
Abstract
Study Design:
Retrospective study.
Objective:
To identify if a 1- to 2-level posterior lumbar fusion at higher altitude is an independent risk factor for postoperative deep vein thrombosis (DVT) and pulmonary embolism (PE).
Methods:
A national Medicare database was queried for all patients undergoing 1- to 2-level lumbar fusions from 2005 to 2014. Those with a prior history of DVT, PE, coagulopathy, or peripheral vascular complications were excluded to better isolate altitude as the dependent variable. The groups were matched 1:1 based on age, gender, and comorbidities to limit potential cofounders. Using ZIP codes of the hospitals where the procedure occurred, we separated our patients into high (>4000 feet) and low (<100 feet) altitudes to investigate postoperative rates of DVTs and PEs at 90 days.
Results:
Compared with lumbar fusions performed at low-altitude centers, patients undergoing the same procedure at high altitude had significantly higher PE rates (P = .010) at 90 days postoperatively, and similar rates of 90-day postoperative DVTs (P = .078). There were no significant differences in age or comorbidities between these cohorts due to our strict matching process (P = 1.00).
Conclusion:
Spinal fusions performed at altitudes >4000 feet incurred higher PE rates in the first 90 days compared with patients receiving the same surgery at <100 feet but did not incur higher rates of postoperative DVTs.
Keywords
Introduction
Following many orthopedic surgeries, chemical antithrombotic medication is a mainstay of the anticoagulation protocol, yet for patients undergoing spinal fusions, the risk of postoperative hematomas (0.2%-1.5%) causing symptomatic cord compression frequently outweighs the benefits of chemical anticoagulation. 1 -3 Other modalities such as sequential compression devices, compression stockings, and early ambulation can also be utilized to lessen the venous thromboembolic (VTE) risk. 1,4 -6 Identification of VTE risk factors and the management of these hazards is another strategy to prevent their occurrence.
Higher altitudes lead to physiological changes that may predispose to VTEs, including deep vein thrombosis (DVT) and pulmonary embolism (PE). Other researchers have shown a correlation with postoperative VTEs based on the altitude of surgical center, thus indicating those in a higher elevation may be more at risk for VTEs. 7 -10 While this concept has been evaluated for postoperative orthopedic patients undergoing acute air travel, the influence of altitude has never been explored in spine surgery patients. 11
Knowledge of VTE risk factors and the possible mitigation of these risks could lead to improved patient outcomes for spine surgery patients. By comparing the rates of PEs and DVTs in patients undergoing spinal fusions at a low altitude to those at a higher altitude, we can determine if altitude is a potentially modifiable risk factor for VTEs following spinal fusion. This study is the first to evaluate the impact of altitude on spine surgery patients.
Materials and Methods
Data Source
PearlDiver (PearlDiver Technologies, West Conshohocken, PA, USA) is a privately owned dataset containing the full 100% sample of Medicare data during a studied period. It registers various interventions and conditions based on Current Procedure Terminology (CPT) codes as well as International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) diagnoses and procedures. This data is anonymous and de-identified; no institutional review board was required. Medicare was the nationwide insurance provider for our patient selection. A thorough evaluation of the PearlDiver database was performed for patients undergoing 1- to 2-level posterior lumbar fusions from 2005-2014.
Patient Selection
Using ICD-9 procedural code terminology, we were able to isolate patients who underwent posterior lumbar spinal fusion surgery (ICD-9: 81.07, 81.08) of 1-2 levels (ICD-9: 81.62). To limit cofounders, we excluded those also having fusions of the cervical or thoracic spine (ICD-9: 81.01 - 81.05) as well as those undergoing a revision spinal fusion (ICD-9: 81.30 to 81.39) (Supplemental Table S1). Patients with a prior history of DVT (ICD-9: 453.40), PE (ICD-9: 41.51), VTE (ICD-9: V12.51), hematological coagulopathies (ICD-9: 289.81 289.82), unspecified coagulation defects (ICD-9: 28.69), or peripheral vascular complications (ICD-9: 997.2) were excluded from our study to remove potential cofounders and further isolate altitude as the variable of interest. 8
After application of this criteria, the resulting cohorts was then separated based on the geographic location of the actual surgery. The 5-digit zip codes provided through Zip-Codes (Datasheet LLC, Hopewell Junction, NY, USA) gave the geographic locations of the continental United States with regard to altitude (Figure 1). We separated our groups into high altitude (>4000 feet) and low altitude (<100 feet).
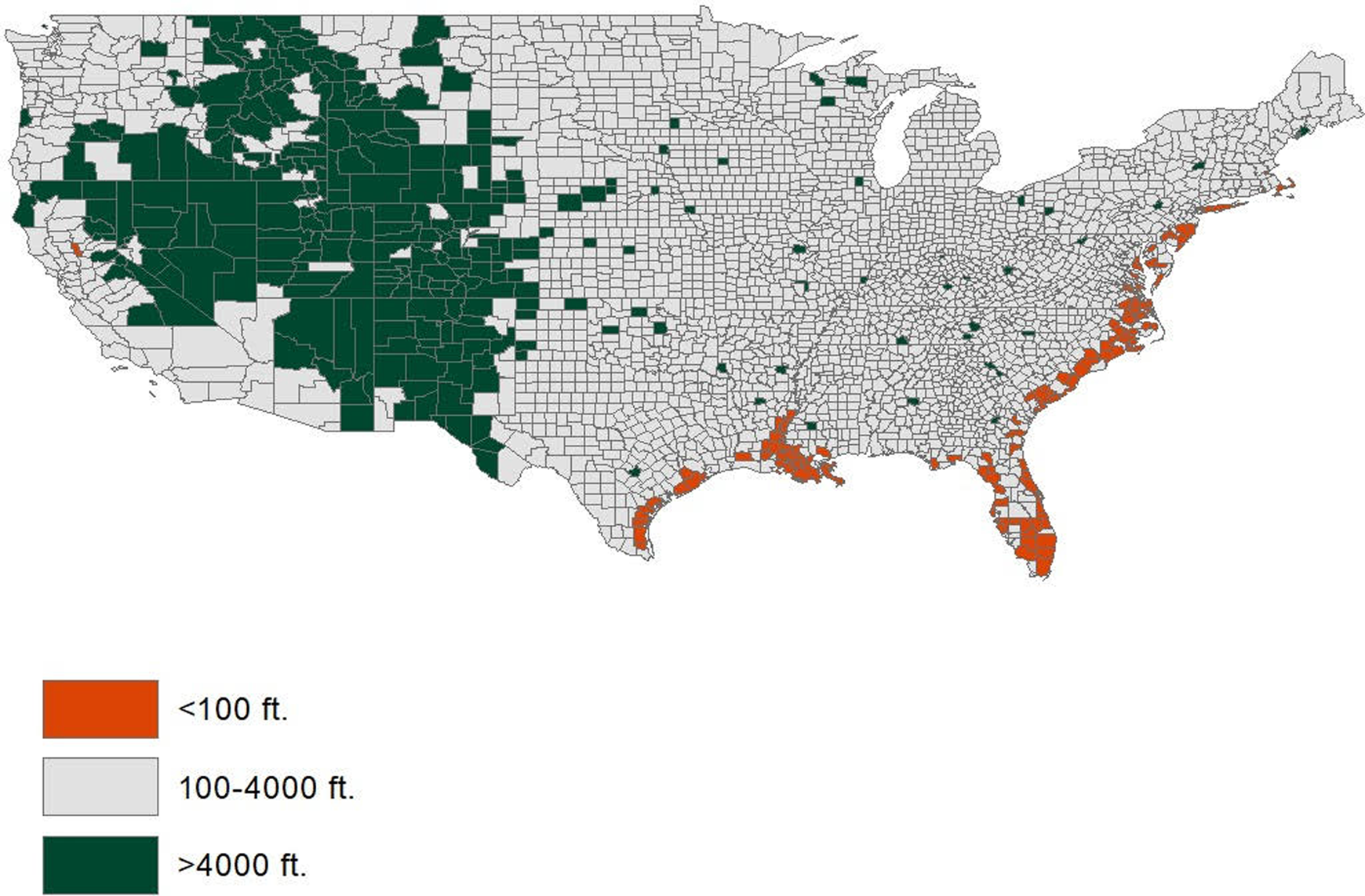
Geographic altitude (feet) of the mainland United States.
Data Analysis
Using Boolean operations, our 2 groups were matched based on age, gender, Charleston Comorbidity Index (CCI), and comorbidities known to be associated with postoperative VTEs: hypertension, body mass index >30 kg/m2, tobacco use, diabetes mellitus, and hyperlipidemia. Matching was performed strictly on a one-to-one basis, where for every patient in the cohort study, there was one patient in the control group selected. As has been demonstrated in other orthopedic Medicare database research, CCI is a marker to ensure that both cohorts were matched properly and no statistical difference existed between the 2 groups. 12,13 Since comorbidities represent categorical variables, a Pearson chi-square analysis was performed to determine the significance between the study and control groups, whereas Welch’s t test was utilized to test for significance in CCI between the cohorts.
The rates of PEs and DVTs were compared between high and low altitudes 90 days postoperatively using binary logistic regression analysis. A P value <.05 was used to define statistical significance. Descriptive and statistical analysis were performed using the software Statistical Package for Social Sciences [SPSS] version 23 (IBM Corp, Armonk, NY).
Results
A total of 155 173 low-altitude patients and 44 320 high-altitude patients were initially identified as having primary 1- to 2-level posterior lumbar fusions performed between 2005 - 2014. After patient matching, each cohort had 44 289 patients. The majority of patients were female (55.5%) and in the 65- to 74-year age-group (53.6%). Also, the majority of the patients had a previous diagnosis of hypertension (82.1%) and hyperlipidemia (64.4%). Interestingly 41.6% of patients were diabetic and 22.6% were recoded as tobacco users. There were no significant differences in age or comorbidities between these 2 cohorts as a result of our strict matching process (P = 1.00). The CCI of the matched cohorts was 5.93 ± 2.61 (P = 1.00) (Table 1).
Combined High- and Low-Altitude Cohort: Demographics Characteristics Spinal Fusion.a
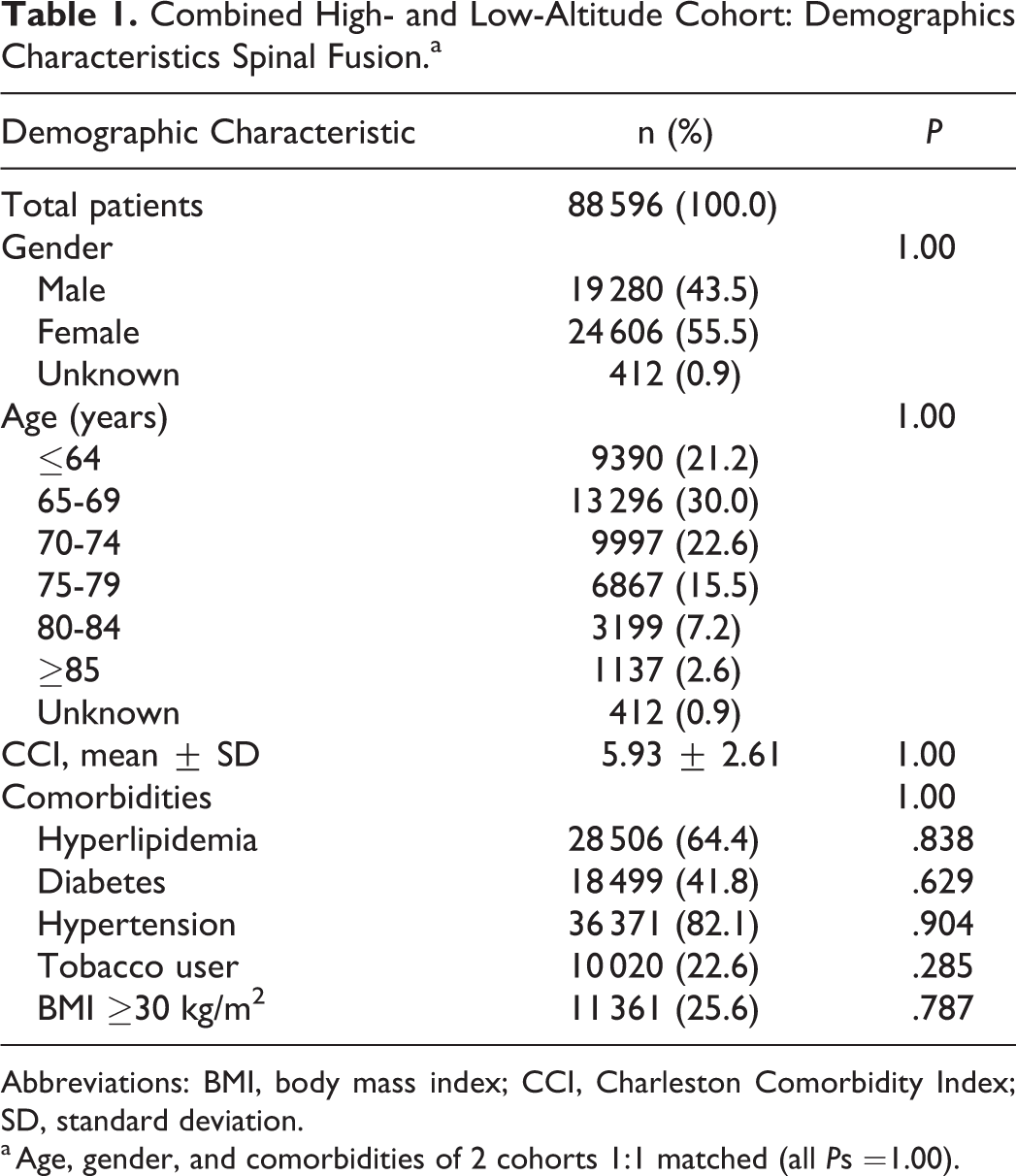
Abbreviations: BMI, body mass index; CCI, Charleston Comorbidity Index; SD, standard deviation.
a Age, gender, and comorbidities of 2 cohorts 1:1 matched (all Ps =1.00).
Ninety Days Postoperative
The high-altitude group at 90-days postoperative had rates of DVTs and PEs of 0.84% and 0.49%, respectively; this was compared to low altitude with rates of 0.97% for DVTs (P = .078) and 0.35% for PEs (P = .010). At 90 days postoperatively, there were significantly higher rates of PEs (odds ratio [OR] 1.38; P = .010) for patients at higher altitude, yet similar rates DVTs (OR 0.86; P = .078) (Table 2 and Figure 2).
DVT and PE Rates Following 1- to 2-Level Posterior Lumbar Fusions at Various Altitudes.a
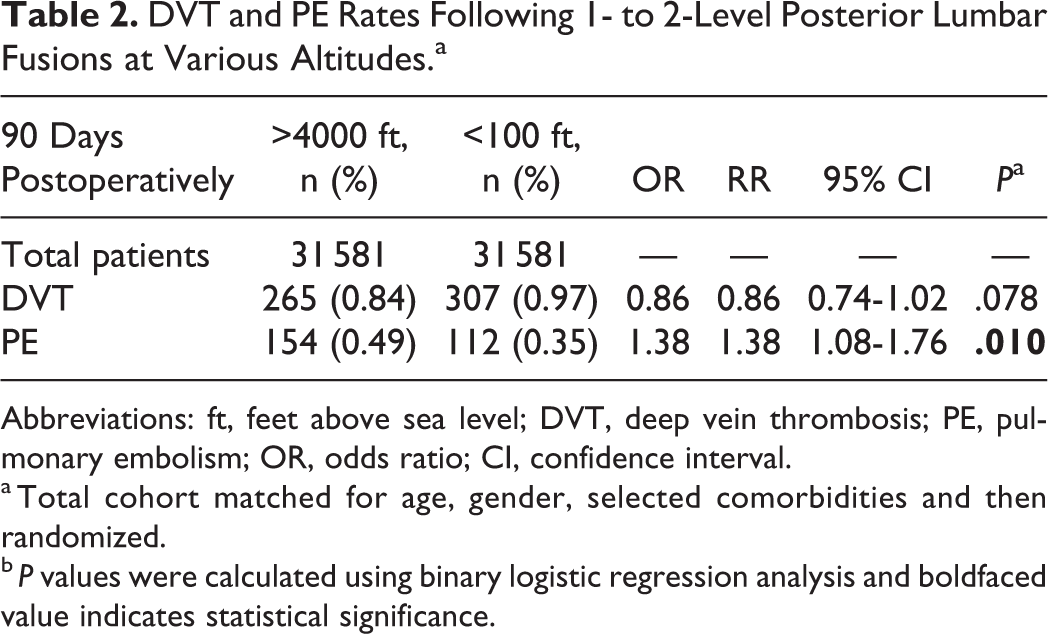
Abbreviations: ft, feet above sea level; DVT, deep vein thrombosis; PE, pulmonary embolism; OR, odds ratio; CI, confidence interval.
a Total cohort matched for age, gender, selected comorbidities and then randomized.
b P values were calculated using binary logistic regression analysis and boldfaced value indicates statistical significance.
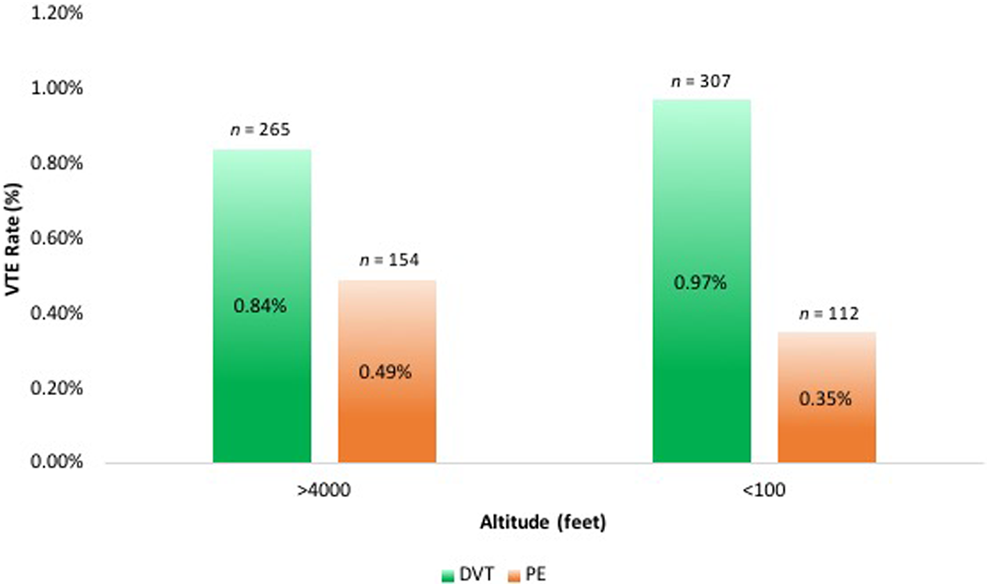
Ninety-day postoperative VTE rates at high- and low-altitude centers. DVT, deep vein thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism.
Discussion
Prior Orthopedic Reviews of VTEs and Impact of Altitude
Previously, certain orthopedic procedures have been shown to have higher VTE rates at high altitudes. 9 Tyson et al 9 reviewed 35 877 undergoing knee arthroscopy at 1000 feet vs 4000 feet and determined those at higher elevations were at a significantly higher risk of DVT but not PE. Similarly, Cancienne et al 8 reviewed 64 291 Medicare patients undergoing the same procedure but compared 100 feet with 4000 feet to determine that at both 30 and 90 days postoperatively, the rates of VTE, DVT, and PEs were increased in the higher altitude cohort. Damador et al 10 reviewed Medicare patients undergoing a total hip arthroplasty at 100 feet to 4000 feet and determined a significantly higher rates of 90-day postoperative PEs (1.59) but not DVTs. A strength of those studies is the uniformity with the procedures they examined, in that there is considerably less variation compared to spine fusion techniques. That said, those studies are potentially flawed due to the wide range of anticoagulation protocols used following joint arthroplasties procedures, which cannot be accounted for in using these databases. Similar to this current study, those insurance database studies are not able to identify the method of VTE diagnosis (ie, clinical, ultrasound, angiogram), which is a potential cofounder that hopefully is mitigated from using such a large sample of patients.
A presumed strength of this current study is the very low rate of anticoagulation usage following spine surgeries, due to the significant epidural hematoma risks. Likely, this lack of anticoagulation in the vast majority of our studied cohort potentially makes the postoperative management of this spine group more uniform and comparable as opposed to other published orthopedic studies concerning elevation and VTE risks.
Physiological Considerations
There are many physiological changes occurring at higher altitudes that may predispose to higher VTE rates; however, the precise etiology of altitude-associated hypercoagulability has not been identified. At higher elevations, a hypobaric, hypoxic environment leads to increased erythropoietin production, sustained hyperventilation, and changes in the oxygen-hemoglobin dissociation curve. 14,15 Decreased partial pressures of oxygen correlate with decreased oxygen saturation percentages, and Ninivaggi et al 16 demonstrated that at high altitudes oxygen saturation can decrease as much as 10% from baseline. These acute physiologic changes ultimately result in a systemically hypoxic state, which is associated with increased endothelial cell damage, vascular permeability, and activity of the coagulation cascade via significant increases in factor VIIa, prothrombin, and thrombin-antithrombin complexes. 16,17 During the initial acclimatization period to higher altitudes, these systemic changes create a hypercoagulable state 18 ; however, it is not clear if this change directly causes VTEs. What has been shown is that this elevation results in a sympathetic alteration that promotes coagulation and shifts the immune response to a pro-inflammatory state. 19,20
Possible Causes
While this cohort had 1.38 times the risks of PEs, we did not demonstrate a significant increase in DVT risk when it came to performing lumbar fusions at high altitude versus low altitude 90-days postoperatively. One theory for this finding may be due to the site of injury/insult. Surgery to the lower extremities may predispose one to DVTs as this insult is occurring at a site already at risk for developing a DVT, unlike spine surgery. Additionally, it could be hypothesized that those surgically treated degenerative disc disease living at different altitudes have negligible differences in lifestyles that would predispose to DVTs. Even so, this cohort was already matched for DVT risk factors (listed in the Methods section) to better isolate altitude as variable. Furthermore, it is likely that many patients did in fact develop DVTs but were asymptomatic and never formally diagnosed. This discrepancy might also explain why a significant difference is able to be reported for the more symptomatic PEs as compared to the frequently underdiagnosed DVTs. While we would assume the rates of asymptomatic DVTs would be equivalent in both altitude settings, additional prospective studies would be required to confirm.
It is also possible that some of the PEs recorded were found incidentally or not actually clinically relevant, but due to different management protocols certain centers are more likely to order additional studies to evaluate a patient postoperatively. 21 -23 For instance, if by chance there are several high elevation centers that happen to have a lower threshold for ordering duplex ultrasound then these centers would inherently have higher rates of VTEs in that they were actively looking for them at a more frequent rate. Unfortunately, our methods and data does not allow us to identify which patients or centers obtained imaging studies to aid the diagnosis. Additionally, while the DVT risk at high altitude was significantly higher than that at low altitude, the low event rates at both conditions suggest that this difference has low clinical relevance despite being statistically significant. Further studies evaluating the effects of altitude on postoperative patients could better identify potentially modifiable risk factors.
Financial Impact
Apart from the concern for patient outcomes associated with VTEs, the financial burden of VTEs in spine patients should also be considered. For patients undergoing surgery for spinal deformity, a VTE is associated with a 230% to 310% increase in hospital costs. 24 Furthermore, a national inpatient survey review from 2002 to 2008 showed that VTEs after thoracic/thoracolumbar spinal fusions were associated with significantly increased total hospital costs ($260 208 vs $115 474), longer hospital stays (16.6 vs 6.74 days), as well as increased patient mortality (4.33% vs 0.33%). 25 These increased costs associated with VTEs are also continued on an outpatient and readmission basis. One study of 204 308 spinal fusion patients showed those with VTEs had significantly higher readmission rates and generated higher outpatient service payments ($8075, $11 134, and $13 202 more at 6, 12, and 18 months). 26
Limitations
As with all database studies, human error with data input into a complex coding system potentially creates opportunities for faulty coding or underreporting. While this may under report actual VTE rates, theoretically these errors would occur at equal rates in both cohorts studied. It is also possible that our elevation parameters, which we based on prior non-spine-related studies, 7,8,27 may not adequately identify if altitude was a risk factor for this cohort and other elevations would instead show a risk. Additionally, there is an inability to screen patients preoperatively based on our methods, and so preexisting DVTs or PEs may not have been excluded. Similarly, we are unable to determine if certain patients moved between studied elevation groups both prior to surgery or post operatively. For example, we could not account for patients that normally reside in a one of the two studied elevation and returned there shortly after the surgery that was actually in the other elevation group (as in travel tourism).
Additionally, because of the nature of this work as an insurance database study, we were also unable to account for operative times and postoperative complications such as incidental durotomies, which would result in a prolonged hospital stay and an increased risk of VTEs; however, we would expect durotomies to occur at equal rates. This study assumes that discharged patients will remain at this similar altitude for the 90 days postoperatively, but we do not have data to confirm this reasonable assumption. As discussed above, VTE prophylaxis in the postoperative period is controversial and variable for spine surgeons and we were unable to compare any discrepancies in our cohorts that may bias one group. Furthermore, we were unable to account for potential increased screening or physician awareness that potential occurs in higher elevation spine practices.
Conclusion
While we are not proposing changes to chemoprophylaxis protocols from the data reported in this study, it is feasible to consider high altitude as a risk factor for PEs following lumbar fusions and should be a variable in risk stratification. Other orthopedic procedures have demonstrated higher VTE rates based on altitude, and posterior lumbar fusions performed at higher altitudes specifically demonstrated an increased rate of postoperative PEs within the first 90 days. Future studies with uniform diagnostic guidelines and anticoagulation protocols should compare spine procedures performed at various altitudes to further investigate the correlation between elevation and VTEs following lumbar fusions.
Supplemental Material
Supplemental Material, GSJ828349_suppl_mat - High Altitude Is an Independent Risk Factor for Developing a Pulmonary Embolism, but Not a Deep Vein Thrombosis Following a 1- to 2-Level Lumbar Fusion
Supplemental Material, GSJ828349_suppl_mat for High Altitude Is an Independent Risk Factor for Developing a Pulmonary Embolism, but Not a Deep Vein Thrombosis Following a 1- to 2-Level Lumbar Fusion by Chester J. Donnally, Ajit M. Vakharia, Jonathan I. Sheu, Rushabh M. Vakharia, Dhanur Damodar, Kartik Shenoy and Joseph P. Gjolaj in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.