
Abstract
Study design
Systematic Review
Objectives
Vertebral Artery Injury (VAI) is a potentially serious complication of cervical spine fractures. As many patients can be asymptomatic at the time of injury, the identification and diagnosis of VAI can often prove difficult. Due to the high rates of morbidity and mortality associated with VAI, high clinical suspicion is paramount. The purpose of this review is to elucidate incidence, diagnosis, treatment and outcomes of VAI associated with cervical spine injuries.
Methods
A systematic search of electronic databases was performed using ‘PUBMED’, ‘EMBASE’,‘Medline (OVID)’, and ‘Web of Science, for articles pertaining to traumatic cervical fractures with associated VAI.
Results
24 studies were included in this systematic review. Data was included from 48 744 patients. In regards to the demographics of the focus groups that highlighted information on VAI, the mean average age was 46.6 (32.1-62.6). 75.1% (169/225) were male and 24.9% (56/225) were female. Overall incidence of VAI was 596/11 479 (5.19%). 190/420 (45.2%) of patients with VAI had fractures involving the transverse foramina. The right vertebral artery was the most commonly injured 114/234 (48.7%). V3 was the most common section injured (16/36 (44.4%)). Grade I was the most common (103/218 (47.2%)) injury noted. Collective acute hospital mortality rate was 32/226 (14.2%), ranging from 0-26.2% across studies.
Conclusion
VAI secondary to cervical spine trauma has a notable incidence and high associated mortality rates. The current available literature is limited by a low quality of evidence. In order to optimise diagnostic protocols and treatment strategies, in addition to reducing mortality rates associated with VAI, robust quantitative and qualitative studies are needed.
Introduction
Vertebral Artery Injury (VAI) is a potentially serious complication of cervical spine fractures. The vertebral arteries (VA) provide vital blood supply to the occipital lobe, brainstem and cerebellum. 1 The left VA is dominant in 50% of the population, the right in 25%, and the arteries demonstrate equal calibre in 25% of the population, 2 with respective diameter of approximately 3-5 mm. Each respective VA can be divided into 4 segments (V1-4). V1 (pre-foraminal) commences at the origin to the transverse foramen of cervical vertebra C6. V2 (foraminal) lies through the transverse foramen of C2-C6. V3 (extradural) starts from C2, where the artery loops and turns lateral to ascend into the transverse foramen and continues through C1 to pierce the dura. V4 (intracranial) runs from the dura at the lateral edge of the posterior atlanto-occipital membrane to their confluence on the medulla to form the basilar artery.
The incidence of VAI in patients with blunt cervical spine trauma ranges from .53% to 39% in the literature.3-5 This wide variation in incidence is most likely due to differences in sample size and the diagnostic imaging modality (digital subtraction angiography (DSA), magnetic resonance angiography (MRA) or Computed Tomography Angiograms (CTA)) employed, as well as patient selection bias. Recently, there has been a higher incidence of VAI reported, most likely due to advances in imaging technology. 3 Nevertheless, fractures involving the transverse process, which can extend into the transverse foramina, and fractures with associated subluxation are particularly renowned for increased risk of VAI.6,7
Broadly, VAI can be categorized into traumatic and spontaneous. Traumatic VAI can be further subdivided into blunt and penetrating injuries and can include dissection, intimal tears, stenosis or traumatic aneurysm.
8
VAI can be graded using the Denver scale,
6
illustrated in Figure 1. Although the majority of patients are initially asymptomatic,
7
believed to be due to delayed thrombus formation and development of the vascular injury, VAI can have devastating consequences including permanent neurological deficits and associated mortality. Therefore, high clinical suspicion is important regarding the possibility of VAI in patients presenting with cervical spine trauma. As such, the purpose of this review is to elucidate incidence, diagnosis, treatment and outcomes of VAI associated with cervical spine injuries denoted in academic literature. By doing so, efficacious, multi-disciplinary, timely treatment protocols may be improved and implemented for this vulnerable cohort. Denver Grading Scale for blunt cerebrovascular injuries. Grabowski G, Robertson RN, Barton BM, Cairns MA, Webb SW. Blunt Cerebrovascular Injury in Cervical Spine Fractures: Are More-Liberal Screening Criteria Warranted? Global Spine J. 2016 Nov;6 (7):679-685.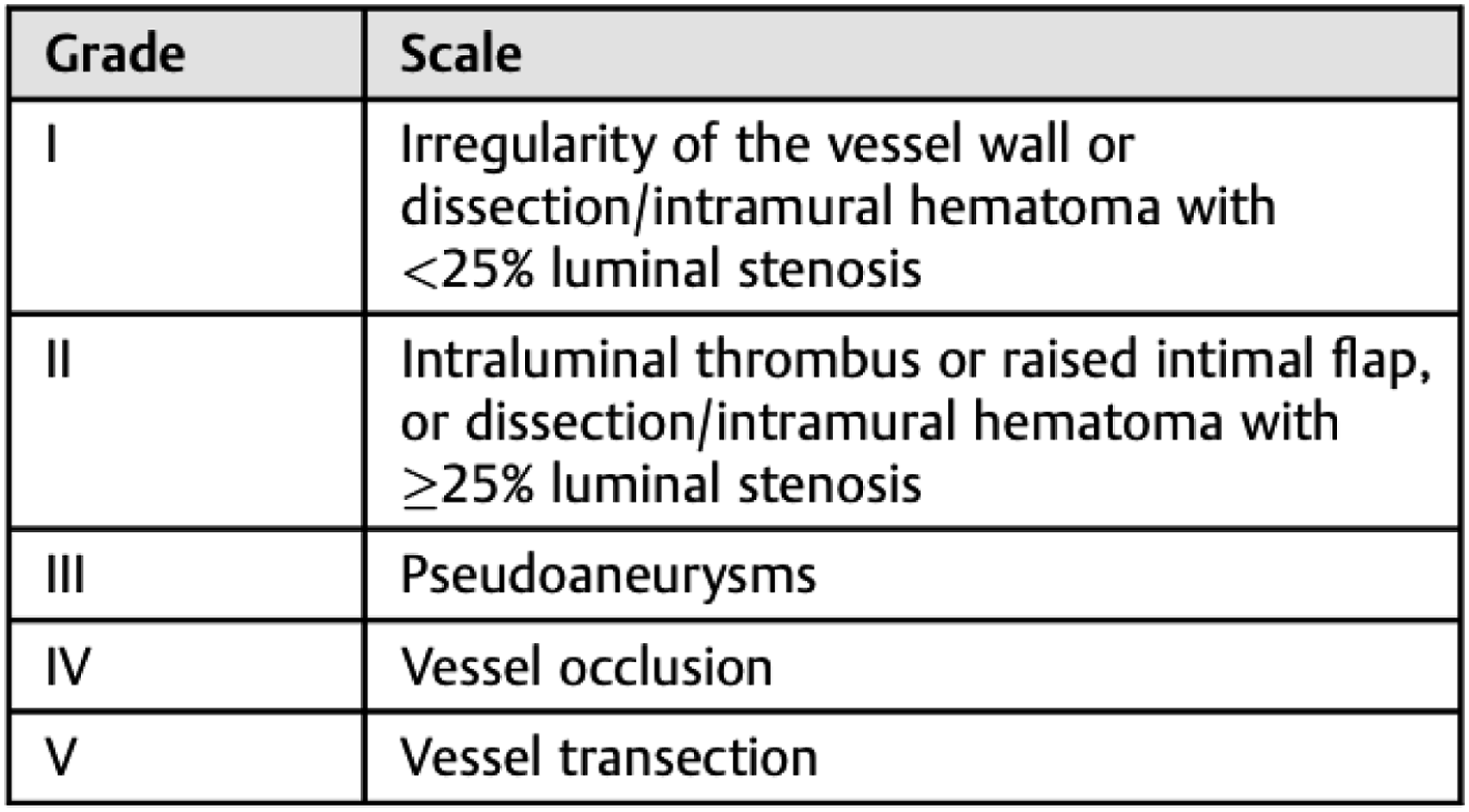
Methods
Search Strategy and Data Extraction
A systematic review was conducted in accordance to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A formal systematic search was performed of the PubMed, Embase, Medline (OVID) and Web of Science databases to identify relevant titles up to and including February 26th 2022, for studies relating to traumatic cervical fractures with associated vertebral artery injury.
The search was performed by 2 independent reviewers (HCT and NOS), using a predetermined search strategy that was designed by the senior authors. Details in relation to the search strategy can be found in Supplementary Appendix 1. Retrieved studies were reviewed to ensure studies met the predefined inclusion and exclusion criteria (see below). Discordances in opinion were resolved through consultation with a third author (JM). Manual cross-referencing of reference lists from studies was undertaken to identify further potential articles for inclusion.
Data extraction was also performed by 2 independent reviewers (HCT and NOS), with study details, basic patient clinicopathological characteristics, management strategies and outcomes recorded. Furthermore, information extracted was based on the PICOTS framework (Population, Intervention, Comparator, Outcomes, Timing and Setting). GraphPad Prism (Version 8.3.0) was utilised for analysis and figures.
Eligibility Criteria
The inclusion criteria were as follows: 1) Published studies demonstrating vertebral artery injury in cervical spinal trauma. 2) Published in the English language. 3) Published after 2000.
The exclusion criteria were as follows: 1) Abstract only. 2) Studies failing to discuss or denote VAI. 3) Paediatric cohorts aged less than 18 years. 4) Case reports
Risk of Bias
Assessment of potential bias was assessed using Newcastle- Ottawa scale (NOS) risk of bias tool and the results tabulated. This assessment tool grades each study as being ‘satisfactory’ or ‘unsatisfactory’ across various categories. We assigned stars to evaluate study quality: 7 stars - “very good”, 5-6 stars “good”, 3-4 stars “satisfactory” and 0-2 stars “unsatisfactory”. The critical appraisal was completed by 2 reviewers independently (HCT and NOS), where once again a third reviewer (JM) was asked to arbitrate in cases of discrepancies in opinion.
Aims and Objectives
The overall aims and objectives of this study were as follows: 1. To elucidate the incidence of associated VAI in cervical spine trauma patients 2. To outline the characteristics of VAI and presentation in cervical spine trauma patients 3. To report on management strategies and outcomes of patients with VAI
Results
Study Selection/Included Studies
The systematic search strategy identified a total of 977 studies, of which 448 duplicate studies were manually removed. The remaining 529 studies were screened for relevance, before 54 full texts were reviewed. In total, 24 studies fulfilled our inclusion criteria and were included in this systematic review4,5,9-30 (Figure 2). Due to heterogeneity in study method and results presented, a collative summary of findings was deemed appropriate. PRISMA flowchart outlining the systematic search process.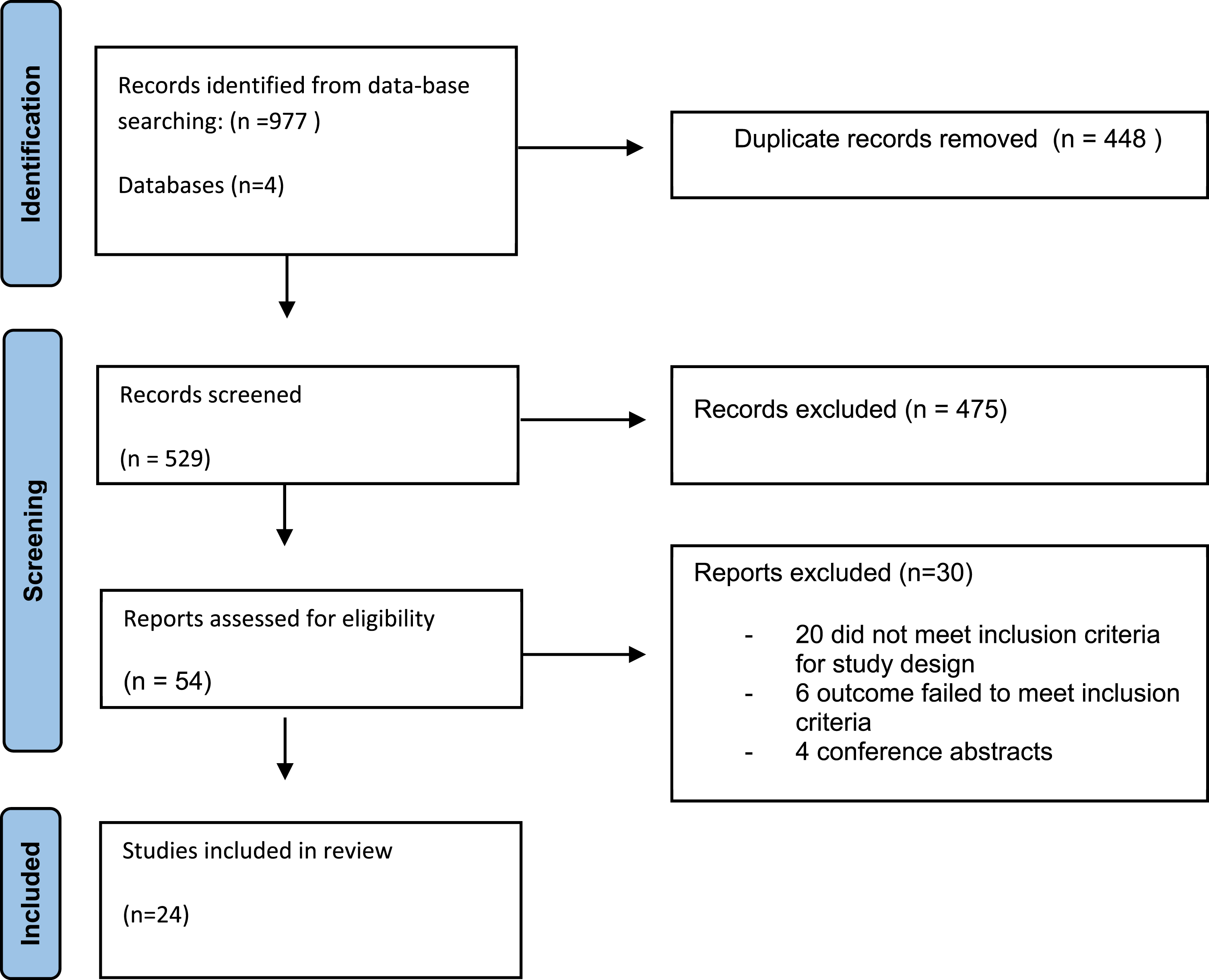
Baseline Characteristics
The data collected was highly heterogenous. The majority of studies had contrasting and inconsistent study population groups. In total, there was data included from 48 744 patients. All 24 studies were population-based studies concerned with cervical fractures, 17/24 of which had sub-cohort analysis for patients with confirmed VAI and 2/24 for cervical spine fracture patients suspicious for VAI
Baseline study characteristics.
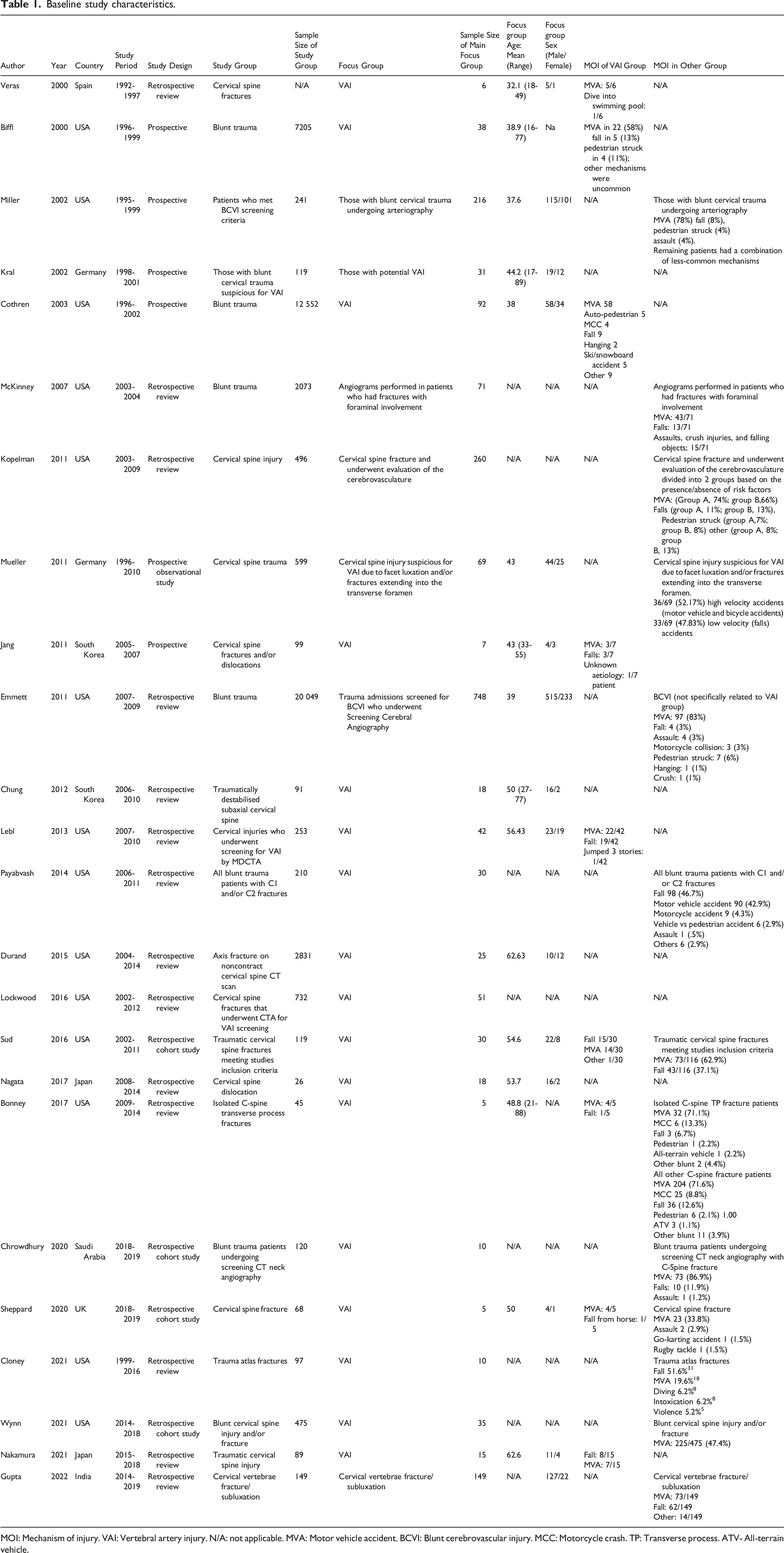
MOI: Mechanism of injury. VAI: Vertebral artery injury. N/A: not applicable. MVA: Motor vehicle accident. BCVI: Blunt cerebrovascular injury. MCC: Motorcycle crash. TP: Transverse process. ATV- All-terrain vehicle.
Risk of Bias
The risk of bias was assessed in included studies. One study was deemed ‘very good’, thirteen studies were rated as ‘good’. Seven studies were noted to be “satisfactory”, and 3 studies were found to be “unsatisfactory”. The risk of bias was assessed using Newcastle-Ottawa Scale (NOS) 32 and is presented in Supplementary Appendix 2.
Vertebral Artery Injury
Incidence of VAI
22/24 studies reported on the incidence of VAI. Study cohorts included: blunt trauma patients screening for blunt cerebrovascular injury (BCVI) with diagnostic angiography (11/24), cervical spine fractures and/or dislocation (7/24), blunt trauma patients (1/24), isolated axis fractures (1/24), isolated atlas fractures (1/24), isolated C-spine transverse process fractures (1/24), patients with cervical spine injury and VAI (1/24), angiograms performed in patients who had fractures with foraminal involvement (1/24). Figure 3 displays the reported VAI incident rates across the studies. Incidence of VAI. VAI: Vertebral artery injury.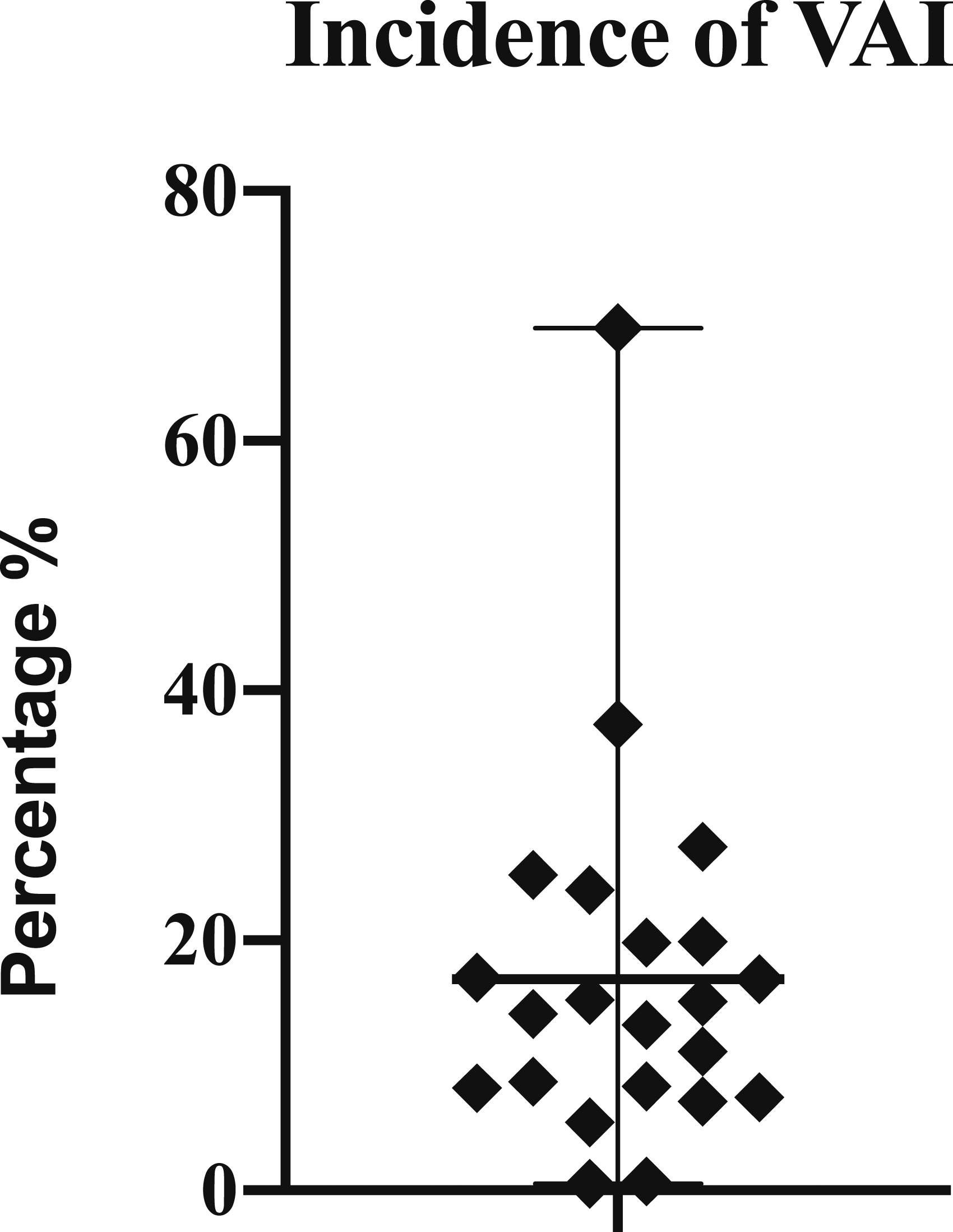
It is challenging to calculate a true incidence of VAI because of the heterogenous study populations. Some studies gave incidence of VAI in all blunt trauma patients compared to others which only reported on VAI in those who had undergone screening for high risk of VAI. Amongst all study populations included in this study, the overall incidence is 596/11 479 (5.19%). To analyse further, the incidence of VAI associated with any patient presenting with cervical spine fractures and/or dislocation was 14/807 (1.7%), trauma atlas (C1) fractures 8/97 (8.2%), isolated axis fractures who had undergone subsequent CTA 25/67 (37.3%) and blunt trauma patients 38/7205 (.53%). 11/24 studies focused on blunt trauma patients screening for BCVI undergoing diagnostic angiography (CTA, DSA, MRA, angiography), with a collective incidence of 410/3490 (11.7%). One study focused on isolated C-spine transverse process fractures, reported an incidence of 5/45 (11.1%).
Mechanism of Injury (MOI)
Of the 17/24 studies which outlined VAI as their main focus group/cohort of interest, 9/17 described the MOI. Motor vehicle accidents (MVA) was the most common injury in 7/9 studies, with falls being the most common in 2/9. In total, of the VAI studies which analysed MOI 139/240 (57.9%) were MVA and 61/240 (25.4%) falls. Other injuries were uncommon but consisted of; pedestrians hit by vehicles, jumping from buildings, snow-sport accidents, horse riding accidents, hangings, diving into swimming pools and others. The remaining 7/24 studies denoting incidental cases of VAI did not report on MOI.
Location of VA Affected
Overall, 11/24 studies reported on whether the vertebral artery (VA) affected was right, left or bilateral. In total, 234 VAs were reported on across these studies. The right VA was the most commonly injured 114/234 (48.7%) followed by the left 97/234 (41.5%), with bilateral injury being the least common injury 23/234 (9.8%). Two studies reported on whether the injury was unilateral or bilateral. Both studies report unilateral injury to be more common than bilateral injury (53/71 (74.6%) vs 11/18 (61.1%)). Three studies report the particular section of the VA injured. V3 was the most common section injured (16/36 (44.4%)), followed by V1/2/3 (6/36 (16.7%)) and V1/2 (2/36 (5.6%)), (Figure 4). Location of VAI. VA: vertebral artery.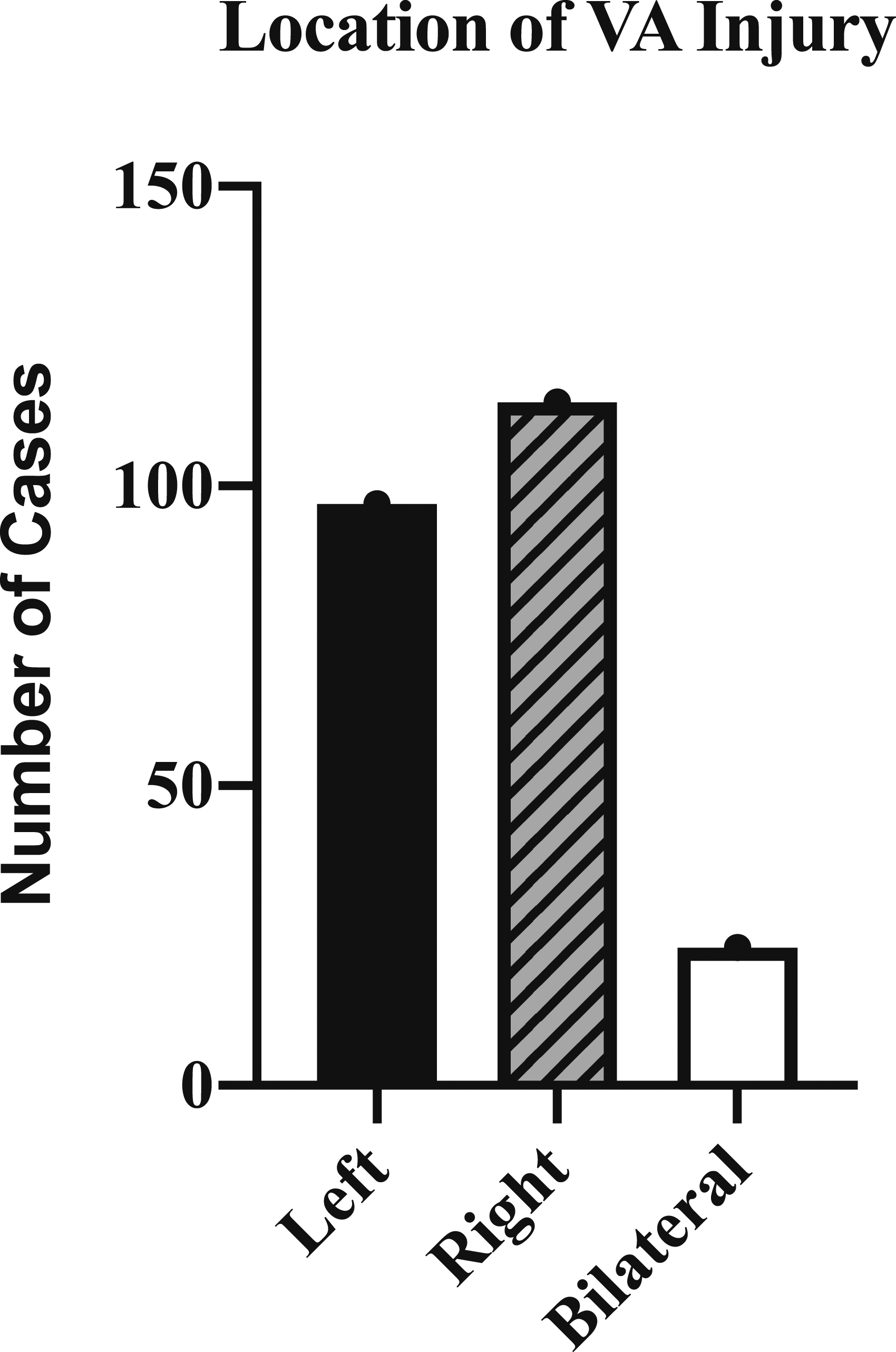
Type of Injury to the VA
Overall, 18/24 studies reported on the type of injury which occurred to the VA. In total, 11/18 of these used the Denver Scale
33
(Biffl et al) to classify these injuries. Furthermore, 9/11 of those studies using the Denver scale reported comprehensive characteristics of the entire cohort, while 2/11 studies only reported which grade was the most common and did not give specific figures. From the 9/11 studies which did give figures for each grade, there were 218 patients analysed (Figure 5). Grade I was the most common (103/218 (47.2%)) injury noted. Others included; Grade II/(53/218 (24.3%)), Grade III (8/218 (3.7%)), Grade IV (53/218 (24.3%)), and Grade V (1/218 (.5%)). In total, 7/18 studies (82 patients with VAI) did not use the Denver scale to demonstrate the injuries. Overall characteristics of injury included occlusion (40/82 (48.8%)), dissection (34/82 (41.5%)), stenosis (4/82 (4.9%)), occlusive-dissection (2/82 (2.4%)), and compression (2/82 (2.4%)). One study was only concerned with VA dissections secondary to injury, Gupta et al
16
noted an incidence of VA dissection of 14.1% (21/149). Grades of VAI. VA: vertebral artery.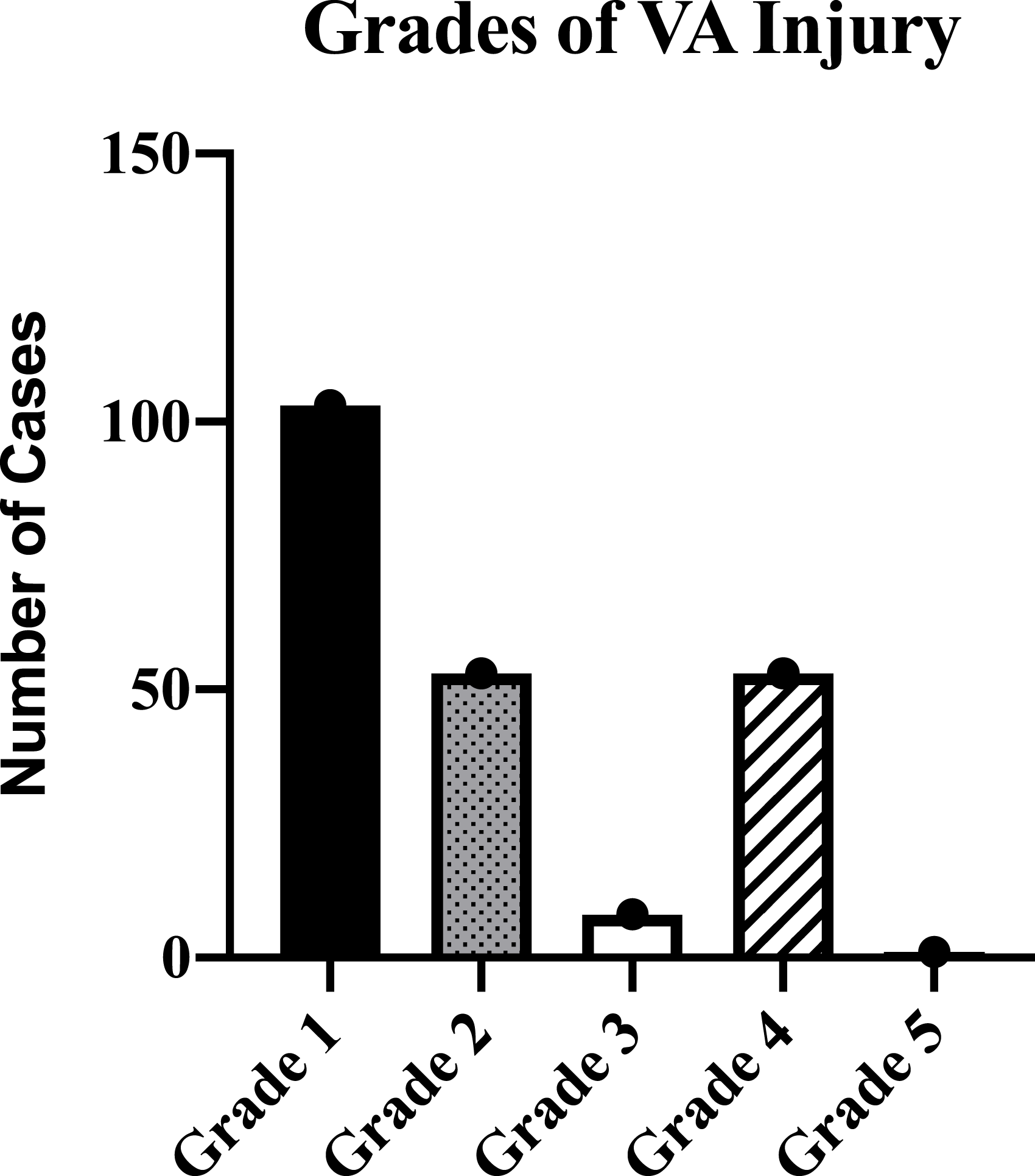
Presentation/Symptoms/Neurological Status
Vertebral Artery Injury Overview.
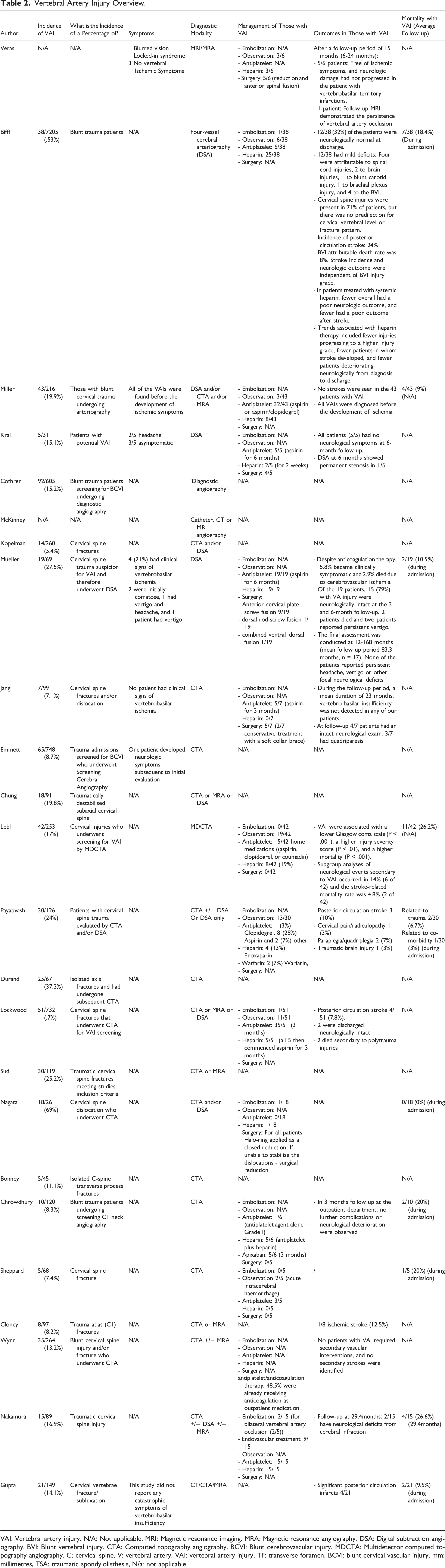
VAI: Vertebral artery injury. N/A: Not applicable. MRI: Magnetic resonance imaging. MRA: Magnetic resonance angiography. DSA: Digital subtraction angiography. BVI: Blunt vertebral injury. CTA: Computed topography angiography. BCVI: Blunt cerebrovascular injury. MDCTA: Multidetector computed topography angiography. C; cervical spine, V: vertebral artery, VAI: vertebral artery injury, TF: transverse foramen, BCVI: blunt cervical vascular injury, mm: millimetres, TSA: traumatic spondylolisthesis, N/a: not applicable.
Diagnostic Modality
All 24 studies reported on the diagnostic modality they utilised. The modalities used overall were CT, CTA, DSA, MRI, MRA and catheter angiography. In the majority of studies, a combination of 2 or more diagnostic modalities were used on the same patient during their admission/part of follow-up. However, no specific reasoning or rationale was provided as to why the studies employed 2 or more different diagnostics modalities. In total, 13/24 reported using CT/CTA, 10/24 reported using DSA, 10/24 used MRI/MRA and 2/24 used catheter angiography (Figure 6). Diagnostic Imaging Modality Utilised and corresponding publications. DSA: Digital Subtraction Angiography, CTA: Computed Topography Angiography. MRA: Magnetic Resonance Angiography, MDCTA: multidetector computed tomographic angiography.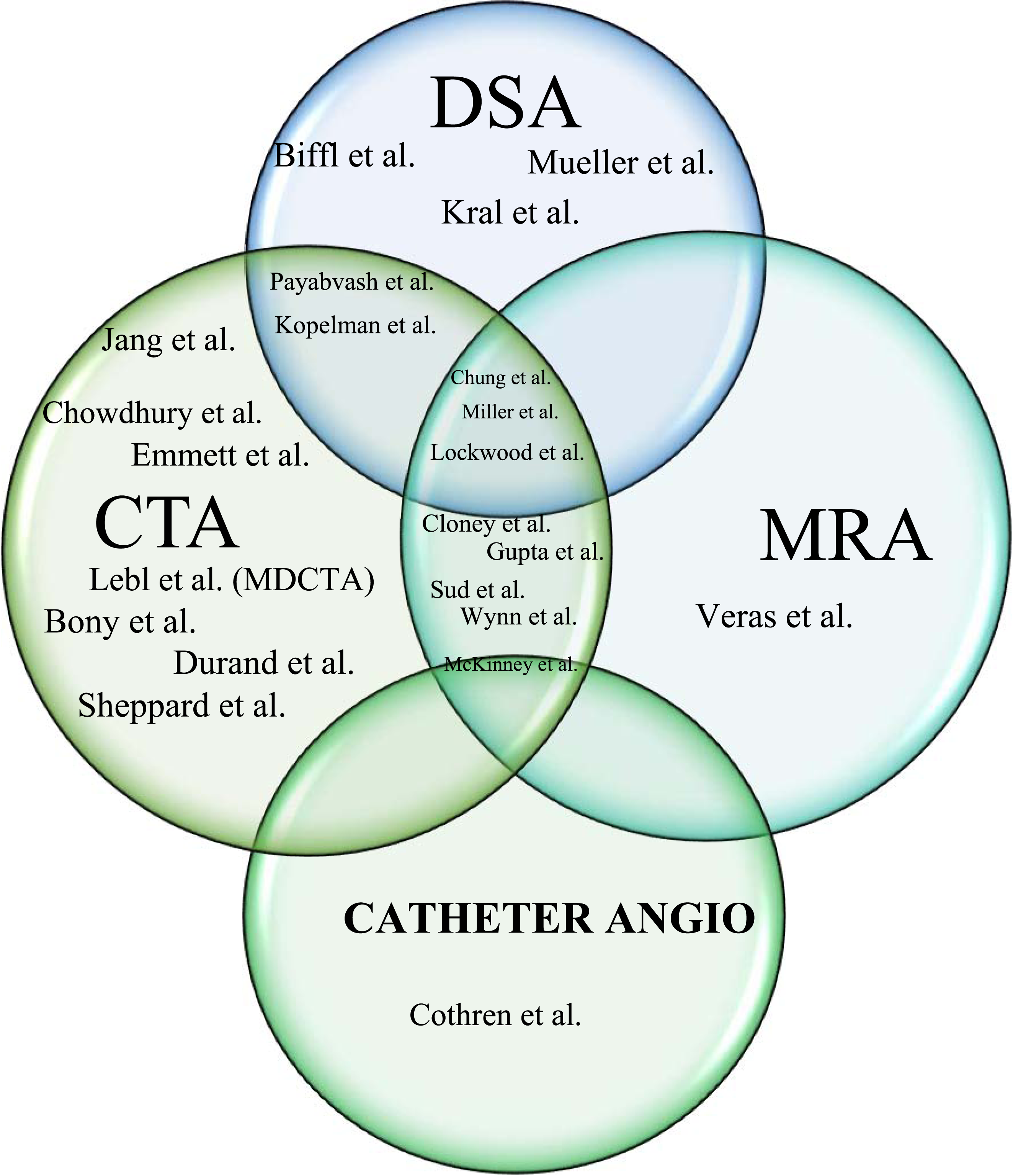
Management
Overall, 13 studies (285 patients) provided comprehensive detail of management strategies. In the majority of studies, the mainstay of treatment was with antiplatelet or anticoagulation agents, or both. Overall, 147/285 (51.6%) received an antiplatelet agent, either as a monotherapy or additional to an anticoagulant after the acute period ranging for 3-6 months. In total, 57/285 (20%) were observed without any antiplatelet or anticoagulant. Authors reported that often this was due to contraindications or acute cerebral haemorrhage on imaging. In total, 95/285 (33.3%) received heparin in the acute period, in the majority of cases for 2 weeks, before either switching to antiplatelet monotherapy or discontinuing all antiplatelet/anticoagulation agents. 5/285 (1.8%) were commenced on Apixaban for 3 months after 2 weeks of intravenous Heparin. Warfarin was commenced in 2/285 (.7%) patients for an unknown amount of time. 5/285 (1.8%) patients underwent embolization of the VA, with 2/5 (40%) of these being for bilateral vertebral artery occlusion. Whether or not a patient underwent surgery for fracture management or to control the VAI is unclear and inconsistent, and therefore we cannot comment on the statistics in this regard. Mueller et al 4 was the only study to describe in detail which VAI patients underwent which surgery. Anterior cervical plate-screw fusion 9/19 (47.4%), dorsal rod-screw fusion 1/19 (5.3%) and combined ventral–dorsal fusion 1/19 (5.3%). See Table 2 for full descriptions of reported management.
Outcomes in Those with VAI
Overall, 10/24 studies reported on mortality. 9/10 reported on mortality during the initial admission (Figure 7). The mortality rate in this group was 32/226 (14.2%), ranging from 0-26.2% The reason for the high mortality in 1 study was related to the fact that its study population were those screened for being high risk of BCVI and for whom angiogram was indicated, however, the VAI-attributable mortality rate was only 4.8% (2 of 42). Only 1/10 study reported on a mortality rate at their follow-up (mean: 29.4months) - 4/15 (26.6%). In-Hospital Mortality Associated with VAI. VAI: vertebral artery injury.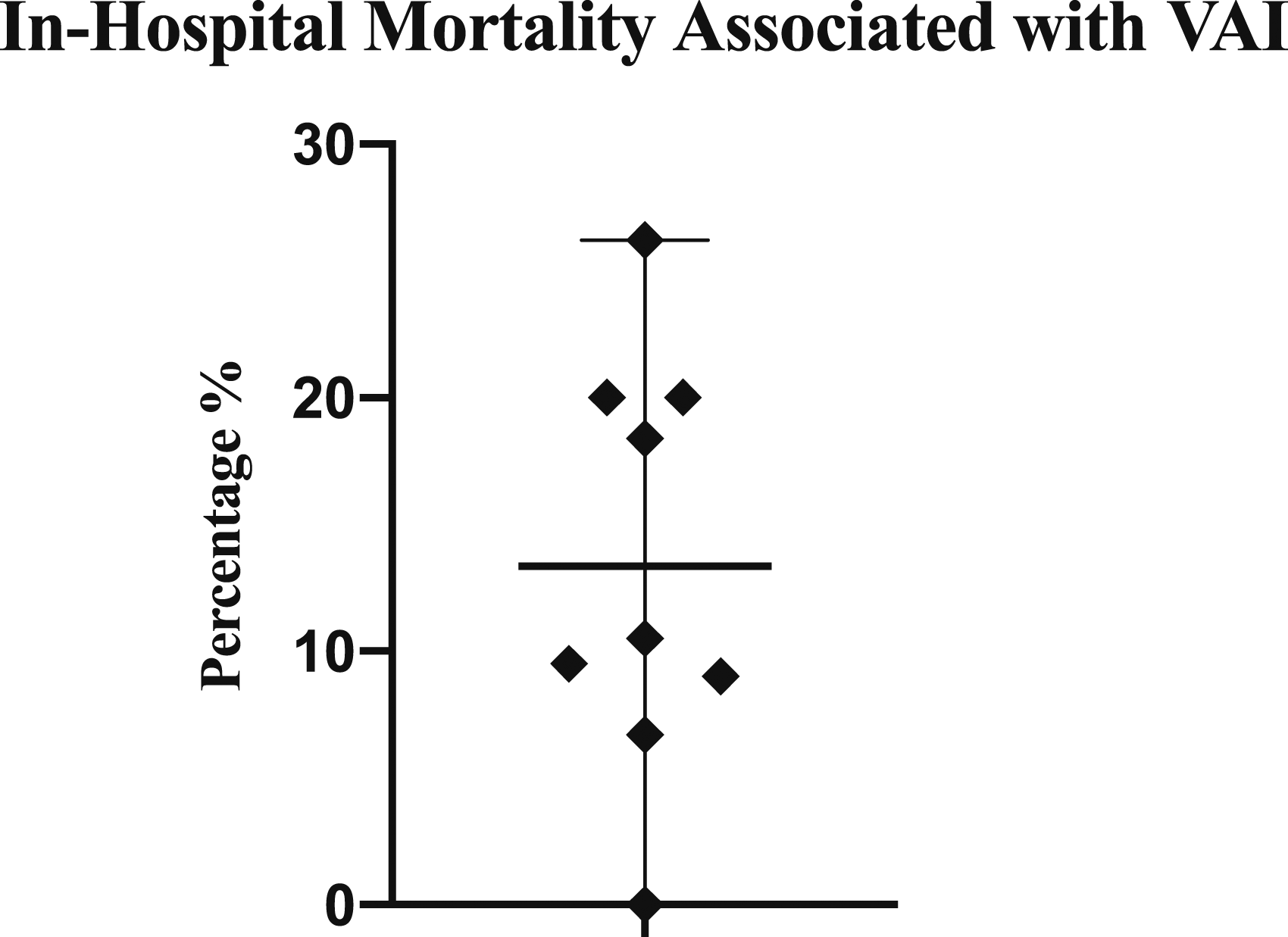
Overall, 14/24 studies reported on outcomes of patients. The outcomes reported are highly heterogenous and therefore the outcomes are displayed as a descriptive narrative in Table 2. Furthermore, it is challenging to differentiate in the studies whether poor outcomes were a consequence of the cervical spinal injury, the VAI, or both. 6/24 studies (with a total of 62 patients) report on follow-up outcomes at outpatient clinic. The mean follow-up across these 6 studies was 26.6 months (3 - 83.3 months). 5/6 of these studies (52 patients) reported on residual neurological deficit at mean follow-up. 46/52 (88.5%) had no neurological symptoms or signs of vertebrobasilar infarct at mean follow-up. 2/6 studies reported on follow-up imaging at outpatient clinic. 1/62 (1.6%) patient’s follow-up MRI demonstrated the persistence of vertebral artery occlusion and 1/62 (1.6%) DSA at 6 months showed permanent stenosis. Full description of outcomes at follow-up are available in Table 2.
Fracture/Injury to Vertebrae and VA
Vertebrae Level
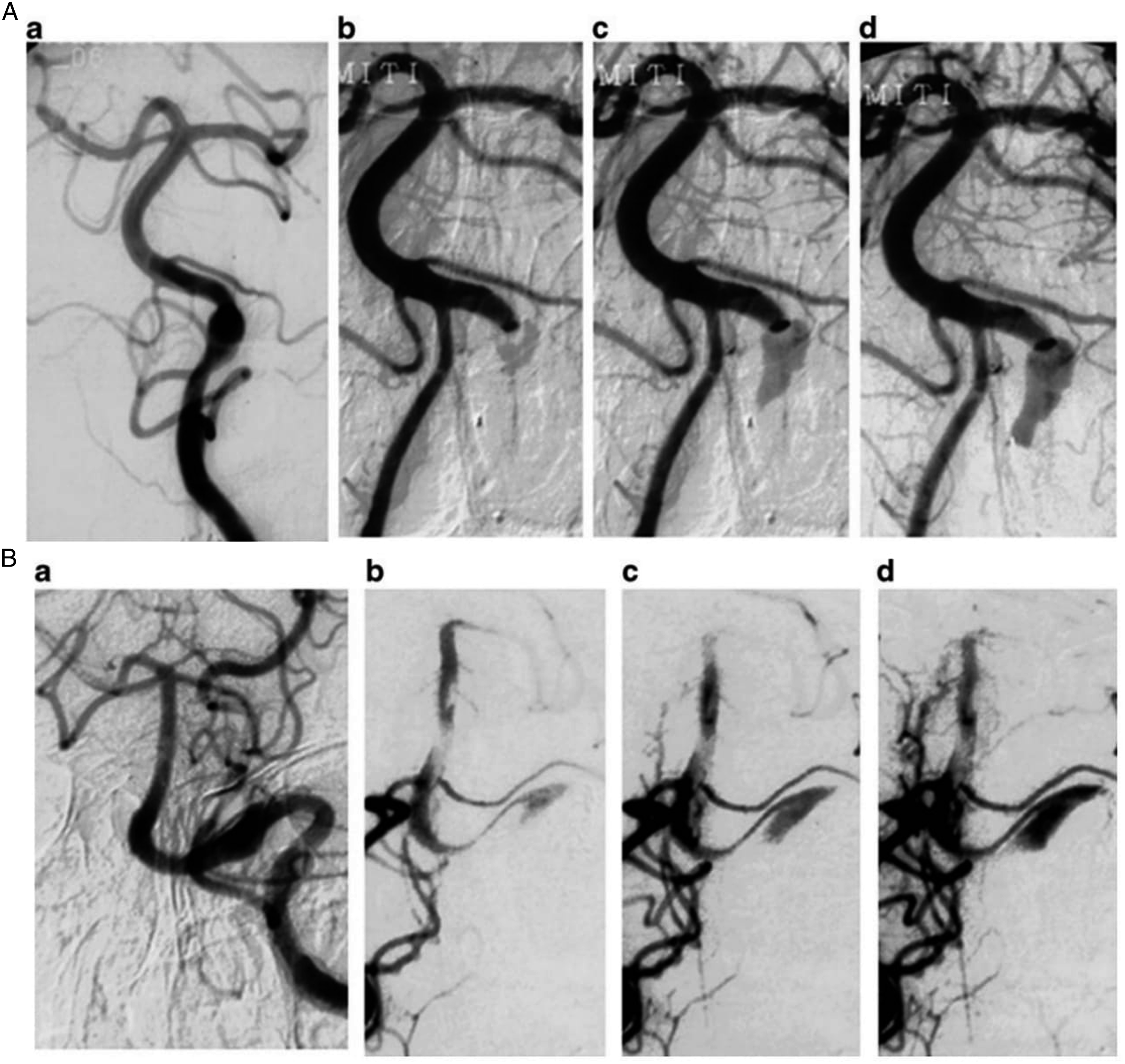
Overall, 12/24 studies reported on where the level of injury/fracture had occurred. There were 285 fractures/injuries in total amongst all patients. The most common level was C5 (71/285 (24.9%)), followed by C2 (56/285 (19.6%)) and C6 (56/285 (19.6%)). Others included; C1 (33/285 (11.6%)), C4 (31/285 (10.9%)), C3 (20/285 (7.0%)) and C7 (18/285 (6.3%)). 1/24 studies reported on the 3 most common levels (most common: C6, followed by C5, then C4 and C3. 1/24 studies were only concerned with fractures at C1. Similarly, 1/24 studies analysed only C2 fractures, and 1/24 analysed those with C1 and C2 injuries. 8/24 did not report any information on the level (Figures 8 and 9). Type 4 left vertebral artery injury with acute ischemic stroke following corrective spinal surgery. A) CTA demonstrating a cervical spine fracture/subluxation with occlusion of the left vertebral artery (arrow). B) CTA demonstrating occlusion of the left vertebral artery (arrow). C) DWI sequence obtained after corrective cervical spine surgery with evidence of an acute ischemic stroke. D) MRA demonstrating restored patency of the previously occluded vertebral artery (1). Type A dissecting aneurysm. A) DSA of the left vertebral artery showing a fusiform dilation. b, c, d Consecutive angiograms of the right vertebral artery during balloon test occlusion showing that the site of dissection is opacified distal to proximal (2). Type B dissecting aneurysm. A) DSA of the left vertebral artery showing a fusiform dilation. b, c, d Consecutive angiograms of the right vertebral artery during balloon test occlusion showing that the site of dissection is opacified proximal to distal (2).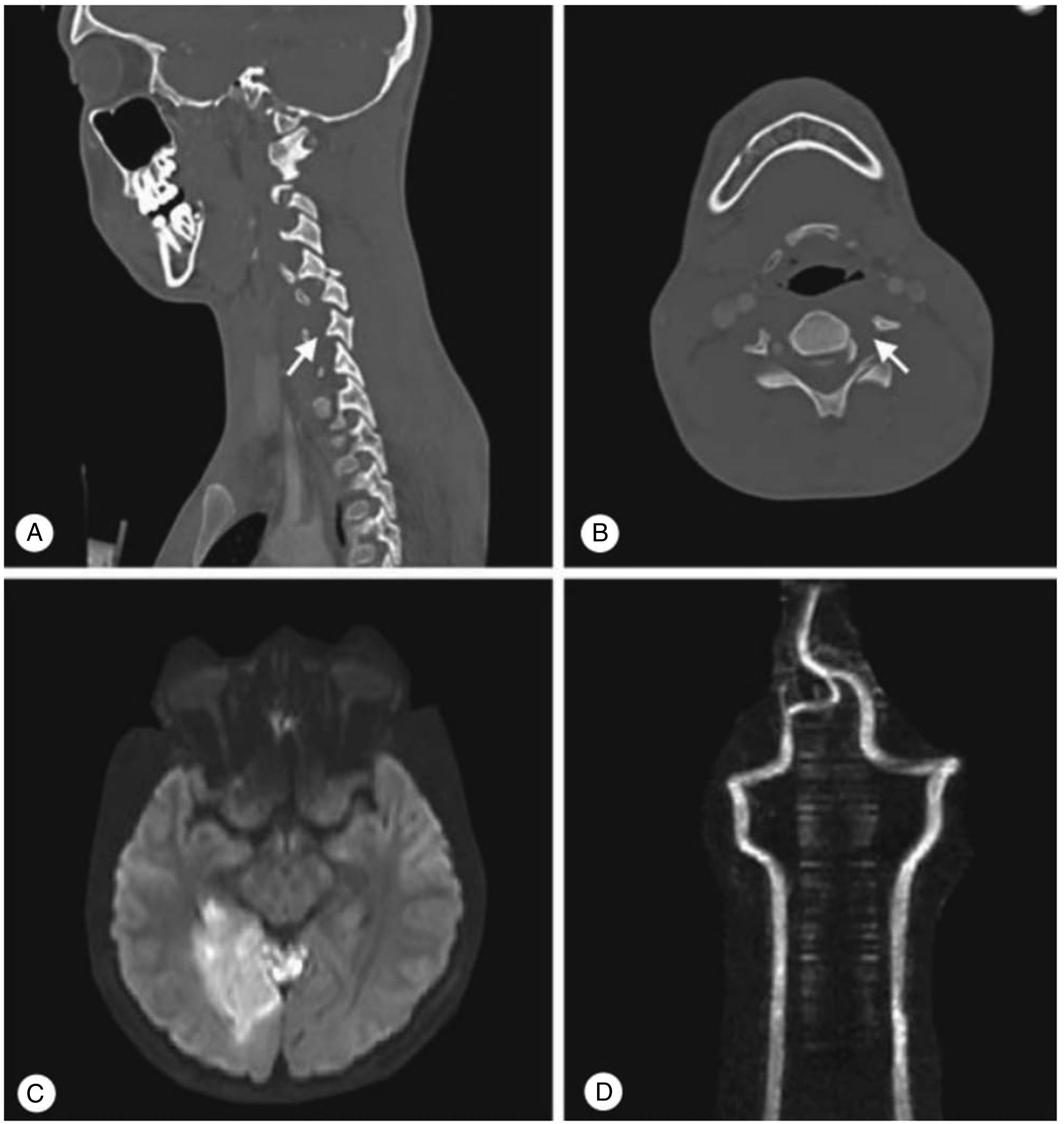
Injury/Fracture Characteristics
Statistically significant factors associated with greater odds of having vertebral artery injury.
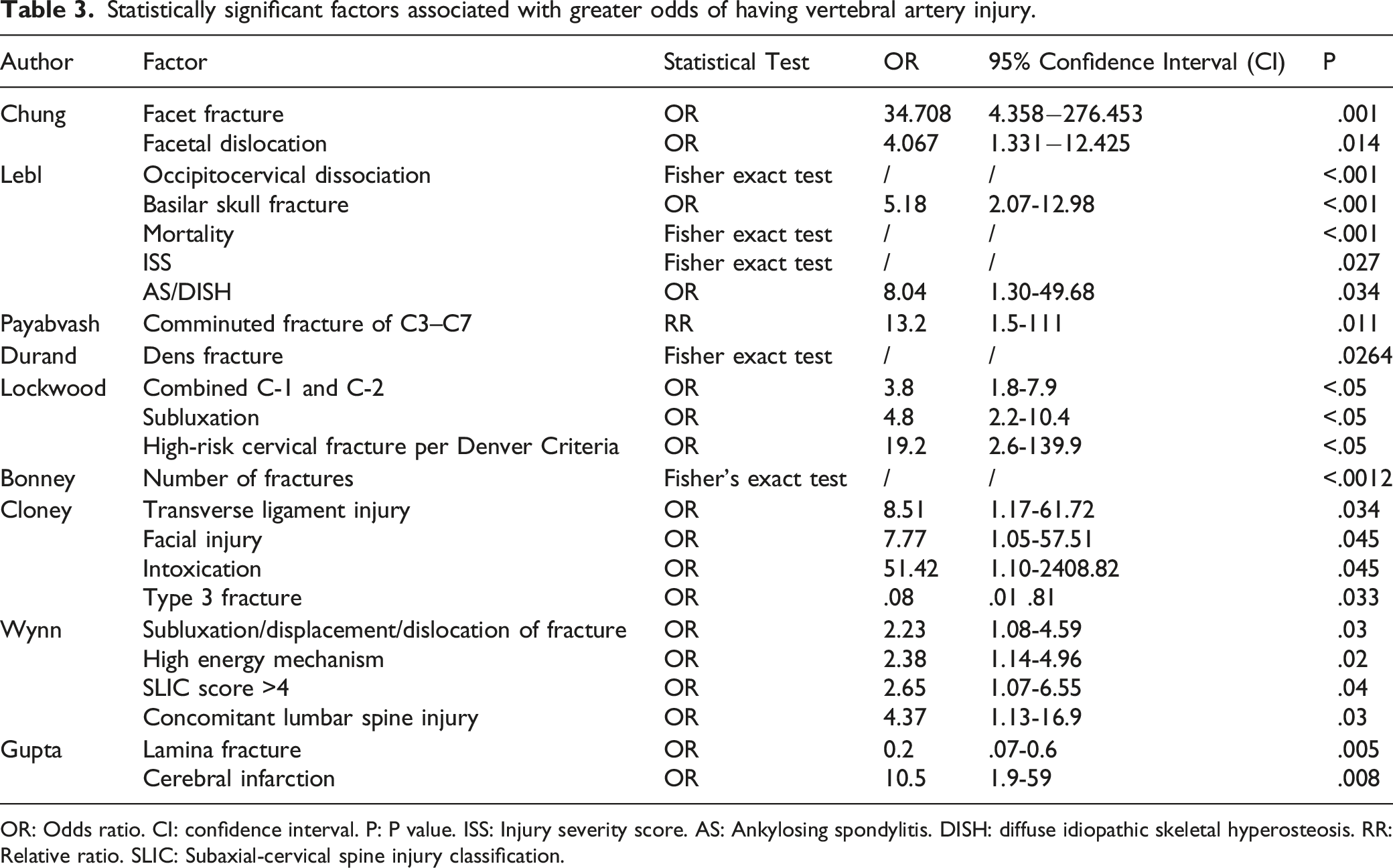
OR: Odds ratio. CI: confidence interval. P: P value. ISS: Injury severity score. AS: Ankylosing spondylitis. DISH: diffuse idiopathic skeletal hyperosteosis. RR: Relative ratio. SLIC: Subaxial-cervical spine injury classification.
Significant and non-significant transverse foramen injuries and association to VAI.
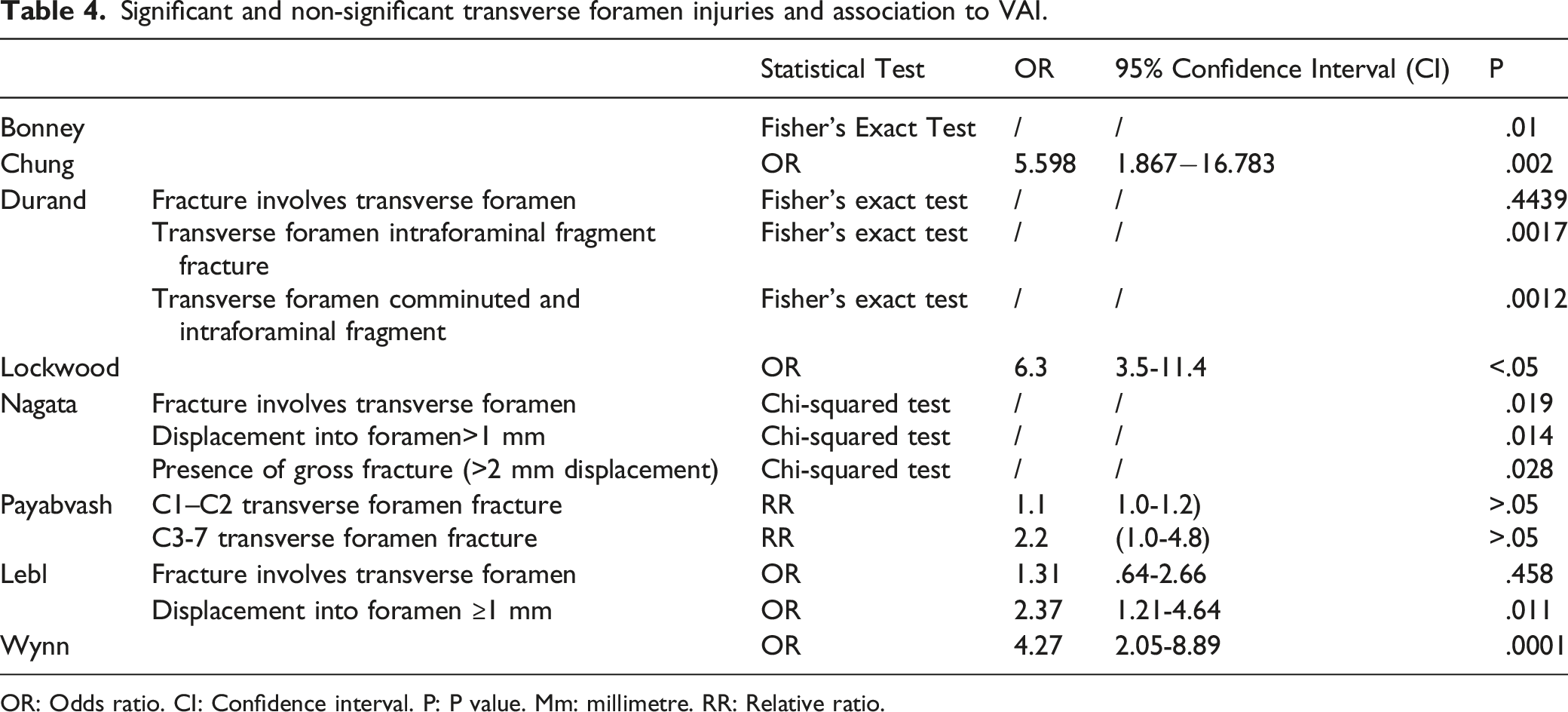
OR: Odds ratio. CI: Confidence interval. P: P value. Mm: millimetre. RR: Relative ratio.
Discussion
Injury to the cervical spine occurs in 2.4% of blunt trauma patients. 34 The majority of the spinal injuries (60%) involve young healthy males between 15 and 35 years old with cervical spine injuries being the most common location of traumatic injury to the spine. 35 The cervical spine remains the most common level for spinal cord injury (SCI), representing 55% of all SCIs. 36 The first incidence of VAI associated with cervical spine fracture was described by Carpenter et al in 1961. 12 Since then, a variation of VAI incidence (.53-39%) has been reported in the literature, with high rates of morbidity and mortality shown across studies. Certain studies have reported mortality rates as high as 31%. 37 From our review, only 1 study examined VAI attributable mortality (4.8%). 20 We found a collative mortality rate of 14.2% during initial admission, pooled with other risk factors for mortality in cervical trauma.
As such, identification and diagnosis is paramount to negating morbidity and mortality rates associated with VAI in cervical spine trauma patients. This can prove difficult in a significant proportion of patients as many present without symptoms. Therefore, practicing spine surgeons must maintain a high degree of clinical suspicion. Recent studies have sought to elucidate high risk characteristics predictive of VAI. Results have identified the following risk factors; upper cervical fracture (OR: 2.34 (95% CI 1.93, 2.84) p<.001), multiple levels fractured (1.25 (95% CI 1.04, 1.51) p = .02), involvement of the transverse foramen (OR: 11.31 (95% CI 9, 14.22) p<.001), high-energy injuries (OR: 1.79 (95% CI 1.43,2.23) p<.001), and subluxation or dislocation (OR: 1.96 (95% CI 1.43,2.63) p<.001).38,39 The intimate relationship of the VA with the transverse process in the cervical spine requires close attention, especially when the transverse process fracture extends into the transverse foramen (TF).29,35 Woodring et al 40 performed arteriography on 8 patients who had cervical fracture with TF involvement - 7 (88%) had blunt VAI. This fragile relationship between TF fractures and VAI is corroborated by our findings, which found an overall incidence of VAI in TF fracture of 45.2%.
High clinical suspicion can be aided by modern advancements in diagnostic imaging. The main diagnostic techniques utilized include; CTA, DSA, MRA, catheter angiography and less notably, US doppler. Although DSA is traditionally the gold standard, our study suggests that CTA is the most commonly adopted in this setting (54.2% of studies included in the systematic review). Numerous studies have demonstrated high accuracy levels of CTA in detecting “clinically significant injuries”.41,42 CTA is becoming the opportunistic screening test of choice under both urgent and emergency circumstances.
However, review of the literature shows discordance in its use as a first line diagnostic tool. Mitha et al report CTA has high sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of CT of 98%, 100%, 100%, 99%, and 99% respectively. 43 In Mueller et al, 4 results show a high degree of concordance between DSA and CTA in the detection of a VAI. Nonetheless, prior studies have demonstrated false positive rates as high as 47% when used in the setting of blunt cervical injury for identification of VAI. 44 Similarly, a systematic review in 2013, which highlighted 8 studies examining 5704 carotid or vertebral arteries in 1426 trauma patients, the sensitivity and specificity for BCVI detection with CTA vs DSA was 66% (95% CI, 49%-79%; I = 80.4%) and 97% (95% CI, 91%-99%; I = 94.6%), respectively. Novel CT models are capable of much faster acquisition times (multidetector CT) compared to conventional CT. Many centres believe this has improved accuracy of VAI, 42 yet there remains a lack of comparative robust evidence to date for identification accuracy of VAI. MRA, another non-invasive diagnostic procedure, has considerable advantages, including; the lack of iodinated contrast products, avoidance of bony artefact, and earlier diagnosis of cerebral infarction. 45 However, screening studies have reported poor specificity at 67%, with sensitivities ranging from 50-75%. 46 Similarly, a recent meta-analysis reported an overall sensitivity of 55%. 47
Similar to VAI identification and diagnosis, it is vital that this devastating injury is managed in an organised, evidence-based manner in order to improve patient outcomes. Furthermore, spinal trauma centres should take a multidisciplinary approach, involving early neurological, orthopaedic and vascular input. The mainstay management strategy for surgically inaccessible injuries is antithrombotic therapy,48,49 however, associated injuries often present a contraindication to antithrombotic therapy. The literature has shown up to 30% of trauma patients are contraindicated for antithrombotic therapy based on concomitant injuries.31,50 Endovascular intervention is another option, however stents also require antithrombotic therapy post-placement. For patients with BCVI who do not have a persistent neurologic deficit in the territory of the injured artery and who do not have contraindications, antithrombotic therapy is recommended (unfractionated heparin and antiplatelet agents) over no such therapy.51-53 Neurologic outcomes are improved in symptomatic patients, and fewer ischemic neurologic events (stroke) occur in asymptomatic patients who are treated with antithrombotic therapy.54,55 The optimal medical treatment of VAI is still under debate, and an evidence based protocol on anticoagulation in patients with VAI does not exist. However, anticoagulative treatment appears standard therapy to date, as it is associated with reduced occurrence of secondary stroke.56,57 Previous studies showed a decreased stroke rate from 30-50% to 2-10% using anticoagulation or antiplatelet therapy.56,58 Regarding surgical intervention, early surgical fixation is considered to be indicated when concerned with an unstable cervical spine fracture in order to prevent further potential neurological and VAI damage. 43 Although a consensus regarding VAI treatment is lacking, early diagnostic steps followed by a standardised treatment protocol is key. Intravenous anticoagulation, and if accessible and indicated – early stabilization, in the acute stage followed by an oral anticoagulant are seen as protection of the vertebrobasilar circulation, although more robust randomised trials are needed.
Delphi studies are an example of technique which can lead to improved treatment strategies and protocols. This model can improve efficient use of health care resources within the field of cervical trauma and has been utilized with success in other challenging pathologies 59 and in the setting of acute cervical spine trauma. 60
The review had several limitations. Firstly, the majority of the studies were retrospective reviews. Robust prospective, randomised controlled trials and qualitative Delphi studies are needed to define treatment and diagnostic protocols. Although the incidence of VAI in blunt cervical trauma remains low, the importance of deriving effective treatment protocols remain essential due to poor outcomes and high mortality rate. Secondly, there was a small number of directly relevant studies in the literature, and the quality of studies was low. Furthermore, there are no randomised controlled trials regarding management strategies to date. Thirdly, there was heterogeneity of study design, outcome measures and study populations between the included studies which precluded substantial collative meta-analysis. Finally, the true VAI attributable mortality rate was not calculated, given only 1 study commented on it. Furthermore, the majority of studies were retrospective in design and did not control for other confounding factors.
Nevertheless, our study provides an indication of incidence, characteristics, and effective management strategies that will aid spine surgeons in maintaining a high degree of clinical suspicion in order to attempt to minimise morbidity and mortality rates associated with VAI.
Conclusion
VAI secondary to cervical spine trauma has a notable incidence and high associated mortality rates. Ultimately, this is a rare but life-threatening injury. There is a high incidence of VAI when associated with transverse foramina injury. The current available literature is limited by a low quality of evidence. In order to optimise diagnostic protocols and treatment strategies, in addition to reducing mortality rates associated with VAI, robust quantitative and qualitative studies are needed. Utilizing evidence-based clinical parameters to predict chance of VAI may avoid unnecessary advanced imaging, alongside improving patient outcome. Nevertheless, practicing spine surgeons should reserve a high degree of clinical suspicion for associated VAI when dealing with traumatic cervical injuries.
Supplemental Material
Supplemental Material - The Incidence, Characteristics and Outcomes of Vertebral Artery Injury Associated with Cervical Spine Trauma: A Systematic Review
Supplemental Material for The Incidence, Characteristics and Outcomes of Vertebral Artery Injury Associated with Cervical Spine Trauma: A Systematic Review by Hugo C. Temperley, Jake M. McDonnell, Niall J. O’Sullivan, Caitlin Waters, Gráinne Cunniffe, Stacey Darwish, and Joseph S. Butler in Global Spine Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Compliance with Ethical standards
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent to be included in the study, or the equivalent, was obtained from all patients.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.