
Abstract
Study Design
Systematic review.
Objective
Ceramic-based bone grafts have been widely utilized to reduce the need for iliac crest bone grafting given the complications associated with the harvest of iliac crest autograft. As a family, ceramics vary widely based on differences in composition, manufacturing, porosity, and structure, which may ultimately affect their efficacy. This article reviews the current data of ceramics used in different environments in the lumbar spine to achieve arthrodesis.
Methods
Medline, EMBASE, and Cochrane Central Register of Controlled Trials were searched for publications from 1980 to 2013 involving ceramic-based bone grafts in the lumbar spine. Variables such as age of patients, volume of ceramic, procedure, time to evaluation, method of evaluation, specific composition of ceramic, adjuncts used with ceramic products, type of fusion, and fusion rate were compared using a multivariate logistic regression model.
Results
Thirty studies with 1,332 patients met the final inclusion criteria. The overall fusion rate for all ceramic products as a bone graft extender in the lumbar spine was 86.4%. Age, gender, method of evaluation (plain radiographs, computed tomography, or combination), or specific ceramic product did not significantly affect fusion rate. Ceramics used in combination with local autograft resulted in significantly higher fusion rates compared with all other adjuncts, and bone marrow aspirate and platelet concentrates resulted in significantly lower fusion rates.
Conclusions
Ceramic-based bone grafts represent a promising bone graft extender in lumbar spine fusion when an osteoinductive stimulus, such as local bone graft is available.
Introduction
Lumbar spine fusions are performed at a rate of 200,000 per year in the United States 1 ; yet, the choice of graft used by each surgeon varies. 2 Historically, autologous iliac crest bone graft has been the gold standard for lumbar arthrodesis; however, postoperative pain, complications, and patient preference have led to the rapid decline in its recent use. 3 , 4 , 5 Consequently, the spinal biologics arena has exploded in new products, research, and applications.
Ceramic-based bone grafts are synthetic products that have been widely utilized to reduce the need for iliac crest bone grafting. Ceramic matrices are inorganic, ionically bonded preparations that comprise a large collection of bone graft substitutes. 6 As a family, ceramics vary widely based on differences in composition, manufacturing, porosity, and structure. Ceramic products include a variety of compounds including tricalcium phosphate, calcium sulfate, and hydroxyapatite. Each of these possible components has different binding, biodegradability, and mechanical properties.
Ceramic scaffolds can be constructed to mimic the mineral phase of bone and are available as compact or porous forms. Porosity allows for mesenchymal cell adhesion, proliferation, and differentiation into mature osteoblasts. 7 The greater the porosity of a ceramic, the more its mechanical strength and resorption rate are compromised. 6 Optimal pore size has been reported between 150 and 500 µm to enhance interface activity, bone ingrowth, and biodegradation. 8 Ceramic matrices are inherently brittle with low fracture resistance and tensile strength, thus have been used with rigid internal fixation in orthopedic applications, which protects from loading forces until host bone ingrowth has occurred. 7
Ceramics provide a reliable osteoconductive matrix but in general, lack osteoinductive potential. Consequently, successful arthrodesis rates are substantially higher when utilized with a source of cells such as local autograft or bone marrow aspirate. Ceramics are biodegradable; however, remodeling occurs by a different process than normal bone remodeling. Material is resorbed through foreign-body giant cells, instead of osteoclasts, and complete resorption may not occur for up to 10 years. 9
Ceramics offer several advantages compared with other bone graft substitutes. They are biologically inert and generally do not induce a host inflammatory response. In addition, they are able to be sterilized without loss of structural integrity, minimizing the risk for disease transmission. Also, ceramics can be cut and molded into various shapes to appropriately match different environments such as those in posterolateral and interbody lumbar fusions. Finally, the cost of ceramics is traditionally less than that of other bone graft substitutes such as growth factors. 6 , 7
Although the use of ceramic-based scaffolds in spine surgery has dramatically increased in recent years, a systematic review of these studies has yet to be performed. This article will review whether ceramics are an adequate bone graft extender with autogenous bone graft in lumbar spine arthrodesis.
Methods
Medline, EMBASE, and Cochrane Central Register of Controlled Trials were searched for publications from 1980 to 2013 using a combination of the keywords “lumbar spine fusion,” “ceramic,” “arthrodesis,” “calcium phosphate,” “hydroxyapatite,” and “calcium sulfate.” Query results were reviewed by two independent observers, and articles for inclusion in this study were selected using the following criteria:
Original clinical research studies involving the use of ceramic-based bone grafts in lumbar spine arthrodesis in patients over the age of 18
Level of evidence of IV or above, graded and agreed upon according to Journal of Bone and Joint Surgery (American Edition) guidelines by two independent reviewers 10
Sample size of >10 patients with a diagnosis of either lumbar spondylolisthesis and/or degenerative disk disease
Lumbar fusion procedure from one to three levels
Fusion rate outcome reported with a minimum of 1-year radiographic follow-up (either plain radiograph or computed tomography [CT] scanning)
Published in English
After an initial query of 80 studies, 30 met all of the inclusion criteria (Fig. 1). For clinical studies that met the inclusion criteria, fusion rate was defined by plain radiographs alone (40%), CT scan (13%), or a combination thereof (47%; Table 1). Of the studies that used plain radiographs alone, 50% used flexion-extension radiographs and 50% used static radiographs. CT scans were often used in cases of disagreement between independent reviewers or to confirm pseudarthrosis. It should be noted that several studies included in this analysis used plain radiographs to determine fusion status of interbody fusions (64% of interbody studies).
Fusion rate by X-ray versus CT

Abbreviation: CT, computed tomography.
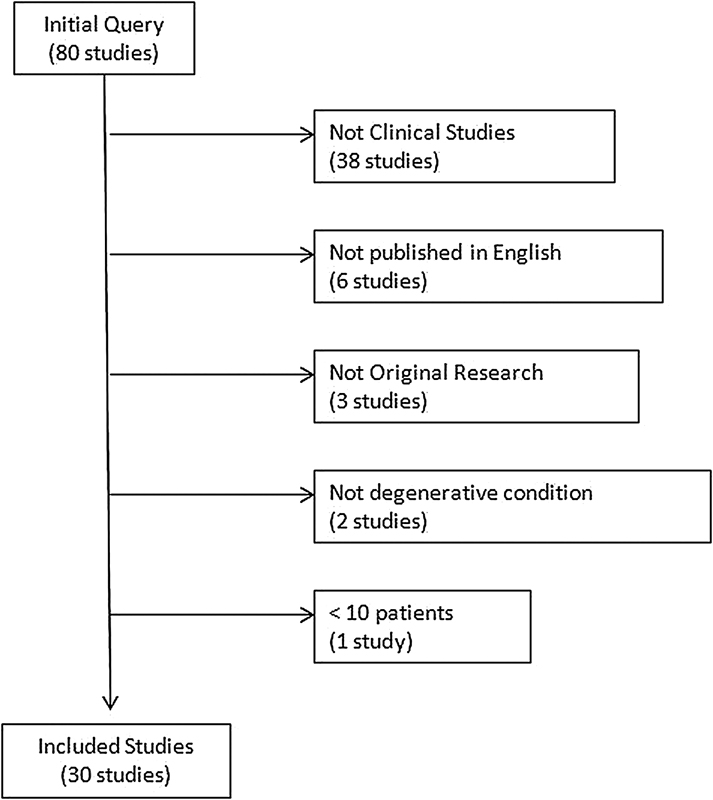
Query results and exclusion.
Continuous variables such as age of patients, volume of ceramic, time to evaluation, and fusion rate were compared using multivariate logistic regression models with a p < 0.05 considered statistically significant. SAS 9.2 statistics packed was used (SAS Institute, Inc., Cary, NC), and all analyses were conducted using PROC GLIMMIX and PROC LOGISTICS procedures.
Results
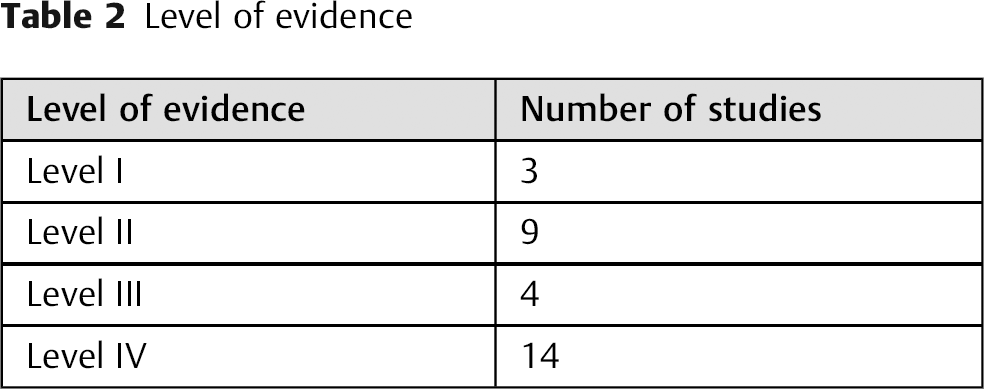
A total of 30 studies met the final inclusion criteria (Fig. 1). 11 , 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36 , 37 Level of evidence varied with three studies reaching level I criteria (Table 2). Collectively, a total of 1,332 patients were included for this review. Twenty studies described using ceramics as granules, six as strips, three as blocks, and one study was indeterminate. The volume of ceramic used averaged 8.7 cc/level (range 5 to 22 cc) and volume of ceramic used had no correlation to successful fusion (p = 0.45). The dimensions of ceramic strips or blocks varied widely depending on the study.
Level of evidence
The overall successful fusion rate for all ceramic products as a bone graft extender in the lumbar spine was 86.4%. Age or gender did not significantly affect fusion rate (p = 0.19). Reported fusion rate did not differ depending on evaluation method (plain radiographs, CT scan, or combination; Table 1). Time to evaluation of fusion status significantly affected fusion rates and ranged from 12 to 70 months. The longer the time, the greater the fusion rate (p = 0.03).
Ceramics were almost exclusively used as bone graft extenders with a variety of adjuncts (Table 3). In some studies, adjuncts were also used together such as bone marrow aspirate (BMA) and local autograft (five studies), iliac crest autograft and demineralized bone matrix (one study), and local autograft and platelet concentrates (two studies). Two studies used ceramic products alone. One study used a ceramic product as part of an anterior interbody fusion with a titanium locking plate and reported a fusion rate of 90%. The second study used a ceramic product as part of a circumferential fusion and reported a fusion rate of 77.6%. Local autograft alone with a ceramic bone graft extender (10 studies, 453 patients) demonstrated a fusion rate of 89.8% (range 52.6 to 100%), which was significantly greater when compared with all other adjuncts (p = 0.01; Table 3). Notably, ceramics plus bone marrow aspirate alone resulted in a significantly reduced fusion rate compared with all other adjuncts (72.6%, p = 0.03). Bone marrow aspirate was obtained from the iliac crest in all of the included studies. Ceramics when combined with local autograft and platelet concentrates resulted in a significantly lower fusion rate (78.2%, p = 0.01).
Fusion rate by adjunct
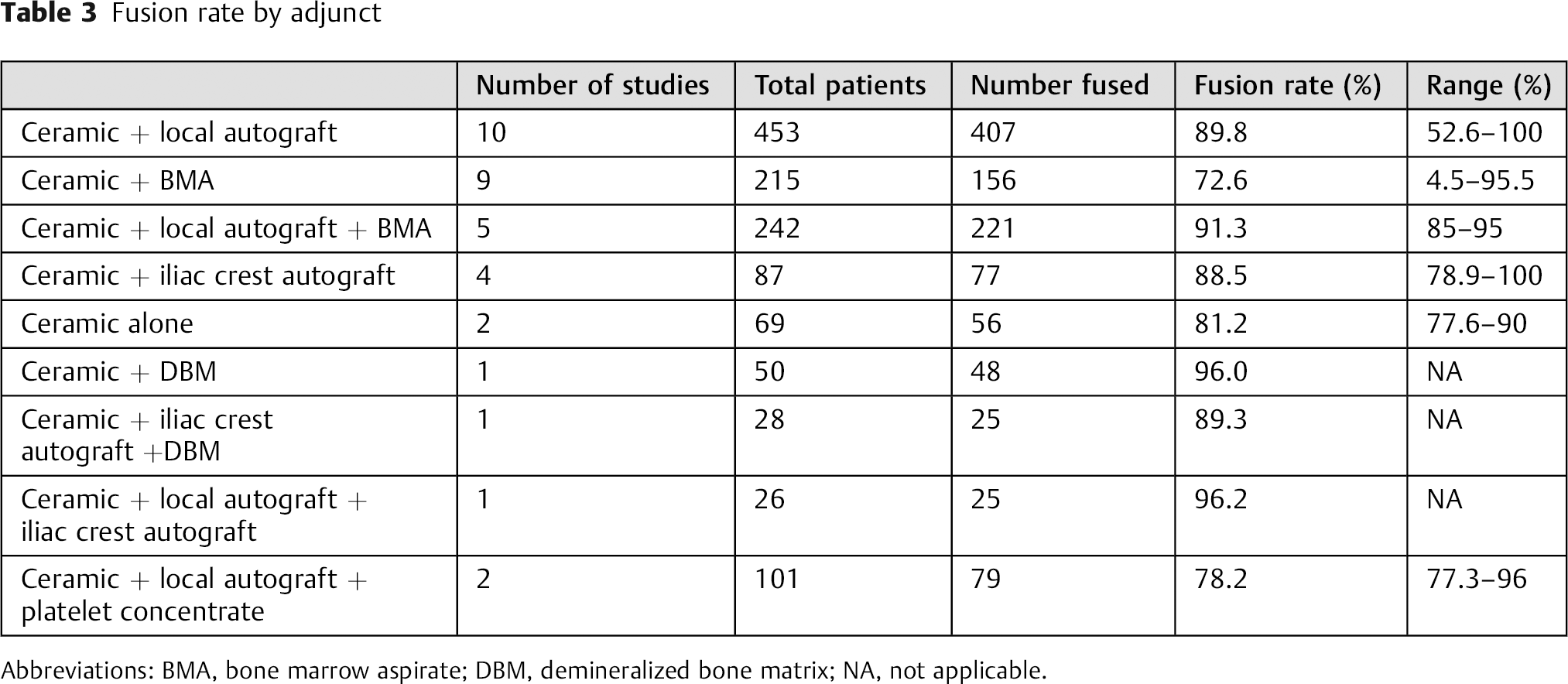
Abbreviations: BMA, bone marrow aspirate; DBM, demineralized bone matrix; NA, not applicable.
Posterolateral intertransverse fusion technique was used in 24 studies with 994 total patients, with a reported fusion rate of 85.6% (Table 4). Because all of the interbody fusion studies included posterior instrumentation, they were grouped together as circumferential fusions, which included anterior (four studies), posterior (six studies), and transforaminal interbody (two studies) techniques. The fusion rate with the circumferential technique was 88.8%, which was not significantly greater than that of posterolateral fusion alone (p = 0.64).
Fusion rate by procedure
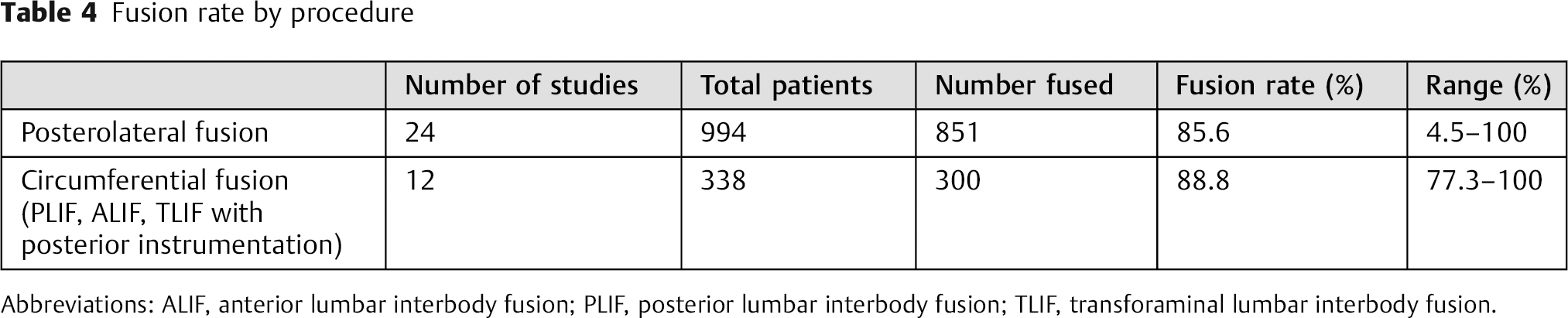
Abbreviations: ALIF, anterior lumbar interbody fusion; PLIF, posterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion.
Although a plethora of different compositions of ceramic products were reported (Table 5), there was no statistically significant difference in fusion rates between the different compositions utilized.
Fusion rate by product
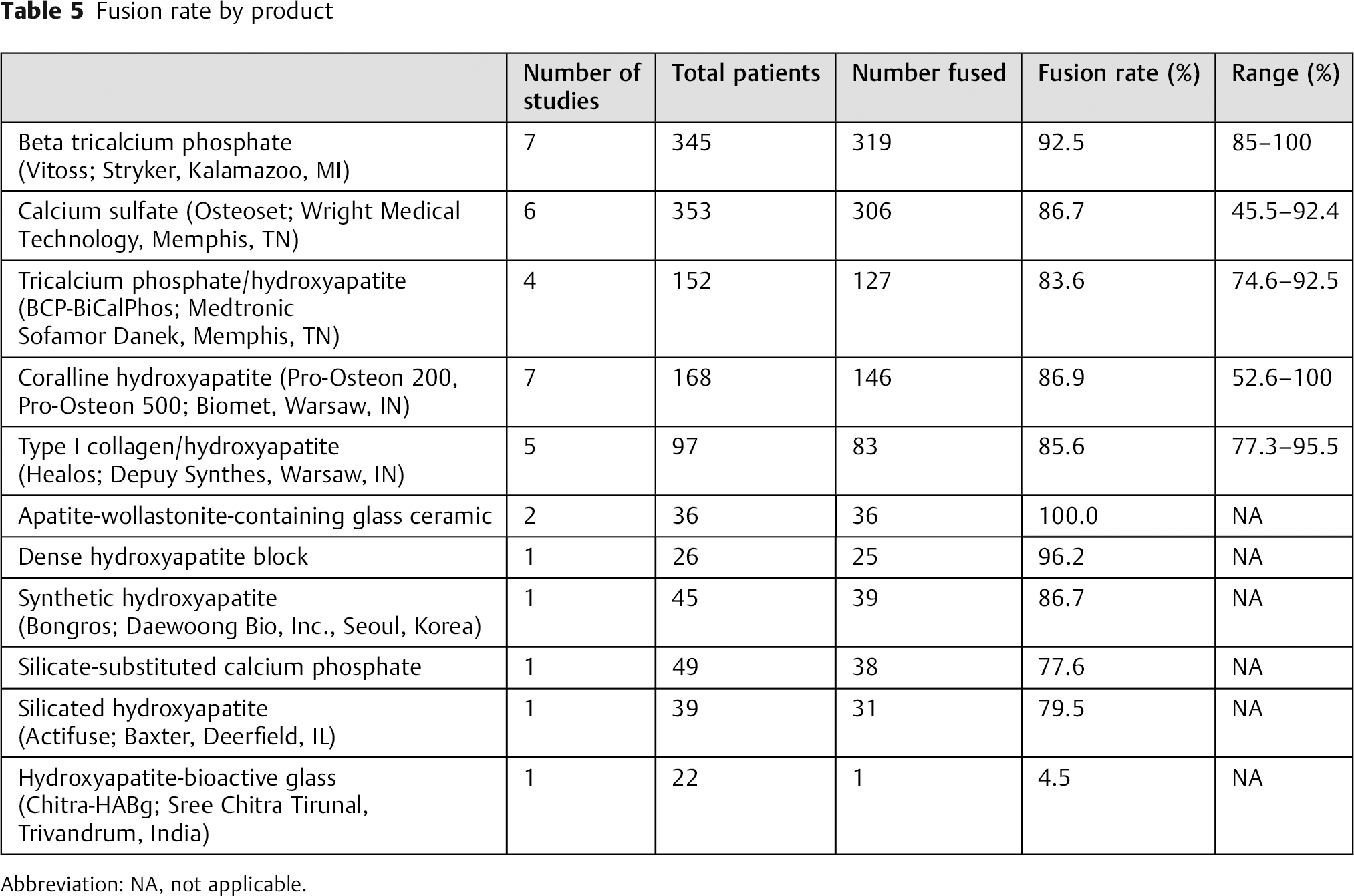
Abbreviation: NA, not applicable.
Discussion
Ceramic-based bone grafts compose one member of the heterogeneous family of spinal biologics. Ceramics offer several advantages compared with other bone graft extenders such as inertness, ease of sterilization, flexibility of shape, and safety profile. However, ceramics harbor low tensile strength, susceptibility to fracture, and a need for an osteoinductive adjunct that can pose limitations to its use. Despite these limitations, ceramics have been studied extensively as a bone graft extender for lumbar spine fusion.
Data from a total of 30 studies examining over 1,300 patients who underwent lumbar spine arthrodesis with a ceramic as a bone graft extender demonstrate a fusion rate of 86.4%, which is comparable to that of historically reported rates from iliac crest bone graft in the same anatomic location. Three level I studies analyzed the use of a ceramic product as part of a lumbar arthrodesis. Korovessis et al prospectively divided 60 patients with degenerative lumbar stenosis and instability who underwent decompression and posterolateral fusion to receive iliac crest bone graft or hydroxyapatite mixed with local autograft and bone marrow aspirate. 11 Fusion was evaluated at 2 years postoperatively with plain radiographs and CT imaging. Nineteen of 20 patients had successful fusion in the autologous iliac crest bone graft cohort compared with 18 of 20 patients in the ceramic with local autograft and BMA cohort. Dai and Jiang prospectively randomized 62 patients undergoing single-level instrumented posterolateral lumbar fusion for degenerative lumbar spinal stenosis over a 2-year period to use either β-tricalcium phosphate (TCP) with local autograft or autogenous iliac crest bone. 16 Fusion was evaluated at 24 to 36 months postoperatively with flexion-extension radiographs. All patients in this study demonstrated successful fusion. Finally, Kanayama and colleagues prospective randomized 20 patients with degenerative spondylolisthesis to either hydroxyapatite-TCP granules with local autograft or osteogenic protein-1 putty as part of a single-level posterior arthrodesis. 23 Nine of 10 patients in the ceramic group demonstrated radiographic evidence of arthrodesis at 1 year on flexion-extension radiographs.
Local autograft appears to be the ideal adjunct to accompany a ceramic extender (limited recommendation). Local autograft is the most frequently studied (35% of patients), leads to higher fusion rates than other treatments, and can be harvested from the same incision as the surgical procedure. Although local autograft has led to high fusion rates in posterolateral fusion, 38 , 39 oftentimes the volume of graft is insufficient to achieve adequate load transfer. 40 In these cases, a bone graft extender is indicated to increase the chance of success.
Patients who had bone marrow aspirate alone as an adjunct experienced a significantly lower fusion rate compared with those in other treatment groups. The most likely explanation for this finding is the fact that the technique, volume, and processing methods of BMA were not standardized across the studies included for analysis. In unconcentrated aspirate, there may be an insufficient quantity of cells and growth factors necessary to induce reliable fusion. Patient factors can also influence the quality of the bone marrow aspirate that is obtained 41 ; the poorer the health of the patient, the poorer the quality of the bone marrow aspirate. Finally, platelet concentrates had lower fusion rates when combined with local bone and a ceramic extender, which is consistent with other reports utilizing platelet concentrates. 42 , 43
Because the prospect of achieving a solid bony fusion in the lumbar spine differs depending on surgical technique such as posterolateral, posterior interbody, and anterior interbody surgery, biologics in these environments need to be evaluated separately. Fusion rates did not significantly differ in circumferential fusions compared with posterolateral techniques alone. Although fusion rates are typically higher with circumferential fusion, the variability in assessing fusion status and the number of included patients may have contributed to the lack of difference between the groups. Despite these limitations, the data in this study suggest that ceramic-based scaffolds are an effective bone graft extender in each of these anatomic locations, including the posterolateral space that is under tensile forces (limited recommendation).
Ceramic-based bone grafts are comprised of a variety of individual compounds, such as collagen, tricalcium phosphate, calcium sulfate, and hydroxyapatite. Cell adhesion, biodegradability, and mechanical properties differ for each of these components. For example, calcium sulfate is completely resorbed in vivo within several weeks, 44 as opposed to hydroxyapatite that can take years to biodegrade. Tricalcium phosphate and coralline hydroxyapatite typically have greater porosity to allow for cell adhesion and growth compared with other ceramic components. Despite the inherent differences between each product's composition, processing techniques, and formulation, with the number of studies included and limitations of this review, no difference in fusion rates was found.
There are limitations to the conclusions made from this study. Approximately half the studies included were level IV, limiting the strength of the conclusions. Although all studies included patients with a degenerative lumbar pathology, critical exclusion criteria were not standardized. As a result, important patient variability could have influenced fusion rates including cigarette smoking, immunosuppression, and medical comorbidities. Also, given the lack of standardization and variability in reporting, we were unable to obtain information on other important complications such as infection. In addition, radiographic reporting methods varied among studies, which could certainly affect outcomes. Finally, because volume and technique of ceramic use was so inconsistently reported, recommendations could not be drawn from these data.
Conclusions
Ceramic-based bone grafts represent a promising bone graft extender in lumbar spine fusion when an osteoinductive stimulus, such as local bone graft, is available. In a research environment where an urgent need for more clinical data for biologic product exists, ceramics are a relatively well-studied class of products to achieve successful lumbar arthrodesis.
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this article.