
Abstract
Study Design:
Prospective, nonrandomized, clinical study.
Objective:
Epidural steroid injections (ESIs) are an important diagnostic and treatment modality for spine pathology. The success of these injections has been attributed to the anatomic location reached by the injectate. This study evaluates injectate dispersal patterns after cervical interlaminar ESI using magnetic resonance imaging (MRI).
Methods:
Patients between the ages of 18 and 85 years with cervical radiculopathy were identified. After obtaining consent for study participation, a gadolinium-enhanced cervical ESI was administered via an interlaminar approach under fluoroscopic guidance. Study participants underwent a cervical spine MRI within 15 minutes of administering the injection. Craniocaudal dispersal and the presence or absence of circumferential dispersal was assessed.
Results:
The injectate dispersed a mean of 8.11 cm in the cranial direction, 6.63 cm in the caudal direction, and 360° circumferentially. No adverse events related to the ESI were reported.
Conclusions:
Fluoroscopy-guided cervical interlaminar ESI resulted in nearly uniform circumferential dispersal within the epidural space with multilevel migration in the cranial and caudal directions. MRI is a safe and accurate tool to evaluate spinal injectate dispersal.
Introduction
Epidural steroid injections (ESIs) are an important diagnostic and treatment modality for spine pathology, most notably radiculopathy. ESI can provide pain relief and functional improvement, especially for patients who are refractory to, or cannot tolerate, oral medications. 1 -3 The success of these injections has been attributed to the anatomic location reached by the injectate. 4 Both the diagnostic and therapeutic applications for ESI assume that the injectate remains in close proximity to the injection site to achieve its intended benefits.
A better understanding of cervical ESI injectate dispersal is paramount to understanding the clinical utility of these injections. Fluoroscopy has been the traditional imaging modality to evaluate injectate dispersal. 5 -8 These “epidurograms” visualize the injectate dispersal in 2-dimensions at the time of the injection. Combining anteroposterior and lateral views can be helpful to overcome the limitation of a 2-dimensional view. However, the inherent quality of fluoroscopic images restricts the ability to accurately assess the injectate dispersal.
Evaluation of lumbar spine ESI with computed tomography (CT) revealed extensive dispersion throughout the epidural space in the lumbar spine. The CT scans were performed 15 minutes after the injection procedure, possibly allowing additional time for the injectate to disperse to additional anatomic structures. 9 Considering the radiation exposure with both fluoroscopy and CT, and the superior image quality with magnetic resonance imaging (MRI), we propose a novel method for evaluating cervical ESI dispersal using MRI.
The purpose of the current study was to evaluate the injectate dispersal pattern after cervical interlaminar ESI using MRI. To the authors’ knowledge, there have been no studies evaluating spinal injectate dispersal using MRI.
Materials and Methods
With approval from our institutional review board, study candidates were recruited from the spine clinics at the authors’ institution from March 2015 to February 2016. Major inclusion criteria included adult males, adult females who were surgically sterile or postmenopausal, and cervical radiculopathy diagnosed by the enrolling provider. Major exclusion criteria included allergy to the injectate, contraindications to having an MRI, and renal disease. Severity of cervical spine pathology was not an exclusion criterion. Informed consent was obtained from all study participants after the risks, benefits, and alternative treatments were discussed in depth.
A single fellowship-trained musculoskeletal radiologist with extensive experience in administering interlaminar ESIs performed all of the injections. Patients were prepped and draped in the usual sterile manner in the prone position. Local anesthesia with 1% lidocaine was administered to the skin. A 22-gauge Tuohy needle was advanced to the ligamentum flavum at the C7-T1 interval under fluoroscopic guidance. The needle was placed into the posterior epidural space using the loss of resistance technique, after which less than 1 mL of nonanionic, iodinated contrast was injected. A lateral fluoroscopic image was taken to confirm appropriate positioning of the needle. A 10.1-mL mixture containing 2 mL of 10 mg/mL dexamethasone, 8 mL normal saline, and 0.1 mL of gadolinium contrast (Omniscan, GE Healthcare, Little Chalfont, Buckinghamshire, UK) was injected. The needle was removed, and a dressing was applied.
Within 15 minutes of completing the ESI, study participants underwent a cervical spine MRI. T1-weighted sagittal (Figure 1) and axial (Figure 2) images were used to evaluate the postinjection dispersal pattern. A single board-certified radiologist measured the dispersal patterns for axial and circumferential extent using calibrated internal measurement software (PACS System Centricity, GE Healthcare).

Sagittal MRI image showing gadolinium-enhanced contrast dispersion. Cranial epidural extent was at the level of the posterior arch of C1. Caudal epidural extent was to the T5 inferior endplate, which was better viewed on a subsequent sagittal slice.
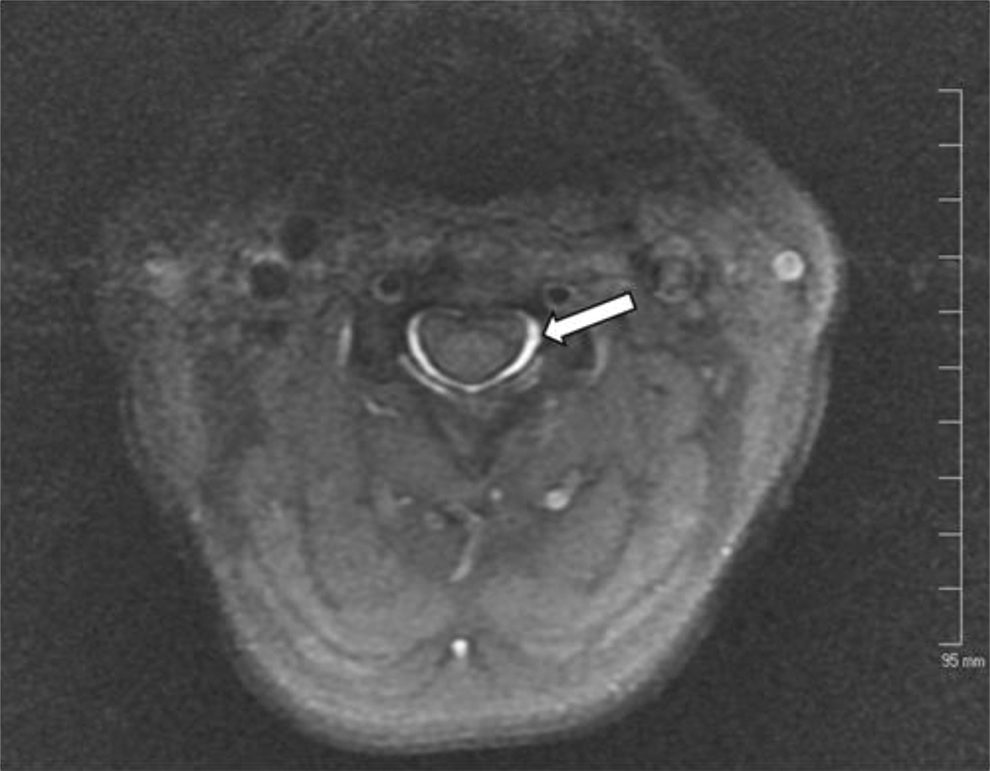
Axial MRI image at the level of the C3 body demonstrating circumferential contrast dispersion. This image is of the same patient in Figure 1.
Statistical analyses were performed using Excel (Microsoft, Redmond, WA) and SigmaPlot (San Jose, CA). Means and standard deviations (SDs) were determined for each outcome measure.
Results
A total of 20 patients with cervical radiculopathy were consented and enrolled in the study. Four patients were not included in the statistical analysis. Two patients withdrew and 2 patients were post–consent screen failures. A total of 16 patients (8 males and 8 females) completed the cervical ESI with gadolinium and subsequent MRI. The mean age of study participants was 51.2 years, with a range of 39 to 64 years. The mean body mass index was 29.2 kg/m2, with a range of 23 to 35 kg/m2.
The caudal extent of injectate dispersal was below the field of view for 5 of the patients. In these subjects, the caudal dispersal measurement is the most inferior measurement on the MRI field of view for statistical purposes. MRI measurements revealed a mean cranial migration of 8.11 cm with a standard deviation of 1.78 cm and a range of 3.3 to 10.7 cm. Mean caudal migration was 6.63 cm with a standard deviation of 3.35 cm and a range of 0 to 10.7 cm. Mean craniocaudal dispersal was at least 14.73 cm with a standard deviation of 3.15 cm and a range of 9.3 to 18.7 cm. This equates to a mean of 8.8 spinal levels from the injection site with a standard deviation of 1.5 levels and range of 6.5 to 12 levels. All 16 patients had circumferential dispersal of the injectate (Table 1). There were no adverse events reported from the injectate or injection procedure.
Gadolinium-Enhanced Injectate Migration Data.
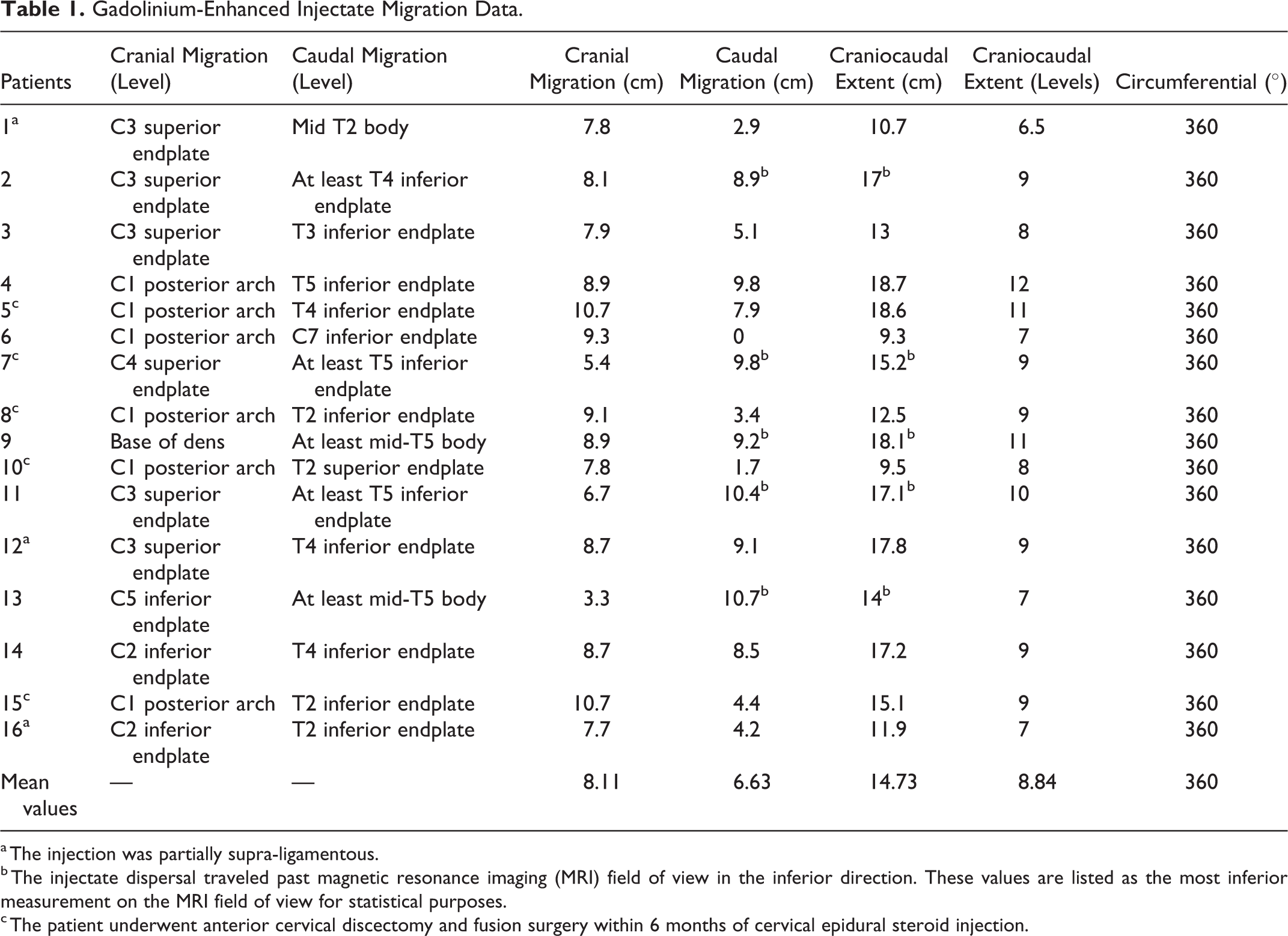
a The injection was partially supra-ligamentous.
b The injectate dispersal traveled past magnetic resonance imaging (MRI) field of view in the inferior direction. These values are listed as the most inferior measurement on the MRI field of view for statistical purposes.
c The patient underwent anterior cervical discectomy and fusion surgery within 6 months of cervical epidural steroid injection.
Discussion
Cervical interlaminar ESI evaluated with MRI demonstrated extensive injectate dispersal throughout the epidural space. Multilevel injectate migration was seen in the cranial and caudal directions, with circumferential spread being observed in all patients. These findings are similar to those reported in previous publications assessing contrast spread after cervical ESI using fluoroscopy. 5,7,10 However, the mean craniocaudal distance of 8.8 levels (14.73 cm) in this investigation was over twice that reported in these studies. Differences in imaging modality used for evaluation and timing of the performance of postinjection imaging are possible explanations for this observed difference.
The timing of evaluation ESI injectate dispersal should be emphasized. The MRI scans in this study were performed approximately 15 minutes after the injection procedure. Paisley et al previously used CT scans 15 minutes after lumbar ESI to evaluate injectate dispersal, which allowed time for the injectate to diffuse throughout the epidural space. 9 Their results, similar to ours, revealed a larger degree of spread in cranial, caudal, and circumferential directions when compared with results from fluoroscopic imaging assessed at the time of injection. 5,7,10 Given the 2 independent variables of method of imaging and time delay, the variable most responsible for the increased injectate dispersal detected cannot be elucidated at this time.
A major question regarding interlaminar cervical ESI centers on anterior contrast spread. Transforaminal ESI have been postulated to be superior to interlaminar ESI in this regard, but the evidence in support of this assumption is considered to be lacking. 11 Every interlaminar cervical ESI in this study demonstrated nearly uniform circumferential injectate dispersion. This is consistent with the report from Kim et al, who observed ventral epidural spread in 93.3% of their cohort of patients following the injection of 3 mL of contrast. 5 Choi et al demonstrated significantly greater anterior epidural spread using a modified interlaminar approach versus a transforaminal approach. 12 Our findings of circumferential spread are in contrast with Goel et al, who reported a 44.6% incidence of ventral epidural spread. 7 All of these referenced articles used fluoroscopy to evaluate injectate dispersal rather than axial imaging, which likely explains the variability in findings.
In this investigation, MRI was found to be a safe and accurate method of evaluating injectate dispersal. No adverse events were reported secondary to the ESI or the injectate itself in this study. To the authors’ knowledge, this is the first study to use MRI to evaluate ESI injectate dispersal. The literature mostly consists of reports using fluoroscopy to assess contrast spread. However, MRI is better able to detect contrast spread in multiple planes that might not be detected with fluoroscopy, and our study demonstrated that adding only 0.1 mL of gadolinium (Omniscan, GE Healthcare) to the injection mixture was sufficient to detect contrast dispersal on MRI. Confirming accurate needle placement using live fluoroscopy, and having an experienced provider familiar with contrast patterns, likely will help reduce the potential rare but serious complications associated with ESI. 13,14
Limitations of this study include the lack of reporting of preinjection and postinjection visual analogue scores for pain. While this data was collected, postinjection scores were not available for all subjects, thus limiting our ability to analyze the data and draw meaningful conclusions from it. In addition, the primary aim of this study was to evaluate injectate dispersal and the role of MRI in assessing the same, not the clinical efficacy of cervical ESIs, which has been frequently reported on in the literature. 15 Another limitation was the relatively small sample size. However, having a larger sample size would unlikely significantly influence the effect size given the consistent patterns of injectate dispersal in our study population. In addition, all study injections were performed by a single fellowship-trained musculoskeletal radiologist who has extensive experience in administering interlaminar ESIs. Therefore, these results might not be generalizable to all practitioners. Finally, this study only assessed the interlaminar approach for cervical ESI. Injectate dispersal for transforaminal and other modified approaches requires further investigation.
Conclusions
Fluoroscopy-guided cervical interlaminar ESI resulted in nearly uniform circumferential dispersal of injectate within the epidural space with multilevel migration in the cranial and caudal directions. A better understanding of spinal injectate dispersion can help guide treatment, especially in patients with multilevel disc disease. This study provides a radiologic rationale for performing C7-T1 ESI for cervical radiculopathy, and has shown MRI to be a safe and accurate tool to evaluate dispersal of cervical ESI injectate.
Footnotes
Authors’ Note
This study was podium presented at the Global Spine Congress in Milan, Italy, May 3 to 6, 2017.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Goldstein is an AOSpine member. The other authors have no conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received research support from the University of Missouri Orthopaedic Association.