
Abstract
Study Design:
A systematic review.
Objective:
The objective of this study was to determine the safety and efficacy of stand-alone anterior lumbar interbody fusion (sa-ALIF) for the treatment of symptomatic isthmic spondylolisthesis of L5-S1 by assessing the level of available clinical and radiographic evidence.
Methods:
A systematic review utilizing Medline, Embase, and Scopus online databases was undertaken. Clinical, radiographic, and adverse outcome data were extracted for the relevant isthmic spondylolisthesis cases with the intention of undertaking a meta-analysis.
Results:
The database search between January 1980 and December 2015 yielded 23 articles that concerned sa-ALIF for isthmic spondylolisthesis of L5-S1. Only in 9 of the 23 articles data could be extracted specific to sa-ALIF for isthmic spondylolisthesis of L5-S1. There was considerable inconsistency in the standards for reporting outcomes of the surgery due to which meta-analysis could not be undertaken, and hence each article was reviewed.
Conclusions:
There was insufficient evidence to support the safety and efficacy of sa-ALIF for the treatment of isthmic spondylolisthesis of L5-S1. Although sa-ALIF is widely documented in the literature, there was insufficient evidence to support its use in treating this specific pathology. The unique pathological and anatomical situation that isthmic spondylolisthesis of L5-S1 presents must be recognized and its treatment with sa-ALIF should be well thought out.
Keywords
Introduction
Spondylolysis commonly occurs in the population, although progression to symptomatic spondylolisthesis is rare. 1,2 Nonoperative treatment is preferential; however, a number of surgical treatment approaches exist should conservative management fail. Anterior lumbar interbody fusion (ALIF) is one such surgery indicated for isthmic spondylolisthesis (IS) and a range of other spinal pathologies. When compared with posterior fusion techniques, ALIF potentially allows for maximum removal of painful degenerated discs, superior interbody column support, superior fusion rates and arrest of spondylolisthesis, restoration of sagittal balance, and restoration of the disc height. 3 -8 ALIF may be undertaken in conjunction with a posterior approach fusion or posterior instrumentation with the aim of reducing the spondylolisthesis. Some studies advocate this circumferential fusion and reduction approach, particularly in cases of high-grade spondylolisthesis, as it stops the progression of kyphosis and improves clinical and radiographic outcomes. 9 -16 Other studies documenting stand-alone ALIF (sa-ALIF) have reported comparable results to circumferential fusion with the potential benefit of shorter operating times and sparing of posterior muscle damage. 4,5,7,9,17 -22 The latter may be helpful in preventing accelerated adjacent segment degeneration after spinal fusion. 23
Of late sa-ALIF has become a prevalent treatment approach for symptomatic IS of L5-S1. However, the literature reports cases of mixed primary pathology, level of fusion, and variations of ALIF often in combination with posterior instrumentation. 6,20,24 -36 While there is much literature on fusion of L5-S1 for IS, the bulk of the literature focuses on posterolateral fusion (PLF). In 2006, a review of 29 IS fusion studies identified only 3 studies concerning stand-alone L5-S1 ALIF. 25 -28
Despite the use of sa-ALIF for isthmic spondylolisthesis of L5-S1, there is no systematic review supporting its use for this indication. With the loss of posterior tension band and wedged disc shape, isthmic spondylolisthesis of L5-S1 presents a unique biomechanical environment compared to other pathologies treated with sa-ALIF. Keeping these factors in mind, a systematic review of the available literature was undertaken with the intention to perform a meta-analysis.
Methods
Article Search
A systematic review of literature was undertaken following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. 37 Medline, Embase and Scopus online databases were searched for journal articles in English from January 1980 to December 2015. Only journal articles concerning clinical and radiographic studies were considered. The search strategy, as presented schematically in Figure 1, was intentionally designed to be highly sensitive and of low specificity to ensure that no potentially relevant article was excluded on the basis of poor keyword assignment or regional variations in terminology and spelling.
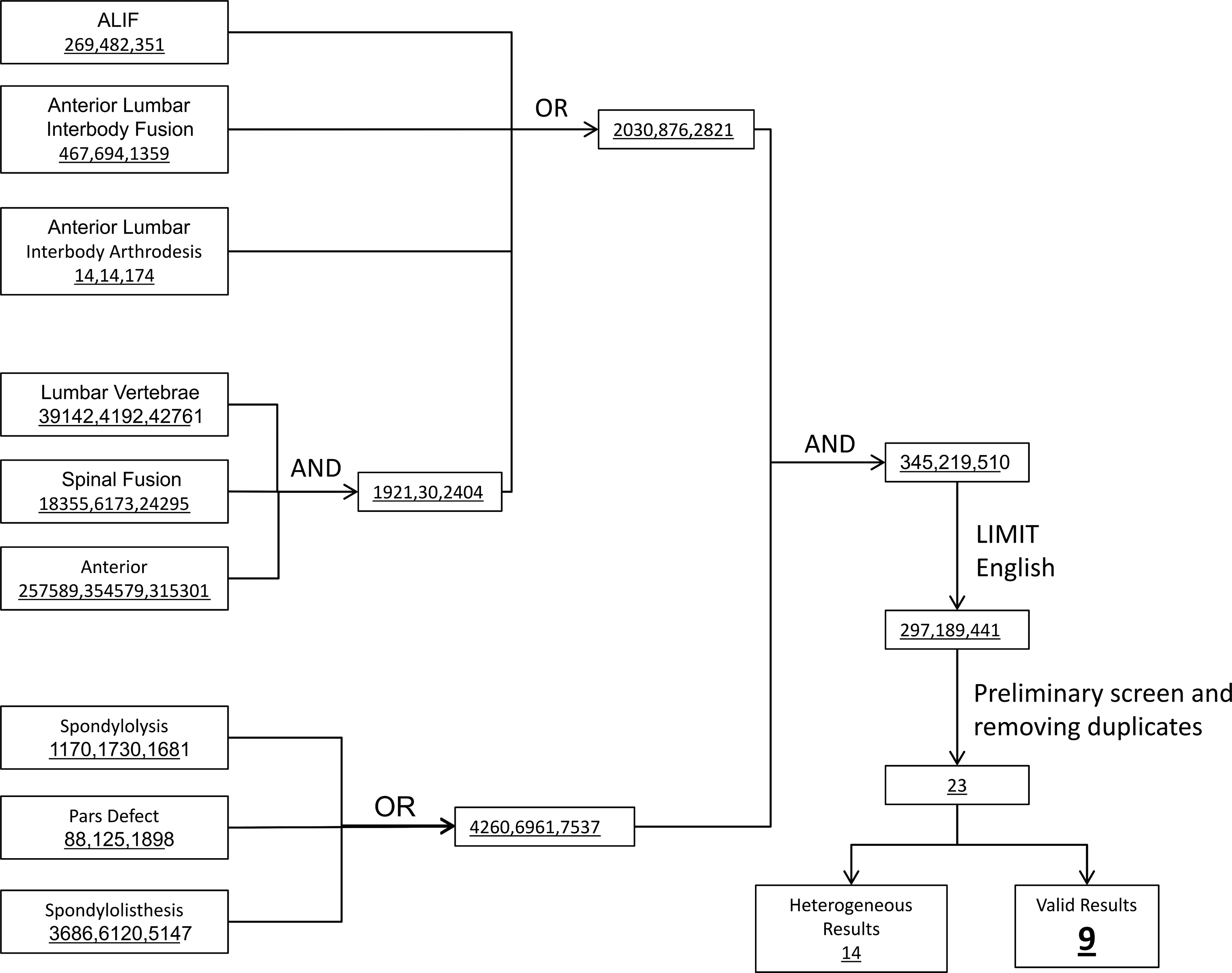
Search strategy used for online article search. Number of articles returned in the order Medline, Embase, and Scopus. “AND” and “OR” represent Boolean operators.
The initial screening process identified 23 potentially suitable articles that reported patient outcomes for sa-ALIF for IS of L5-S1. Stand-alone ALIF was defined as fusion of a purely anterior approach which employed interbody cages with or without anterior plating. These 23 articles included mixed cohorts if appropriate patients were identified in the methodology.
Tabulation of Study Variables
The relevant studies were classified according to a number of criteria including study format, patient populations, and surgical variations, as presented in Supplemental Table S1 (available in the online version of the article).
Regarding study format, articles were classified as prospective (n = 2) or retrospective studies (n = 21). Articles that did not specify were assumed to be retrospective. Articles were classified as having short (<2 years, n = 4), mid (2-6 years, n = 8), or long term (>6 years, n = 11) follow-up periods. There was a clear division between articles with respect to the age of patient at surgery. Articles could either be classified as dealing with juveniles (mean age <16 years, n = 7) or adults (mean age >34 years, n = 16). There was likewise a clear division between those concerning low-grade (Meyerding Grades 0-II, n = 12) and high-grade (Grades III-V, n = 7) spondylolisthesis. Four articles failed to specify grade. All articles describing results with high-grade spondylolisthesis comprised juvenile patients only, while all low-grade spondylolisthesis studies comprised adult patients only.
With regard to surgical technique, the approach was recorded as either retroperitoneal (n = 11), transperitoneal (n = 6), or not specified (n = 6). Although surgical descriptions were not always detailed, the interbody graft type and any anterior instrumentation were recorded. Furthermore, if an article presented multiple cohorts receiving other fusion surgeries the alternative fusions were recorded.
Identification of Study Outcomes
Preoperative, postoperative, and follow-up outcomes were extracted for the 23 identified articles. Outcomes were divided into 5 main categories, namely, complications, clinical outcomes, radiographic outcomes, surgical measures, and functional/physical exam, as indicated in Table 1.
Indication of the Reporting Outcomes Presented and the Frequency With Which Each Was Reported Among the 23 Articles.
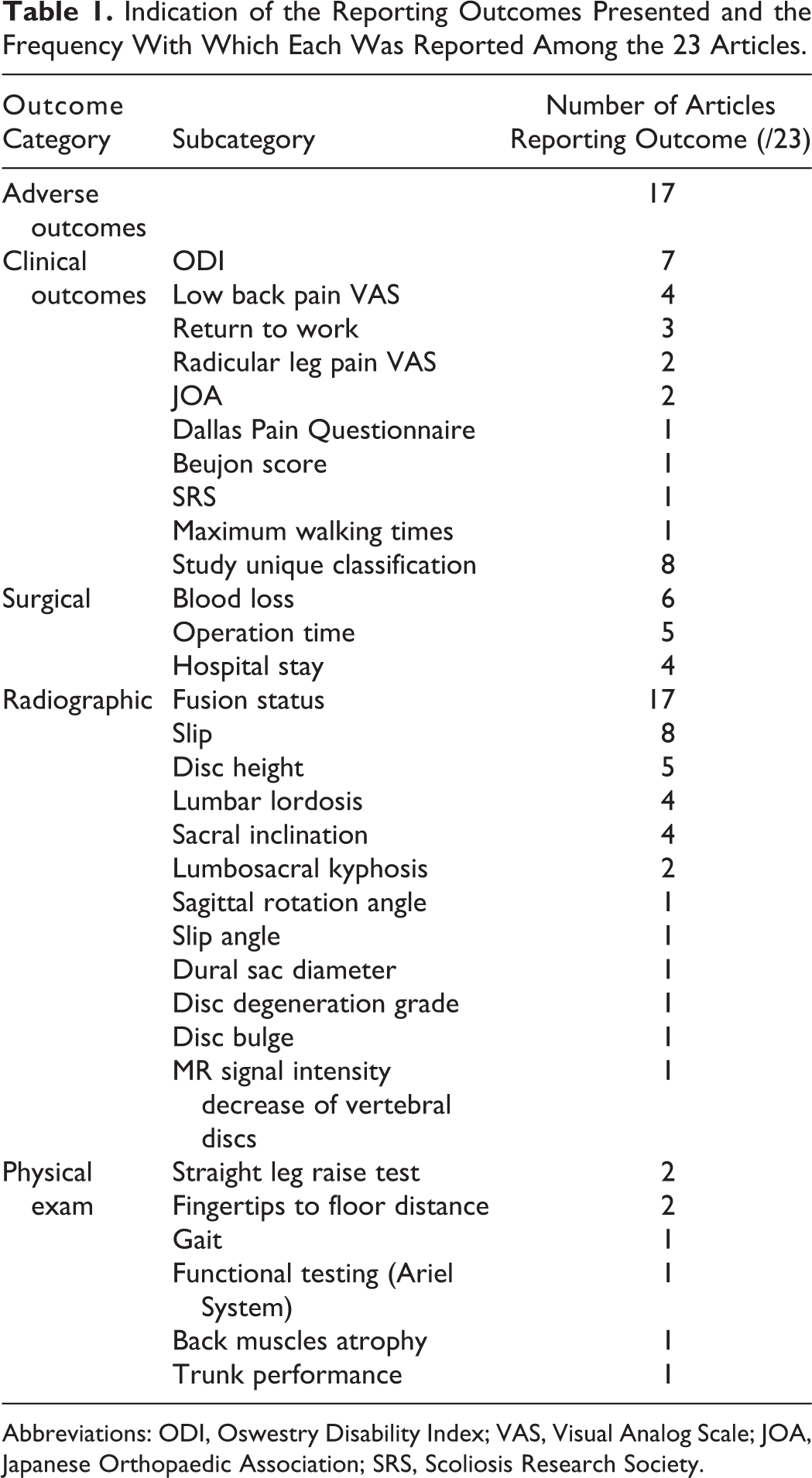
Abbreviations: ODI, Oswestry Disability Index; VAS, Visual Analog Scale; JOA, Japanese Orthopaedic Association; SRS, Scoliosis Research Society.
Fusion status and adverse events were reported by 17 articles. For the purposes of this review, adverse events were further classified as perioperative, early, late/persistent, and reoperation. Early complications were classified as resolving spontaneously or through conservative approaches or requiring surgical intervention in less than 9 months after the first surgery. Late/persistent complications included those continuing or first presenting greater than 9 months after surgery. If a perioperative, early, or late/persistent complication required surgical intervention, it was classified as a reoperation accordingly. As such, some complications such as retrograde ejaculation (RE), pain, and neurological deficits could fall into either category depending on the duration and resolution.
Apart from fusion status and adverse events there were no patient outcome assessments common to more than 8 articles. In excess of 32 different measures were identified including a number of articles reporting study-specific clinical assessments.
Final Screen: Exclusion of Articles With Heterogeneous Results
Articles with heterogeneous results were excluded. Heterogeneity was defined as studies where sa-ALIF for IS of L5-S1 results could not be isolated from those of other surgical procedures, level of fusion, and/or primary pathology. As such, 14 of 23 articles had heterogeneous results and were excluded. 6,20,24,26 -36
Three of the relevant articles reported varying outcomes and conclusions on the same surgical cohort. 10,13,18 As a result, only 6 cohort studies and 1 case report representing 92 surgical cases qualified for the purpose of this review.
Analysis of Study Outcomes
Outcomes reported by each article were highly variable preventing direct comparison and aggregation of results. Reporting standards were incongruous with most studies being retrospective and lacking baseline data.
When taking into account both the limited number of cases and low level of available evidence, meta-analysis could not be undertaken. In its place, an analysis of each qualifying study was undertaken to determine whether there was a general consensus on the safety and efficacy of the procedure.
Results
Aunoble et al (2006)
Aunoble et al 5 presented medium-term follow-up (26.2 months mean) from a prospective study of 20 adult low-grade spondylolisthesis patients. Endoscopic sa-ALIF, which incorporated anterior plating, was undertaken between February 2001 and March 2003.
Ten adverse events were reported, one of which required reoperation. One perioperative complication, injury to the left common iliac vein, was resolved during surgery. Two early wound infections were noted; but no thrombolytic events, RE, or abdominal wall weakness was observed. Hypoesthesia of the lateral cutaneous nerve was noted in 6 patients but only one case continued as a persistent complication. There was one reoperation due to persistent pain and pseudarthrosis due to a propioni bacterium acnes infection. The anterior instrumentation and interbody device were removed and replaced by posterior instrumentation.
Mean Oswestry Disability Index (ODI) score improved from 57% preoperatively to 30% at 6 weeks (P < .0001) and 21% at last follow-up (P < .05 compared with 6-week score). 38 Visual analogue scale (VAS) pain scores for lower back decreased significantly from 6.5 to 2.7. 39 Radicular leg pain VAS scores also decreased from 6.2 to 3.4, but no statistical significance on the decrease was reported. The average time for return to work was 5.5 months; however, 2 patients never returned to work.
Fusion was defined as the absence of a peri-implant lucency surpassing more than 50% of the total implant surface, a translation equal or less than 3 mm, and the absence of implant breakage. There was one case of pseudarthrosis as mentioned earlier. Average slip reduced from 19% preoperatively to 5% postoperatively and was noted as stable with time. Two patients displayed an increase of 13 or more degrees in local lumbar lordosis. This manifested as posterior facet pain which was treated with local corticosteroids and had resolved at last reported follow-up.
Helenius et al (2006), Remes et al (2006), and Lamberg et al (2007)
Helenius et al 10 presented long-term follow-up results (17.2 years mean) from 3 cohorts of adolescent patients with high-grade IS of L5-S1 (mean age at surgery 14.4 years). Surgery was undertaken between 1977 and 1991 with 3 surgical cohorts, namely, sa-ALIF (n = 21), PLF (n = 23), and circumferential fusion (ALIF combined with PLF; n = 26). The 3 surgical cohorts were selected chronologically, representing the evolution of operating strategy, as opposed to random selection. Lamberg et al 18 and Remes et al 13 presented the same cohorts of patients with additional outcome criteria.
Five sa-ALIF patients developed postoperative complications (4 early and 1 late) that required reoperation. One developed peroneal nerve paralysis, which was reoperated on twice. Three underwent decompression for L5 or S1 radicular pain. The late complication was slip progression to spondyloptosis requiring a PLF reoperation. One patient in the PLF cohort had a symptomatic nonunion requiring reoperation. One circumferential patient required prolonged hospitalization for wound infection and one developed scoliosis requiring a further 5 reoperations including circumferential refusion.
Mean ODI, low back pain VAS scores, radicular leg pain VAS scores, and Scoliosis Research Society (SRS) questionnaire scores were presented. 40 There was no baseline preoperative data to allow meaningful comparison. If the ungrounded assumption is made that the preoperative mean scores were not significantly different across the 3 cohorts, then the circumferential scores were better than PLF and sa-ALIF (ODI: P = .045 and P = .051; low back pain VAS: P = .082 and P = .041; SRS: P = .025 and P = .065, all respectively).
A physical exam was undertaken at follow-up to complement the patient questionnaires. Again there was no preoperative data. It was noted that 2 PLF patients and 1 circumferential patient were straight leg test positive (≤60°). There were 3 PLF, 2 sa-ALIF, and 9 circumferential patients with weak or absent unilateral or bilateral patellar or Achilles tendon reflexes. Four PLF patients had diminished S1 dermatome sensation and one had diminished hallux extension strength. Two sa-ALIF patients had nondermatomal sensory deficiencies. Results from spinal mobility and trunk performance tests indicated a significantly greater loss of lumbar flexion associated with the PLF and circumferential cohorts. A significantly higher prevalence of back muscles atrophy was observed in the posterolateral group compared with the anterior fusion group.
Nonunion was defined as a segmental movement ≥3° at fusion levels. Three PLF and 1 circumferential patients displayed nonunion postoperatively. Only 1 nonunion was fully fused at follow up. Progression of slip by ≥10% was found in 4 PLF, 1 sa-ALIF, and 3 circumferential patients. Progression of lumbosacral kyphosis ≥10° occurred in 9 PLF, 3 sa-ALIF, and 3 circumferential patients. Decrease in disc height at L4-L5 was noted for 5 PLF, 7 sa-ALIF, and 1 circumferential patients. Progression of slip was not statistically significant but lumbosacral kyphosis and decrease of disc height were.
Possible bias was identified as technical expertise was gained with time to the advantage of the chronologically later cohorts. Similarly, the validity may have been affected as the mean follow-up for PLF, sa-ALIF, and circumferential were 21.7, 14.0, and 16.3 years, respectively, so the PLF patients were significantly older. When this bias and the lack of preoperative clinical data are taken into account, an objective comparison between cohorts cannot be made.
Muschik et al (1997)
Muschik et al 19 compared medium- and long-term results from 2 adolescent cohorts receiving surgery for high-grade spondylolisthesis between 1987 and 1992. The first cohort received sa-ALIF (n = 29) while the second received ALIF with reduction and posterior instrumentation (n = 30). Surgical option was designated chronologically with the stand-alone technique preceding the reduced. As a result, stand-alone and reduced cohorts had varying average follow-up periods (sa-ALIF 125 months, reduced ALIF 67 months). It was hypothesized that the considerable shorter mean follow-up time for the reduction cohort was not “enough time to develop secondary degenerative changes” of adjacent spinal levels. This temporal bias meant that cohorts could not be objectively compared.
In the stand-alone cohort there were 3 early adverse outcomes and 1 late adverse outcome. The early adverse outcomes were 1 wound infection and 2 cases of self-resolving RE. The long-term adverse outcome was failed fusion requiring reoperation.
The only clinical data presented were the number of patients who were relieved of symptoms, which is subjective and nonreproducible quantitatively. The number of symptom-free patients increased from 6 preoperatively to 20 postoperatively (P < .01) in the sa-ALIF group. A spondylolisthesis of greater than 30° was the indication for prophylactic treatment of asymptomatic patients.
In the sa-ALIF group, there were no significant changes in percentage slip, slipping angle, or sacral inclination postoperatively or at the follow-up, whereas all 3 parameters were significantly improved in the cohort receiving additional posterior instrumentation. Pseudarthrosis was defined as “an observed instability of the segment L5-S1.” One sa-ALIF patient of the 7 patients who displayed pseudarthrosis (14%) was free of symptoms. In comparison, 19 of the 22 patients with solid fusion (86%) were free of symptoms (P < .01). The average time to fusion was 17 ± 10 months in the sa-ALIF group compared to 7 ± 5 months in the posterior instrumentation group. Compared with the clinical outcomes in the sa-ALIF group, the study failed to show any additional benefits in clinical symptoms with the reposition of the slipped vertebra in the posterior instrumentation group.
Tiuasanen et al (1996)
Tiuasanen et al 16 presented retrospective medium-term outcomes of 2 adolescent cohorts with high-grade IS of L5-S1, receiving surgery between 1982 and 1990. There were 11 patients in the sa-ALIF cohort (mean follow-up 4.2 years) and 16 in the circumferential fusion cohort (mean follow-up 5.3 years).
Two sa-ALIF patients (18%) and 2 circumferential patients (13%) had adverse events. One patient from each cohort developed postoperative peroneal weakness and was reoperated on. At follow-up, one patient from each cohort had a sensory disturbance. The mean operating time and blood loss were 35% and 70% less for the sa-ALIF cohort (155 minutes and 538 mL) when compared with the circumferential cohort (242 minutes and 1706 mL).
A 20.6% (sa-ALIF cohort) and 16.3% (circumferential cohort) increase in postoperative mean Japanese Orthopaedic Association (JOA) disability scores was reported; however, there was no significant difference between the cohorts. 41 ODI scores and the results of functional testing were reported at follow-up but no baseline data was recorded.
Nonunion was defined as a segmental movement ≥3° in the flexion/extension radiographs. All patients had solid fusion at follow-up. Preoperative, postoperative, and follow-up mean slip noted no statistical significance between groups or in improvements. For the stand-alone cohort, mean lumbosacral kyphosis was reduced by 17.1° postoperatively but by final follow-up had increased to a value that was not significantly different from the mean preoperative value. A mean reduction of lumbosacral kyphosis of 13.3° postoperatively and 5.8° at follow-up was recorded in the circumferential cohort (P < .001). The authors indicated that a longer follow-up was required to determine if the progression of kyphosis had any clinical impact.
Kim et al (1993)
Kim et al 7 presented short-term (17.6 months mean) clinical and radiographic results for 23 adult patients with low-grade spondylolisthesis (13) and intervertebral disc herniations (10). Patients received sa-ALIF at L5-S1 (n = 4), L4-L5 (n = 17), or multiple levels (n = 2) between July 1985 and February 1989. Demographics and outcomes were tabulated separately for each individual patient. Only 2 cases (patients 2 and 12) were relevant to this review. While the surgical technique was adequately described, no adverse events or the lack thereof were discussed.
Clinical outcomes were reported as excellent, good, fair, or poor according to the authors’ subjective criteria. Patient 2 was excellent at 3 months, good at 1 year, and excellent at 2 years. Patient 12 was excellent at both 3 months and 1 year but lost to follow-up at 2 years.
Fusion rates were calculated from periodic computed tomography but no definition or method of rate calculation was provided. The time of fusion for patient 2 was 24 months, while patient 12 was fused at 6 months. Postoperative changes in dural sac diameter and disc bulge were determined from computed tomography. Patients 2 and 12 exhibited a 1.0 mm and 0.5 mm increase of AP dural sac diameter, respectively; decrease of 0.2 mm and no change of lateral dural sac diameter, respectively; and a 0.8 mm and 2.2 mm decrease of disc bulge, respectively. In absence of data on any adverse outcomes, safety of the surgery could not be determined. Furthermore, the efficacy of results was difficult to determine due to the subjective nature of clinical appraisal.
Sevastikoglou et al (1980)
Long-term retrospective results (2-14 years) for 10 adolescent patients with high-grade spondylolisthesis of L5-S1 were reported. 22 Demographic data and results were tabulated for each patient allowing 6 relevant cases of sa-ALIF for IS of L5-S1 to be identified. There were no perioperative or early complications. It was noted that at the final follow-up, all patients were free from complaints, which may imply there were no late complications.
Clinical outcomes were determined by comparing pre- and postoperative symptoms and physical exam findings. Preoperatively 5 patients had an abnormal gait of which all had improved or were normal at 3-month follow-up, and all were normal at final follow-up. All patients had either unilateral or bilateral sciatica preoperatively of which 5 had complete relief at 3-month follow-up. The sixth patient had only partial relief at 3-month follow-up but complete relief at final follow-up. Four patients had back pain preoperatively, all of which were relieved at the final follow-up. Straight leg raise test was positive in all patients preoperatively, of which 3 were negative at final follow-up while the remaining 3 showed improvement.
All patients were defined as having safe fusion at the follow-up, although no definition of “safe fusion” was given. Only preoperative degree of slip was reported, and no appreciable reduction of spondylolisthesis was seen in radiographs as a result of preoperative traction.
Phan and Mobbs (2015)
Phan and Mobbs 42 presented a case report of a 72-year-old man who underwent sa-ALIF at L5-S1 for Grade 1 isthmic spondylolisthesis with predominant bilateral L5 radiculopathy. On postoperative day 9, the patient experienced a sudden onset of severe low back pain and reoccurrence of original radiculopathy. Computed tomography scan revealed a fracture through the sacral promontory with significant anterior listhesis of L5 on S1 and pullout of the inferior S1 screw. An urgent revision surgery was performed to place percutaneous pedicle screws and restore the initial correction of spondylolisthesis.
Discussion
To the best of our knowledge, this is the first review undertaken to isolate results specifically pertaining to sa-ALIF for IS of L5-S1. From a biomechanical standpoint, anterior and circumferential fusion approaches are considered superior over posterior or PLF in stopping the progression of severe spondylolisthesis or lumbosacral kyphosis, as the posterior fusion mass cannot withstand tension alone. 16,43,44 Circumferential fusion is a more extensive process with a significantly greater intraoperative blood loss and longer operation time, but allows for the repositioning of the slipped vertebra and arrests the progression of lumbosacral kyphosis. Stand-alone ALIF avoids posterior muscle damage and epidural fibrosis, allows for the maximum removal of the disc, and restoration of sagittal alignment (some inadvertent reduction in vertebral slippage might occur due to the lordotic position of the patient on operating table), but insufficient initial stability provided through the cage may lead to pseudarthrosis.
Clinical Outcomes
Clinical outcomes relate to disability (ie, ODI, JOA scores, etc), pain (ie, VAS scores, analgesia use, etc), and a patient’s global health (ie, Short Form-36 [SF-36], quality-adjusted life years, etc). For a study to comprehensively measure clinical outcomes, at least one metric from each of these 3 categories should be included in clinical reporting. None of the articles reviewed achieved this. Wide variations in outcomes reported as indicated in Table 1 demonstrates poor consistency in reporting. Even when articles reported using the same outcome measures, poor reporting standards meant much data was invalid. ODI was the most commonly reported clinical outcome (6 of 9 reviewed articles); however, only 1 study presented preoperative baseline data, 5 reflecting that only 1 article was undertaken prospectively (mean ODI score decreased from 57% preoperative to 21% at final follow-up; mean VAS back pain improved from 6.5 to 2.7). Therefore, for any meaningful comparison across different clinical studies, standardization of clinical outcomes reporting is strongly recommended with prospective documentation of preoperative status.
Data on adverse events was reported for 5 of the 6 surgical cohorts and a case report representing 90 patients (Table 2). Rate of adverse events across all cohorts was 24% (22 of 90 patients), with a range of 0% to 100% (a case report) between cohorts. Reoperation rate across all cohorts was 11% (10 of 90 patients), with a range of 0% to 100%. The wide variation in rates could partly be attributed to the variation in follow-up periods across different studies. Out of the 10 reoperations 3 were performed for L5 or S1 radicular pain, 2 for pseudarthrosis, 2 for peroneal nerve weakness, 1 each for sacral fracture, deep wound infection, and spondyloptosis.
Adverse Events for All the Relevant Surgical Cohorts and the Case Report. More Incidents of Early Complications (<9 Months Postsurgery) Were Reported Compared With Perioperative or Late Complications.
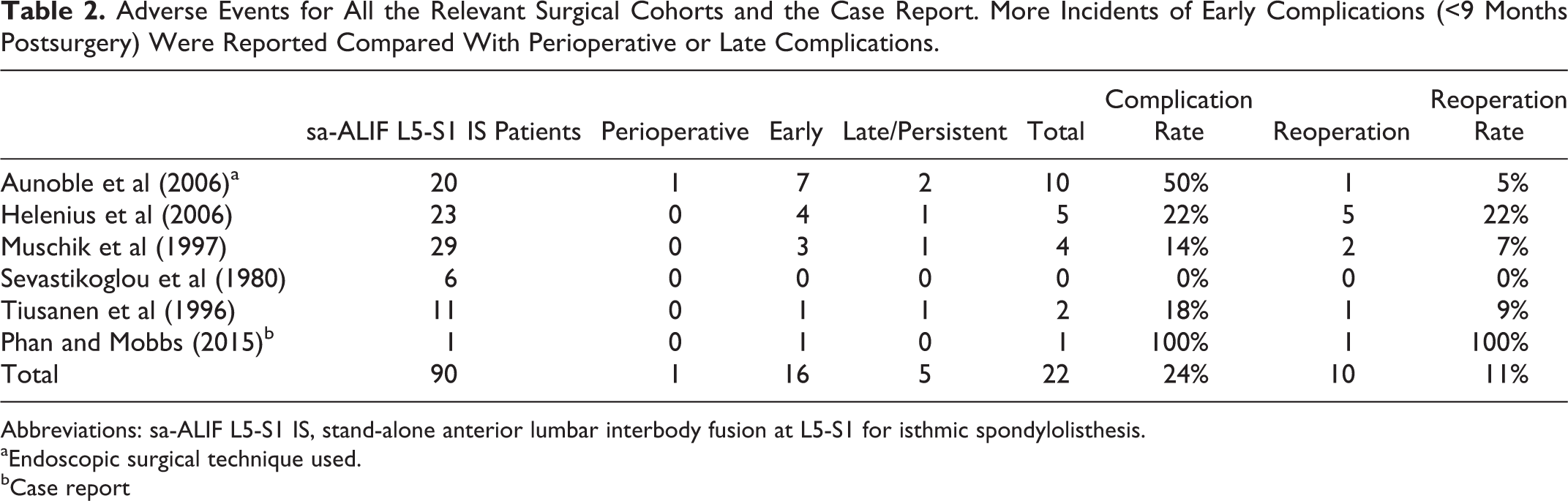
Abbreviations: sa-ALIF L5-S1 IS, stand-alone anterior lumbar interbody fusion at L5-S1 for isthmic spondylolisthesis.
aEndoscopic surgical technique used.
bCase report
Radiographic Outcomes
Radiographic results were determined from comparing preoperative, postoperative, and follow-up imaging. Twenty of the 23 originally identified articles reported preoperative grade of spondylolisthesis. Nineteen reported cohorts were of either solely low-grade or solely high-grade spondylolisthesis. All low-grade spondylolisthesis articles were cohorts of adult patients (n = 13), while all high-grade spondylolisthesis articles were cohorts of adolescent patients (n = 7). This clear distinction between adult low-grade spondylolisthesis and adolescent high-grade spondylolisthesis suggests distinct pathological processes exist between age groups. High-grade spondylolisthesis most commonly develops in adolescents with congenitally weak or dysplastic pars interarticularis. 45,46 This occurs particularly when the posterior arch is not completely ossified and the intervertebral disc is still very elastic. 45 -47 On the other hand, low-grade spondylolisthesis is more common in adults, where degenerative changes make the intervertebral disc less compliant and hence less prone to large degrees of slippage. Further investigation into the difference in response to surgery between these 2 conditions is required and future reporting needs to clearly make this differentiation.
Most commonly reported radiographic measurements were fusion rates and reduction in slip (Table 3). Whether or not any correlation between these parameters and clinical outcomes exists is still controversial. 48 -51 Whether or not a correlation exists could not be determined in this study because only 9 of the 92 cases were tabulated in a way which allowed statistical analysis. In this review, fusion rates were reported by 6 of the 9 articles; however, there were 3 different radiographic definitions for fusion and 2 articles gave no definition. 7,22 Eight cases of pseudarthrosis were reported in total, of which 6 were asymptomatic and 2 required reoperation.
Radiographic Outcomes for All the Relevant Surgical Cohorts. The Difference Between Preoperative Slip and Slip at the Final Follow-up Was Not Significant in Any of the Studies.
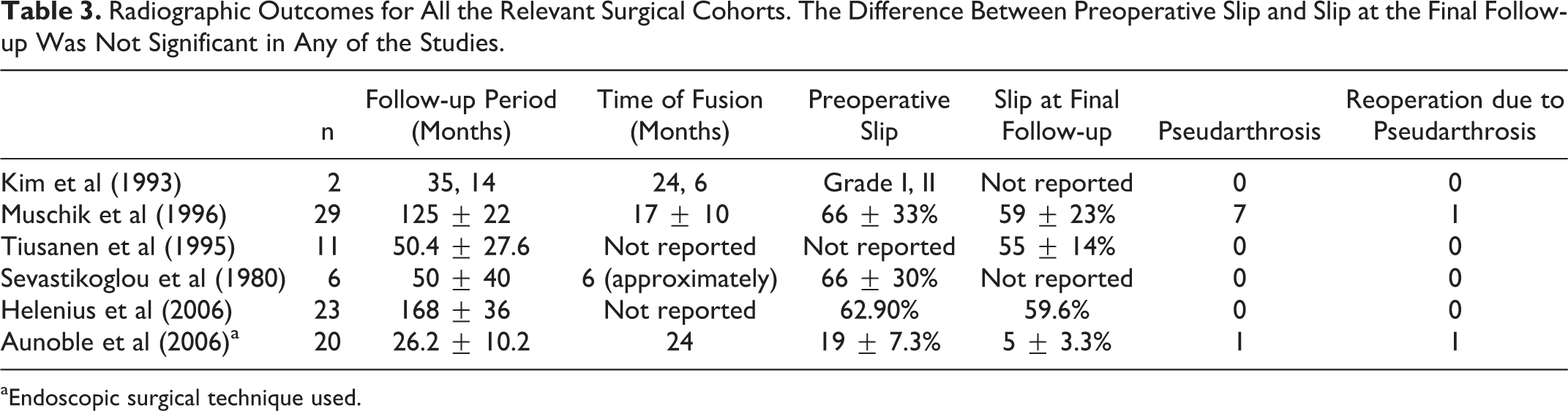
aEndoscopic surgical technique used.
Only 2 articles reviewed tabulated demographic and outcome data for each patient. 7,22 Tabulation of individual cases allows relevant data to be extracted regardless of the mix of a cohort. Most case series for lumbar fusion are relatively small (mean n = 68 for 23 articles), so individual tabulation is feasible and as such the authors recommend this method of reporting. Three trials (reported by 5 articles) compared sa-ALIF with other lumbar fusion techniques. 10,13,16,18,19 Two of these trials assigned patients to surgeries in a temporal fashion and hence any comparisons are biased. 10,13,18,19 Surgeons increase their technical skill over time and as such the chronologically later cohorts receive an unfair advantage. Furthermore, follow-up was undertaken at the same point in time for all cohorts such that chronologically earlier cohorts had longer follow-up periods. Hence, the chronologically later cohorts with shorter follow-up were advantaged because degenerative changes that affect clinical outcomes develop only over extended periods of time. The authors recommend that studies comparing surgical techniques select cohorts randomly and ensure clinical and radiographic follow-up is undertaken at uniform times.
There was insufficient evidence to support the safety and efficacy of sa-ALIF for the treatment of isthmic spondylolisthesis of L5-S1. The resection of the anterior longitudinal ligament and loss of posterior tension band at this level may allow surgeons to inadvertently overdistract L5-S1 interbody space, and as such authors recommend that if sa-ALIF is performed, the choice of interbody cage dimensions should be based on the physiological height of the disc.
Conclusions
A systematic review of the literature was undertaken to determine the safety and efficacy of sa-ALIF performed for isthmic spondylolisthesis of L5-S1. Although sa-ALIF is widely documented in the literature, there was insufficient evidence to support its use in treating this specific pathology. The unique pathological and anatomical situation that isthmic spondylolisthesis of L5-S1 presents must be recognized and its treatment with sa-ALIF should be well thought out.
Footnotes
Acknowledgements
The authors would like to thank Dr Wayne Viglione and Dr Suzanne Ollerenshaw for their constructive critical feedback, which greatly improved this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an International Postgraduate Research Scholarship from the Australian government—Department of Industry, Innovation, Science, Research and Tertiary Education and University of New South Wales to UC. The authors gratefully acknowledge an internal research grant from Spine Service, which further supported this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.