
Abstract
Study Design
Retrospective cohort study.
Objective
To investigate the effect of preoperative epidural steroid injection (ESI) on quality outcomes and costs in patients undergoing surgery for cervical degenerative disease.
Methods
We queried the MarketScan database, a national administrative claims dataset, to identify patients who underwent cervical degenerative surgery from 2007 to 2016. Patients under 18 and patients with history of tumor or trauma were excluded. Patients were stratified by ESI use at 3, 6, 12, 18, and 24 or more months preoperative. Propensity score matched controls for these groups were obtained. Baseline demographics, postoperative complications, reoperations, readmissions, and costs were compared via univariate and multivariate analysis.
Results
97 117 patients underwent cervical degenerative surgery, of which 29 963 (30.7%) had ESI use at any time preoperatively. Overall, 90-day complication rate was not significantly different between groups. The ESI cohorts had shorter length of stay, but higher 90-day readmission and reoperation rates. ESI use was associated with higher total payments through the 2-year follow-up period. Among patients who received preoperative ESI, male sex, history of cancer, obesity, PVD, rheumatoid arthritis, nonsmokers, cervical myelopathy, BMP use, anterior approach, 90-day complication, 90-day reoperation, and 90-day readmission were independently associated with increased 90-day total cost.
Conclusion
ESI can offer pain relief in some patients refractory to other conservative management techniques, but those who eventually undergo surgery have greater healthcare resource utilization. Certain characteristics can predispose patients who receive preoperative ESI to incur higher healthcare costs.
Introduction
With the overall aging population of the United States, the number of people managing chronic spinal pain has increased substantially. 1 Many of these patients undergo conservative treatment such as physical therapy, anti-inflammatory medication, or activity restriction prior to surgical intervention. 2 Epidural steroid injection (ESI) is one such nonoperative intervention for management of pain associated with spinal degenerative disease.3-6 While ESI can benefit some chronic spinal pain patients,7,8 a multicenter, prospective comparative study found no difference between ESI and other nonoperative management. 9 Despite questions about its efficacy, ESI has become increasingly common in recent years.4,5 Between 2000 and 2013, the number of Medicare beneficiaries who underwent epidural injections for spine pain increased 7.8% annually. 10
Although conservative management with ESI is increasingly popular, patients who are refractory to such treatment should be considered for surgical intervention.11,12 Indeed, 26% of patients with cervical radiculopathy ultimately undergo surgery for failed conservative management. 13 Given the frequency of ESI in management of degenerative spine disease prior to surgery, previous articles have reported the impact of preoperative ESI on the rates of postoperative complication.14-17 However, data on other outcome measures and costs is lacking, particularly in the context of cervical degenerative disease. As such, in this study, we used a national administrative database to investigate the effect of preoperative ESI on reoperations among patients undergoing surgery for cervical degenerative disease. We secondarily assess rates of complication, readmission, and payments between these groups. We hypothesized that reoperation rates would be higher among patients undergoing preoperative ESI.
Methods
Data Source
This study obtained a sample of the MarketScan Commercial Claims and Encounters database (Truven Health Analytics, Ann Arbor, MI) from January 1, 2007 to December 31, 2016. This database is a collection of commercial inpatient, outpatient, and pharmaceutical claims of more than 75 million employees, retirees, and dependents representing a substantial portion of the U.S. population covered by employer-sponsored insurance. MarketScan contains 53 million patient inpatient records, 40 million with employer-sponsored insurance, 3.7 million with Medicare Part B, and 6.8 million on Medicaid. The MarketScan database contains International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) and 10th revision, Clinical Modification (ICD-10-CM), Current Procedural Terminology (CPT), and Diagnosis Related Group (DRG) codes, as well as National Drug Codes (DEA).
Inclusion Criteria
Patients who underwent surgery for cervical degenerative disease were identified via use of ICD-9 codes. Of these patients, only those who also had a CPT code indicating a cervical surgery were included in this study. ESI was identified by relevant CPT codes up to 3, 6, 12, 18, and 24 or more months prior to the index cervical degenerative surgery. Because multilevel codes would not allow us to control for length of procedure, the cohort was limited to 1- or 2-level procedures. Patients younger than 18 years of age and patients with a history of tumor or trauma were excluded. All codes used can be found in Supplementary Table 1.
Variables and Outcomes
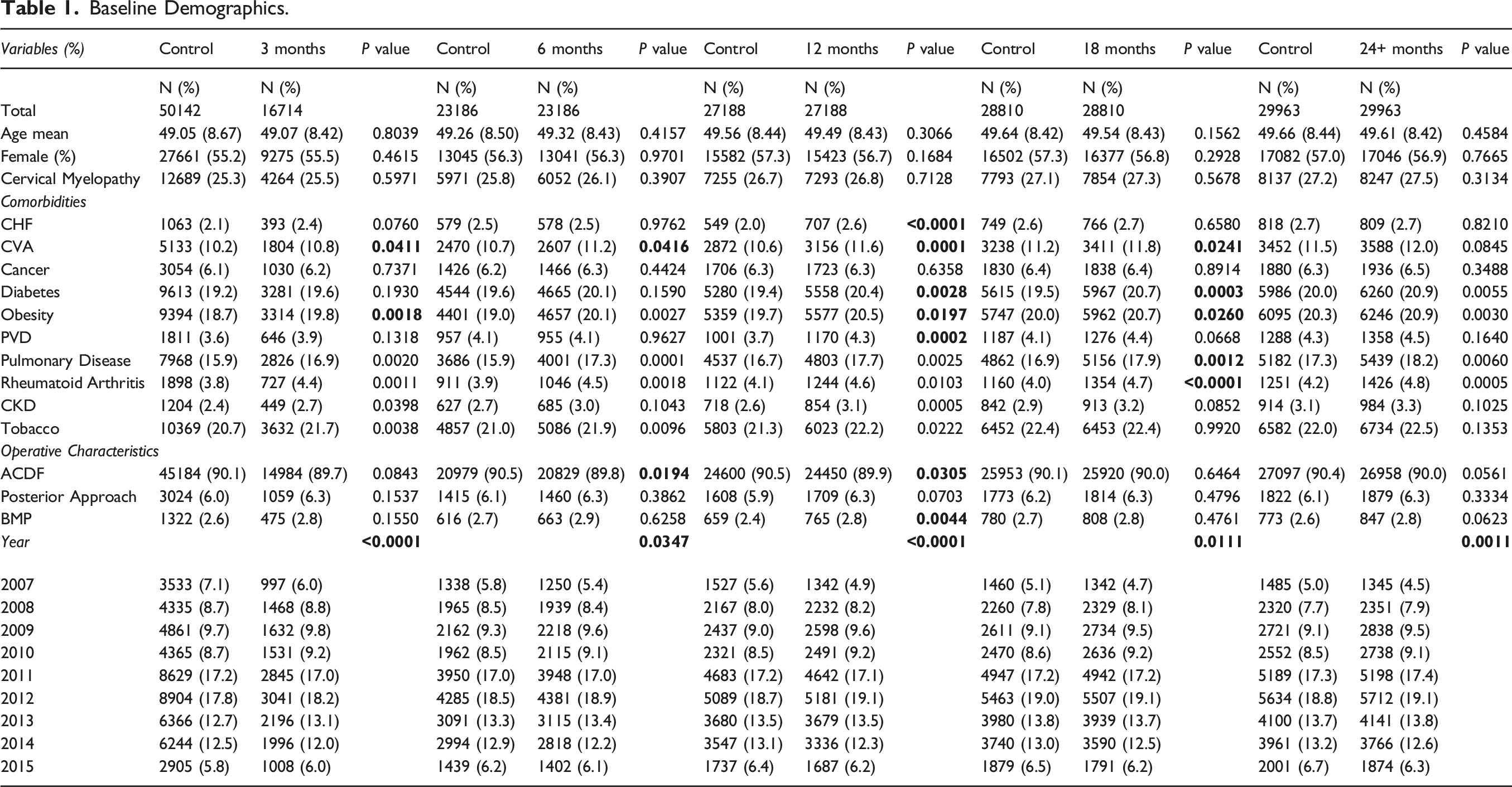
Baseline Demographics.
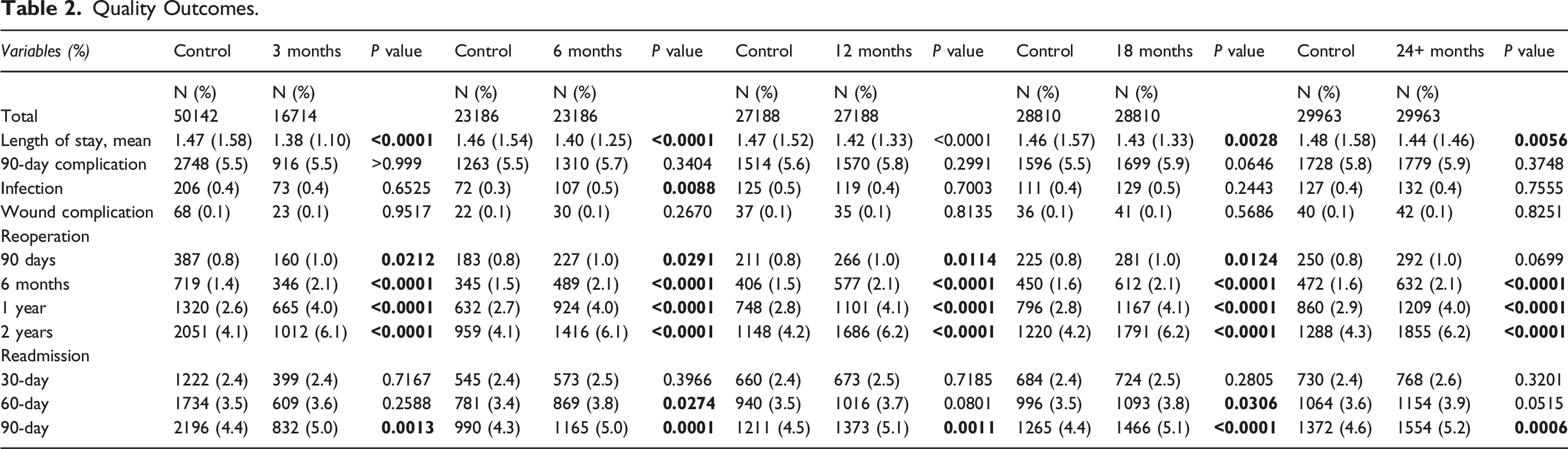
Quality Outcomes.
Payments.

To isolate the impact of the ESI procedure on postoperative outcomes, propensity score matching was conducted. All baseline demographics and comorbidities that were significantly different at baseline were matched between the 2 groups. (Supplementary Table 2) Propensity score matching was performed using R Studio (Boston, MA). Student’s t-test or Mann–Whitney U test and chi-square test were used to compare continuous and categorical variables, respectively. The significance level was defined as a two-sided α < .05. Multivariable logistic and linear regression was used to adjust for the effect of baseline characteristics (Supplementary Tables 3, 4) on outcomes (postoperative complication, reoperation, readmission) and cost, respectively. T-test for slope and ANCOVA were used to test for nonzero slope and difference in slopes, respectively. To identify independent predictors of 90-day cost among patients with preoperative ESI, demographics, comorbidities, and operative characteristics were tested in a multivariable linear regression analysis with backward variable elimination until only those that were significant (P < .05) or trending (P < .1) remained. Statistical analyses after matching were performed using SAS Enterprise Guide (Cary, NC).
Ethical Considerations
All data from these databases are de-identified, and thus, Institutional Review Board approval was waived for this study and was deemed exempt from patient informed consent requirements.
Results
Patient Cohort
97 117 patients underwent surgery for cervical degenerative disease, of which 16 714 (17.2%), 23 186 (23.9%), 27 188 (28.0%), 28 810 (29.7%), and 29 963 (30.9%) had ESI use up to 3, 6, 12, 18, and 24+ months before surgery, respectively (Supplementary Table 2). After propensity score matching, matching cohorts of patients who did not use ESI were obtained. Cohorts were better matched, with some differences in comorbidities (Table 1).
Mean length of stay was significantly lower in the ESI cohort at all timepoints. The overall 90-day postoperative complication rate was not significantly different between groups at all timepoints. Rates of reoperation were higher in the ESI cohort at 6 months, 1 year, and 2 years after the index surgery for all timepoints. Rate of reoperation was also higher at 90 days for all timepoints except the 24+ months group. Rates of readmission were comparable at 30 days, but higher in the ESI cohort at 90 days for all timepoints (Table 2). These findings were consistent after adjusting for differences in baseline characteristics, including year of surgery (Supplementary Table 3).
Median hospital and total payments of the index hospitalization were higher in the ESI cohort at all timepoints. Median total payments were higher at 90 days, 6 months, 1 year, and 2 years after the index hospitalization at all timepoints (Table 3). Total inpatient costs increased significantly over the study period for the control and 24+ month cohorts (P < .0001). There was no significant difference between the growth rate in costs between those 2 cohorts (P = .94) (Figure 1). These findings were consistent after adjusting for differences in baseline characteristics, except for hospital payments at the 3 and 6 month timepoints (Supplementary Table 4). Median total cost of inpatient stay for patients undergoing surgery for cervical degenerative disease with preoperative ESI, 2007-2015. ESI, epidural steroid injection.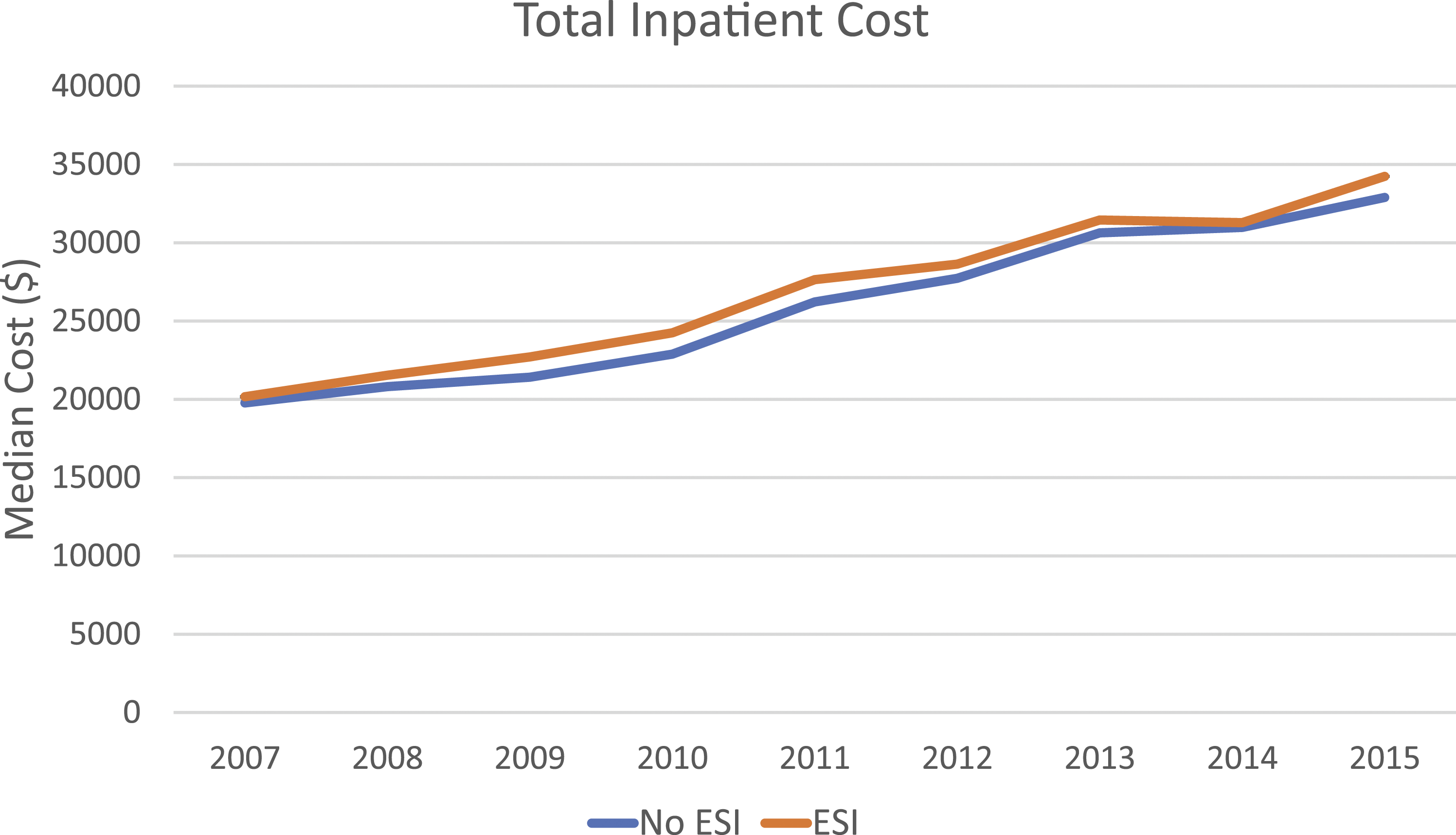
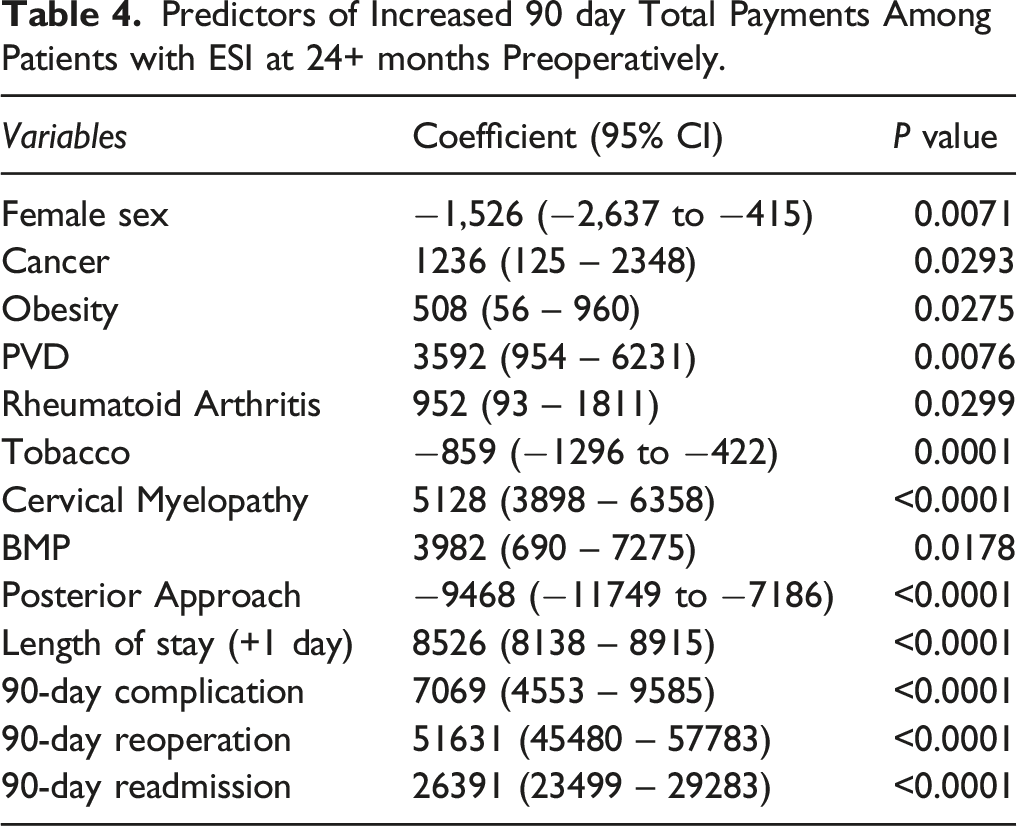
Predictors of Increased 90 day Total Payments Among Patients with ESI at 24+ months Preoperatively.
Discussion
ESI is an intervention used for patients who experience chronic spinal pain without symptom relief from other nonoperative strategies such as physical therapy, opioid medication, or activity restriction.2-5 Although ESI can prevent or delay a need for surgery, patients who do not respond to the treatment are considered for operative management.6,16 As a result, understanding the role of ESI use in postoperative outcomes and costs is extremely relevant to spine surgeons. In this study, we utilized a large national administrative claims dataset to investigate the relationship between these variables. Using propensity score matching, we were able to identify cohorts that were well matched for baseline comorbidities and isolate the results of ESI use. To our knowledge, this study is the first to characterize the effect of preoperative ESI on healthcare utilization and rates of readmission and revision surgery after cervical degenerative surgery.
Certain postoperative complications have been studied in patients who received ESI preoperatively. In a retrospective cohort study on patients with lumbar degenerative disease, Hartveldt et al found that ESI does not increase the risk of postoperative surgical site infection, though longer hospital stay and posterior approach did. 17 Both Yang et al and Zusman et al found no overall increase in complication rate for patients undergoing ESI prior to thoracic or lumbar procedures, but the risk for wound complications was increased.14,15 In cervical degenerative disease, Cancienne and colleagues 16 reported that cervical ESI was associated with increased rate of postoperative infection, if conducted within 6 months of posterior spinal fusion or 3 months of ACDF. Notably, similar to previous studies, our study found no difference in overall complication rates. However, we additionally found no difference in postoperative infection or wound complications, except at the 6 months timepoint, consistent with previous findings (Table 2).
Readmission rates after surgery for cervical degenerative disease have been studied extensively in different patient cohorts. Using the Nationwide Readmissions Database, Rumalla et al reported 30- and 90-day readmission rates of 2.67 and 5.97% for patients undergoing anterior surgery and rates of 5.4 and 10.0% for patients undergoing posterior surgery for cervical degenerative disease, respectively.18,19 Similarly, Schafer and colleagues 20 reported 90-day readmission rates of 5.4 and 12.3% for anterior or posterior approaches in a prospective, multicenter study. The 30-day readmission rate was higher in a Medicare cohort (7.9%) after elective surgery for cervical degenerative disease. 21 The readmission rates in our cohorts fall within this range: 2.4 and 4.3–4.6% at 30 days and 90 days, respectively, in the control groups, and rates of 2.4–2.5 and 5.0–5.2% across all timepoints (Table 3). Previous MarketScan studies from our group have stratified this rate by surgical approach and found similar trends to other studies in the literature.22,23 While there is a statistical difference in the readmission rates, the absolute difference is less than 1%, which may not be as clinically significant. Similarly, while reoperation rates are statistically higher, they fall under the normal limits reported in the literature. Surgeons should be careful in interpreting this data for patient care and hospital system decision-making.
In addition to quality measures, healthcare utilization is of particular importance in management of spine degenerative disease and much work has been done to characterize the cost-effectiveness of ESI.10,24-27 In a retrospective cohort study, Manchikanti et al 24 demonstrated the cost-utility of cervical ESI in patients refractory to previous conservative management. Alvin and colleagues similarly reported that cervical ESI is more cost-effective than other nonoperative treatment modalities in the short-term. 27 However, ESI does not relieve pain symptoms in all patients and in some repeat ESI are undertaken. 28 As a result, as Carreon et al 26 noted in their study of lumbar ESI, for patients who improve, cost per QALY is acceptable, but for those who do not improve, cost per QALY is theoretically infinite. In spite of the many articles on costs of ESI, ours is the first to report that preoperative ESI increases total costs associated with cervical degenerative surgery. This may be partially attributed to the increased length of stay and readmission rate in the ESI cohort, though this effect persists up to 2 years after the index stay, and the difference in mean costs increases across that same timespan (Table 3). It is important to note that this may be due to underlying differences in the 2 cohorts that cannot be adjusted due to the limitations of the claims database, for example, complexity of pathology. Furthermore, we identified multiple medical comorbidities, BMP use, revision surgery, and readmission as independent predictors of 90-day total cost among patients who received preoperative ESI (Table 4).
One limitation of this study is that multilevel procedures were not included, because the codes utilized in the claims dataset prevent any controlling for number of levels involved. MarketScan analyses are also inherently limited by the nature of the data available;29-31 for example, we were unable to control for operative time, estimated blood loss, or disease complexity, which can all affect the rate of postoperative complication. Finally, patients who undergo surgery after ESI generally have greater comorbidities (Supplementary Table 2). However, we attempted to mitigate the effects of these baseline differences using propensity score matching. As such, we believe this study offers useful, novel information on the impact of preoperative ESI on postoperative outcomes and costs of cervical degenerative disease.
Conclusion
ESI can offer pain relief in some patients refractory to other conservative management techniques, but those who eventually undergo surgery have greater healthcare resource utilization. While readmission and reoperations are statistically higher, these differences may not be clinically significant. Spine surgeons should be aware of the potential effects of ESI use when evaluating surgical candidates.
Supplemental Material
sj-pdf-1-gsj-10.1177_21925682211050320 – Supplemental Material for Do Epidural Steroid Injections Affect Outcomes and Costs in Cervical Degenerative Disease? A Retrospective MarketScan Database Analysis
Supplemental Material, sj-pdf-1-gsj-10.1177_21925682211050320 for Do Epidural Steroid Injections Affect Outcomes and Costs in Cervical Degenerative Disease? A Retrospective MarketScan Database Analysis by Harsh Wadhwa, Kunal Varshneya, Martin N. Stienen and Anand Veeravagu in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.