
Abstract
Study Design
Systematic Review and Meta-Analysis.
Objective
Identify the incidence, mechanism of injury, investigations, management, and outcomes of Vertebral Artery Injury (VAI) after cervical spine trauma.
Methods
A systematic review and meta-analysis were conducted in accordance with the PRISMA guidelines (PROSPERO-ID CRD42021295265). Three databases were searched (PubMed, SCOPUS, Google Scholar, CINAHL PLUS). Incidence of VAI, investigations to diagnose (Computed Tomography Angiography, Digital Subtraction Angiography, Magnetic Resonance Angiography), stroke incidence, and management paradigms (conservative, antiplatelets, anticoagulants, surgical, endovascular treatment) were delineated. Incidence was calculated using pooled proportions random effects meta-analysis.
Results
A total of 44 studies were included (1777 patients). 20-studies (n = 503) included data on trauma type; 75.5% (n = 380) suffered blunt trauma and 24.5% (n = 123) penetrating. The overall incidence of VAI was .95% (95% CI 0.65-1.29). From the 16 studies which reported data on outcomes, 8.87% (95% CI 5.34- 12.99) of patients with VAI had a posterior stroke. Of the 33 studies with investigation data, 91.7% (2929/3629) underwent diagnostic CTA; 7.5% (242/3629) underwent MRA and 3.0% (98/3629) underwent DSA. Management data from 20 papers (n = 475) showed 17.9% (n = 85) undergoing conservative therapy, anticoagulation in 14.1% (n = 67), antiplatelets in 16.4% (n = 78), combined therapy in 25.5% (n = 121) and the rest (n = 124) managed using surgical and endovascular treatments.
Conclusion
VAI in cervical spine trauma has an approximate posterior circulation stroke risk of 9%. Optimal management paradigms for the prevention and management of VAI are yet to be standardized and require further research.
Introduction
Traumatic vertebral artery injury (TVAI), whether induced by blunt or penetrating trauma, refers to damage to the vertebral arteries resulting from such trauma. 1 Such injuries can be either spontaneous or traumatic, the former being linked to intrinsic vessel wall weakness associated with vascular or connective tissue conditions, leading to vessel dissection. 1 Traumatic injuries often arise from blunt trauma to the head and neck, though penetrating trauma can also be a cause. These injuries often result in strokes or transient ischemic attacks due to compromised blood flow through the posterior circulation, which the vertebral arteries supply. Consequently, patients may exhibit stroke-related symptoms like impaired speech, swallowing and balance, along with ataxia and visual disturbances. 2
TVAIs can result from various injuries to the cervical spine's bones and ligaments, including fractures, excessive bending, subluxations/dislocations, extensions, and rotational traumas. Notably, fractures involving the transverse foramen have been associated with VAI rates as high as 88%. 3 Unstable vertebral body fractures, such as tear-drop fractures, and fractures with anterolisthesis of 3 mm or more, are particularly prone to causing VAI. It's important to note that the absence of visible fractures on imaging does not explicitly rule out the possibility of VAI. 4
Identification of patients at high risk for cerebrovascular damage involves using the modified Denver screening criteria. Computed Tomography Angiography (CTA) is the preferred initial diagnostic imaging technique. 5 Based on injury severity, location, and symptoms, treatment modalities such as fibrinolysis, anticoagulation, anti-platelet therapy, endo-vascular intervention, or open surgical repair can be employed. 6
However, despite the importance of TVAI, its incidence following cervical spine trauma is unknown, with reported incidence ranging from .5% to 39%.7,8 The preferred imaging protocols for diagnosing or screening for VAI after cervical spine trauma remain uncertain, with different institutions utilising CTA, Digital Subtraction Angiography (DSA), and Magnetic Resonance Angiography (MRA) alone or in combination. Similarly, the optimal management strategy for VAI remains unclear, with strategies encompassing anti-platelet and anticoagulant therapies, and primarily conservative approaches. 6
This systematic review and meta-analysis endeavours to tackle the following research inquiry: Among individuals with cervical spine trauma, what is the prevalence of VAI? Additionally, it examines the imaging protocols utilised for diagnosis and the array of management strategies employed to mitigate the risk of stroke.
Methods
Search Strategy and Selection Criteria
A systematic review and meta-analyses were conducted in accordance with the preferred reporting items for the systematic review and meta-analyses (PRISMA) statement. 58 The study was registered with PROSPERO (CRD42021295265). No changes were made to the published protocol.
We searched Scopus, PubMed, Google Scholar and CINAHL Plus for all articles including cervical spine trauma and VAI, from inception until 31/12/2021. The last search date was 31/12/2021. The search strategy used for PubMed can be found in Table 2 in the appendix section. Bibliographies and reference lists of included articles were scanned to identify additional studies in the review. Papers were limited to the English Language due to the feasibility of translation. The Population, Intervention, Comparator, Outcome, and Study Design (PICOS) criteria 10 were used, and the inclusion criteria can be found in Table 1 (appendix). The inclusion criteria included studies of adults (≥16 years) with a population of patients with cervical spine trauma including blunt and penetrating trauma, which contained details on the incidence and mechanism of injury. We also included the investigations of these studies (CTA, MRA and DSA), stroke incidence, and management strategies (conservative, anticoagulant therapy, and antiplatelet therapy). Studies excluded included case reports, case series of <5 cases, editorials, animal-based studies, children <16 years, and studies with an iatrogenic mechanism of VAI.
Study Selection and Screening
Articles identified from the search were transferred to an online platform (Rayyan 2016, 5:210) for screening of titles and abstracts. 9 After the removal of duplicates using Endnote X9 (Endnote Desktop for Mac 2021), titles were screened against the population, intervention, comparison, outcome, and study design criteria (PICOS) by two blinded and independent reviewers. Following this, abstracts were screened, followed by full text using the same process to identify papers suitable for inclusion. Disagreements were resolved between the two reviewers, and if consensus was not reached, senior authors were consulted for clarification.
Data Extraction and Outcomes
Results combined from our search were incorporated into a Microsoft Excel Sheet utilising all available information provided by the authors, including supplementary files. Data extraction was conducted independently by two authors and varying data points were discussed and resolved. The data extraction followed a pre-piloted standardised data collection proforma. Data Extraction included baseline patient demographics (age, Body Mass Index (BMI), gender, co-morbidities), cohort size, admission Glasgow Coma Score (GCS) score, mechanism of injury (blunt, penetrating, iatrogenic), and Denver scoring classification. 11 Investigation methods (CTA, DSA, MRA), first-line treatment strategy employed (conservative, antiplatelet therapy, anticoagulation therapy, surgical), outcomes including stroke, mortality and mean follow-up were also included. The primary outcome measure was the incidence of VAI and overall stroke risk. The secondary outcome measures were the investigations employed and variation in management between different treatment centres.
Risk of Bias Assessment
The risk of bias was assessed using the Newcastle-Ottawa Quality Assessment Form for Cohort Studies (59). The assessment was divided into Selection, Comparability and Outcome and stars were awarded for each of the domains. The mean value out of a total score of 9 was 7.56 for all included papers. Of the 44 studies, 38 studies were classified as good and 6 as fair. None of the studies were deemed to be of poor quality. Figure 1 (supplementary) and Table 1 (supplementary) summarise the results of the risk of bias assessment in the appendix.
Data Analysis
Data was extracted into a Microsoft Excel spreadsheet and then exported to R version 4.0.1 for analysis and figure generation. Data analysis was performed using R Studio (meta and metafor packages). For the meta-analysis, we used a random effect model for pooled proportions estimates for incidence calculations. We generated forest plots for incidence rates based on a random intercept model, including 95% Confidence Intervals (CI). For each random effect model, we tested heterogeneity using the maximum restricted likelihood estimator. Prevalence was calculated using pooled proportions methods using the inverse variance method. Total heterogeneity and I2 characteristics were also calculated. Publication bias was evaluated and presented as funnel plots. A regression analysis was performed using Egger’s test 12 to assess the symmetry of each funnel plot, for comparisons with fewer than 25 studies.
Results
Included Reviews
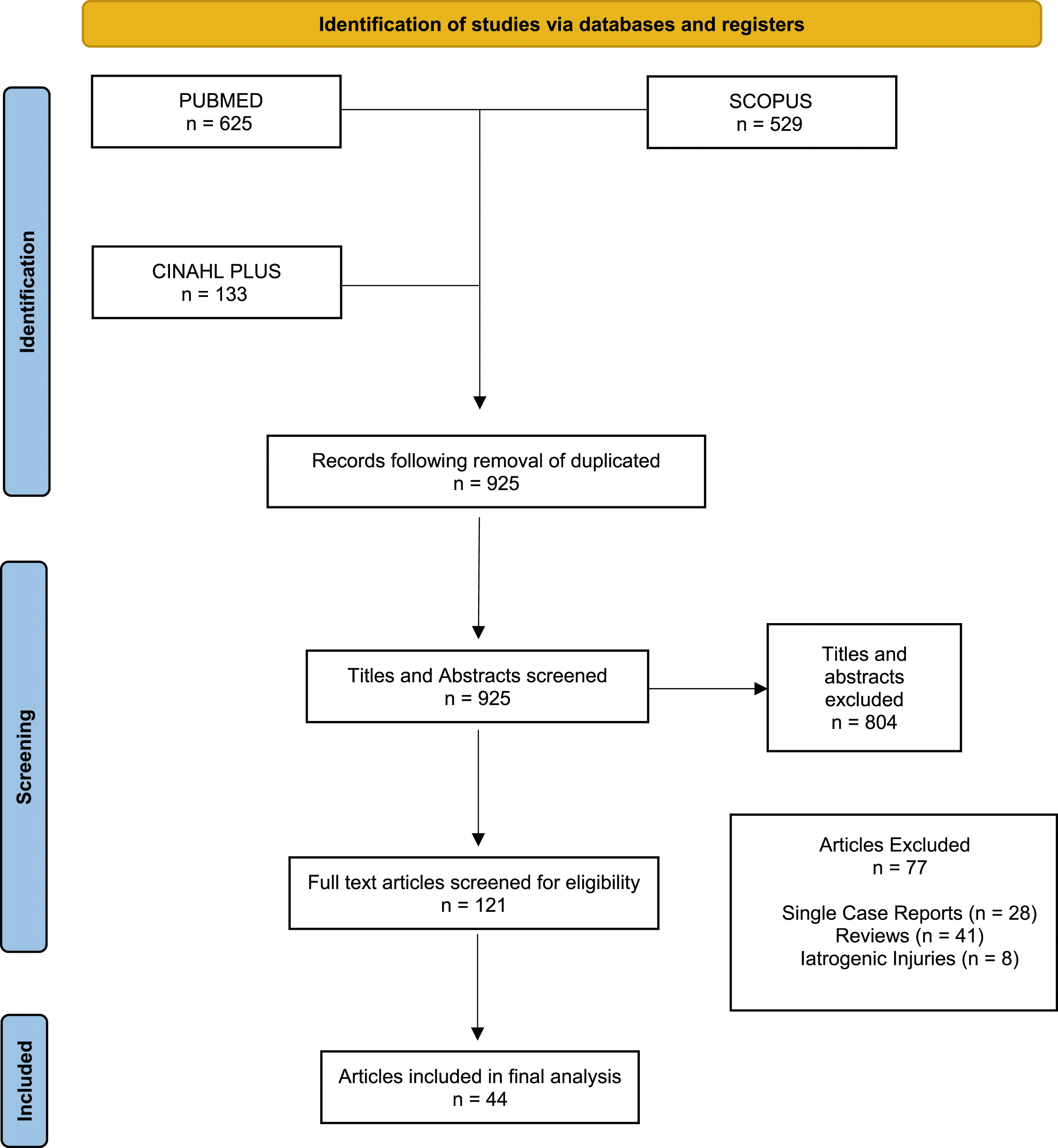
The PRISMA chart of the selection of studies is shown in Figure 1. A total of 1287 records were identified by searching databases PubMed, SCOPUS and CINAHL Plus. Of these, 362 were duplicates and removed. The remaining 925 records underwent screening. Following the screening, a total of 44 papers met the inclusion criteria for this review.
Study and Patient Characteristics
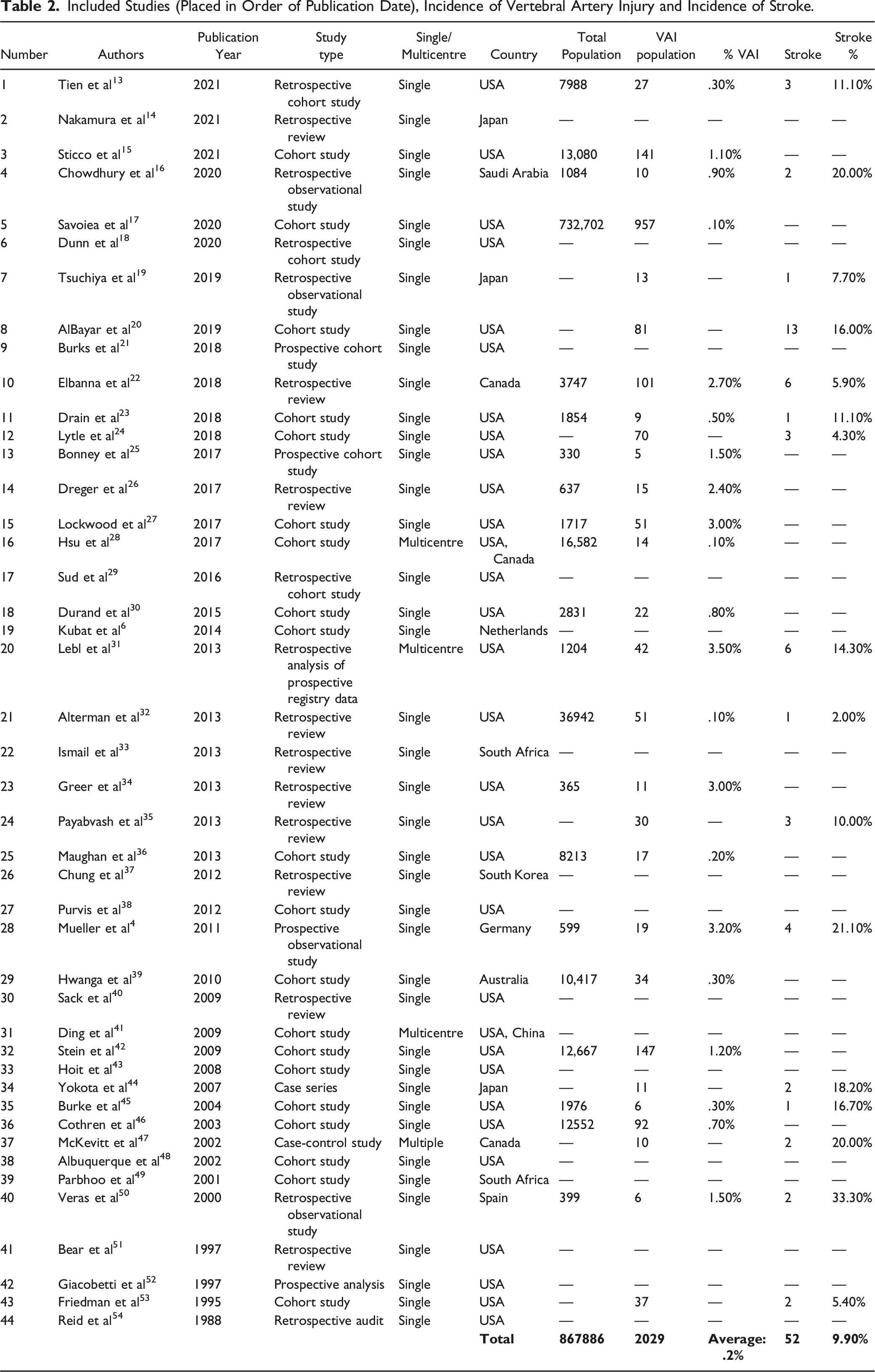
44 papers were selected for this study. All included studies were observational studies with 42 cohort studies, one case-control study and one case series. Forty studies were single-centre and four were multi-centre studies. Table 2 (appendix) summarises the included studies.
Blunt and Penetrating Injuries
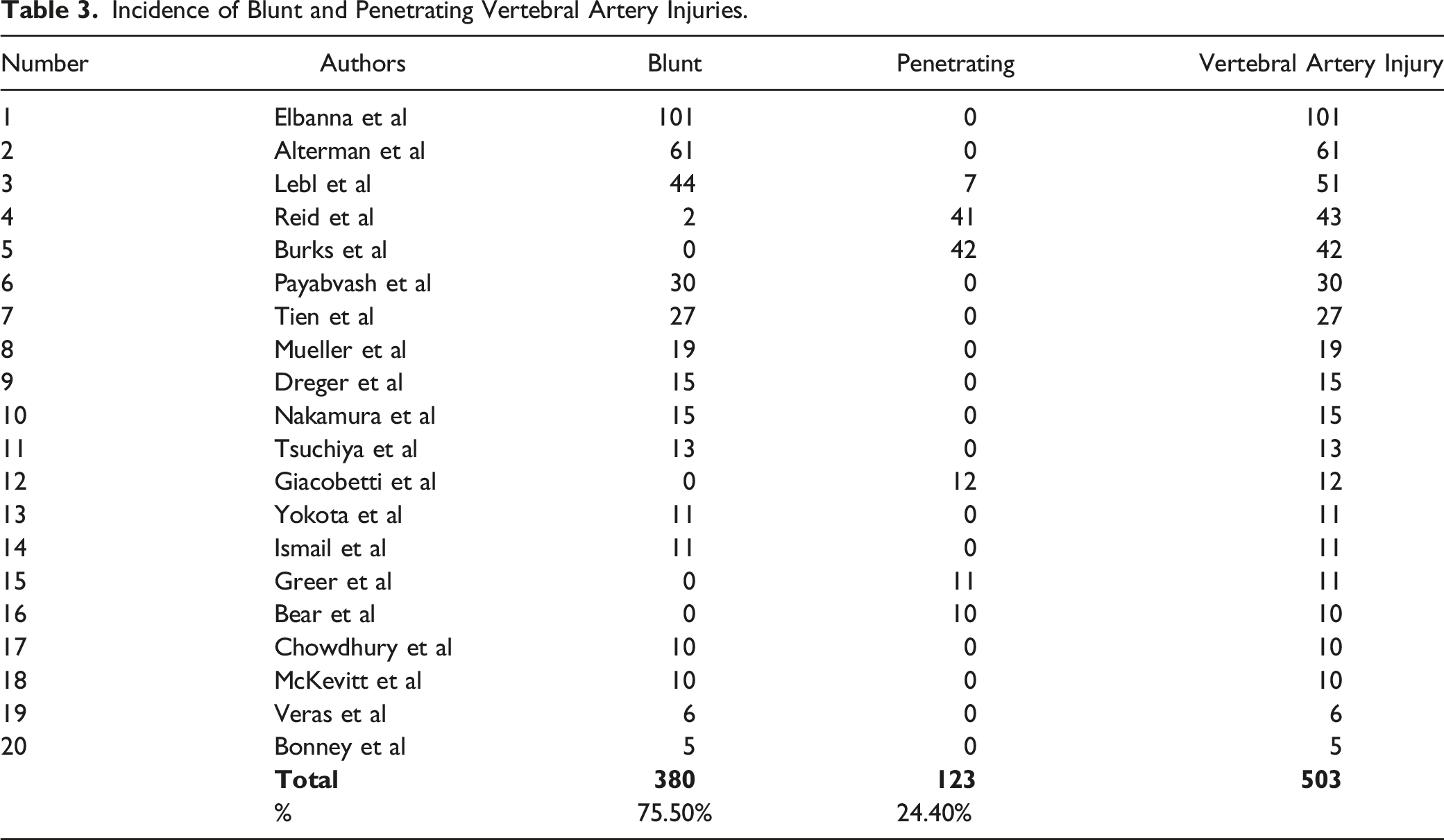
Cervical spine trauma-causing VAIs are divided into blunt and penetrating injuries. Of these, we found that among 20 of the 44 papers with this data, 75.5% (n = 380/503) patients had a blunt injury, and among six papers, 24.5% (n = 123/503) patients had a penetrating injury. The mechanisms of injury include falls, motor vehicle accidents, swimming injuries and cycling falls. The numbers have been summarised below in Table 3 (appendix).
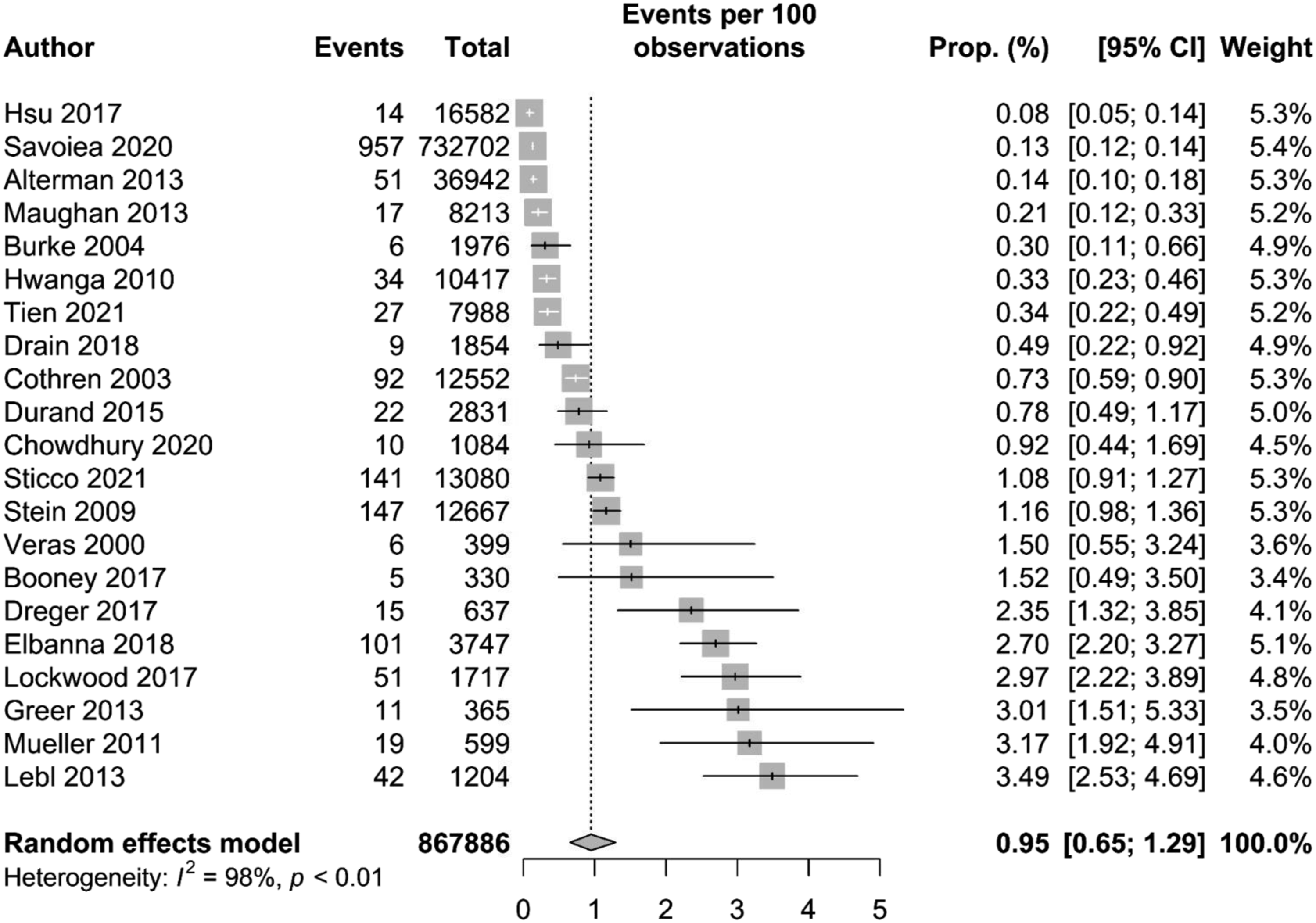
Pooled Incidence
In total, 21 of the 44 studies contained data on VAI incidence and were included in the analysis (867,886 total patients). The overall pooled incidence of VAI was .95% (95% CI 0.65-1.29). The range of incidence was .1%–3.2%. Table 2 (appendix) summarises the population included, and Figure 2 displays the forest plot of the incidence.
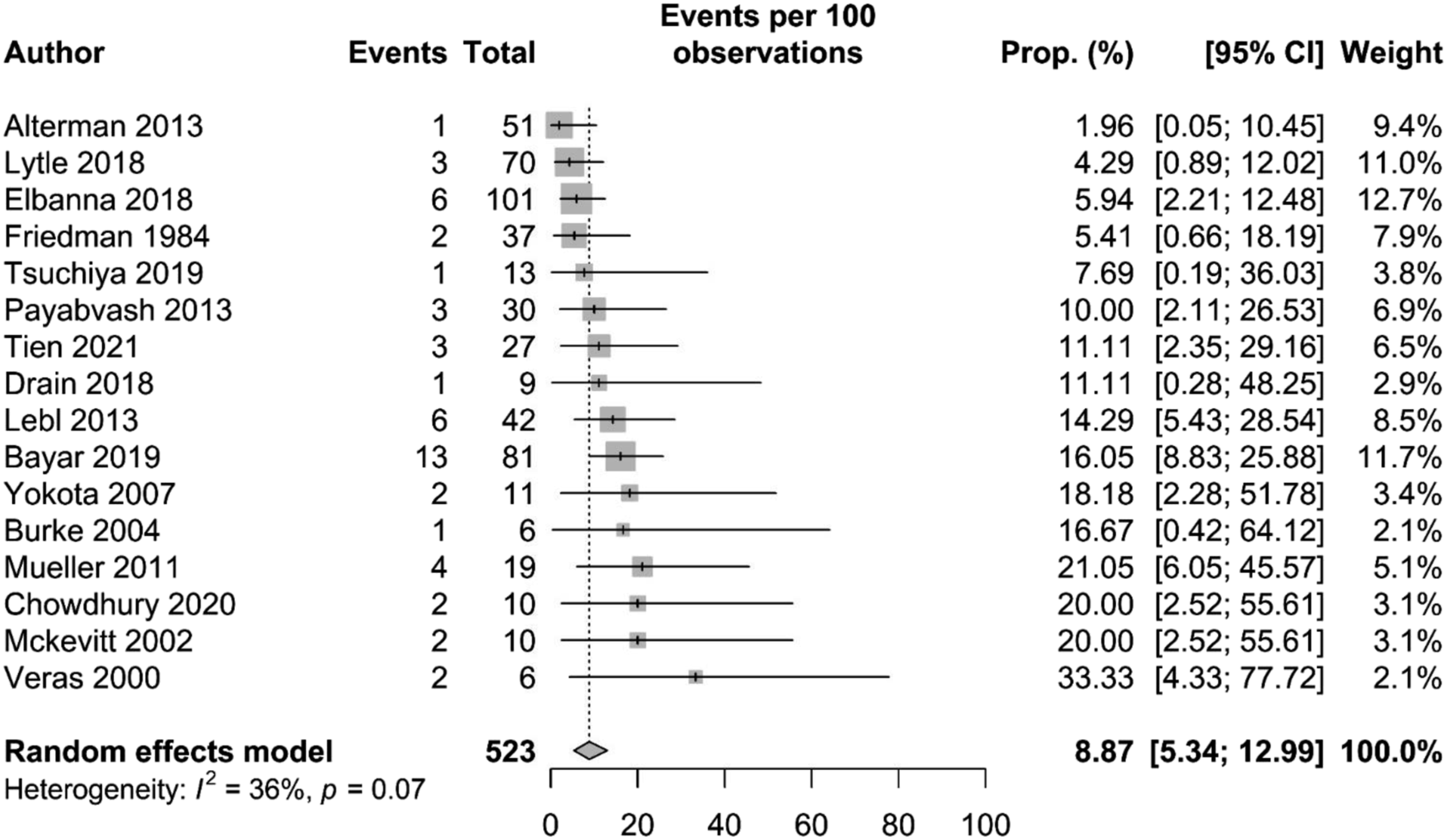
Stroke Analysis in Patients After Presenting With VAI
In total, 16 of the 44 studies contained data on stroke incidence and were included in the analysis (523 patients with VAI). The overall pooled incidence of stroke in VAI patients was 8.8% (95% CI 5.3 – 12.9). The range of incidence was 2.0%–33.3%. Table 2 (appendix) summarises the population including stroke number in patients and Figure 3 displays the forest plot of the incidence.
Investigations
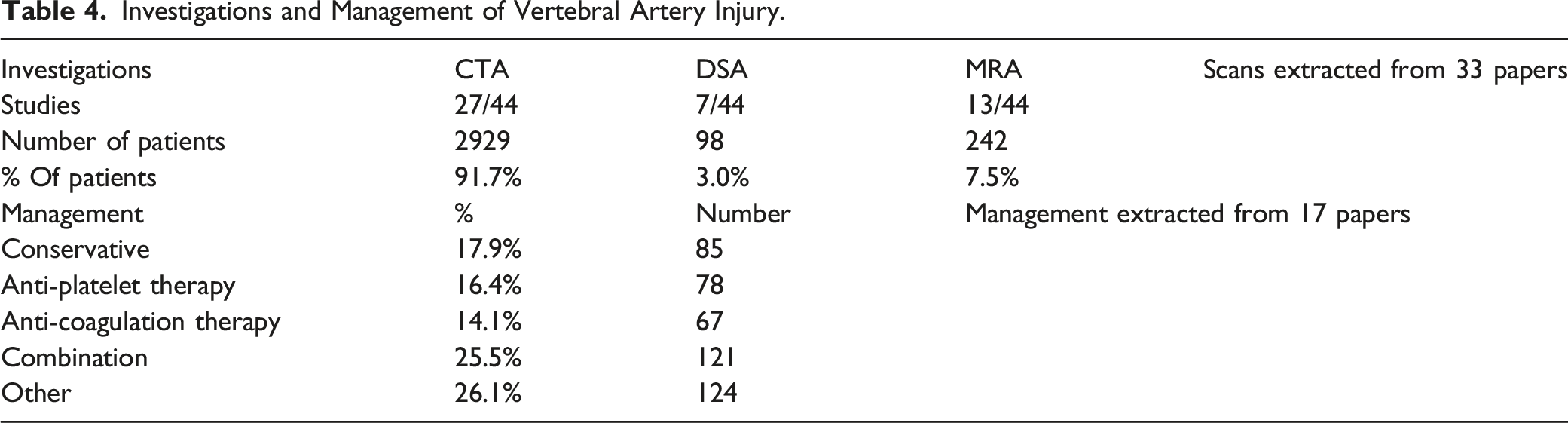
Investigative options for VAI were available from 33 papers included in the review (3215 patients) and are summarised in Table 4. The most used investigation method was CTA (91.7%, 2929 patients). DSA was used among 3.0% (98 patients) and MRA was used for 7.5% (242 patients) of the total cohort.
Management
Management options for VAI were available from 17 papers included in the review (475 patients) and are summarised in Table 4 (appendix). The most utilised management strategy was combined anticoagulation and antiplatelet therapy (25.5%, n = 121/475). 16.4% (n = 78/475) were managed with just antiplatelet, 14.1% (n = 67/475) with anticoagulation, and 17.8% (n = 85/475) managed with conservative/expectant management. Other management options (n = 124/475) included a variety of surgical methods, stents, embolisation and endovascular techniques and the reason for the variation could not be delineated.
Discussion
Key Findings
Our review highlights that the overall incidence of VAI after cervical spine trauma is .95%, with an 8.87% stroke risk.
From 44 studies that were reviewed, 20 divided data on the mechanism (n = 503) of injury into blunt and penetrating. This showed that 75.5% of patients suffered from blunt trauma, with 24.5% having suffered penetrating trauma.
Mechanism of Injury
The vertebral artery may sustain traumatic or spontaneous injuries. Traumatic injuries can result from penetrating trauma as well as blunt trauma to the head and neck. Examples of mechanisms of traumatic VAI are motor vehicle accidents, gunshot wounds, falls from heights, and hyperextension of the neck injuries. 1 The inherent weakening of the artery wall, frequently brought on by underlying vascular or connective tissue disorders, which result in the dissection of the vessel, is what results in spontaneous injuries. 5 A degree of damage can range from an imperfection in the artery wall, to total transection with cerebral or extracranial haemorrhage. Although they might not have any symptoms, patients frequently present with a headache and neck pain. Especially in younger individuals, vertebral artery damage is a significant contributor to stroke and transient ischemic attack. Sanelli et al, found a .53% incidence of VAI in all blunt trauma hospitalizations in a sizable study, with cervical spine injuries occurring in 71% of these injuries. 55
VAI is a potentially serious complication that can arise from fractures in the cervical spine. The most common fractures leading to damage of the vertebral artery are those that extend into the foramen transversarium of the transverse process, fractures spanning the upper cervical spine from C1 to C3, and cases of facet dislocations or subluxations. These injuries can occur either by directly compressing the artery within the foramen or by stretching the vertebral artery between adjacent vertebrae. 55
Temperley et al, found that the most prevalent type of cervical spine fracture associated with VAI is a fracture of the transverse process extending into the foramen transversarium. In their study, 45.2% of patients with VAI had involvement with the FT. Among 192 patients from 8 out of 24 studies that reported facet joint involvement, 40.1% sustained a facet joint injury. Vertebral subluxation was reported in 35% of the 220 patients from 7 out of 24 studies, and vertebral/cranial dislocation was reported in 8.6% of the 151 patients from 7 out of 24 studies. Other less frequently reported fracture types included burst fractures, Hangman fractures, Jefferson fractures, subaxial fractures, lateral mass fractures, lamina fractures, pedicle fractures, arch fractures, and ligamentous injuries.3,46
Studies have shown that a significant percentage (70%) of cases involving VAI after cervical spine trauma exhibit neurological symptoms within the first 24 hours. However, there have been instances where there was a delay of up to 18 hours between the injury and the onset of neurological symptoms in 44% of cases.4,11 This delay could be due to the gradual progression of thrombosis or the worsening of vascular injury to a more severe state, such as a pseudoaneurysm or dissection. The overall documented mortality rate associated with VAI ranges from 4% to 8%. 3 Rapid diagnosis is crucial for timely management and improved patient outcomes.
Comparison of Imaging for TVAI: CTA vs DSA vs MRA
Following our findings from the 33 papers that discussed investigations performed for TVAI, most patients had CTA, MRA being the second most used imaging modality and a small proportion of the patients had DSA for diagnostic purposes.1,2 Historically, DSA has been regarded as the gold standard for vascular damage in the head and neck diagnosis. 1 The reasons for this could include DSA being an invasive procedure and is not as widely accessible as CTA in smaller institutions. Additionally, DSA is only capable of evaluating the vascular lumen and may not be able to identify cases of non-stenotic intramural haemorrhage. 2
Currently, DSA is limited to evaluating high-risk patients with inconclusive or negative results from CTA. In head and neck vascular imaging, CTA has become the preferred primary screening method due to advancements in CT (Computed Tomography) technology. Notably, recent improvements, especially with 64-slice and higher CT scanners, have led to superior detection of blunt cerebrovascular injuries (BCVI) through CTA. 2
When compared to DSA, CTA in one study was demonstrated to have a high sensitivity of almost 98% and a specificity of nearly 100%. 2
When used in conjunction with MRI, MRA performs a complementary function in the simultaneous identification of strokes and vascular damage. It is, however, less sensitive than either CTA or DSA when compared to its capacity to identify vascular damage. According to studies, MRA has modest sensitivity for TVAI detection in the range of 47% to 60%. 2 Hence, CTA is the prime method of investigation at present in the acute setting.
Screening and Managing TVAI
Based on an analysis of 17 research papers that focused on management options for traumatic vertebral artery injuries (TVAI), our study found that most traumatic vertebral artery injuries were treated nonoperatively, with conservative therapy being the most common approach. Surgical and endovascular treatments were also often utilised.
The treatment aims to avoid vertebrobasilar ischemia both directly and indirectly. No additional treatment is necessary for patients with a full vertebral artery thrombosis who are asymptomatic and have an undamaged contralateral vertebral artery. 11 According to Cothren et al, intravenous heparin should be administered to patients who have nonocclusive vertebral artery injuries (intimal disruption, dissection, pseudoaneurysm). In the subacute period, oral warfarin anticoagulation for at least 3 to 6 months is advised as a secondary prophylactic. The regimen may be changed to aspirin, clopidogrel, or aspirin/dipyridamole if a subsequent MRI investigation or ultrasound exam reveals a persistent vascular blockage or a full resolution of vertebral artery dissection.11,56
However, in a recent review, Keser et al, examined two multi-centre international trials: CADISS7,8 and TREAT-CAD6, which inspected the safety and efficacy of anticoagulation and antiplatelet therapies for stroke prevention in cervical artery dissection (CAD). Due to low sample sizes in both trials primarily because the incidence of CAD is generally low, they concluded that there was no clear consensus on an antithrombotic treatment regimen for stroke prevention in cervical artery dissection and certain experts in the field believe that anticoagulation should be followed by antiplatelet therapy after imaging and clinical course. The current guidelines have identified this as a knowledge gap. 57 Moreover, if neurologic impairments such as progressive loss of consciousness or cerebellar symptoms occur, the patients should be monitored with the use of head CT because of deteriorating dissection or embolic injury, and surgical intervention may be necessary. 8
Based on the likelihood of bleeding, the location of the lesion, and the severity of the damage, clinicians can decide whether to treat symptomatic patients with anticoagulant or antiplatelet medication. For patients who have a contraindication to anticoagulant or antiplatelet medication and are at high risk for progression, endovascular therapy and surgical repair are reserved. 5
Surgical and Endovascular Management
Surgical Management
Surgical intervention on the vertebral arteries is technically challenging and tends to be reserved for patients unsuitable for anticoagulation, who have failed with endovascular options or who have uncontrollable haemorrhage. 56 After a VAI, a surgeon must ensure that they can – (i) Attain control over the haemorrhage, (ii) Prevent immediate central nervous system ischemia, (iii) Avert potential postoperative issues like embolism and pseudoaneurysm. 6
The intraoperative approach to managing VAI involves using haemostatic agents, microvascular repair, or artery ligature. Initial bleeding during VAI is addressed with direct haemostatic tamponade using agents like Gelfoam or Surgicel, but this approach involves risks including uncontrolled bleeding, ischemia, and delayed complications. 11 Conventional angiography is recommended after controlling bleeding to assess the situation. While some studies suggest post-tamponade anticoagulation, most VAI cases require further evaluation and treatment. Depending on the vertebral artery’s condition, subsequent management options include endovascular procedures, surgical clipping, repair, connection, or ligation. Primary microvascular repair or connection restores regular blood flow, but suturing a damaged vertebral artery is challenging due to the extensive injury site, requiring sharp margins despite factors like substantial bleeding and surrounding structures. Thus, the use of conventional angiography is strongly recommended once bleeding control via direct tamponade is achieved. 3
Nevertheless, suturing a damaged VA presents technical challenges due to the extensive injury site. The requirement for sharp margins when suturing the damaged VA, coupled with factors such as substantial bleeding, VAI within the bony canal, and surrounding venous plexus, can impede the management process. Hence, microvascular primary repair or connection is suggested if technically feasible, particularly in cases of dominant VAI involving hemodynamically stable patients without interference from neighbouring structures.3,11
Endovascular Management
Modern advancements have greatly improved endovascular approaches for treating vertebral artery injuries (VAI). In cases of iatrogenic VAI, intraoperative or urgent angiography it is recommended that precise injury assessment and bleeding control is performed. Although assembling an endovascular team during hemodynamic instability poses challenges, the growing adoption of endovascular treatments has increased access to skilled interventionists and well-equipped facilities. 48 Coil occlusion of the vertebral artery is suitable when sufficient collateral blood flow is confirmed, offering benefits in bleeding control and recurrence reduction. However, maintaining proper collateral flow is crucial to prevent ischemic strokes. 1 Continued imaging assessments are vital to monitor the vascular conditions after an acute intervention, as delayed complications such as haemorrhagic events or embolic infarctions associated with these vascular abnormalities can emerge days or even years after a VAI. 6 Therefore, ongoing imaging with techniques like CTA, MRA, or angiography is necessary for individuals with VAI, and various endovascular techniques can be utilised to manage pseudoaneurysms or arteriovenous fistulas. 3
Limitations
A major limitation of this study was a lack of geographic data available, and therefore its relevance to VAI could not be studied. Papers not published in English were also excluded from the study. Iatrogenic causes for VAI were not discussed in this paper because only a small portion of the population had an iatrogenic cause for VAI. The timeline of stroke incidence after a VAI could also not be standardised due to significant variations. Additionally, surgical data could not be compiled due to the heterogonous data in studies.
However, this study included 44 papers and provides the first quantification of VAI incidence, and stroke risk in a total patient population of 1777 patients. This can be used to guide screening paradigms, which makes this highly valuable for researchers.
Conclusion
Vertebral artery injuries are common after cervical spine trauma, especially due to blunt injuries, posing a significant risk of posterior circulation stroke. While CTA is a primary diagnostic tool, more research is needed to compare alternative radiographic methods. Prompt medical therapy is imperative for preventing complications in low-grade VAIs following surgical fixation of unstable fractures. The complex treatment of arterial injuries in spine trauma requires a case-by-case approach, suggesting consultation with cerebrovascular specialists and consideration of antiplatelet or anticoagulant treatment, even though standardised management approaches for VAI still require further investigation.
Supplemental Material
Supplemental Material - A systematic review and meta-analysis of vertebral artery injury after cervical spine trauma
Supplemental Material for A systematic review and meta-analysis of vertebral artery injury after cervical spine trauma by Kartik Goyal, Jesvin T. Sunny , Conor S. Gillespie, Martin Wilby, Simon R. Clark, Radek Kaiser, Michael G. Fehlings, and Nisaharan Srikandarajah
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
PICOS Inclusion Criteria. PRISMA Flow diagram, of study selection for inclusion in this review and meta-analysis. Included Studies (Placed in Order of Publication Date), Incidence of Vertebral Artery Injury and Incidence of Stroke. Incidence of Blunt and Penetrating Vertebral Artery Injuries. Forest plot of cumulative incidence of Vertebral Artery Injury. Forest plot of cumulative incidence of stroke after Vertebral Artery Injury. Investigations and Management of Vertebral Artery Injury.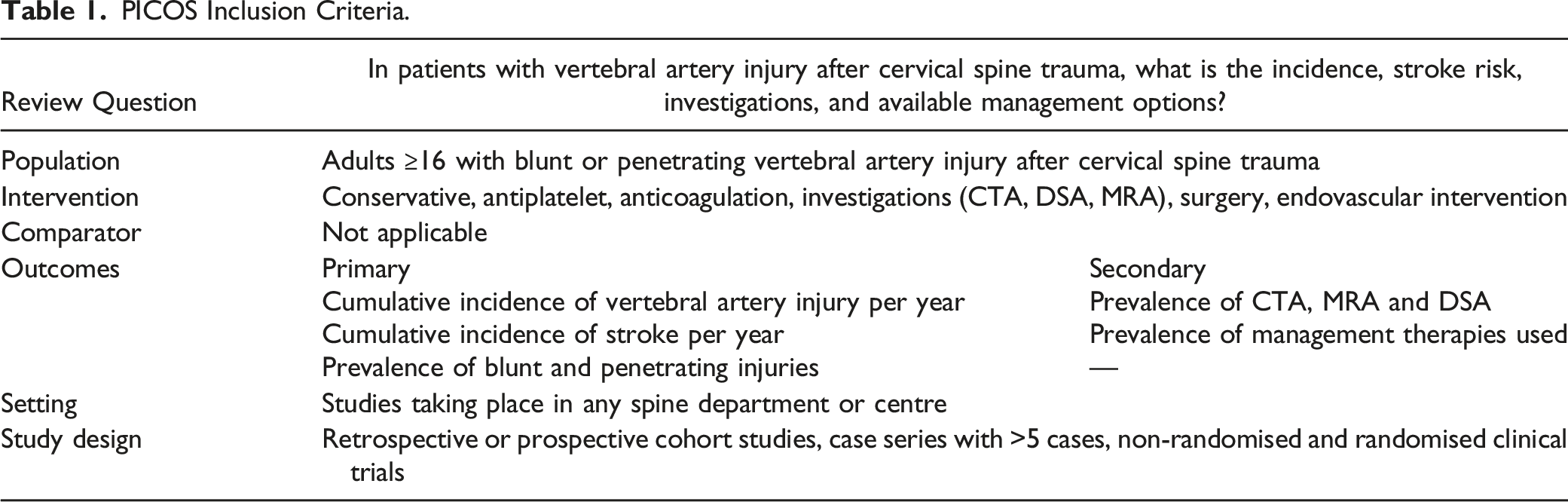
Review Question
In patients with vertebral artery injury after cervical spine trauma, what is the incidence, stroke risk, investigations, and available management options?
Population
Adults ≥16 with blunt or penetrating vertebral artery injury after cervical spine trauma
Intervention
Conservative, antiplatelet, anticoagulation, investigations (CTA, DSA, MRA), surgery, endovascular intervention
Comparator
Not applicable
Outcomes
Primary
Secondary
Cumulative incidence of vertebral artery injury per year
Prevalence of CTA, MRA and DSA
Cumulative incidence of stroke per year
Prevalence of management therapies used
Prevalence of blunt and penetrating injuries
—
Setting
Studies taking place in any spine department or centre
Study design
Retrospective or prospective cohort studies, case series with >5 cases, non-randomised and randomised clinical trials
Number
Authors
Publication Year
Study type
Single/Multicentre
Country
Total Population
VAI population
% VAI
Stroke
Stroke %
1
Tien et al
13
2021
Retrospective cohort study
Single
USA
7988
27
.30%
3
11.10%
2
Nakamura et al
14
2021
Retrospective review
Single
Japan
—
—
—
—
—
3
Sticco et al
15
2021
Cohort study
Single
USA
13,080
141
1.10%
—
—
4
Chowdhury et al
16
2020
Retrospective observational study
Single
Saudi Arabia
1084
10
.90%
2
20.00%
5
Savoiea et al
17
2020
Cohort study
Single
USA
732,702
957
.10%
—
—
6
Dunn et al
18
2020
Retrospective cohort study
Single
USA
—
—
—
—
—
7
Tsuchiya et al
19
2019
Retrospective observational study
Single
Japan
—
13
—
1
7.70%
8
AlBayar et al
20
2019
Cohort study
Single
USA
—
81
—
13
16.00%
9
Burks et al
21
2018
Prospective cohort study
Single
USA
—
—
—
—
—
10
Elbanna et al
22
2018
Retrospective review
Single
Canada
3747
101
2.70%
6
5.90%
11
Drain et al
23
2018
Cohort study
Single
USA
1854
9
.50%
1
11.10%
12
Lytle et al
24
2018
Cohort study
Single
USA
—
70
—
3
4.30%
13
Bonney et al
25
2017
Prospective cohort study
Single
USA
330
5
1.50%
—
—
14
Dreger et al
26
2017
Retrospective review
Single
USA
637
15
2.40%
—
—
15
Lockwood et al
27
2017
Cohort study
Single
USA
1717
51
3.00%
—
—
16
Hsu et al
28
2017
Cohort study
Multicentre
USA, Canada
16,582
14
.10%
—
—
17
Sud et al
29
2016
Retrospective cohort study
Single
USA
—
—
—
—
—
18
Durand et al
30
2015
Cohort study
Single
USA
2831
22
.80%
—
—
19
Kubat et al
6
2014
Cohort study
Single
Netherlands
—
—
—
—
—
20
Lebl et al
31
2013
Retrospective analysis of prospective registry data
Multicentre
USA
1204
42
3.50%
6
14.30%
21
Alterman et al
32
2013
Retrospective review
Single
USA
36942
51
.10%
1
2.00%
22
Ismail et al
33
2013
Retrospective review
Single
South Africa
—
—
—
—
—
23
Greer et al
34
2013
Retrospective review
Single
USA
365
11
3.00%
—
—
24
Payabvash et al
35
2013
Retrospective review
Single
USA
—
30
—
3
10.00%
25
Maughan et al
36
2013
Cohort study
Single
USA
8213
17
.20%
—
—
26
Chung et al
37
2012
Retrospective review
Single
South Korea
—
—
—
—
—
27
Purvis et al
38
2012
Cohort study
Single
USA
—
—
—
—
—
28
Mueller et al
4
2011
Prospective observational study
Single
Germany
599
19
3.20%
4
21.10%
29
Hwanga et al
39
2010
Cohort study
Single
Australia
10,417
34
.30%
—
—
30
Sack et al
40
2009
Retrospective review
Single
USA
—
—
—
—
—
31
Ding et al
41
2009
Cohort study
Multicentre
USA, China
—
—
—
—
—
32
Stein et al
42
2009
Cohort study
Single
USA
12,667
147
1.20%
—
—
33
Hoit et al
43
2008
Cohort study
Single
USA
—
—
—
—
—
34
Yokota et al
44
2007
Case series
Single
Japan
—
11
—
2
18.20%
35
Burke et al
45
2004
Cohort study
Single
USA
1976
6
.30%
1
16.70%
36
Cothren et al
46
2003
Cohort study
Single
USA
12552
92
.70%
—
—
37
McKevitt et al
47
2002
Case-control study
Multiple
Canada
—
10
—
2
20.00%
38
Albuquerque et al
48
2002
Cohort study
Single
USA
—
—
—
—
—
39
Parbhoo et al
49
2001
Cohort study
Single
South Africa
—
—
—
—
—
40
Veras et al
50
2000
Retrospective observational study
Single
Spain
399
6
1.50%
2
33.30%
41
Bear et al
51
1997
Retrospective review
Single
USA
—
—
—
—
—
42
Giacobetti et al
52
1997
Prospective analysis
Single
USA
—
—
—
—
—
43
Friedman et al
53
1995
Cohort study
Single
USA
—
37
—
2
5.40%
44
Reid et al
54
1988
Retrospective audit
Single
USA
—
—
—
—
—
Number
Authors
Blunt
Penetrating
Vertebral Artery Injury
1
Elbanna et al
101
0
101
2
Alterman et al
61
0
61
3
Lebl et al
44
7
51
4
Reid et al
2
41
43
5
Burks et al
0
42
42
6
Payabvash et al
30
0
30
7
Tien et al
27
0
27
8
Mueller et al
19
0
19
9
Dreger et al
15
0
15
10
Nakamura et al
15
0
15
11
Tsuchiya et al
13
0
13
12
Giacobetti et al
0
12
12
13
Yokota et al
11
0
11
14
Ismail et al
11
0
11
15
Greer et al
0
11
11
16
Bear et al
0
10
10
17
Chowdhury et al
10
0
10
18
McKevitt et al
10
0
10
19
Veras et al
6
0
6
20
Bonney et al
5
0
5
%
75.50%
24.40%
Investigations
CTA
DSA
MRA
Scans extracted from 33 papers
Studies
27/44
7/44
13/44
Number of patients
2929
98
242
% Of patients
91.7%
3.0%
7.5%
Management
%
Number
Management extracted from 17 papers
Conservative
17.9%
85
Anti-platelet therapy
16.4%
78
Anti-coagulation therapy
14.1%
67
Combination
25.5%
121
Other
26.1%
124
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.