
Abstract
Study Design:
Retrospective cohort study.
Objective:
The objective of this study is to determine how often patients with degenerative cervical myelopathy (DCM) and initially treated with cervical steroid injections (CSI) and to determine whether these injections provide any benefit in delaying ultimate surgical treatment.
Methods:
All patients with a new diagnosis of DCM, without previous cervical spine surgery or steroid injections, were identified in PearlDiver, a large insurance database. Steroid injection and surgery timing was identified using Current Procedural Terminology (CPT) codes. Multivariate logistic regression identified associations with surgical treatment.
Results:
A total of 686 patients with DCM were identified. Pre-surgical cervical spine steroid injections were utilized in 244 patients (35.6%). All patients underwent eventual surgical treatment. Median time from initial DCM diagnosis to surgery was 75.5 days (mean 351.6 days; standard deviation 544.9 days). Cervical steroid injections were associated with higher odds of surgery within 1 year (compared to patients without injections, OR = 1.44, P < .001) and at each examined time point through 5 years (OR = 2.01, P < .001). In multivariate analysis comparing injection types, none of the 3 injection types were associated with decreased odds of surgery within 1 month of diagnosis.
Conclusions:
While cervical steroid injections continue to be commonly performed in patients with DCM, there is an overall increased odds of surgery after any type of cervical injection. Therefore injections should not be used to prevent surgical management of DCM.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) is a broad term for various degenerative conditions of the cervical spine resulting in compression of the cervical spinal cord and eventual neurological dysfunction.1,2 This term encompasses the multiple different etiologies of myelopathy in the cervical spine. 3 For example cervical spondylotic myelopathy (CSM) describes myelopathy resulting from spondylotic changes to cervical spine including disc height loss, ligamentum hypertrophy, uncovertebral hypertrophy, and osteophyte formation. Ossification of the posterior longitudinal ligament (OPLL) is a distinct degenerative process resulting in ossific changes in the posterior longitudinal ligament (PLL) creating anterior mass effect and spinal cord compression. These are in contrast to cervical myelopathy caused my congenital stenosis, or a preexisting idiopathic narrowing of the spinal canal. In the setting of moderate to severe spinal cord compression with progressive neurological symptoms, standard treatment of DCM typically involves surgery,1,4 either in the form of anterior decompression with anterior cervical discectomy and fusion (ACDF) or cervical disc arthroplasty (CDR) or posterior decompression, via multiple different surgical techniques including laminectomy, laminoplasty, and posterior laminectomy and fusion.5-8
Currently, cervical steroid injections (CSIs) are being used for diagnosis and treatment of degenerative spine pathology, including cervical radiculopathy and spondylosis. 9 The purported benefits of this approach include short-term management of spondylotic or radicular symptoms via inhibition of both the inflammatory pathway cascade and afferent nociceptive signaling.10,11 Rarely, however, complications of cervical spine steroid injections may result leading to hematoma or infarction involving the spinal cord. 10
There is currently a lack of any evidence in the literature supporting any utility of CSIs for treatment of DCM. 12 Despite this lack of evidence, and general consensus among surgeons against CSIs, patients often present for surgical consultation after having previously received CSIs for treatment of DCM. This may be due to their effectiveness in radiculopathy and spondylosis cases. Given that CSIs may be targeted to multiple locations, including the epidural space, the transforaminal region, or the zygapophyseal joints, differing injection modalities may also have variable therapeutic effects. The aim of the current study is to determine how often patients with DCM are initially treated with cervical steroid injections (CSI) and to determine whether these injections provide any benefit in delaying ultimate surgical treatment.
Materials and Methods
Institutional Review Board (IRB) Approval was received for this study from the Hospital for Special Surgery Institutional Review Board, study ID# 2019-1127. Patient consent was not required because this study only used publicly available de-identified data.
A retrospective cohort study was conducted of the PearlDiver health insurance patient registry (PearlDiver Inc, Colorado Springs, CO, USA), which included patients treated across the United States between January 2007 through March 2017. This database includes deidentified patient-level insurance claims information across select commercial, Medicaid, and various forms of Medicare health plans. All patients with a new diagnosis of DCM (ICD-10: M47.12, M50.XXX; ICD-9: 721.1, 722.71) without previous cervical spine surgery or steroid injections in the previous 5 years were included. Patients with a concurrent diagnosis of cervical radiculopathy were excluded (ICD-10: M54.12, ICD-9: 723.4) as CSIs are commonly used in this population.
Administration of cervical epidural, transforaminal, or zygapophyseal steroid injections was determined based on their associated Current Procedural Terminology (CPT) codes (62 310, 62 311, 62 320, 62 320, 62 321, 64 470, 64 472, 64 479, 64 480, 64 490, 64 491, 64 492). Timing of associated surgical treatment (cervical decompression, fusion, or arthroplasty, from anterior or posterior approaches) was similarly determined based on CPT coding of the surgical procedures typically utilized to manage DCM (22 542, 22 548, 22 551, 22 552, 22 554, 22 585, 22 590, 22 595, 22 600, 22 614, 22 856, 22 858, 22 861, 22 864, 63 001, 63 015, 63 020, 63 035, 63 040, 63 043, 63 045, 63 048, 63 050, 63 051, 63 075, 63 076, 0090 T, 0092 T, 0095 T, 0098 T, 0163 T).
Multivariate logistic regression was utilized to determine the association of steroid injection administration with surgical treatment at various time points after initial diagnosis. Fisher’s Exact Test and odds ratios were utilized as appropriate. Significance for all observed associations was assigned when P < .01. Multivariate statistical analysis was conducted using R (Version 1.0.143, R Project for Statistical Computing, Vienna, Austria). Data visualizations and supplementary statistics were calculated using Excel 365 (Version 2003, Microsoft Corporation, Redmond, Washington, USA).
Results
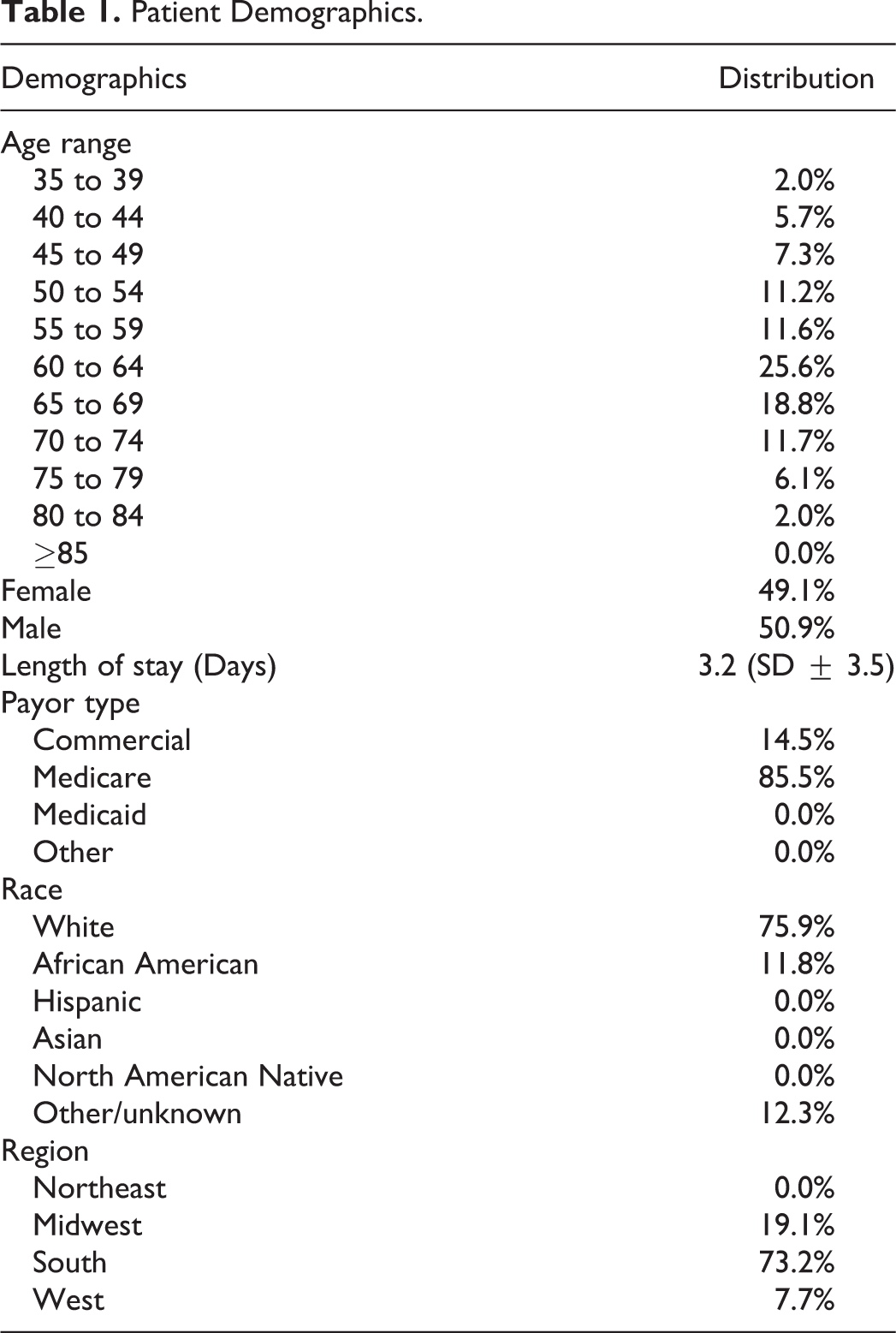
A total of 686 DCM patients were retrospectively identified in the PearlDiver database. A total of 244 patients underwent preoperative cervical spine steroid injections. Of these, 185 patients (75.8%) underwent epidural steroid injections, 35 (14.3%) underwent zygapophyseal injections, and 24 (9.8%) underwent transforaminal steroid injections. All patients underwent eventual surgical treatment. Median time from initial DCM diagnosis to surgery was 75.5 days (mean 351.6 days; standard deviation 544.9 days). Patient age range mode was 65 to 69 (25.6%, Table 1). Percentage of female patients was 49.1%. Surgical care was provided primarily in the hospital inpatient setting (88.0%) with the remaining cases managed with a same day discharge hospital outpatient procedure (12.0%). Payor distribution was the following: 86.4% Medicare (all forms), 13.6% commercial, and 0.0% Medicaid or other payors.
Patient Demographics.
Distribution of surgical treatment timing following DCM diagnosis varied by injection type (Figure 1). Nearly two-thirds (69.9%) of surgical intervention occurred within the first 3 months following DCM diagnosis for patients that did not receive a steroidal injection to manage symptoms early on. In contrast, approximately half of patients receiving transforaminal and zygapophyseal injections (50.0% and 51.4%, respectively) opted for surgical management of DCM between 3 and 6 months. Additionally, no patients treated with transforaminal injections received surgical management for DCM during the first 3 months following diagnosis. Similarly, no patients treated with zygapophyseal injections received surgical management for DCM during the first month following diagnosis. There was a statistically significant decrease in surgical management within 1 and 3 months for patients managed with either transforaminal or zygapophyseal injections relative to surgically managed cases that did not involve any steroid injection approach (P < .01). In contrast, epidural injections did not lead to a significant delay in surgical intervention (P > .01).
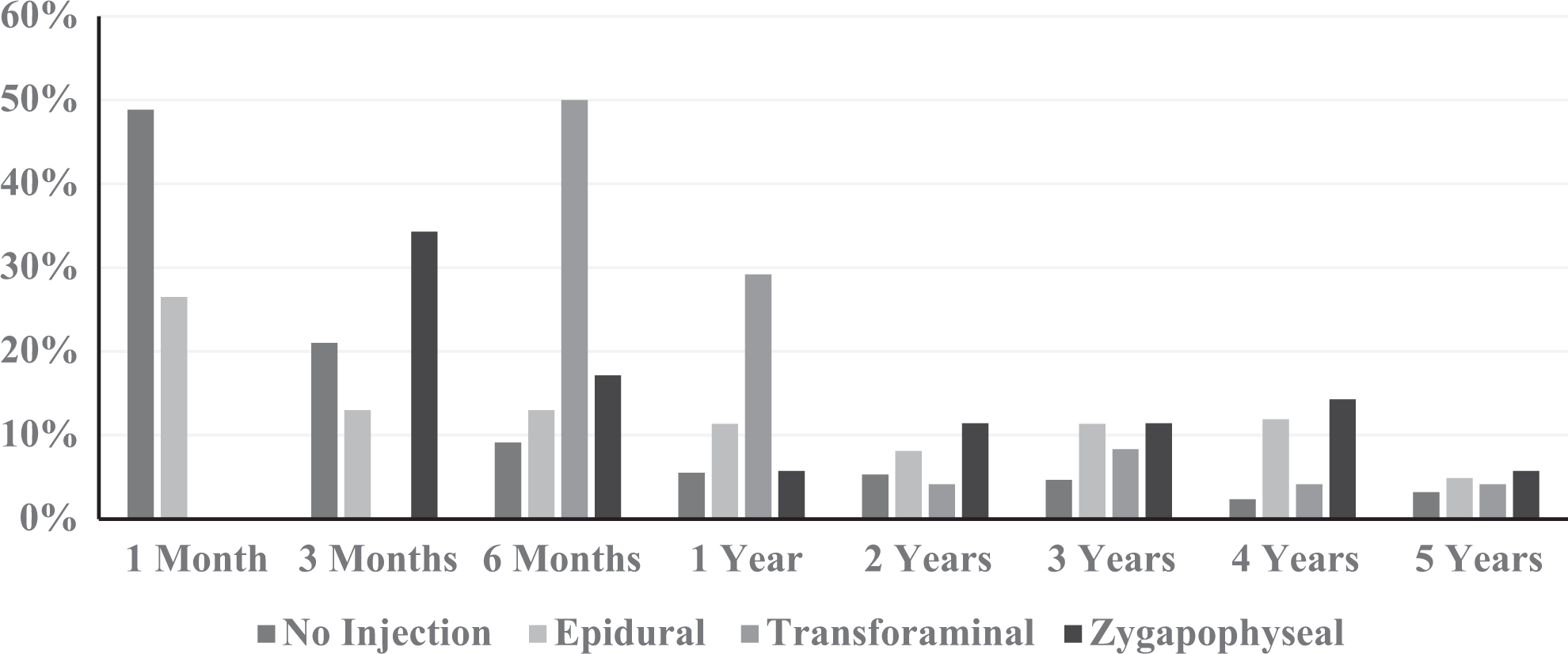
Distribution of surgical timing by injection type.
In multivariate analysis (Table 2), all 3 injection types were not associated with decreased odds of surgery within 1 month of diagnosis (P > .01), compared to patients not receiving injections. However, epidural and transforaminal injections were both associated with increased odds of surgery at 1, 2 and, 5 years after diagnosis (P < .01). Additionally, when all cases of DCM were examined for associations, steroid injections (all 3 approaches, relative to cases without steroid injection therapy) were associated with higher odds of surgery within 1 year (OR = 1.44, P < .01) and remained elevated during each examined time point through 5 years (OR = 2.01, P < .01).
Multivariate Analysis of Association Between Cervical Steroid Injection and Surgery for DCM.a
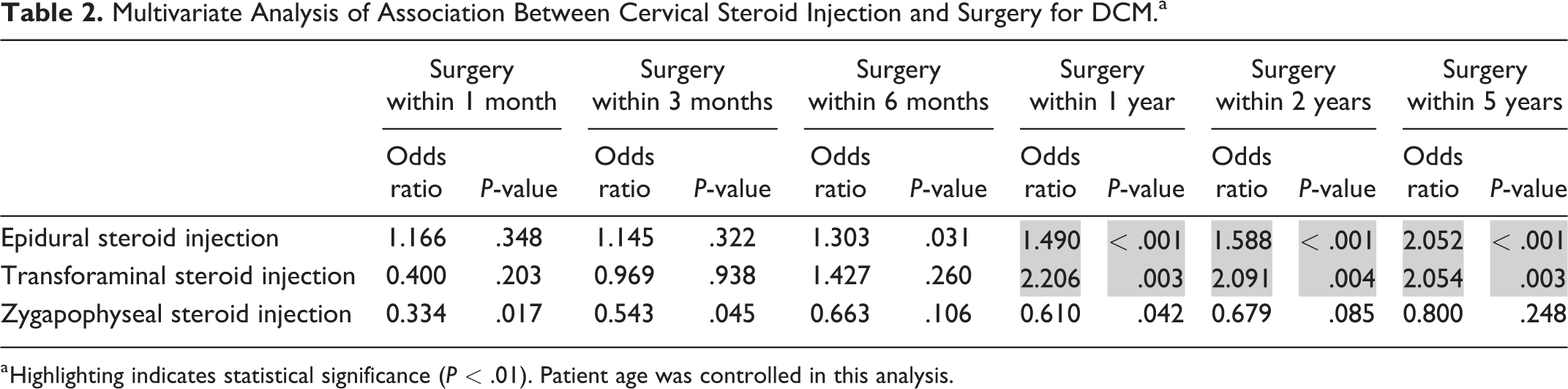
a Highlighting indicates statistical significance (P < .01). Patient age was controlled in this analysis.
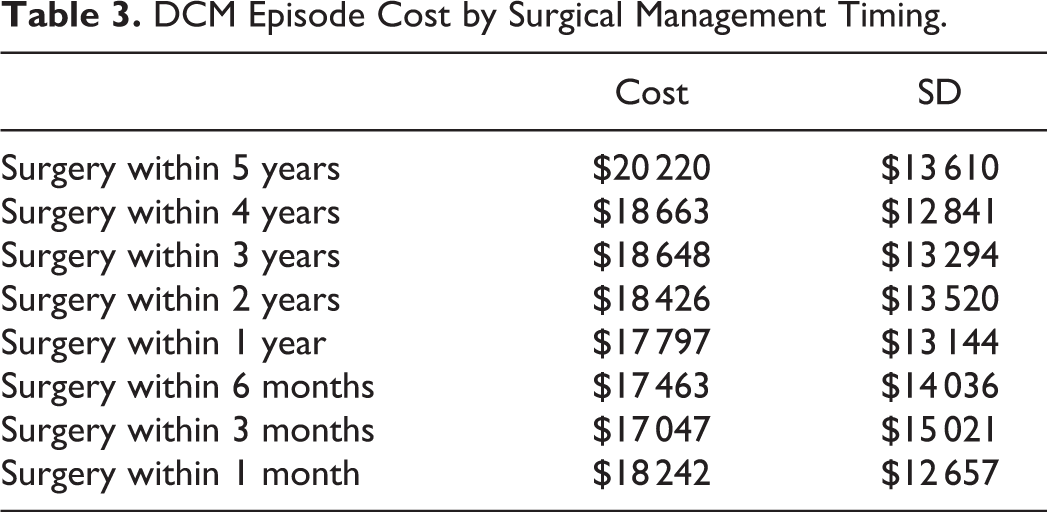
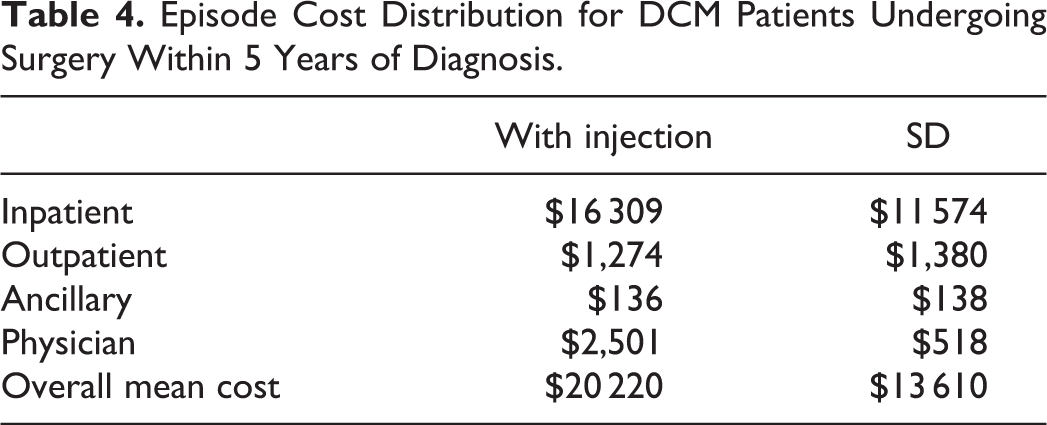
Cost to definitively manage DCM patients was assessed based on actual payor reimbursed amounts. Inpatient, outpatient, and ancillary service care settings for all reimbursed services delivered to a patient during their episode was included if the primary diagnosis of DCM was indicated. On average, $20 220 (σ = $13 610) was reimbursed to care for each patient initially managed with a steroid injection and followed with surgery (Table 3 and Figure 2). Cost of care was found to be significantly greater for surgery taking place after 2 years (P < .001; 2-Tail FET) following DCM diagnosis and steroid administration. Cost of care was concentrated during inpatient surgical management (80.7%) with less expenditure associated with outpatient management and ancillary services during a DCM episode (Table 4).
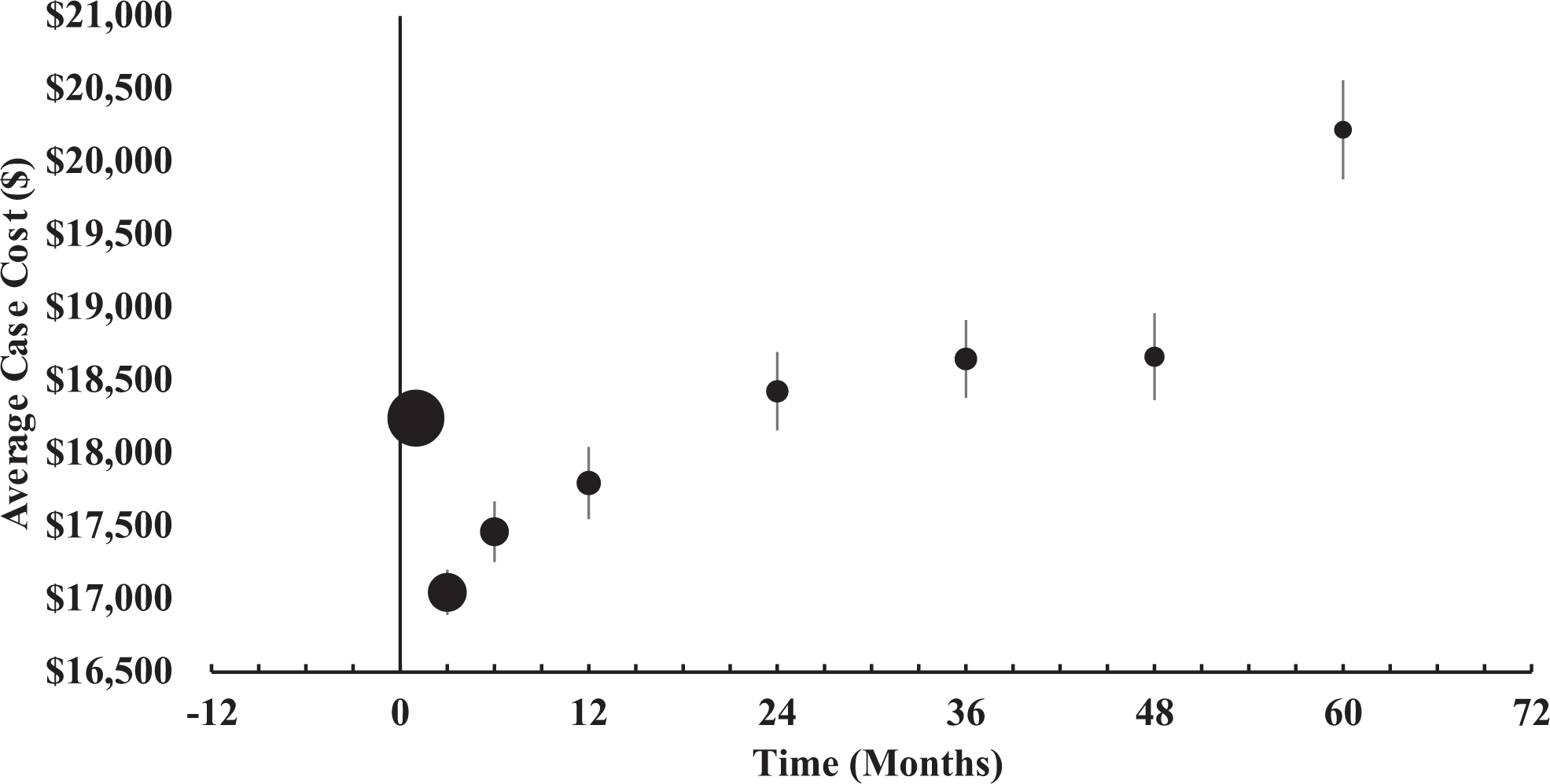
DCM Episode cost by surgical management timing. Circle size indicates relative number of patients treated within period. Confidence intervals of each study were estimated at the 95% level. The confidence interval approximately spans the diameter of the circle at month one (x̄ = $18 242, 95% CI [$18 137-$18 347]).
DCM Episode Cost by Surgical Management Timing.
Episode Cost Distribution for DCM Patients Undergoing Surgery Within 5 Years of Diagnosis.
Discussion
The current study demonstrates that cervical steroid injections do not prevent eventual surgical treatment of DCM. In addition, despite the lack of any evidence to support cervical steroid injections, over a third of patients identified underwent preoperative injections after receiving a diagnosis of DCM. This is an important addition to the available literature because the findings support general consensus among spine surgeons that CSIs are not efficacious in treatment of DCM. In addition, injections result in significant additional healthcare costs that are not justified by any clinical benefit.
Steroid injections for DCM appear to result in a variable relative delays to surgery across approach subtypes examined in this study. Epidural and transforaminal steroid injections were both associated with significantly increased overall odds of surgery within 1 year following diagnosis of DCM, compared with zygapophyseal injections. Cohen et al reviewed the literature on outcomes associated with zygapophyseal steroid injections and found symptom relief lasting upward of 3 months was possible in the majority of a subset of patients which demonstrated acute inflammation of the zygapophyseal joint. 13 However, the current study demonstrates that steroid injections overall do not significantly reduce the odds or meaningfully delay the need for definitive surgical management.
This is important because CSIs are known to be beneficial for treatment of cervical radiculopathy. The mechanism of action is similar to systemic corticosteroid injection, by inhibiting the inflammatory cascade surrounding a cervical nerve root causing radiculitis, albeit at a much higher concentration delivered locally in the epidural space.10,11 This is often given in conjunction with a local anesthetic that also functions to reduce nociceptive signaling. However, unlike cervical radiculopathy, DCM is a progressive pathology resulting from mechanical compression of the spinal cord, rather than the nerve roots, causing irreversible changes. Spinal cord compression from DCM is also often not accompanied by a significant inflammatory reaction, as is seen with radiculopathy or radiculitis.2,3 For this reason, DCM can often present with signs and symptoms of neurological injury without any associated neck or arm pain, and is not effectively alleviated by anti-inflammatory agents such as corticosteroids. Therefore, the novel finding that a majority of patients with DCM in the current study had at least 1 prior CSI is alarming. Especially after considering that patients with a concurrent diagnosis of cervical radiculopathy were excluded. A “dual diagnosis” of myeloradiculopathy would otherwise be an acceptable scenario for use of CSIs to temporarily alleviate radicular symptoms in a patient with concurrent DCM. However, the current study demonstrates that CSIs are frequently used in patients with isolated DCM, a scenario with little to no physiological basis for clinical benefit.
Cost to surgically manage a DCM episode was significantly greater for cases which utilized any steroidal injection approach prior to surgery. Specifically, by the fifth year after diagnosis with DCM, episodic costs were $20 220 when injections were utilized. A recent prospective cohort study by Witiw et al examined the quality-adjusted life year (QALY) impact of surgery for DCM using a Markov modeling approach. 14 Total cost during the diagnostic and treatment processes over 2 years was $14 497 ± $9,357. The reported total cost of DCM episode management in this work is in-line with the 2 year cost reported in our study once adjusted for the spending differential between the Canadian and US health systems. 15 Similarly, surgical costs made up 65.7% of the aggregate cost to treat DCM patients in Witiw et al which compares favorably to the cost distribution reported in our study sample. Given that we report total costs and distribution of costs similar to Witiw et al, the cost per QALY gained falls well below the established US QALY benchmark of $50 000 per QALY.14,16
A recent epidemiological analysis by Manchikanti et al examined the utilization of steroid injections in managing chronic pain in Medicare fee-for-service patients from 2000 through 2018. 17 Steroid injection utilization observed an annual decline of 2.5% during this 19-year period with a net decline of 20.7%. Interestingly, this overall trend obscures the observed increase of steroid injection utilization from 2000 through 2009, a period during which this pain management approach grew 7.3% annually with a net growth of 89.2% over 10 years. CPT coding unpaired with a related diagnostic code means this analysis was unable to differentiate between cervical and thoracic steroid injections. Between 2000 and 2009, cervical/thoracic transforaminal epidurals grew by 10.1% annually and decreased by 2.8% annually from 2009 and 2018. Overall, between 2009 and 2018, the greatest decline in steroid injections was observed in the cervical/thoracic transforaminal injection approach (−35.1%). A critical caveat to this finding provided by the authors of this work is the suggestion that the overall decline in steroidal injections may be related to targeted reimbursement declines enacted by Medicare in 2015 which significantly impacted reimbursement for steroid injections overall. For cervical/thoracic injections, however, utilization change preceded this reimbursement change and began to decline in 2013 (−1.3%) with 2014 observing the greatest utilization decline (−6.9%), potentially reflecting a broader recognition that this palliative measure has generally been overutilized.
Strengths of this study span 3 domains. First, because DCM is a relatively rare diagnosis, utilization of a claims database enables the examination of treatment and outcomes for a large population of DCM patients. Second, assessment of treatment timing and total episodic costs by service provided enables an understanding of the actual cost and timing involved with providing definitive treatment to DCM patients. Third, selection bias was limited by our database approach because the authors were blinded to patient level data.
Limitations to this study span 3 key areas: retrospective study approach, reliance on potentially inaccurate CPT classification of subjects, and generalizability of findings based on sample cohort demographics. First, utilization of a retrospective study approach limits the ability to identify and control for all potential sources of confounding in statistical analysis of the data because of the defined database fields available to examine and test. 18 Retrospective analysis is also unable to prove causality so only demonstrate association between variables is possible. Second, selection bias may inadvertently result because classification of subjects via CPT coding may be inaccurate and lead to misclassification of patients either as inappropriately diagnosed with DCM and onerously included into our analysis or inappropriately diagnosed with another condition and excluded from our study data. 18 Third, demographics of the patients included in this study may limit the generalizability of the reported findings. Recently, reported patient age of the average spine surgery patient was 56.6 years while another nationally scale study specifically on DCM patients managed surgically reported an average patient age of 60.6 years.19-21 Given the skew of age distribution toward older patients of the sample population in this work, both the reported conversion rate from injection to surgical patient and costs may be impacted. Another potential consideration that limits the generalizability of this work is significant Medicare payor skew. Cervical spine surgery patients in the United States typically are insured at similar rates by commercial health plans and Medicare with a smaller percentage (<10.0%) by Medicaid.21,22 Gender and regional distribution of patients appears to be in line with what is typically reported in large national database samples.21,22
In addition, another significant limitation of the current study is the lack of validated patient-reported outcome measures (PROMs). DCM is commonly classified and followed using a number of widely accepted PROMs including the modified Japanese Orthopaedic Association (mJOA) score, the Neck Disability Index (NDI), or patient-reported outcome measurement information system (PROMIS). These PROMs allow for accurate and objective evaluation of the severity of myelopathy, both at baseline and post-treatment. Unfortunately, the national-level dataset utilized in the current study does not contain PROMs data. In addition, patients are deidentified, making post hoc collection of PROMs impossible. As a result, the severity of myelopathy symptoms cannot be determined and compared between patients. In addition, patients with more severe myelopathy symptoms might actually be more likely to receive CSIs, introducing systematic bias into the result of the study. Nevertheless, even with this potential for bias, the current study still has merit by using time to eventual surgical treatment as a surrogate for myelopathy-specific PROMs and by demonstrating no significant benefit after CSIs for patients with DCM, regardless of severity of myelopathy. The finding that the majority of patients with newly diagnosed DCM receive a CSI is also an important and alarming finding of the current study.
The practice of cervical steroid injection, regardless of approach (epidural, transforaminal, or zygapophyseal), does not effectively prevent DCM and only delays surgical treatment by 1-3 months. While clinical benefits have not been demonstrated, steroid injections appear to also increase overall episodic costs of care for patients with DCM. Therefore the current utilization of cervical steroid injections in up to 36% of DCM patients is likely not supported by current evidence, unless specifically used for diagnostic purposes.
Footnotes
Authors’ Note
Location: Hospital for Special Surgery, 535 East 70th Street, New York, NY 10021, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.