
Abstract
Study Design
Retrospective chart review.
Objectives
Lumbar interbody fusion (LIF) can be achieved with various techniques. Evidence supporting the long-term clinical advantages of one technique over another are inconclusive. The purpose of this study was to (1) determine the changes in sagittal parameters in the preoperative, intraoperative, and post-operative phase, (2) evaluate the radiographic maintenance of these parameters over time, and (3) compare the demographics and patient reported outcomes of patients undergoing various LIF techniques.
Methods
We performed a retrospective chart review of patients with degenerative spine disease undergoing single level anterior (ALIF), lateral (LLIF), posterior (PLIF), or transforaminal (TLIF) lumbar interbody fusion. Data collected included patient demographics and diagnosis at time of surgery. Upright lumbar radiographs taken pre-operatively, intra-operatively, and post-operatively were measured for lumbar lordosis (LL), segmental lordosis (SL), posterior disc height (PDH), and foraminal height (FH).
Results
194 patients in a single center were included. PDH and FH increased intra-operatively following ALIF (P < .0001), PLIF (P < .0001), LLIF (P < .0001), and TLIF (P < .0001). SL also increased intra-operatively for ALIF (P = .002) and LLIF (P = .0007). Compared to intra-operative radiographs, PDH and FH decreased at latest post-operative phase for ALIF (P < .03), LLIF (P < .003), TLIF (P < .001), and PLIF (P < .005). SL decreased for ALIF (P = .0008), and TLIF (P = .02). LL did not change postoperatively across techniques. Patient reported outcomes improved post-surgically and disability index decreased, but neither differed between techniques.
Conclusion
LIF, regardless of technique, was shown to provide significant radiographic changes in PDH and FH. Techniques utilizing larger intervertebral cage sizes (ALIF/LLIF) improved SL. Single level LIF did not affect overall LL. No single technique displayed superior radiographic robustness over time.
Introduction
Lumbar interbody fusion (LIF) technique is a popular and effective procedure for the treatment of numerous pathologies of the lower back, such as infection, trauma, neoplasia, as well as degenerative disc pathologies. 1 The goals of LIF surgeries include fusing vertebral levels for dynamic instability, improving spinal fusion rates, restoring alignment, and decompression of neural elements. Over time, different technical approaches to achieve LIF have been developed.
Past studies suggest there is large variability among LIF techniques, each with its own advantages and disadvantages. 2 While anterior lumbar interbody fusion (ALIF) affords the opportunity to utilize a larger cage type and greater fusion rates, its approach is more complicated often necessitating vascular surgery assistance and is often limited to correcting L4-5 and L5-S1 levels. 3 Posterior lumbar interbody fusion (PLIF), affords excellent visualization and decompression, allowing surgeons to directly manipulate the dura and neural elements, however this approach may cause iatrogenic durotomies and poses challenges for restoring lordosis given the relatively smaller cage sizes.4,5 Transforaminal lumbar interbody fusion (TLIF) is another posteriorly based approach which obviates some of the risks of PLIF while allowing for a larger cage sizes.4,5 Lateral lumbar interbody fusion (LLIF) can be used from T12 to L5 and is another option for degenerative and deformity corrections by allowing for large interbody cages, however its approach risks damage to the lumbar plexus, psoas muscle, peritoneum, and ureter.4,6
Given the breadth of options, no standardized surgical approach has been determined, differences in long-term radiographic outcomes remain unclear, and clinical outcomes of LIF remain variable.
The purpose of this study was to (1) evaluate the changes in sagittal radiographic parameters in the preoperative, intra-operative, and at the latest post-operative period, (2) to evaluate the maintenance of these parameters over time, and (3) compare the demographics and patient reported outcome measures of patients undergoing various LIF techniques.
Materials and Methods
Patient Selection
After receiving institutional review board exemption, a retrospective chart review was performed at a large rural integrated health care system. Patients who had undergone single level ALIF, PLIF, LLIF, or TLIF from January 1, 2007 to December 31, 2022 were identified using the following current procedural terminology (CPT) codes 22533, 22630, 22633, 22558. Our inclusion criteria were as follows: patients greater than or equal to 18-year-old diagnosed with degenerative disease of the spine undergoing single level LIF treated by either an orthopaedic spine surgeon or neurosurgeon. Patients were excluded from analysis for the following reasons: non-degenerative diagnoses, inadequate radiographs (including lack of pre-operative, intra-operative, or follow-up imaging), multilevel and revision surgery, and postoperative follow-up less than 1 month. For each patient, we collected information on the level of lumbar fusion, diagnosis, intervertebral body cage type, and type of lumbar fusion. Furthermore, patient demographics such as age, gender, and body mass index (BMI) at time of surgery were collected via manual chart review. Informed consent was not obtained due to the nature of the study in accordance with IRB exempt status.
Radiographic Analysis
Upright lateral lumbar radiographs taken pre-, intra-, and post-operatively were analyzed. Each image was measured to determine lumbar lordosis (LL), segmental lordosis (SL), posterior disc height (PDH), and foraminal height (FH) (Figure 1). LL was measured as the angle from the superior aspect of L1 to the superior aspect of S1. SL was measured as the angle from the inferior aspect of the upper vertebrae fused to the superior portion of the lower vertebrae, ex. inferior border to L3 to superior border of L4 in an L3-4 fusion. PDH was the distance between fused vertebrae at the posterior aspect of the intervertebral disc. FH was measured as the maximum vertical height of the intervertebral foramen. Pelvic incidence (PI) was calculated for each patient using the sum of the sacral slope and pelvic tilt, as previously described. All measurements were performed using the hospital’s picture archiving and communication system (PACS). Chart review and measurements were divided among 3 independent raters. Discrepancies in measurements were confirmed with fellowship-trained spine surgeons to ensure accuracy. If the field of view of the radiograph prevented the appropriate measurement of 1 parameter, for example LL, that measure was omitted. The change (Δ) in a patient’s radiographic measurements was calculated as both an absolute difference and a percent change over the following intervals: preoperative to last follow-up, preoperative to intraoperative, and intraoperative to latest follow-up. Radiographic measurements. Schematic demonstrating measurements taken on upright lateral lumbar x-rays. All segment level measures (SL, FH, PDH) were taken at the spinal level operated on, but are separated in the image for illustrative purposes.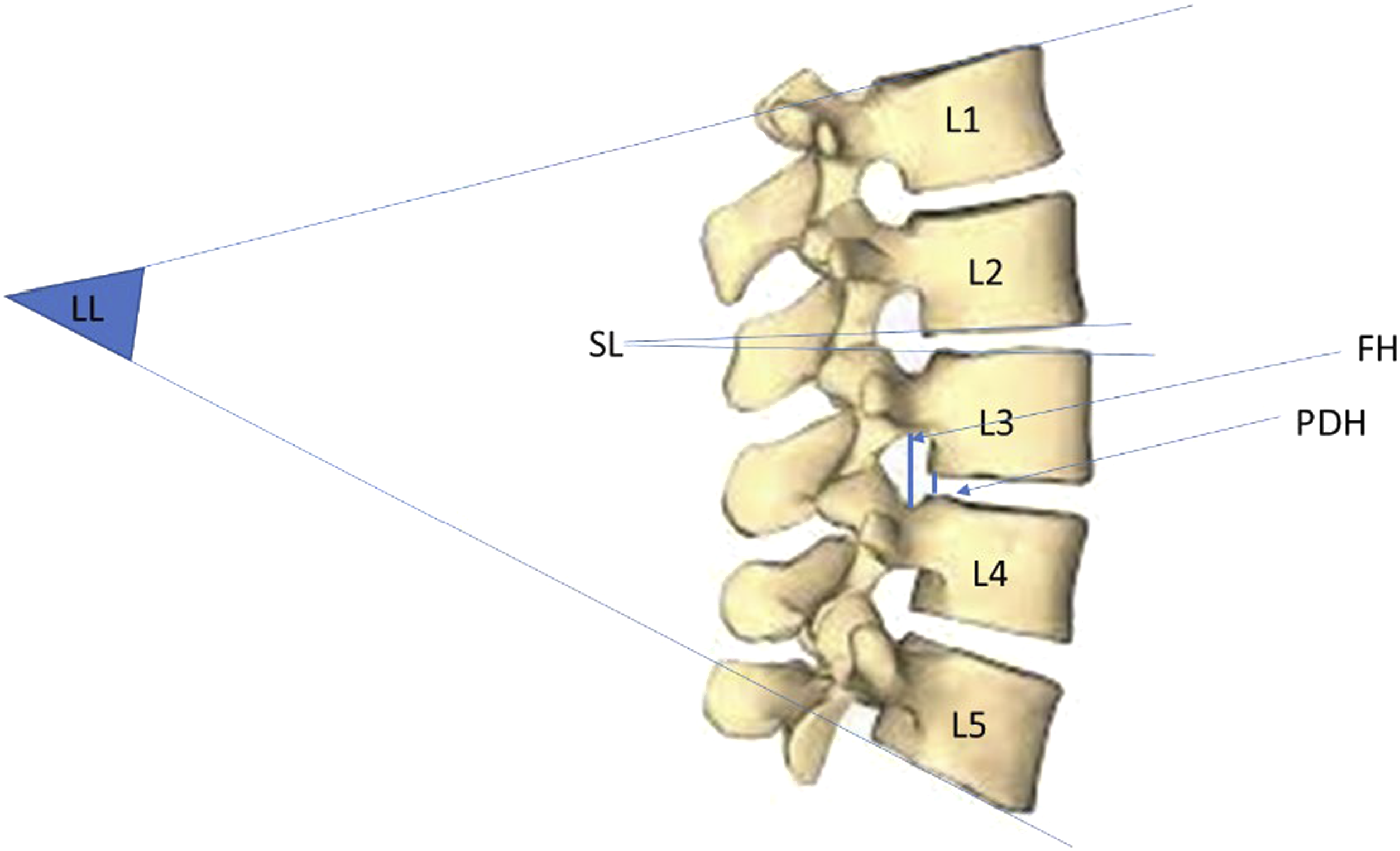
Patient Reported Outcome Measures
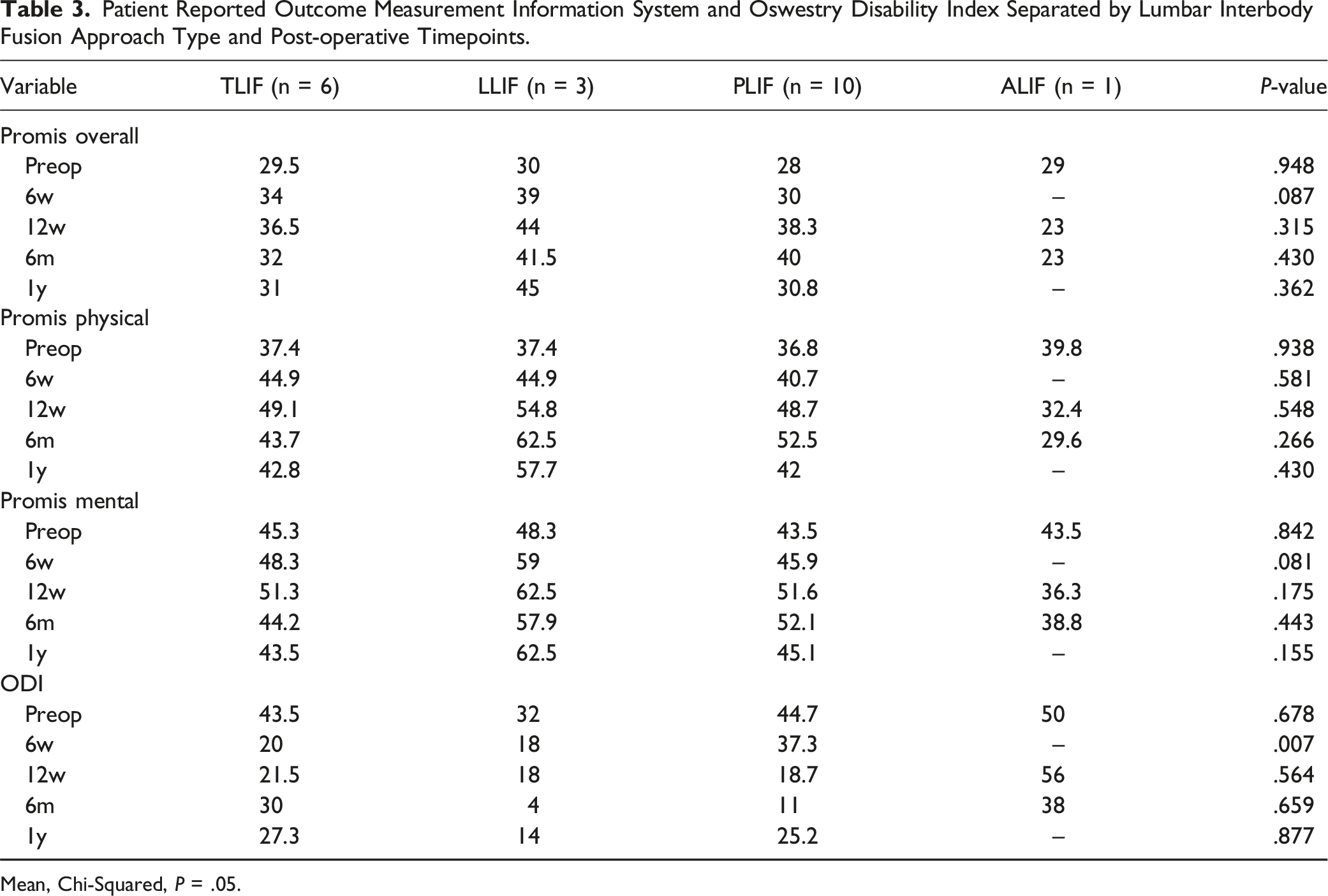
Where available, patient reported outcome measurement information systems scores were collected preoperatively and 6-week, 12-week, 6 months, and 1 year post-operatively. They were collected in the domains of global physical score, global mental score, overall score. In addition, Oswestry Disability Index (ODI) scores were also collected at the same time periods. As most patients did not have this data collected (n = 20), patient reported outcome measures were analyzed separately.
Statistical Analysis
Statistical analysis was performed using SPSS v25 (IBM Corporation, Armonk, NY). A one-way ANOVA was used for continuous variables, while chi-squared was used for categorical data. A post-hoc test using either Tukey’s Honest Significant Difference test (when equal variances are assumed, based on Levine’s test) or Games-Howell test (when equal variances were not assumed) was used to identify where the exact differences between the groups were. Differences between radiographic parameters across timepoints were analyzed with student’s t test. Significance was set at P ≤ .05.
Results
A total of 194 patients met inclusion criteria consisting of 28 ALIFs, 51 PLIFs, 19 LLIFs, and 96 TLIFs. Average follow-up time for ALIF was 23.6 months, PLIF 24.1 months, LLIF 11.2 months, and TLIF 10.4 months. All LIF techniques increased radiographic parameters measured at the time of surgery. Following ALIF, PDH, FH, and SL increased significantly (ΔPDH = +5.3 mm ΔFH = +4.4 mm P < .0001, ΔSL = +5.0°, P = .002). Similarly, LLIF resulted in significant increases in PDH, FH, and SL (ΔPDH = +4.5 mm ΔFH = +4.1 mm P < .0001, ΔSL = +3.3°, P = .0007). Both TLIF and PLIF increased PDH and FH at the time of surgery (TLIF ΔPDH = +3.4 mm ΔFH = +3.5 mm P < .0001; PLIF ΔPDH = +4.5 mm ΔFH = +4.0 mm P < .0001) (Figure 2). Changes in radiographic parameters after lumbar interbody fusion. (A) Lumbar lordosis. (B) Segmental Lordosis. (C) Posterior Disc Height. (D) Foraminal Height. Data plotted as mean ± SD. Paired t test, *P < .05.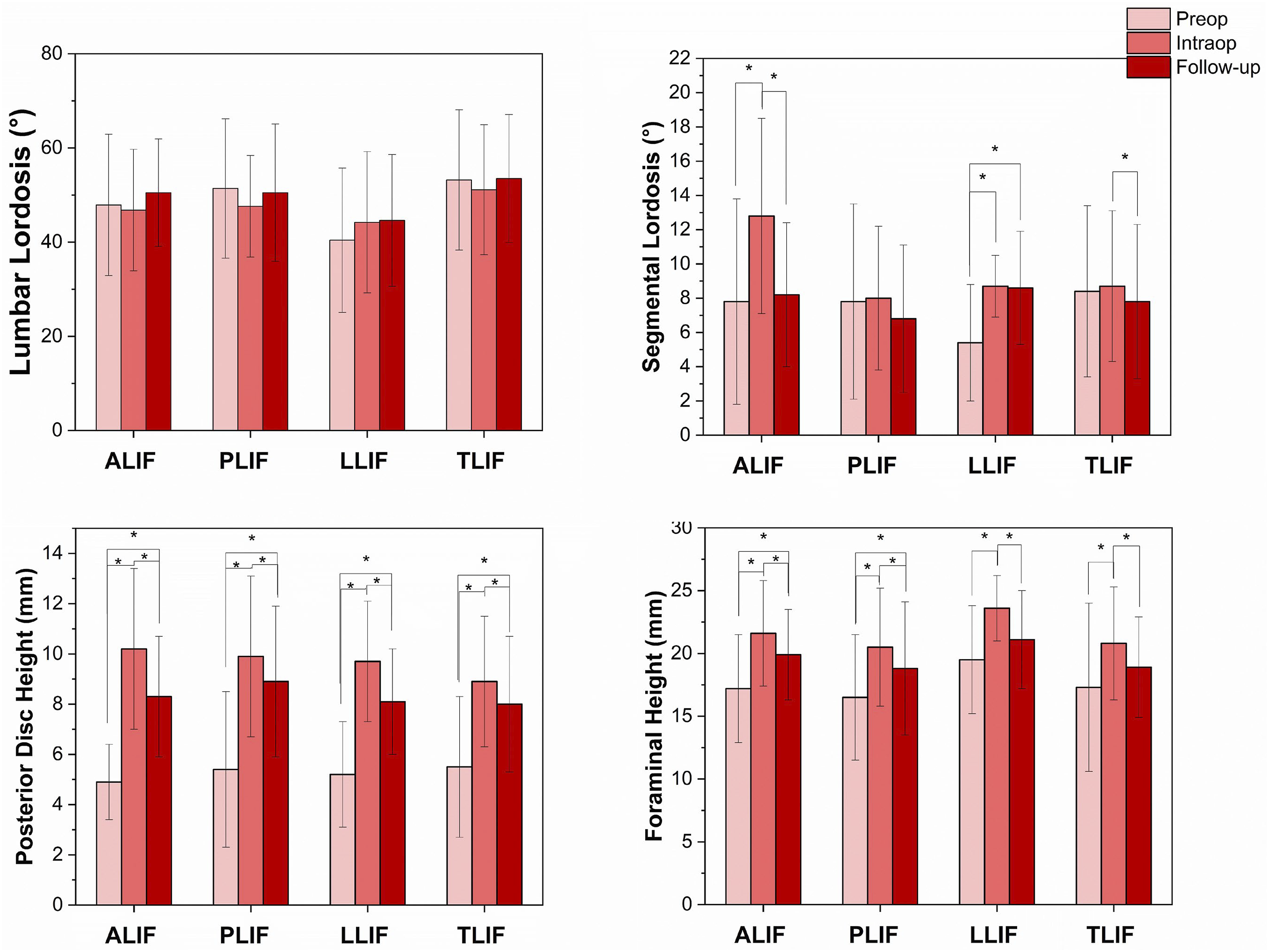
Compared to immediately after surgery, PDH and FH decreased at the latest follow-up for ALIF (ΔPDH = −1.9 mm P = .002, ΔFH = −1.7 mm P = .03), LLIF (ΔPDH = −1.6 mm ΔFH = −2.5 mm P < .003), TLIF (ΔPDH = −0.9 mm ΔFH = −1.9 mm P < .001), and PLIF (ΔPDH = −1.0 mm ΔFH = −1.7 mm P < .005) (Figure 2). SL decreased for ALIF (ΔSL = −4.6°, P = .0008), and TLIF (ΔSL = −.9°, P = .02) (Figure 2). LL did not change at any time point postoperatively across techniques. Accounting for interobserver reliability, no significant differences in the change in radiographic parameters was noted across all techniques at final follow up (P > .05).
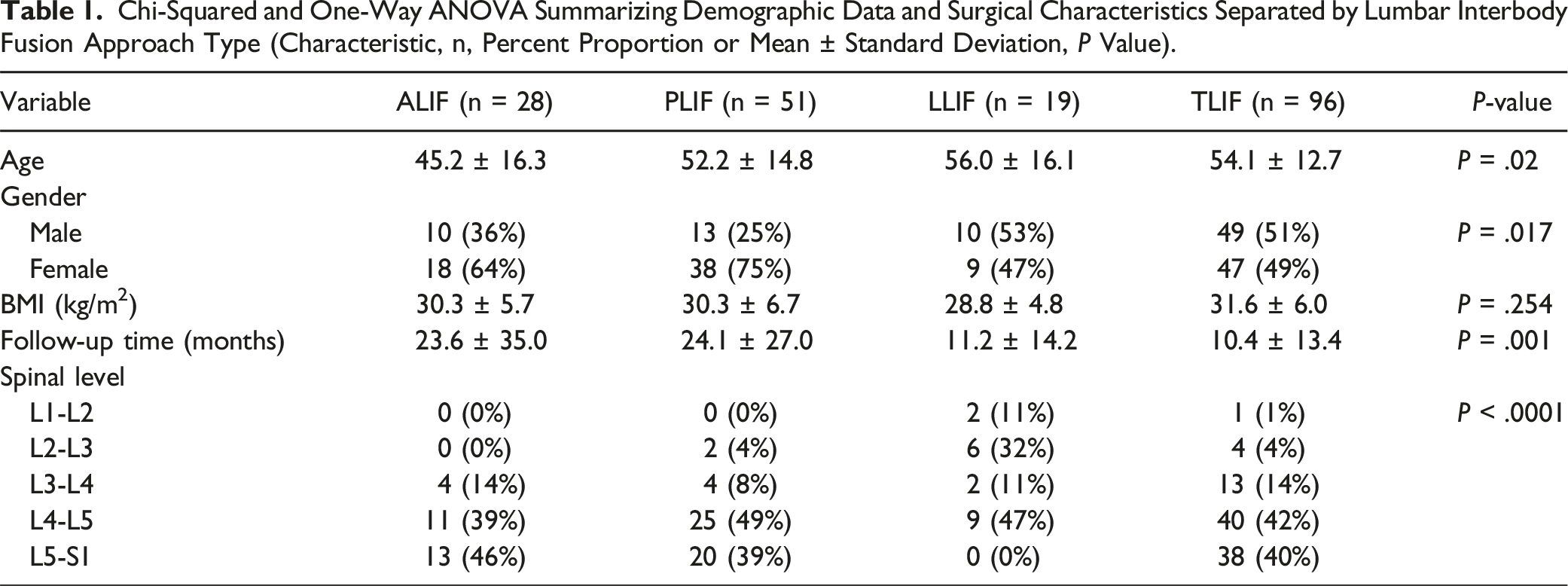
Chi-Squared and One-Way ANOVA Summarizing Demographic Data and Surgical Characteristics Separated by Lumbar Interbody Fusion Approach Type (Characteristic, n, Percent Proportion or Mean ± Standard Deviation, P Value).
Radiographic Measurements After Lumbar Interbody Fusion at Pre-operative, Intra-operative, and Post-operative Timeframes.
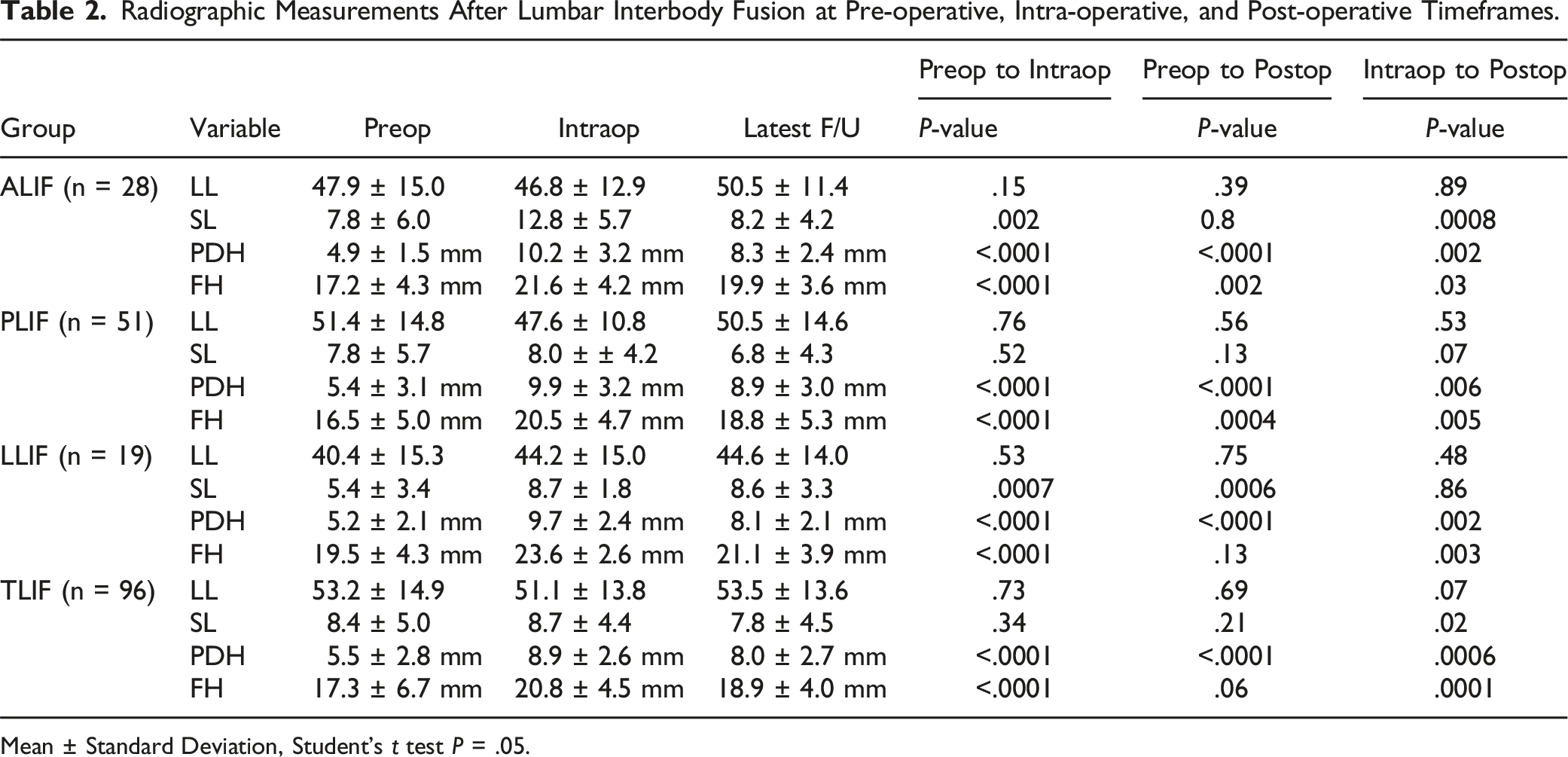
Mean ± Standard Deviation, Student’s t test P = .05.
Patient Reported Outcome Measurement Information System and Oswestry Disability Index Separated by Lumbar Interbody Fusion Approach Type and Post-operative Timepoints.
Mean, Chi-Squared, P = .05.
Discussion
We examined the differences in maintenance and correction of sagittal parameters across pre-, intra-, and post-operative periods among LIF techniques. While there are studies that have examined the radiographic differences between 2 fusion approaches, ex. PLIF vs TLIF,6-8 and 4 fusion approaches,2,9,10 to our knowledge, others have not compared the outcomes of all 4 techniques up to 24 months post-operatively and across a 15-year period. Additionally, our patient population is primarily rural, providing some insight into a less frequently studied group. The results of our study suggest that while there are differences in maintenance and degree of correction among techniques, overall, no single LIF technique has a definitive advantage over another in this modality.
We found that techniques that can utilize a larger intervertebral cage, as in the case of ALIF and LLIF, significantly increased SL, while PLIF and TLIF did not. These findings suggest LIF techniques should be tailored to specific patient pathologies. For example, patients who would benefit from increases in SL should receive ALIF/LLIF. Work by O’Connor et al 10 demonstrated similar results, finding that ALIF/LLIF caused a greater increase in SL than PLIF/TLIF. In contrast to our study, their study only examined radiographic parameters at 6 months post operatively, which may not capture the settling/subsidence that we were able to capture with longer follow-up. Taken together, ALIF and LLIF appear to be superior in changing SL.
One practical implication of our study is that changes in pre-, intra-, and post-operative x-ray parameters may be linked to clinical outcomes after surgery.11,12 At the intra-operative period, each LIF technique provided significant radiographic changes in PDH and FH, but no technique changed overall LL. These findings are in line with those found in the meta-analysis by Teng et al. 9 This may be due to inclusion of single level LIF patients, whose single level correction in SL may not be reflected in the more global LL.13,14
Our study found that compared to pre-operative scores, 2-year postoperative PROMIS scores trended upwards and ODI scores trended downwards for all LIF techniques. These trends suggest that in general lumbar fusion surgery improves patients’ clinical outcomes. However, scores did not differ between groups, suggesting that for the subset of patients examined, no specific LIF technique resulted in superior patient reported outcomes. Still, caution should be used in interpreting these results as only a small portion of our patients had recorded patient reported outcome measures.
Over time, all LIF techniques demonstrated a degree of loss of correction and radiographic settling. This is evidenced by the decrease in values for all techniques. It should be noted that there was no statistical difference between the techniques. The radiographic settling may be caused by multiple factors, including intervertebral cage subsidence, endplate remodeling during the fusion process, osteolysis, and pseudoarthrosis.
Regarding patient demographics, ALIF tended to be the option for younger individuals. This may be due in part to the necessity of operating through the abdomen in ALIF. Operating through the abdomen in elderly individuals raises the risk of encountering unwanted vascular adhesions and vascular retraction, which may explain the decreased age with ALIF. It should be noted however that age alone does not increase the risk of complications in patients undergoing ALIF. 15 However, conditions such as COPD and attributes such as frailty that are associated with age have been shown to be correlated with poor outcomes and increased complications with ALIF surgery.16-18 Although complications related to performing a surgery through the abdomen aren’t correlated with age, subsidence in ALIF is. 19 This correlation between age-related conditions and ALIF complications as well as age with subsidence may explain the younger age in ALIF patients, but further research should be done as other studies have found that there is no correlation between age and surgery approach, at least when comparing ALIF to TLIF. 20 Interestingly, Ye et al 21 compared various clinical outcomes after LIF and found that LLIF/PLIF/TLIF had shorter hospital stays and reduced digestive system complications than ALIF when controlling for age, comorbid conditions, gender, and race. Importantly their study excluded primary fusions. In contrast, Katz et al 22 found that PLIF/TLIF had increased rates of operative time, transfusion, UTI, stroke, and morbidity than ALIF/LLIF. Literature is therefore conflicted regarding which LIF techniques impact clinical outcomes more.
Overtime, Oezel et al 23 demonstrated that patients receiving LIF operations are older, and outcomes are improving in terms of morbidity, length of stay, and blood loss. Although ALIF/LLIF patients had greater improvements, overall improvements in surgical technique and post-operative management appear to account for the changes overtime. Our study data was collected over a 15-year period, capturing both time periods studied in Oezel et al which may help to explain the demographic differences seen in our cohort.
As expected, we also noted significant differences in the spinal levels operated on depending on the approach type. This is due to the limitations of each approach. In LLIF, access to L5/S1 is limited given the position of the lumbosacral plexus, and ALIF is generally limited to the lower lumbar segments given anatomy of the great vessels. 4 In addition, factors such as a patient’s previous surgery, ease of approach, surgeon preference, and individual anatomy likely played a role in spinal level and approach type.
Limitations
The current study is not without limitations. First, due to the retrospective nature of our study design, our data may be prone to selection bias. To this point, we included data across a 15-year study period, which we believe helps limit the potential selection bias of our study. Another limitation of this study was that ALIF and LLIF were not subdivided into standalone LIF vs LIF supplemented with posterior instrumentation. Future studies may wish to investigate the effect of supplementation with posterior instrumentation in LIF to investigate this limitation. In addition, this study primarily examined radiographic findings and a very limited sample of patient reported outcome measures. Further investigations should be performed to increase sample size in analysis of patient reported outcome measures. Our study did not account for heterogenous follow-up times, patient satisfaction, and patient safety metrics such as surgical time, blood loss, and number of incisions. As such, future studies with longer follow-up times are warranted to study the relationship of these parameters to the degree of indirect decompression, as well as its relationship to clinical outcomes. Finally, this study did not specifically address preexisting comorbidities such as osteopenia, osteoporosis, obesity, diabetes, etc. While some of these, namely osteoporosis and obesity, likely play a role in postsurgical outcomes, we did not find that older age or BMI were statistically different between surgical approaches, suggesting they did not play a major role in our results.
Conclusion
Overall, all LIF approaches provided significant changes in PDH and FH. ALIF and LLIF, techniques with the capacity to employ larger interbody cage sizes, also increased SL. Single level LIFs, regardless of approach, did not change overall LL. Despite these differences, no single LIF technique displayed superior radiographic robustness over time. All LIF techniques demonstrated improvement in clinical outcome measures. Surgeon choice of LIF technique should be individualized based on patient specific anatomy, symptoms, surgical goals, and patient expectations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.