and stability difficult.
Summary of Functional Outcomes of Autologous Cells for Intervertebral Disc Repair Across Case Series.
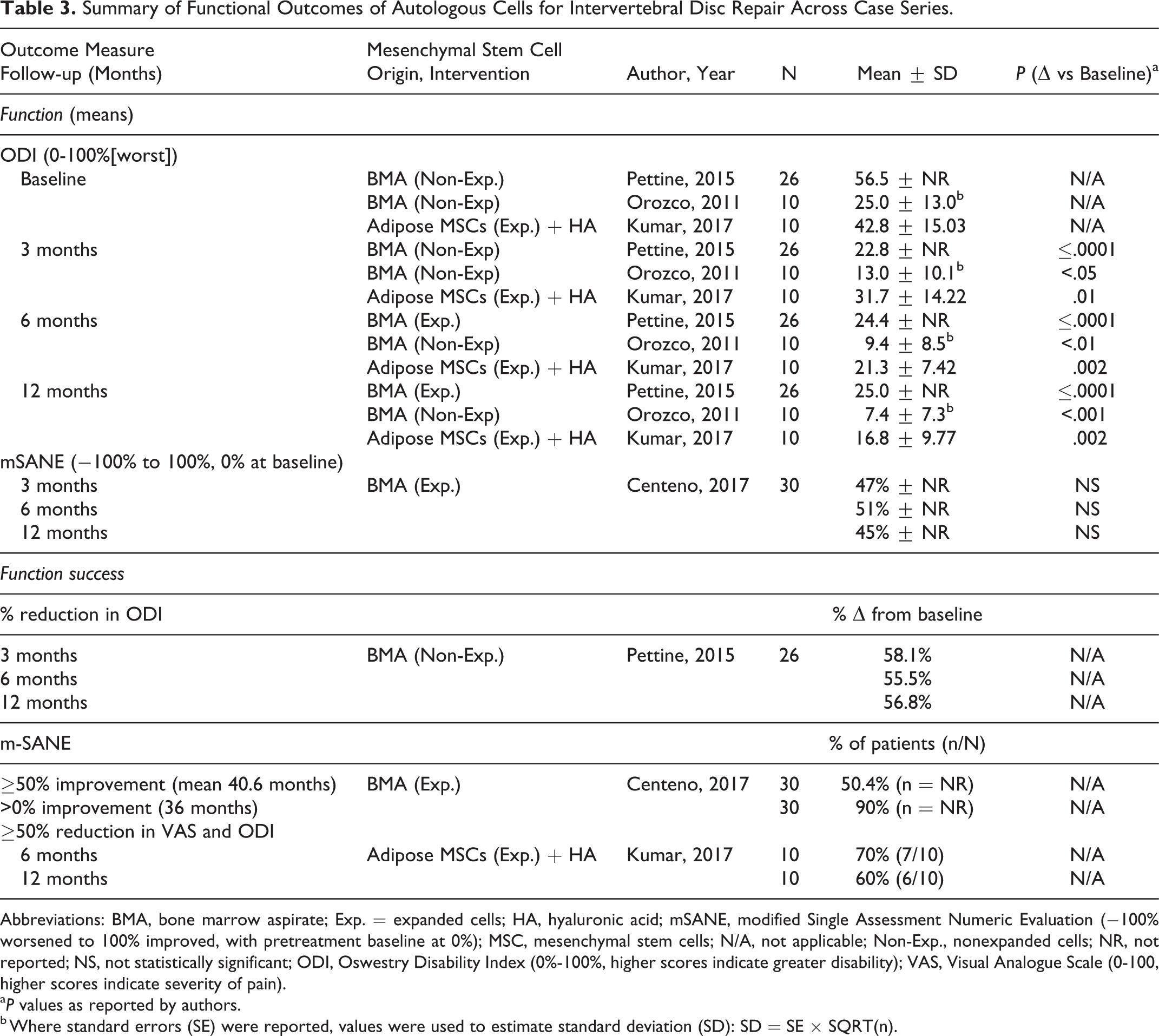
Abbreviations: BMA, bone marrow aspirate; Exp. = expanded cells; HA, hyaluronic acid; mSANE, modified Single Assessment Numeric Evaluation (−100% worsened to 100% improved, with pretreatment baseline at 0%); MSC, mesenchymal stem cells; N/A, not applicable; Non-Exp., nonexpanded cells; NR, not reported; NS, not statistically significant; ODI, Oswestry Disability Index (0%-100%, higher scores indicate greater disability); VAS, Visual Analogue Scale (0-100, higher scores indicate severity of pain).
aP values as reported by authors.
b Where standard errors (SE) were reported, values were used to estimate standard deviation (SD): SD = SE × SQRT(n).
Pain reduction (VAS 0-100 scale) compared with baseline was also consistently seen following autologous cell therapy across most studies at most time frames (Table 4). Exceptions were seen in one study of MCS from BMA, which reported no statistically significant change in VAS pain scores compared with baseline at 6 or 12 months 43 and in another study, which reported that pain reduction was not seen in any patient. 30 Pain reduction relative to baseline appeared to be clinically significant (58% to 64%) at 3, 6, and 12 months in 1 series. 48 Variability around mean estimates was poorly reported or very large in most instances, making conclusions regarding estimate precision and stability difficult.
Summary of Pain Outcomes of Autologous Cells for Intervertebral Disc Repair Across Common Time Frames Across Case Series.
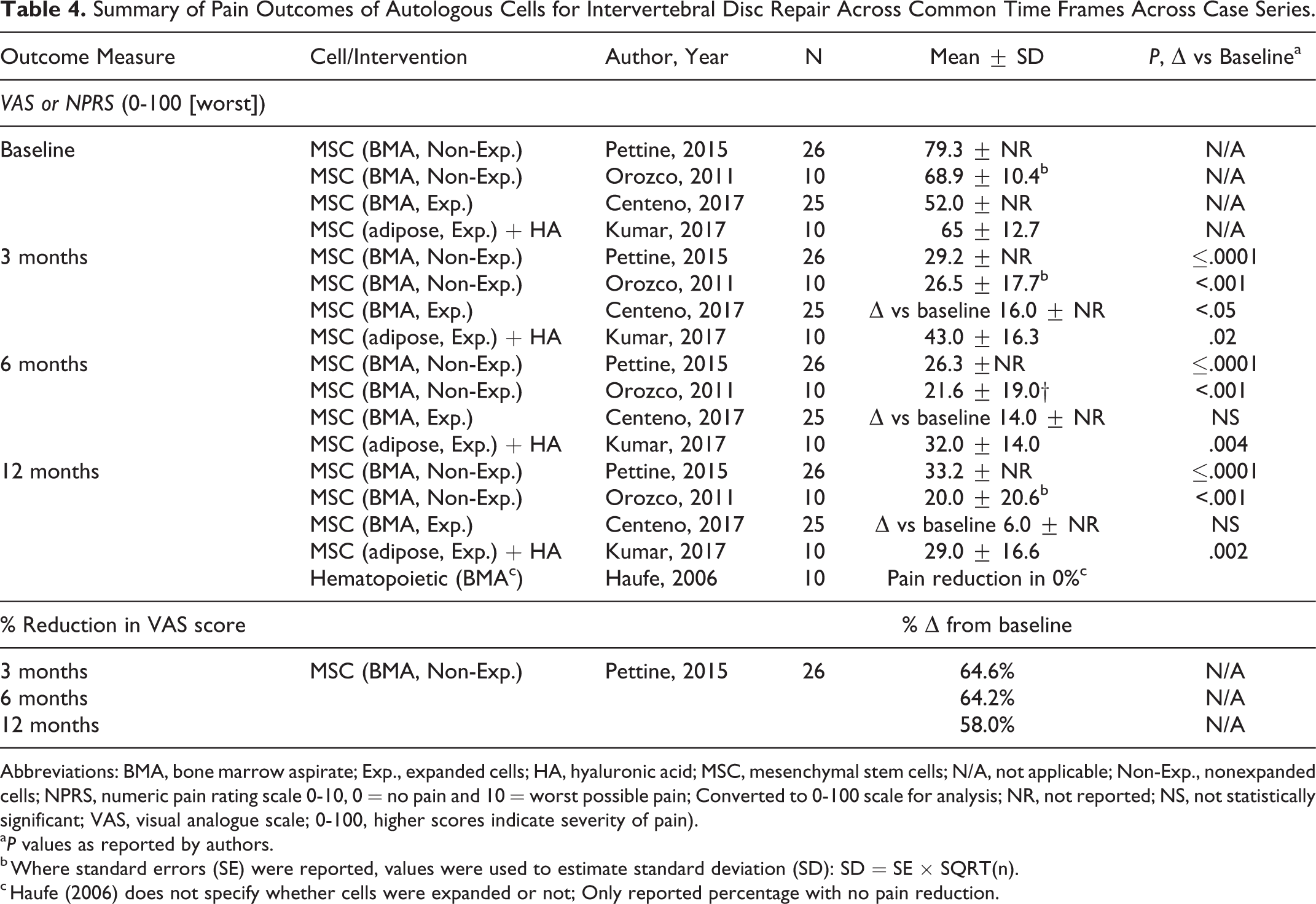
Abbreviations: BMA, bone marrow aspirate; Exp., expanded cells; HA, hyaluronic acid; MSC, mesenchymal stem cells; N/A, not applicable; Non-Exp., nonexpanded cells; NPRS, numeric pain rating scale 0-10, 0 = no pain and 10 = worst possible pain; Converted to 0-100 scale for analysis; NR, not reported; NS, not statistically significant; VAS, visual analogue scale; 0-100, higher scores indicate severity of pain).
aP values as reported by authors.
b Where standard errors (SE) were reported, values were used to estimate standard deviation (SD): SD = SE × SQRT(n).
c Haufe (2006) does not specify whether cells were expanded or not; Only reported percentage with no pain reduction.
Success, defined as ≥50% reduction in VAS and ODI was achieved by 70% (7/10) patients at 6 months and maintained by 60% by 12 months in 1 small series (N = 10). 45
With regard to secondary outcomes, 1 series reported a significant difference in SF-36 PCS at 12 months, but not in the MCS in 1 series. 29 Disc height did not appear to change substantially from baseline based on 2 series 29,45 (Appendix Tables E).
Key Question 2: Safety
Allogenic Cell Sources
Evidence of safety across the 2 studies of allogenic cell sources was sparse. No major adverse events were identified in the RCT in either treatment group; authors reported that fewer allogenic MSC recipients required nonsteroidal anti-inflammatory drugs (NSAIDs; 25% vs 66.6%) versus sham and 8.3% of both groups received opioids. 46 Similarly, no treatment-related adverse events were observed in the case series of allogenic chondrocyte implantation; however, 20% (3/15) of participants had subsequent total disc arthroplasty by 12 months for persistent low back pain. 44 Neither study likely had sufficient power to detect rare adverse events (Table 5).
Summary of Safety Outcomes.
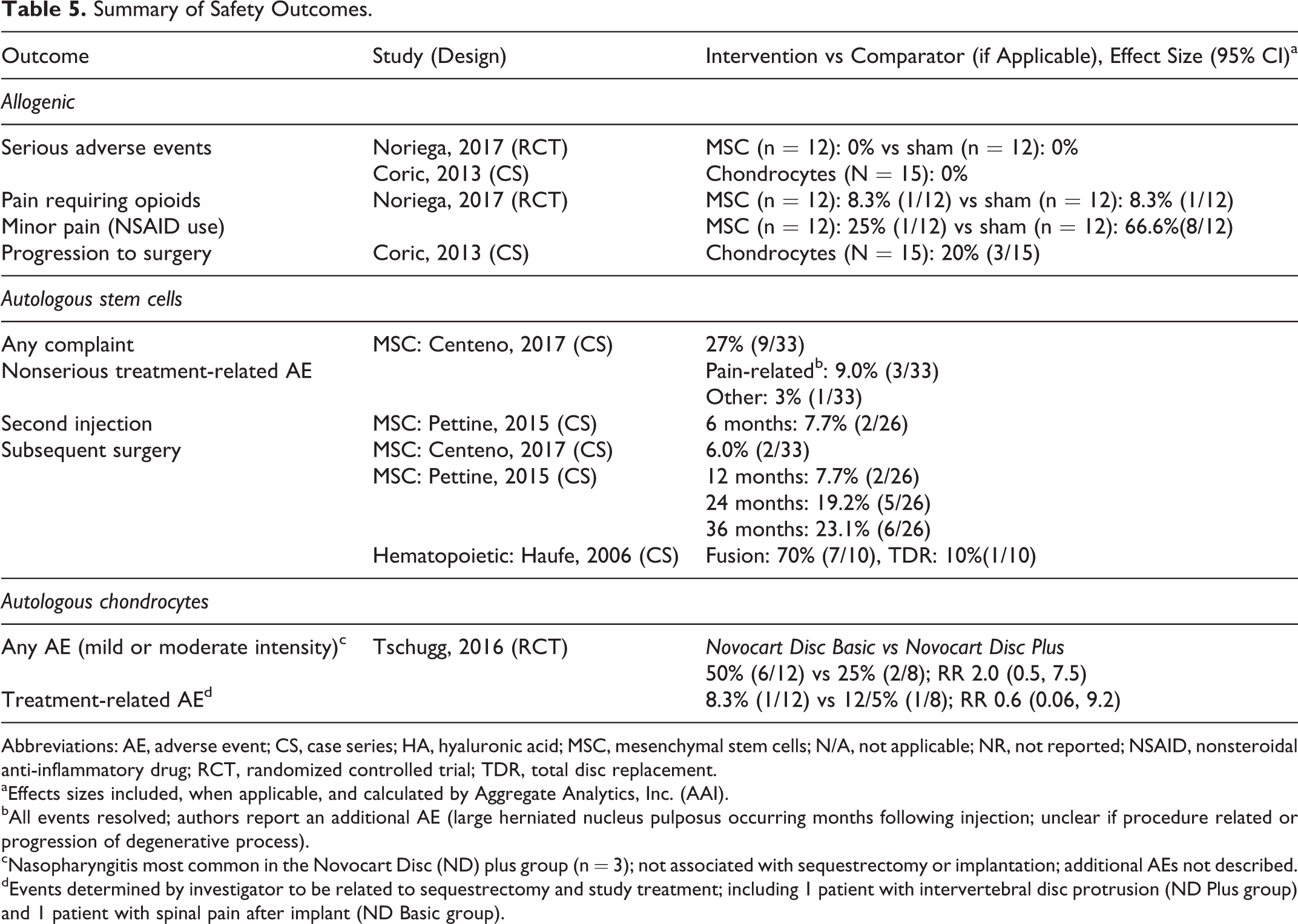
Abbreviations: AE, adverse event; CS, case series; HA, hyaluronic acid; MSC, mesenchymal stem cells; N/A, not applicable; NR, not reported; NSAID, nonsteroidal anti-inflammatory drug; RCT, randomized controlled trial; TDR, total disc replacement.
aEffects sizes included, when applicable, and calculated by Aggregate Analytics, Inc. (AAI).
bAll events resolved; authors report an additional AE (large herniated nucleus pulposus occurring months following injection; unclear if procedure related or progression of degenerative process).
cNasopharyngitis most common in the Novocart Disc (ND) plus group (n = 3); not associated with sequestrectomy or implantation; additional AEs not described.
dEvents determined by investigator to be related to sequestrectomy and study treatment; including 1 patient with intervertebral disc protrusion (ND Plus group) and 1 patient with spinal pain after implant (ND Basic group).
Autologous Cell Sources
Evidence for the safety of cell therapy across 5 small case series of autologous cells sources was sparse and poorly reported. The need for subsequent surgery was reported across 3 series was high (6% to 80%) (Table 5). The patient populations consisted of those who had already failed conservative care. No serious adverse events (treatment related or otherwise) were observed in the 4 series reporting on such events; however, studies may have been underpowered to detect such events. Two series reported that no nonserious treatment-related adverse events were observed 29,45 and 1 series reporting pain-related events that resolved. 43
One small, moderately high risk of bias phase I pilot RCT (N = 24) 50 comparing autologous disc chondrocyte transplantation with Novocart Disc Plus (ND Plus) versus Novocart Disc Basic (ND Basic) reported preliminary safety data through 6 weeks only, of patients with symptomatic low back pain who failed adequate conservative or interventional treatment. Sequestrectomy of the affected disc was performed and the extracted tissues were transferred for manufacturing of ND Plus. The pilot was considered of poor quality due to inadequate concealment of treatment allocation, differential loss to follow-up, and differences in patient baseline characteristics (the ND Plus group had higher proportion of patients that were male, and proportions who reported tobacco use and full-time work; fewer ND Plus patients had adjacent degenerative disc disease and reported less analgesic medication use, particularly NSAIDS. Adverse events were more common in the ND Plus group (50%, 6/12) compared with the ND Basic group (25%, 2/8) and only 1 treatment event was considered serious (IVD protrusion) and the patient underwent further surgery. Authors reported nasopharyngitis as the most common event. Firm conclusions regarding the relative safety of the two cell preparations were not possible given the study limitations.
Key Question 3: Modification of Treatment Effect
Allogenic Cell Sources
Included studies were not designed to evaluate modification of treatment by demographic or other factors and none reported subgroup analyses on factors of interest (eg, number of treated levels).
Autologous Cell Sources
Included studies were not designed to evaluate modification of treatment by demographic or other factors and with one exception did not provide information on such factors. One small (N = 26) case series 48 provided limited subgroup data for patients who had 1- versus 2-level injection, those aged ≤40 years old versus >40 years old and for MSC concentrations of <2000 CFU-F (colony-forming unit fibroblasts) with >2000 CFU-F (Table 6). Statistical analyses were only reported for the comparison of cell concentrations. Authors reported that mean ODI and VAS scores were significantly improved for patients receiving >2000 CFU-F compared with those receiving <2000 CFU-F. As these reports do not compare MSC to an alternative treatment, conclusions regarding modification of treatment effect (heterogeneity of treatment effect) were not possible. Conclusions regarding comparisons within the other subgroups were not possible as data provided were inadequate for analysis.
Key Question 3: Subanalyses (Across All Patients From Authors’ Original Population; Pettine, 2015).
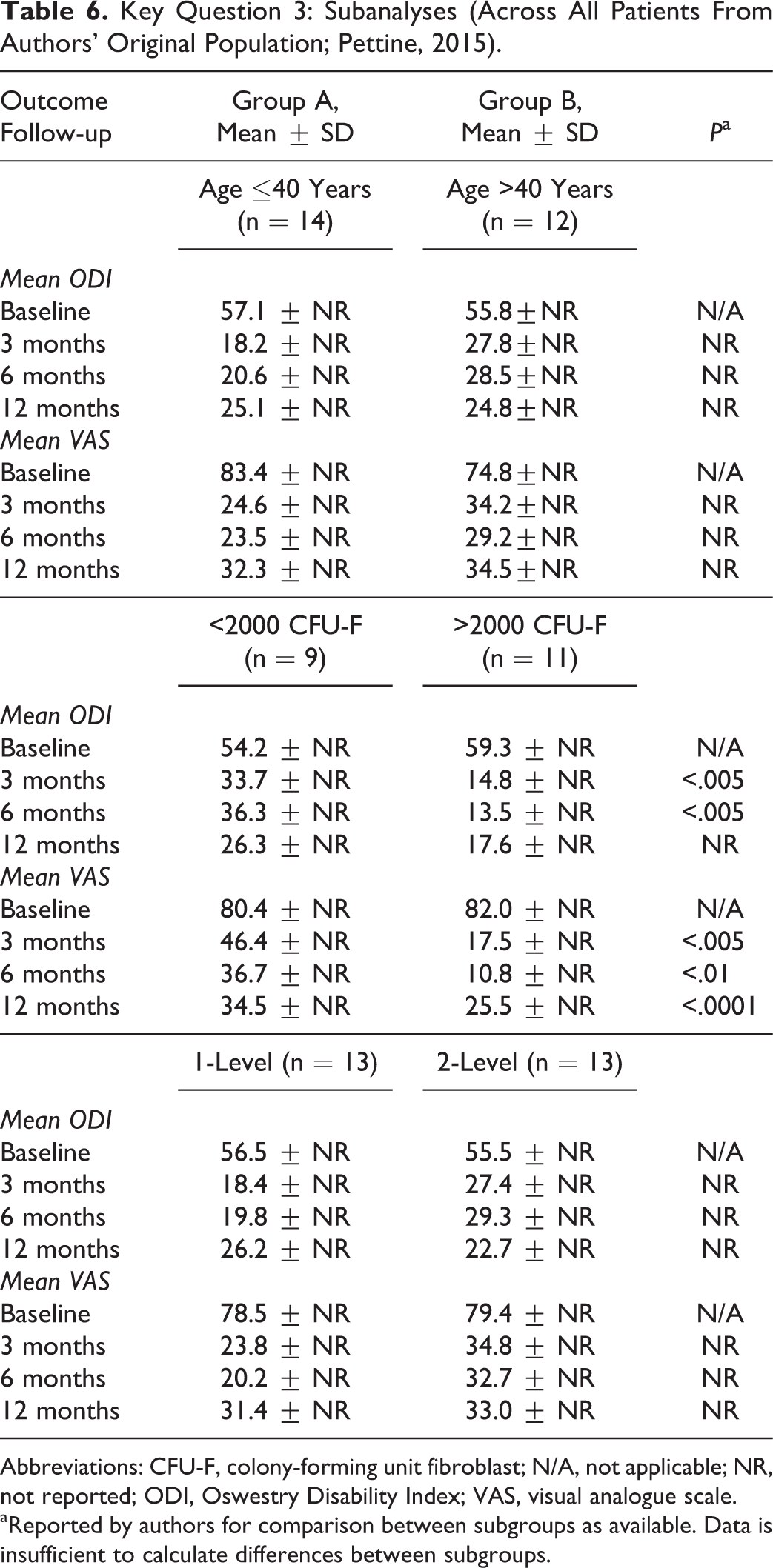
Abbreviations: CFU-F, colony-forming unit fibroblast; N/A, not applicable; NR, not reported; ODI, Oswestry Disability Index; VAS, visual analogue scale.
aReported by authors for comparison between subgroups as available. Data is insufficient to calculate differences between subgroups.
Key Question 4: Economic Studies
No full economic studies were identified for either lumbar or cervical IVD.
Evidence Summary, Overall Quality (Strength) of Evidence
No evidence on use of cell therapy for cervical IVD repair was identified. Studies of cell therapy for lumbar IVD repair primarily consisted of small case series. The quality of evidence was very low with regard to the benefits and safety of stem cell therapy for lumbar IVD repair in patients who have failed conservative care primarily due to substantial risk of bias and lack of precision, (Tables 7 and 8).
Evidence Summary: Overall Quality (Strength) of Evidence for Effectiveness and Safety of Allogenic Cell Therapy for Lumbar Intervertebral Disc Repair.a
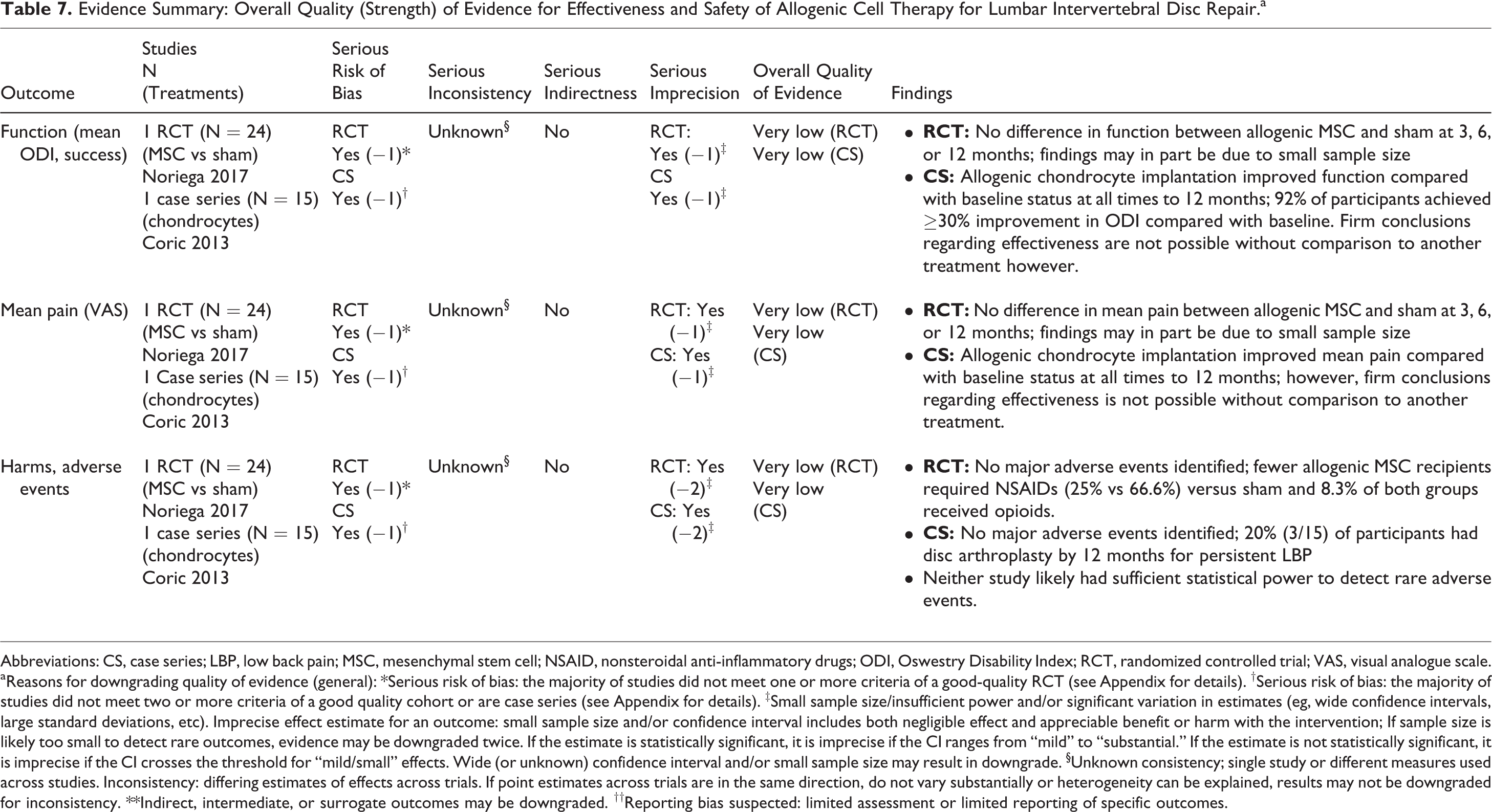
Abbreviations: CS, case series; LBP, low back pain; MSC, mesenchymal stem cell; NSAID, nonsteroidal anti-inflammatory drugs; ODI, Oswestry Disability Index; RCT, randomized controlled trial; VAS, visual analogue scale.
aReasons for downgrading quality of evidence (general): *Serious risk of bias: the majority of studies did not meet one or more criteria of a good-quality RCT (see Appendix for details). †Serious risk of bias: the majority of studies did not meet two or more criteria of a good quality cohort or are case series (see Appendix for details). ‡Small sample size/insufficient power and/or significant variation in estimates (eg, wide confidence intervals, large standard deviations, etc). Imprecise effect estimate for an outcome: small sample size and/or confidence interval includes both negligible effect and appreciable benefit or harm with the intervention; If sample size is likely too small to detect rare outcomes, evidence may be downgraded twice. If the estimate is statistically significant, it is imprecise if the CI ranges from “mild” to “substantial.” If the estimate is not statistically significant, it is imprecise if the CI crosses the threshold for “mild/small” effects. Wide (or unknown) confidence interval and/or small sample size may result in downgrade. §Unknown consistency; single study or different measures used across studies. Inconsistency: differing estimates of effects across trials. If point estimates across trials are in the same direction, do not vary substantially or heterogeneity can be explained, results may not be downgraded for inconsistency. **Indirect, intermediate, or surrogate outcomes may be downgraded. ††Reporting bias suspected: limited assessment or limited reporting of specific outcomes.
Evidence Summary: Overall Quality (Strength) of Evidence for Effectiveness and Safety of Autologous Cell Therapy for Lumbar Intervertebral Disc Repair.a
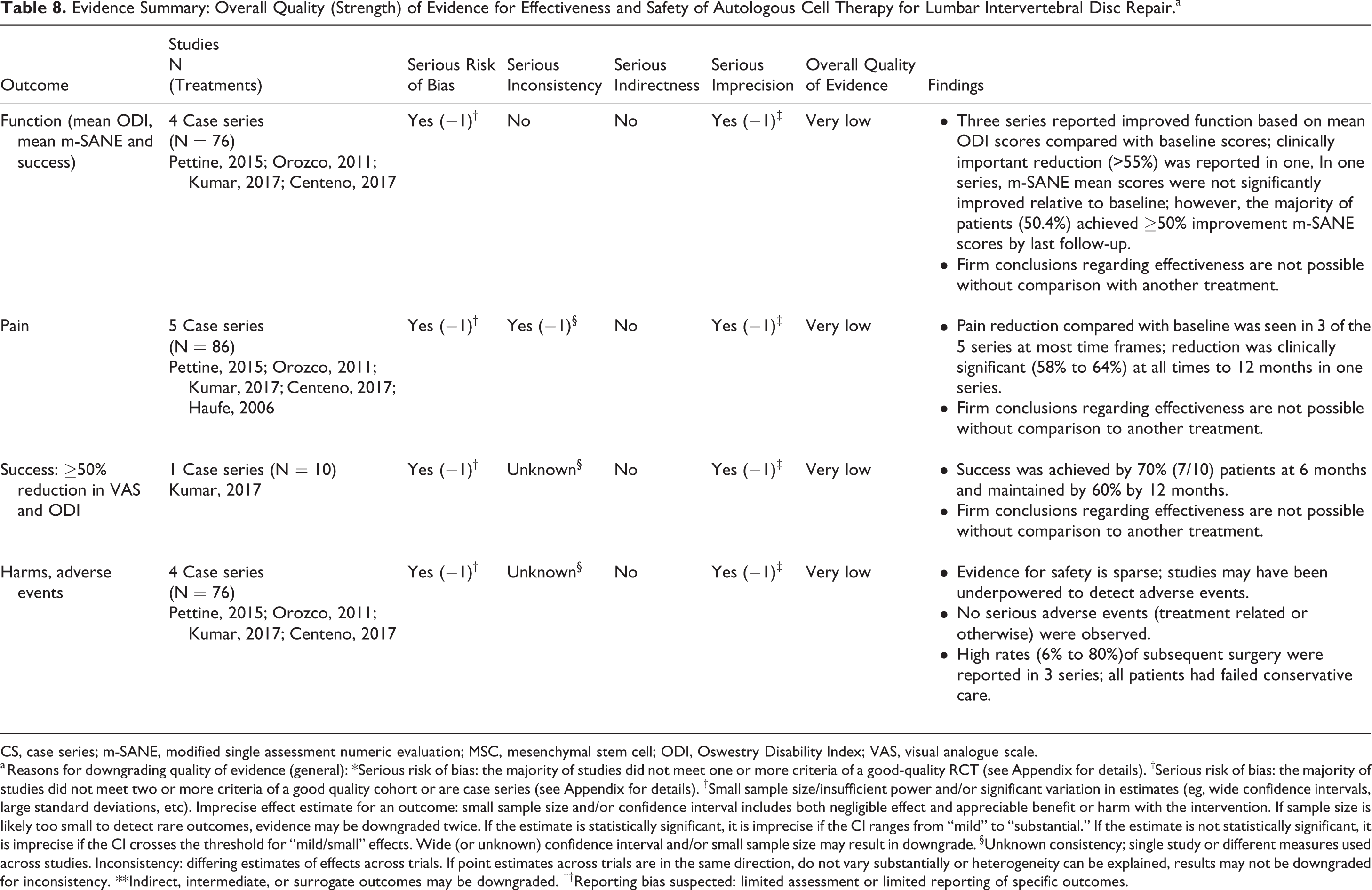
CS, case series; m-SANE, modified single assessment numeric evaluation; MSC, mesenchymal stem cell; ODI, Oswestry Disability Index; VAS, visual analogue scale.
a Reasons for downgrading quality of evidence (general): *Serious risk of bias: the majority of studies did not meet one or more criteria of a good-quality RCT (see Appendix for details). †Serious risk of bias: the majority of studies did not meet two or more criteria of a good quality cohort or are case series (see Appendix for details). ‡Small sample size/insufficient power and/or significant variation in estimates (eg, wide confidence intervals, large standard deviations, etc). Imprecise effect estimate for an outcome: small sample size and/or confidence interval includes both negligible effect and appreciable benefit or harm with the intervention. If sample size is likely too small to detect rare outcomes, evidence may be downgraded twice. If the estimate is statistically significant, it is imprecise if the CI ranges from “mild” to “substantial.” If the estimate is not statistically significant, it is imprecise if the CI crosses the threshold for “mild/small” effects. Wide (or unknown) confidence interval and/or small sample size may result in downgrade. §Unknown consistency; single study or different measures used across studies. Inconsistency: differing estimates of effects across trials. If point estimates across trials are in the same direction, do not vary substantially or heterogeneity can be explained, results may not be downgraded for inconsistency. **Indirect, intermediate, or surrogate outcomes may be downgraded. ††Reporting bias suspected: limited assessment or limited reporting of specific outcomes.
Discussion
The overall strength of evidence for efficacy and safety of cell therapy for lumbar IVD repair was very low. No studies focusing on cervical spine were identified. Cellular therapies for IVD regeneration propose to restore nucleus pulposus and maintain normal extracellular matrix production by injecting allogenic or autologous disc cells, chondrocytes, or undifferentiated stem cells. Immunomodulatory effects of MSCs on NP cells in response to inflammatory cytokines could potentially prevent the aggravation of inflammatory cascade, thereby obviating ingrowth of pain-inducing vasculature and nerve fibers. 18 In our analysis, one study showed clinically significant (>55%) reduction in ODI 47 -49 while in another study clinical treatment success was achieved in 70% of the patients. 45 Three studies reported improved VAS scores using autologous cell based intervention 29,45,47 -49 whereas 2 studies using BMA or hematopoietic stem cells BMA, showed no improvement with autologous cell-based intervention. 30,43 Need for subsequent surgery after cell therapy could not be clearly determined due to the inconsistency and disparity across the studies. Analysis across few studies showed need for subsequent surgery ranging from 6% to 80%. 30,43,44,47 -49
Among several factors defining efficacy and feasibility, the disc level and severity of spine pathology are major factors dictating the success of cell transplantation. Moderate disc degeneration has been considered as an optimal target for stem cell therapy. 51 Two studies 44,45 indicated clinical improvement with autologous adipose tissue–derived MSCs (AT-MSCs) and allogenic juvenile chondrocytes in Pfirmann grade III-IV discs, respectively. In another study, patients with Pfirmann grade IV-VII showed significant improvement in VAS scores as well. 47 -49 Noriega et al 46 included patients with Pfirmann grade II and reported improvement with allogenic MSCs compared with the baseline measurement. Results from these studies support the notion that cell therapy has a potential to reverse degenerative cascades.
The use of allogenic MSCs remains a significant issue due to the potential of immune rejection. Additionally, the injected dose and cell viability are key variables. Coric et al 44 transplanted a wide range of juvenile derived chondrocytes (between 6.75 and 13.5 × 106 cells/mL) and demonstrated promising results for the use of juvenile-derived chondrocytes. Considering that disc is acellular and aging reduces cell density, cell doses exceeding the normal range might not prove beneficial in obviating degeneration. Thus, a low cell dose might be beneficial considering poor nutrient supply and hypoxic environment. Higher numbers of cells exceeding the capacity of NP might eventually lead to accumulation of dead cells, thereby invoking inflammatory response. 1 Cell leakage is another potential adverse event of cell-based therapies. Bertram et al 52 demonstrated up to 50% reduction in cell leakage with fibrin glue co-administration. In our systematic review, 1 study combined AT-MSCs with hyaluronic acid derivative and showed its safety and tolerability. 45
Previously, Meisel et al 53,54 have shown greater pain reduction at the 2-year follow-up in patients treated with autologous cultured disc–derived chondrocytes compared with patients who received surgical intervention. However, the autologous, noncultured cells reduce the risks of rejection, disease transmission, sample mismatch compared with culture expanded autologous or allogenic cells. Moreover, culture conditions (eg, media reagents, oxygen concentration, pH, etc) might affect cell characteristics and efficacy. Pettine et al 48 showed significant clinical improvement with uncultured BMA MSCs. Kumar et al 45 used AT-MSCs, where cell extraction is less invasive compared with bone marrow. AT-MSCs have additional advantage as they express higher levels of TβRIII, thus have a higher chondrogenic potential. 55
Hernigou et al 56 reported no increased incidence of cancers with autologous BMC injections for up to 22 years posttreatment. Concerns remain, however, about potential systemic infections, tumor growth, and other adverse events with the use of cell therapies. The studies in this systematic review did not report any major adverse events, however it is highly likely that studies included in the review were not equipped sufficiently to identify rare events. To address the host acceptability for the transplanted cells, monitoring of pro-inflammatory response indicators such as C-reactive protein might be helpful in identifying complications like an autoimmune response. Tschugg et al 50 applied this approach to identify incidence of immunological adverse events after intradiscal injection in the ND Plus and ND Basic cohorts. The study showed no indication of clinically significant immunological consequences. 50
Evidence for the efficacy and safety of cell therapy for lumbar IVD repair (allogenic or autologous) was very low, primarily due to the high risk of bias and lack of RCTs. While most case series suggested improved function and pain following cell therapies, the results need to be considered within the context of these limitations. It is not clear to what extent benefits would be seen if directly compared with other minimally invasive or surgical treatments. The only RCT in this systematic review found no difference between allogenic and sham groups in pain or function up to 1 year but may have been underpowered to detect differences between groups. The identified studies lacked subgroup analyses to determine association between patient characteristics or comorbidities with cell therapy success rate.
Furthermore, in our analysis no publications on cervical IVD repair met the inclusion criteria. No conclusion about cost-effectiveness of cell therapy over surgical treatment could be derived due to the lack of comparative economic studies. Low back and neck pain are one of the main drivers of years lived with disability worldwide. In the United States alone, the annual cost for the treatment of chronic low back pain exceeds $100 billion. 57
Conclusions regarding safety are limited. While no serious adverse events were reported, sample sizes were likely inadequate to detect events, particularly those considered to be rare. Despite favorable risk-benefit ratio indicated by clinical studies, clinical evidence for cell based therapies needs to be established.
Conclusions
The quality of evidence for the use of either allogenic or autologous cells for IVD repair was very low. Studies lacked tools to assess treatment heterogeneity depending on patient characteristics, co-intervention or other factors. While no serious adverse events were reported, sample sizes were likely inadequate to detect adverse events, particularly those considered to be rare. To evaluate the efficacy and safety of cell therapies for IVD repair, high-quality comparative studies are needed.
Supplemental Material
Supplemental Material, GSJ_Supplemental_Material - Cell Therapy for Treatment of Intervertebral Disc Degeneration: A Systematic Review
Supplemental Material, GSJ_Supplemental_Material for Cell Therapy for Treatment of Intervertebral Disc Degeneration: A Systematic Review by Dino Samartzis, Niccole M. Germscheid, Michael G. Fehlings, Charles G. Fisher, Marinus de Kleuver, F. Cumhur Öner, S. Tim Yoon, Luiz R. Vialle, Hans-Joerg Meisel, Neha Agarwal, Patrick C. Hsieh, Andrea Skelly, Jong-Beom Park, Darrel Brodke, Jeffrey C. Wang, S. Tim Yoon and Zorica Buser in Global Spine Journal
Footnotes
Acknowledgments
The authors wish to thank Aaron Ferguson for performing literature searches, managing citations, data abstraction, and editing of results tables.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Disclosures outside of submitted work: ZB—consultancy: Xenco Medical, AO Spine (past); Research Support: SeaSpine (paid to the institution). HJM—Dr Meisel is consultant (money paid to institution) - Regenerate Life Sciences GmbH for DiFusion (ongoing), Co.don (past); royalties from: Medtronic, Fehling Aesculap (past); stocks (money paid to institution) - Regenerate Life Sciences GmbH in DiFusion. STY—Dr Yoon owns stock in Phygen, Alphatec; Meditech, royalties Meditech Advisors, Stryker Spine (Paid directly to institution/employer), grant from AOSpine (Paid directly to institution/employer), research support from Biomet (Research support given to AREF), non financial research support from Nuvasive and Medtronic. DB—Consultant – Vallum, Royalties – America, DePuy Synthes, Medtronic, Fellowship Support – AOSpine (paid directly to institution). JCW—Royalties – Biomet, Seaspine, Amedica, DePuy Synthes; Investments/Options – Fziomed, Promethean, Paradigm Spine, Benvenue, Nexgen, Vertiflex, Electrocore, Surgitech, Expanding Orthopedics, Osprey, Bone Biologics, Pearldiver; Board of Directors - North American Spine Society, North American Spine Foundation, AO Foundation, Cervical Spine Research Society; Fellowship Funding (paid to institution): AO Foundation. PCH—Consulting: DePuy Synthes, Medtronic, NuVasive, Zimmer Biomet.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Aggregate Analytics, Inc, received funding from AO Foundation to perform the methodological and analytical aspects of this review. This study was organized and funded by AOSpine International through the AOSpine Knowledge Forum Degenerative, a focused group of international spine experts acting on behalf of AOSpine. Study support was provided directly through the AOSpine Research Department.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.