
Abstract
Study Design:
Ambispective observational cohort study.
Objectives:
Synthetic graft usage avoids morbidity associated with harvest and reduces operative time. This study aims to evaluate outcomes of anterior cervical stabilization surgery using a synthetic cage in comparison with iliac crest bone graft (ICBG) following cervical spine trauma.
Methods:
An ambispective review was conducted on patients from the Alfred Trauma Registry. Consecutive patients treated at a level 1 trauma center, aged 18 years and older who were treated with standalone anterior cervical stabilization following spine trauma (2011-2016) were included in the study. Primary outcome measures were patient overall satisfaction, Neck Disability Index (NDI), neck pain 10-point visual analogue scale (VAS-neck) and arm pain 10-point visual analogue scale (VAS-arm). Secondary outcome measures were radiographic evidence of fusion and rate of revision surgery. All patients had follow-up for at least 1 year.
Results:
Between 2011 and 2016, 114 traumatic disc levels in 104 patients were treated. ICBG was used in 32% and polyetheretherketone (PEEK) cage in 68% of the patients. Both groups had similar demographic metrics. There was no significant difference in primary outcome measures between the graft types: (1) patient satisfaction (P = .15), (2) NDI (P = .11), (3) VAS-neck (P = .13), and (4) VAS-arm (P = .20). Radiology based fusion assessment 6 months postsurgery did not show statistical significance (P = .10). The rates of revision surgery were similar.
Conclusions:
This study showed no significant difference in patient-reported outcome measures when comparing the usage of PEEK cage and ICBG in anterior stand alone cervical spine stabilization. Level 1 evidence studies are required to further investigate this finding.
Keywords
Introduction
Subaxial cervical spine (C3-C7) is a common anatomical site for spine trauma accounting for up to 21.3% of all spine column trauma and up to 50% for traumatic spinal cord injury. 1 Cervical spine trauma resulting in morphological instability or neurological deficits requires surgical decompression, restoration, and fusion in a timely fashion for optimal results. At our center, the surgical rate for spine trauma is approximately 10%. 1 At the same time, we have high compliance with published guidelines for spine trauma surgical indications. 2
The anterior approach in cervical spine surgery first introduced by Smith and Robinson 3 in 1958 is favored over the posterior approach with all considerations being equal, as it is a minimally invasive technique with a smaller surgical footprint. 4 The minimal muscular stripping, smaller incision, and shorter anesthetic time lead to a lesser rate of surgical morbidities. 4,5 For long-term stability, intervertebral body fusion is crucial. The use of iliac crest bone graft (ICBG) is reported to result in a postoperative fusion in 81% to 100% of patients. 5 However, ICBG grafting is also associated with significant rate of morbidity, including donor site infection, wound dehiscence, hematoma occurrence, chronic pain, and dysesthesias. 6 -11 This rate is reportedly as high as 19.37% in a recent systematic review. 6 This has been shown to negatively affect health care costing due to prolonged hospitalization, corrective treatment, and chronic pain management. 12,13
As a result, synthetic cages, bone graft allograft and bone replacements were developed to prevent the morbidity associated with ICBG harvest, and to reduce anesthetic time and length of in-hospital stay. 14 Polyetheretherketone (PEEK) is a nonabsorbable biopolymer that possesses elasticity similar to cancellous bone. PEEK cages are radiolucent, allowing easier assessment of fusion compared with metallic cage. They are anatomically shaped in a variety of shapes and sizes to accommodate cervical endplate variation and can help to increase disc and foraminal height to aid in the decompression of spinal nerves. 15,16 β-Tricalcium phosphate synthetic bone graft is made of a material that is chemically similar to bone. This osteoconductive agent is fully resorbable, allowing native bone to replace the material.
This study primarily aims to evaluate the postoperative patient reported outcomes of anterior cervical stabilization surgery using PEEK cage filled with β-tricalcium phosphate in comparison with ICBG following cervical spine trauma. Secondary outcome measures were radiographic evidence of interbody fusion and rate of revision surgery.
Site and Surgical Method
The Alfred Trauma Service is a state service level 1 trauma center. It admits more than 1500 major trauma patients per year, treating more than 40% of all major trauma cases occurring in the state of Victoria, Australia. 17 About 300 to 350 patients with severe polytrauma had spine trauma, and 30% of these patients underwent spine surgery procedures. 2
The Alfred Spine Service is a combined neurosurgery-orthopedic unit. All consultant surgeons are fellowship trained. The Alfred spine trauma management is based on established spine trauma classification and treatment algorithms, achieving 96.1% compliance with the subaxial cervical spine injury classification (SLIC) and 98.9% agreement with the thoracolumbar injury classification and severity score (TLICS). 2 Anterior cervical stabilization and decompression are based on variations of the Smith and Robinson technique 3,4 for anterior cervical spine surgery. The usage of interbody graft choice is based on surgical training and personal preference. Anterior cervical locking plates were used in all patients regardless of the type of interbody graft.
Method
Study Design
The Alfred Hospital houses an established clinical-quality trauma registry, which contains minimal data set on patient demographic, details of the injury event, the nature of the injuries sustained, the treatment received and discharge status. 18 With approval from the institutional Human Research Ethics Committee, we conducted an ambispective observational review on consecutive Alfred patients, aged between 18 and 80 years, who underwent standalone anterior cervical stabilization using either PEEK cages or ICBG following spine injury from the period of January 2011 to December 2016 (inclusive). As this is an observational study, patients are not randomized into different cervical interbody graft arm of PEEK or ICBG cohorts. Patients were excluded if posterior cervical fixation was performed (n = 25) or age <18 years (n = 3). Medical records of patients who satisfied the inclusion criteria were assessed to retrospectively collect data on surgical metrics (type of cervical interbody graft, disc levels, and length of surgery), pre- and postoperative neurological impairment, cervical spine imaging findings (injury morphology, postoperative radiological fusion), and postoperative complications.
Patient-reported outcomes were assessed using a standardized questionnaire. The questionnaire, which contains patient overall satisfaction, neck disability index (NDI), neck pain 10-point visual analogue scale (VAS), and arm pain 10-VAS were mailed out to all patients at a minimum of 1 year to 5 years after surgery. Failure of questionnaire administration via return mail lead to telephone interviews.
Comparison Variables
The PEEK and ICBG study cohorts were compared in terms of their demographics, mechanism of injury, surgical metrics (type of cervical interbody graft, disc levels and anesthetic time), neurological status as defined by the ASIA (American Spinal Injury Association) Impairment Scale (AIS), 19 cervical spine imaging findings (injury morphology, postoperative radiological fusion), complications, and outcomes (surgical revision rate and ongoing symptoms). Where possible, each disc level was considered separately in this study.
Outcome Metrics
Patient-reported outcomes were (a) NDI, 20 (b) patient overall satisfaction, (c) neck pain 10-point VAS, 21 and (d) arm pain 10-point VAS. 21 The patient-reported outcome metrics were measured at a minimum of 1 year after surgery.
The NDI is a questionnaire designed to measure neck-specific disability. It includes ten items relating to pain, personal care, lifting, reading, headaches, concentration, work status, driving, sleeping, and recreation. Each item was scored from 0 to 5, giving a total maximum score of 50. The results were stratified into 5 categories. NDI scores of 0 to 4 indicates no disability, 5 to 14 indicates mild disability, 15 to 24 indicates moderate disability, 25 to 34 indicates severe disability, 35 to 50 indicates complete disability. 20 Patient overall satisfaction was stratified to “satisfied,” “neither satisfied or dissatisfied,” and “dissatisfied.”
As defined by previous studies, satisfactory outcomes for this study was defined as (a) NDI of 14 or less, 22 (b) patient satisfaction with patients being “satisfied” with their surgical outcome, (c) VAS-neck of 2 or less, 22 and (d) VAS-arm of 2 or less. 23
Radiographic evidence of postoperative interbody fusion and stability was assessed 6 months postsurgery independently by 2 investigators (HL and CK). Any disagreement was resolved by consensus with an experienced investigator (JT). Interbody fusion was defined as evidence of bone bridging and absence of radiolucent gaps between the 2 endplates and bone-graft interface in X-ray or computed tomography (CT). 24,25 Radiologic evidence of stability was defined as the absence of motion between vertebral bodies and spinous process on flexion-extension x-ray. 25
Statistical Analysis
Univariate and bivariate descriptive and inferential statistical methods were used to compare demographic, injury and surgical specific metrics between the 2 groups. The Student t test was used to analyze continuous, noncategorical data, and Fisher’s exact test for categorical data. The sample size was determined to be adequate for the number of predictive variables used in the multivariate models using previously described methods. 26 Binary logistic regression analysis was performed for identification of independent predictors of satisfactory outcomes in patients who underwent standalone anterior cervical stabilization following spine trauma. Construction of best-fit models was performed with the dependent variables being NDI of 14 or less, patient satisfaction, VAS-neck of 2 or less, and VAS-arm of 2 or less. Selection of baseline covariates as independent variables in the model was based on its P value (<.20) and significance based on previous published literature. The backward elimination method was selected to assist model creation. Statistical significance was achieved with a P value <.05. All statistical analyses were performed using STATA/IC version 14.2 (StataCorp, College Station, Texas, USA).
Results
Demographics (Tables 1 and 2)
Between 2011 and 2016, 104 patients had standalone anterior cervical stabilization surgery following trauma. A total of 114 cervical disc levels had surgical stabilization and fusion. The majority of patients had single-level surgery (n = 94, 90%). The remaining 10 patients (10%) had 2-level surgery and received PEEK cages (Table 1).
Anterior Interbody Graft Choice Metrics.
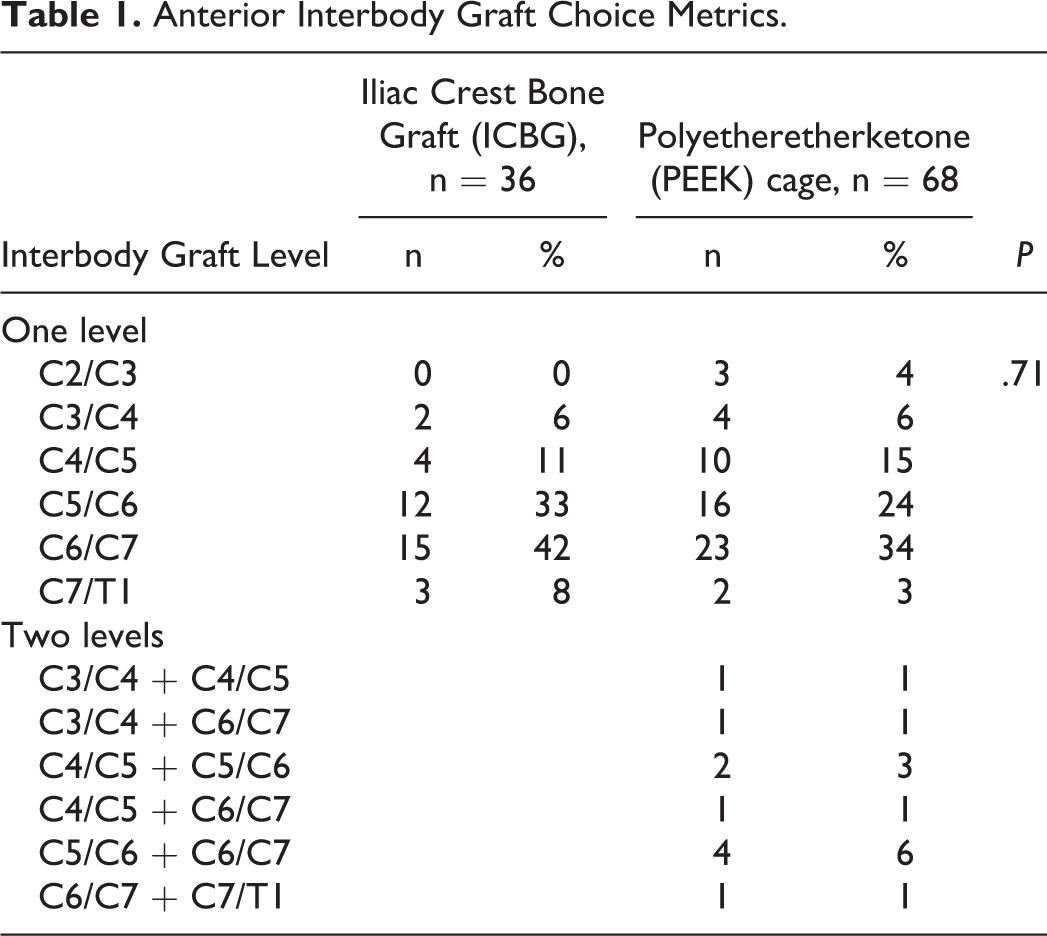
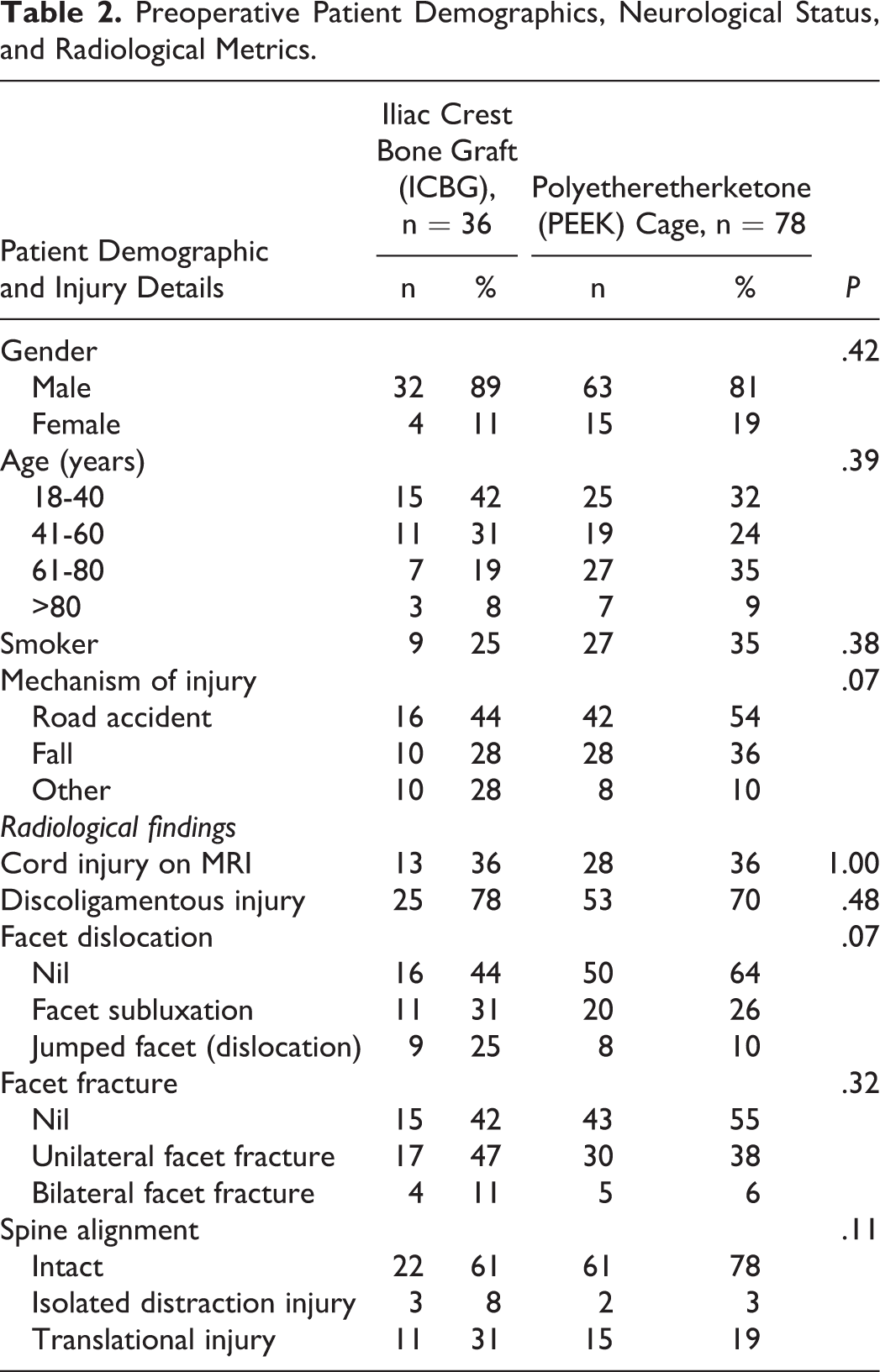
The ICBG cohort (n = 36, 32%) had a mean (±SD) age of 47.8 ± 20.2 years; a male majority (89%) and 25% were smokers. The PEEK cohort (n = 78, 68%) had similar demographics, with a mean (±SD) age of 52.3 ± 19.9 years; a male majority (81%) and 35% were smokers. Both cohorts suffered road traffic accidents as the main mechanism of injury (51%); followed by falls (33%), sporting injuries (6%), trampoline accidents (4%) and water-based accidents (3%) (Table 2).
Preoperative Patient Demographics, Neurological Status, and Radiological Metrics.
Spine-Specific Metrics and Baseline Neurological Deficits (Tables 1 –3)
Both ICBG and PEEK cohorts had similar preoperative cervical spine injury metrics in terms of evidence of cord injury on magnetic resonance imaging (36% vs 36%, P = 1.00) and discoligamentous injury (78% vs 70%, P = .48). The ICBG cohort had higher percentage of facet subluxation and dislocation (56%) compared with the PEEK cohort (36%) but this was not statistically significant (P = .07). About 58% of the ICBG cohort and 44% of the PEEK cohort had unilateral or bilateral facet fractures (P = .32). The translational injury proportions between the 2 groups (ICBR vs PEEK) were statistically similar (31% vs 19%, P = .11). The most common injured disc levels were C6/7 (39%) and C5/6 (30%).
Pre- and Postoperative Neurological Status With Correlation to Anterior Interbody Graft Choice Metrics.
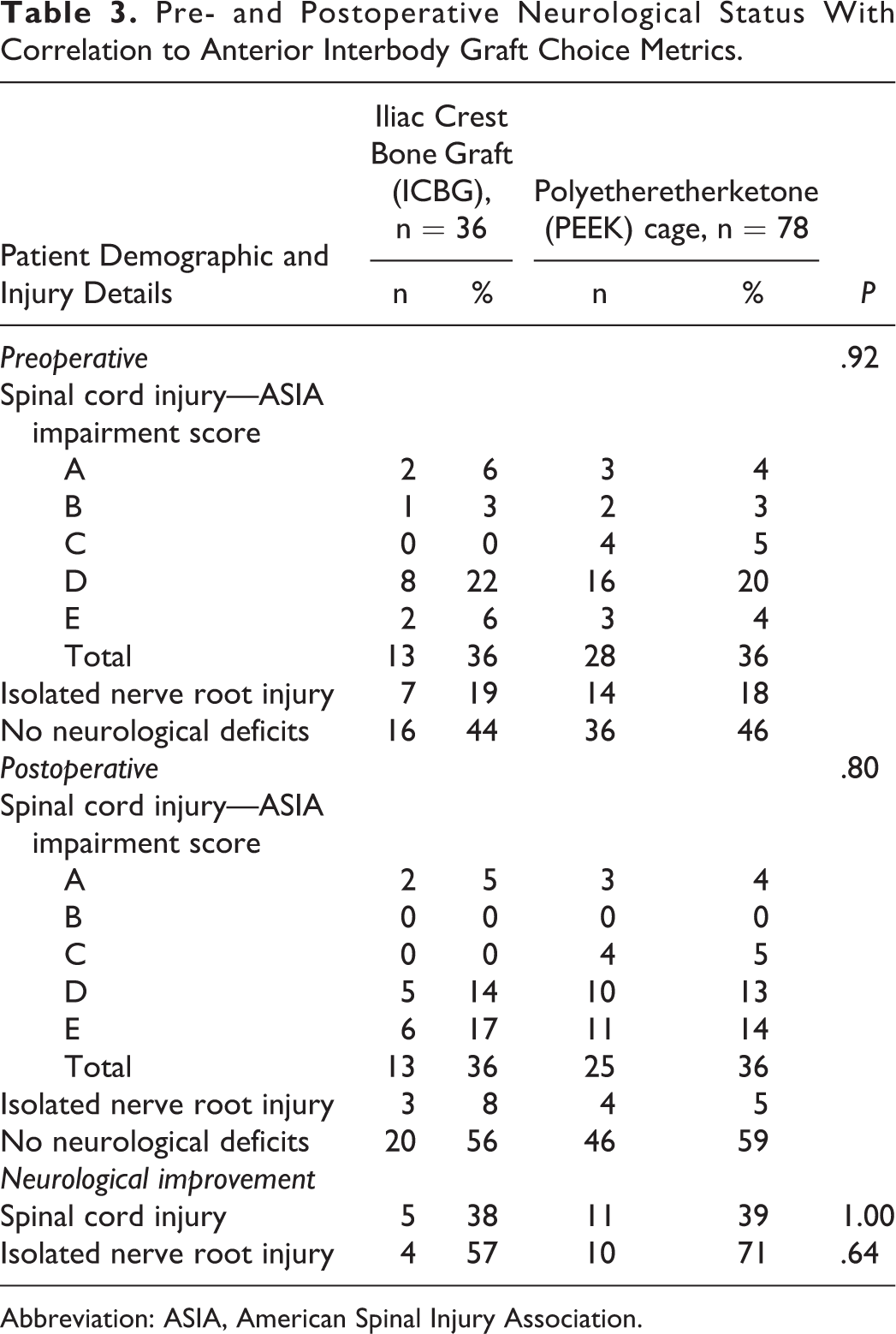
Abbreviation: ASIA, American Spinal Injury Association.
Preoperatively, 54% of the patients (n = 20, 56% in the ICBG cohort; n = 42, 54% in the PEEK cohort) had neurological impairment from spinal cord injury or isolated nerve root injury. The baseline severity of neurological deficits and proportion of spinal cord injury were similar in both the ICBG and PEEK cohorts. In the ICBG cohort, 13 patients (36%) had spinal cord injury, 7 patients (19%) had isolated nerve root injury, and the remainder (n = 16, 44%) were neurologically intact. This is similar to the PEEK cage cohort where 28 patients (36%) had spinal cord injury, 14 patients (18%) had isolated nerve root injury, and 36 (46%) were neurologically intact. The majority of patients who suffered spinal cord injury had impairment consistent with AIS grade D classification (n = 8, 62% in ICBG cohort; n = 16, 57% in PEEK cage cohort). Two patients in the ICBG cohort (15%) and 3 patients in the PEEK cage cohort (11%) had complete recovery of their neurological deficit from spinal cord injury prior to surgery. The proportion of the remaining patients with spinal cord injury were: AIS A (ICBG = 15%; PEEK = 11%); AIS B (ICBG = 8%; PEEK = 7%), and AIS C (ICBG = 0%; PEEK = 14%). Overall, there is no statistical difference with regard to the proportion of preoperative neurological status between the 2 groups (P = .92).
Postoperative Surgical Outcomes Metrics (Tables 3 and 4)
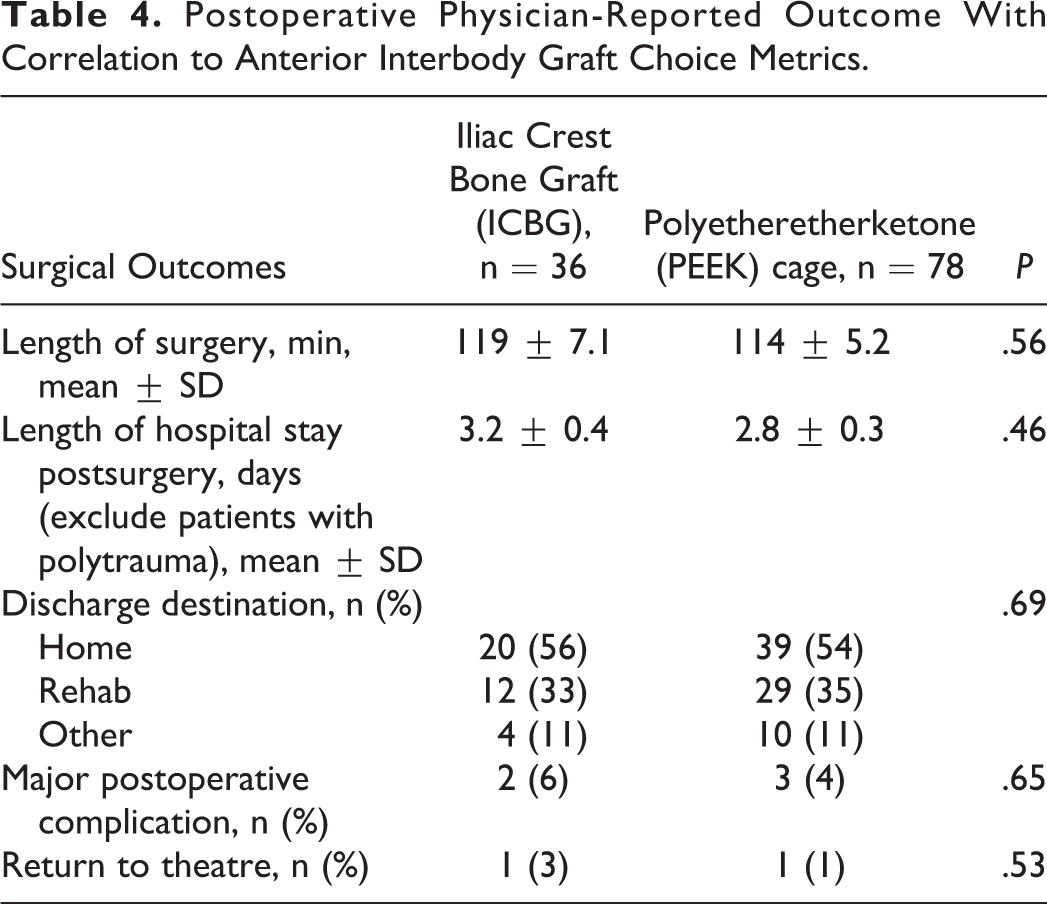
Both the ICBG and PEEK cohorts had similar length of surgery (ICBG cohort mean = 119 minutes; PEEK cohort mean = 114 minutes; P = .56) and length of postoperative hospital stays (ICBG cohort mean = 3.2 days; PEEK cohort mean = 2.8 days; P = .46). Both cohorts also had similar discharge destination (P = .69) with more than half of the patients were discharged home (ICBG = 56% vs PEEK = 54%). The remaining patients were discharged to rehabilitation hospital (ICBG = 33% vs PEEK = 35%) or other destination (ICBG = 11%, PEEK = 11%). Three patients from the ICBG group and 4 patients from the PEEK cage group had major postoperative complications being: (a) recurrent laryngeal nerve palsy (n = 3), (b) anterior cervical plate migration (n = 1), and (c) periprosthetic fracture after fall (n = 1). One patient from each cohort required revision surgery.
Postoperative Physician-Reported Outcome With Correlation to Anterior Interbody Graft Choice Metrics.
Approximately half of the patients (ICBG cohort = 53%; PEEK cage cohort = 56%) had x-ray or CT scans 6 months postsurgery to assess for radiographic evidence of interbody fusion. These scans were assessed independently by 2 investigators (HL and CK). Any disagreement was resolved by consensus with the senior investigator (JT). The ICBG cohort had a higher fusion rate compared to the PEEK cohort, but this did not show statistical significance (ICBG cohort = 14/19, 74% vs PEEK cohort = 21/44, 48%; P = .10). Stability post anterior interbody fusion was also assessed using flexion-extension cervical spine x-rays in about 25% of the patients (n = 5, 16% of ICBG cohort and n = 20, 30% of PEEK cage). Regardless of interbody graft types, all patients who had postoperative flexion-extension radiographs have stable spine alignment (no motion between vertebral bodies and spinous processes on flexion-extension x-ray).
In our study, 39% of the patients with neurological deficits improved in terms of their AIS grading postoperatively. Two of the patients who preoperatively had AIS B impairment had improved to AIS D, 1 patient had improved from AIS C to AIS D and 12 patients improved from AIS D to AIS E. The proportion of AIS improvement was similar between both cohorts (ICBG = 38% vs PEEK = 42%, P = 1.00). All patients with preoperative AIS A impairment have remained neurologically unchanged postoperatively.
Postoperative Patient-Reported Outcome Metrics (Table 5)
A total of 58% of the patients (ICBG cohort = 59%; PEEK cage cohort = 58%) responded to the patient-reported outcome questionnaires. Four patients declined participation in the study. The remaining patients (n = 38) were lost to follow-up. There were 4 study-unrelated deaths in this study, 2 in each cohort.
Postoperative Patient-Reported Outcomes With Correlation to Anterior Interbody Graft Choice Metrics.
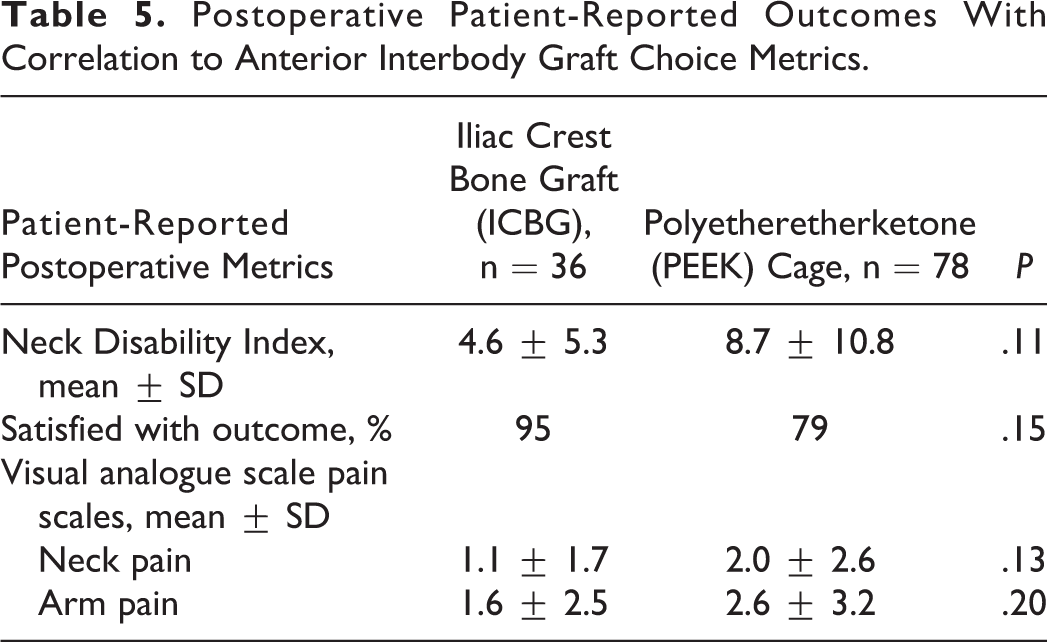
There is no statistical difference in overall satisfaction with outcome of surgery between ICBG (95%) and PEEK (79%) cohorts, P = .15. Both cohorts had similar neck pain 10-point VAS (ICBG cohort mean = 1.1 ± 1.7; PEEK cage cohort mean = 2.0 ± 2.6; P = .13), arm pain 10-point VAS (ICBG cohort mean = 1.6 ± 2.5; PEEK cage cohort mean = 2.6 ± 3.2; P = .20) and NDI scores (ICBG cohort mean = 4.6 ± 5.3; PEEK cage cohort mean = 8.7 ± 10.8; P = .11).
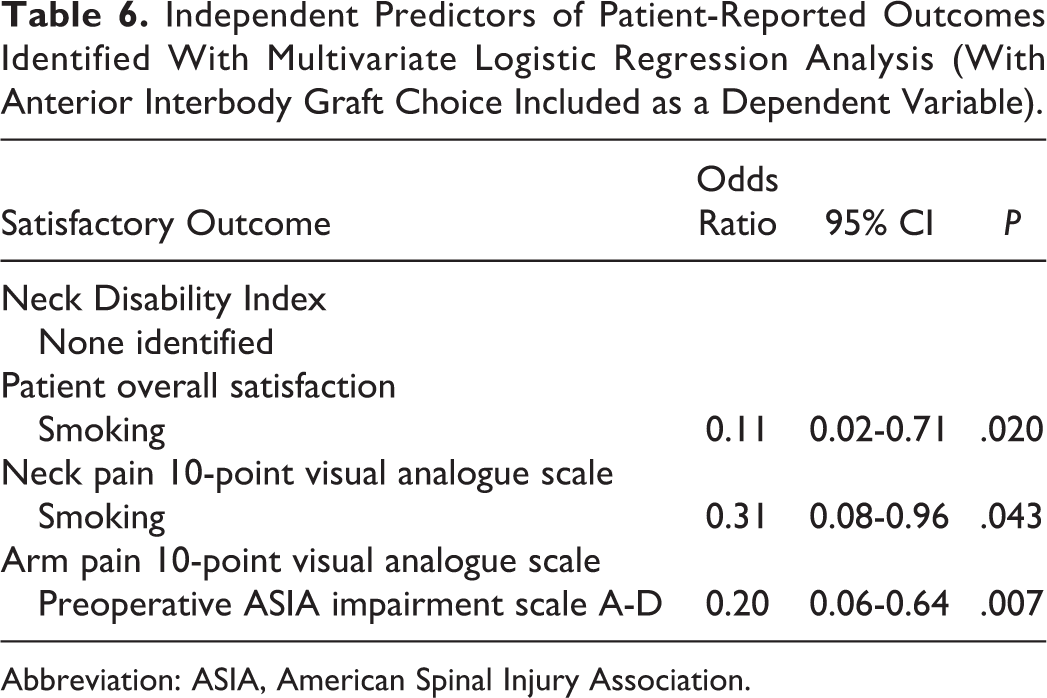
Multivariate Logistic Regression Analysis of Predictors of Satisfactory Outcome (Table 6)
Investigated baseline covariates for multivariate modeling were interbody graft choice (ICBG or PEEK), patient age, gender, smoking status, preoperative neurological deficits from spinal cord injury (AIS A-D), single or 2-level surgery and severity of cervical injury morphology.
Independent Predictors of Patient-Reported Outcomes Identified With Multivariate Logistic Regression Analysis (With Anterior Interbody Graft Choice Included as a Dependent Variable).
Abbreviation: ASIA, American Spinal Injury Association.
Binary logistic regression analyses (Table 6) performed with dependent variables being the NDI, overall patient satisfaction, neck pain 10-point VAS, and arm pain 10-point VAS, did not show any correlation of anterior interbody graft type choice with postoperative patient-reported outcomes at 1 year. The NDI also did not show any correlation to the other tested variables. On the other hand, an active smoking status predicted dissatisfaction with overall satisfaction and neck pain 10-point VAS. As expected, preoperative spinal cord injury negatively predicted for the arm pain 10-point VAS. The Hosmer-Lemeshow test and omnibus test of model coefficients confirmed satisfactory goodness of fit.
Discussion
The utility of PEEK cage with autograft or synthetic bone graft has been well described to have outcome comparable to ICBG in degenerative cervical spine surgery for myelopathy or radiculopathy. 5,16,27 -31 However, there is a paucity of literature on the use of synthetic interbody cage and synthetic graft for cervical spine trauma. This study is unique as it represents the largest ever published series examining the usage of synthetic cage and graft substitute compared with ICBG for stabilization and fusion of cervical spine trauma patients.
This study showed no significant difference in the primary outcomes of patients with anterior stabilization and fusion following cervical spine trauma using synthetic cage/graft construct or autograft. Apart from the NDI, neck pain 10-point VAS, and arm pain 10-point VAS, this study also investigated patient satisfaction. Patient satisfaction represents perhaps the key parameter in the evaluation of any service or intervention-based profession. 32,33
Previous studies, although with smaller number of patients and/or involving some differences in surgical technique, have reported similar findings. Kandziora et al 14 compared the outcomes of a titanium cage filled with autologous cancellous bone (27 patients) and ICBG (26 patients) in monosegment anterior cervical spine fusion for traumatic causes and found no difference in radiological and clinical outcomes. The examined variables included pain, NDI, cervical spine functional score, neurological impairment and patients’ perception of overall surgical outcome based on Odom’s criteria. However, the cage group had significantly less blood loss, shorter operative time, and hospital stay when compared with the autologous graft group. The study also reported 14 patients with complications related to iliac crest harvest. Delépine et al 34 described a series of 30 patients with cervical spine injury without neurological deficits who underwent anterior cervical fusion surgery with PEEK or carbon fiber–reinforced polymer cages. The study found that fusion was achieved in all patients at a mean of 78 days. 34 In a study of 58 patients with cervical spine trauma, Song et al 35 reported a 93.1% fusion rate at 3 months. Hattou et al 36 showed in a study of 29 patients using PEEK cages (filled with hypoxyapatite), a fusion rate of 86.2% at 1 year. All the described studies had used an anterior cervical locking plate, as did our center.
In our center, the rate of spine fusion at 6 months with PEEK cages were lower (48%) when compared with ICBG (74%). This finding, however, did not achieve statistical significance. The commonly regarded inferior rate of fusion of synthetic constructs for anterior spine trauma surgery is the main reason why ICBG is used instead of synthetic constructs. Nevertheless, we acknowledge the variation in fusion grading classifications and the heterogeneity of fusion times in different studies. 25 Regardless of the types of interbody graft, all of the patients who had postoperative flexion-extension x-ray displayed stable spine alignment. The primary outcome results of this study, however, imply noninferiority with regard to patient-reported outcomes when synthetic constructs are used in place of ICBG.
Our study did not show any significant difference in surgical time despite an extra procedure being carried out during ICBG procedures. This is likely because the crest graft harvest was usually performed simultaneously by a co-surgeon to ensure time efficiency. On the other hand, the extra procedure would have a time impact on centers where the entire operation is performed solely by 1 surgeon with a surgical assistant. Our study also contrasted with other published studies with regard to the length of in patient stay, which in our center was no different.
Few studies have investigated the cost-effectiveness of anterior cervical interbody graft using synthetic cage in comparison with ICBG in cervical degenerative diseases but were none in trauma setting, and there was no consensus in these results. Bhadra et al 37 have performed a cost analysis to include implants cost, operative time, hospital stay and concluded that the ICBG and plate cohort incurred a higher cost when compared with cage, bone substitute, and plate group. Donor site morbidity (up to 20%) resulted in lengthened hospital stay and longer operative time have contributed to higher total cost. 37 Similarly, Castro et al 38 found no difference in the estimated cost of titanium mesh in multilevel anterior cervical fusion when compared with ICBG, and harvesting ICBG increased morbidity rate by 22%. Other studies have concluded that PEEK cages are less cost-effective when compared with ICBG. 39,40
It is well acknowledged that there is variation in practice for subaxial cervical spine trauma. 41,42 Some studies have shown similar outcome 43 -46 whereas others have reported poor radiographic outcome following standalone anterior approach when compared to combined anterior posterior or posterior approach in the treatment of cervical spine translational or facet injury. 47,48 In our series, 40% of patients with translational injury underwent combined anterior and posterior fixations. The remaining 26 patients were managed with standalone anterior fixation only, and they did not require additional surgery nor experience loss of reduction or implant failure. Furthermore, we identified that translational injury is not associated with poor prognosis in NDI, VAS-neck, VAS-arm, or patient satisfaction in the multivariate analysis.
Study Strength and Limitation
This is the first clinical quality registry study with prospective data collection methodology and ambispective review comparing patient- and physician-reported outcomes following cervical spine trauma stabilization surgery between PEEK cage with synthetic bone graft (β-tricalcium phosphate) constructs and ICBG. This is also the largest series of consecutive patients studied in cervical spine trauma.
The study uses multivariate methodology with backward stepwise regression analysis to minimize bias. The sample size was determined to be adequately powered for the number of predictive variables used in the multivariate models using previously described methods. 26,49 The Hosmer-Lemeshow test and omnibus test of model coefficients confirmed satisfactory goodness of fit.
Unfortunately, with all registry studies, loss of patients to follow-up is an issue. A major limitation of this study is only 58% of the patients responded to patient-reported outcome questionnaires. In such a study, there was also no randomization of patients with regard to choice of fusion construct. Donor site morbidity was also not recorded in our database.
As there is no routine postoperative imaging protocol in our unit, only 55% of patients had radiographs to assess interbody fusion 6 months postsurgery and 25% of the patients had flexion-extension x-rays to assess stability. The majority of patients had erect x-rays to identify evidence of hardware failure and evidence of fusion. Following anterior cervical interbody fusion, it usually takes three months to one year for fusion to take place. 13,14,16,35,36 Therefore, it may be too early to assess interbody fusion in our study using 6 months postoperative radiograph. Interobserver variation in evaluating fusion in x-rays is also a well-recognized limitation. 50 Unfortunately, only a small proportion of patients had postoperative CT scans. Assessment and management of our postoperative patients are usually based on clinical assessment and patient satisfaction. Nonetheless, this study adds significantly to the current cervical spine trauma literature showing the non-inferiority in patient-reported outcome of synthetic constructs to ICBG in anterior approach cervical spine stabilization and fusion.
Conclusion
This study showed no significant difference in patient satisfaction and cervical spine functional outcome when comparing the usage of PEEK cage (with synthetic bone replacement as graft) and ICBG in anterior alone cervical spine stabilization. Level 1 evidence studies are required to further investigate this finding.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.