
Abstract
Objectives:
To understand the impact of the coronavirus disease-2019 pandemic on sleep services within the United States Department of Veterans Affairs using separate surveys from “pre-COVID” and pandemic periods.
Methods:
Data from a pre-pandemic survey (September to November 2019) were combined with data from a pandemic-period survey (August to November 2020) to Veterans Affairs sleep medicine providers about their local sleep services within 140 Veterans Affairs facilities).
Results:
A total of 67 (47.9%) facilities responded to the pandemic online survey. In-lab diagnostic and titration sleep studies were stopped at 91.1% of facilities during the pandemic; 76.5% of facilities resumed diagnostic studies and 60.8% resumed titration studies by the time of the second survey. Half of the facilities suspended home sleep testing; all facilities resumed these services. In-person positive airway pressure clinics were stopped at 76.3% of facilities; 46.7% resumed these clinics. Video telehealth was either available or in development at 86.6% of facilities and was considered a lasting addition to sleep services. Coronavirus disease-2019 transmission precautions occurred at high rates. Sleep personnel experienced high levels of stress, anxiety, fear, and burnout because of the pandemic and in response to unexpected changes in sleep medicine care delivery.
Conclusions:
Sleep medicine services within the Veterans Affairs evolved during the pandemic with many key services being interrupted, including in-lab studies and in-person positive airway pressure clinics. Expansion and initiation of telehealth sleep services occurred commonly. The pandemic adversely affected sleep medicine personnel as they sought to maintain access to care.
Introduction
The coronavirus disease-2019 (COVID-19) pandemic negatively impacted access to healthcare as providers and health systems scrambled to meet varied and rapidly evolving medical needs.1 –7 Sleep medicine was heavily impacted by the COVID-19 pandemic. 8 The mainstay of obstructive sleep apnea (OSA) treatment is positive airway pressure (PAP). Because the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is transmitted through airborne droplets, clinicians feared that PAP might increase transmission through viral aerosolization.9,10 In response to guidance regarding mitigating SARS-CoV-2 transmission risk from the Centers for Disease Control, World Health Organization, United States Department of Labor Occupational Safety and Health Administration, American Academy of Sleep Medicine (AASM), and Veterans Health Administration (VHA),11–14 healthcare systems drastically reduced and modified the delivery of many sleep services11 –16 including screening individuals for COVID-19-related symptoms, maximizing use of personal protective equipment (PPE), developing and implementing protocols to support healthcare providers, using telehealth, and basing decisions about reintroducing healthcare services on local COVID-19 rates.15,16
Early within the COVID-19 pandemic, healthcare systems were routinely faced with conducting risk: benefit analyses on multiple levels. This was also true of whether or not to advise discontinuation of PAP, especially within households where there may be potential for PAP and other non-invasive ventilation users to potentially transmit SARS-CoV-2 to others within their household. 9 In these scenarios, providers and PAP users were asked to weigh the risks of PAP therapy continuation, and specifically the risk of transmission of SARS-CoV-2, against deleterious effects of discontinuation of PAP against the risks of PAP therapy discontinuation, which includes OSA recurrence, increased daytime sleepiness, psychomotor slowing, and several physiological parameters which may lead to adverse vascular event, including increases in heart rate and blood pressure, elevated urinary catecholamines, perturbations in cardiac repolarization, endothelial dysfunction, and return to unfavorable metabolic profiles.17,18 In more specifically considering PAP discontinuation among those with COVID-19, adverse effects of PAP discontinuation may be especially problematic, given the association between COVID-19 and increased risk of inflammation, coagulopathy, oxidative stress, and further endothelial dysfunction. 19
The VHA is the largest integrated healthcare system in the United States, delivering primary and specialty care services to more than 9 million Veterans annually. 20 The VHA is also the largest employer of healthcare personnel in the United States. 5 Sleep conditions are exceedingly common among Veterans, with OSA being the third most common chronic medical condition among Veterans receiving care within VHA.21,22 Given the very high prevalence of sleep disorders among Veterans, understanding the extent to which the pandemic affected sleep medicine services is of paramount importance. To address this gap in knowledge, we surveyed VHA sleep medicine providers after the first wave and into the second wave of the COVID-19 pandemic, 23 representing a period when geographically diverse centers could reflect on changes in the delivery of sleep medicine services while potentially looking toward how sleep services could be resumed. These results were compared to a survey of sleep centers conducted prior to the pandemic. We sought to identify: (1) the VHA sleep medicine facility- and provider-level impact of the pandemic, (2) plans for reintroducing previously interrupted sleep services, and (3) whether workflow might change longer term as a result of COVID-19. We hypothesized that in-person sleep services would be supplanted by telehealth and that appointments involving PAP would be commonly disrupted.
Methods
Study design
In this observational, cross-sectional study, data from two separate surveys administered to VHA sleep providers about local sleep services were used for this study. This study was completed by research staff during the course of their Addressing Sleep Apnea Post-Stroke/TIA clinical trial (NCT04322162). The initial (pre-pandemic period) survey was the Healthcare Analysis and Information Group (HAIG) VHA National Sleep Medicine Program survey (i.e., HAIG Sleep Survey). The survey instrument was created using the Verint Systems Inc.® survey software (Verint Systems Inc., Melville, NY, USA). The survey was administered to 140 VHA facilities from September 17, 2019, to November 1, 2019. 24 A second survey (pandemic period) was developed for this project with a goal of identifying the effect of the COVID-19 pandemic on sleep medicine services across VHA centers and was administered between August 26, 2020, to November 9, 2020. This anonymous, confidential, and voluntary 106-item survey was administered via Research Electronic Data Capture (REDCap®), Nashville, TN, USA, 25 distributed by the VHA National Program Office for Pulmonary, Critical Care, and Sleep via the VHA sleep medicine email listserv, and was made available to 840 sleep medicine providers across the same 140 VHA facilities (see Supplemental Appendix for both survey instruments). Neither survey has been published.
Participants
The pre-pandemic survey was electronically delivered to all VHA network directors and medical chiefs of staff within all VHA medical centers who distributed the link to sleep medicine program directors. The pandemic survey was electronically sent to sleep medicine program directors, sleep physicians, respiratory technologist, sleep technologists, and registered polysomnographic technologists (RPSGTs); targeting those with experience in clinical sleep medicine as well as operations of sleep medicine clinics and laboratories.
Survey development
The pre-pandemic survey was designed as a comprehensive assessment of the sleep medicine programs and resources at the facility-level throughout the VHA system. The HAIG and a Technical Advisory Group (TAG) of subject matter experts led by the VHA National Program Director for Pulmonary, Critical Care, and Sleep Medicine Services developed the survey. Members of the TAG included those with expertise in clinical sleep medicine and in managing sleep clinics and sleep laboratories, including pulmonologists, neurologists, and behavioral health specialists. The survey was piloted at five sites (3.6% of VHA sleep programs) diverse in their geography and level of sleep care in order to assess its validity, logic, and subject-matter accuracy. 24
The COVID-19 pandemic survey was designed by experts within the VHA with diverse backgrounds from sleep medicine (including physicians, RPSGTs), internal medicine, neurology, health services research/implementation science, and survey design. Similarly, this survey was pilot tested at two sites (1.4% of VHA sleep programs) and was assessed for validity, logic, and subject-matter accuracy. Participating sleep medicine providers had both clinical sleep and clinical operations expertise. The survey was also developed in conjunction with VHA National Program Office for Pulmonary, Critical Care, and Sleep. The first author (JJS) developed the first draft of the survey. Two physicians (JJS and BBK) and one analyst (AJP) collectively mapped questions from the pre-pandemic (HAIG) survey onto the pandemic survey. Consensus was obtained regarding topics to focus on and the order of questions. The survey included questions about: (1) impact of COVID-19 on all sleep services offered (e.g., in-lab diagnostic studies, ambulatory home sleep testing, using PAP) within an individual VHA facility, including cessation of previously offered programs and initiation of new sleep services; (2) how the pandemic affected members of the sleep service; (3) precautions taken to decrease the likelihood of COVID-19 transmission both for patients and for sleep lab personnel; (4) reopening of sleep services, including plans to address any backlog of sleep studies or visits and whether programs started during the pandemic would be continued. The survey included diverse response categories (e.g., “please check all that apply” as well as free text fields).
Inclusion/exclusion criteria
Survey responses were excluded if a survey was started but not completed. If more than one survey at a Veterans Affairs (VA) facility was completed by the same individual within a VHA FACILITY, then only data from the last completed survey was used. If the same VHA facility had multiple respondents, data from respondents who were listed as either the point of contact, sleep medicine director, or sleep lab director in the pre-pandemic survey was prioritized. Study participants for the pre-pandemic survey and the pandemic survey were included if they were involved in the provision of sleep care within their VA facility. Non-sleep care providers/personnel were excluded from receiving each survey.
Data collected
The pre-pandemic survey and the pandemic survey similarly collected facility-level data regarding the number and type of staff dedicated to sleep medicine, diagnostic (e.g., in-lab studies), and treatment services (e.g., PAP) for OSA and other sleep disorders, clinic types (e.g., in-person, virtual, PAP clinics), as well as facility identifier, geographic location of a given VHA facility. The pandemic survey also collected free text responses to the following questions: “How has COVID-19 affected staff within your sleep lab?”; “Once your VHA facility and Sleep Program reopens, what types of services do you envision resuming first?”; and “Once your VHA facility and Sleep Program reopens, what types of services do you envision resuming last?” Data were collected in VHA-approved workplaces. EJM and JJS conducted coding of qualitative free text responses.
Statistical analysis
Fisher’s exact test was used to test whether facilities which provided responses to the pandemic survey differed from sites that did not respond. Summary statistics were reported at the facility-level regarding sleep services which were continued, halted and not restarted, or halted and then restarted during the pandemic. Similarly, summary statistics were reported regarding new sleep services which began during the pandemic, the reported backlog of sleep studies which accumulated during the pandemic survey period, and in-person services and precautions taken to reduce transmission of the SARS-CoV-2 virus. Analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Thematic analyses of qualitative data from free text responses were conducted using NVivo 12 (NVivo 12, Denver, CO, USA). 26
Results
Respondents
The pre-pandemic survey received 140 responses from 140 VHA facilities, representing a 100% facility-level response rate. The pandemic survey received a total of 91 unique participant responses. Sixty-seven VHA facilities among the 140 (47.9% facility response rate) provided at least one response, with 19 facilities providing multiple responses.
Table 1 displays the baseline characteristic data from the VHA facilities which responded versus those that did not respond to the pandemic survey. The VHA facilities were comparable in terms of the service line under which sleep services resides. VHA facilities that responded were more commonly of higher complexity (p = 0.028), offered in-lab diagnostic studies (83.6% versus 42.5%, p < 0.001) and titration sleep studies (83.6% versus 41.1%, p < 0.001), home sleep testing for OSA (74.6% versus 45.2%, p < 0.001), in-person sleep medicine clinics (86.6 versus 53.4%, p < 0.001), and in-person continuous positive airway pressure (CPAP) clinics (38.8% versus 21.9%, p < 0.001). Although there was no difference between respondents and non-respondents regarding use of clinical video telehealth (CVT) sleep clinics (where Veterans receive their telehealth care by physically going to another VHA facility or a VHA Community-Based Outpatient Clinic whereas the sleep medicine provider is at a different VHA facility), respondents were more likely to have had VHA video connect than non-respondents (VVC; where Veterans receive their telehealth from home; 38.8% versus 21.9%, p = 0.029).
Baseline data for VA medical centers overall and by response status to COVID-19 sleep survey. a

COVID-19: coronavirus disease-2019; CPAP: continuous positive airway pressure; VA: Veterans Affairs.
The Facility Complexity Model within the Veterans Health Administration defines the clinical complexity of a VA facility based on the patient population served, clinical services complexity, and education and resourced. Complexity level 1a is the most complex designation. Whereas complexity level 3 is the least complex designation. 24
Pre-existing sleep medicine services impacted by the COVID-19 pandemic, change in sleep medicine clinic capacity, and backlog of sleep medicine services
Table 2 provides data on changes to sleep services during the pandemic for those facilities responding to the pandemic survey. Regarding in-lab sleep services among facilities which offered these services prior to the pandemic: 51/56 (91.1%) of VHA facilities reported that they stopped conducting in-lab sleep diagnostic studies and 51/56 (91.1%) of VHA facilities stopped conducting in-lab PAP titrations. Among the 51 facilities that stopped in-lab diagnostic studies, 39 (76.5%) resumed this service. Among the 51 facilities that stopped in-lab PAP titrations, 31 (60.8%) resumed this service. VHA facilities reported functioning at a reduced capacity for in-lab diagnostic and titration sleep studies: facilities reported operating at a median of 77% of typical capacity for in-lab diagnostic studies and 53. 50% of typical capacity for in-lab titration studies.
Pre-existing sleep medicine services impacted by the COVID-19 pandemic (N = 67).
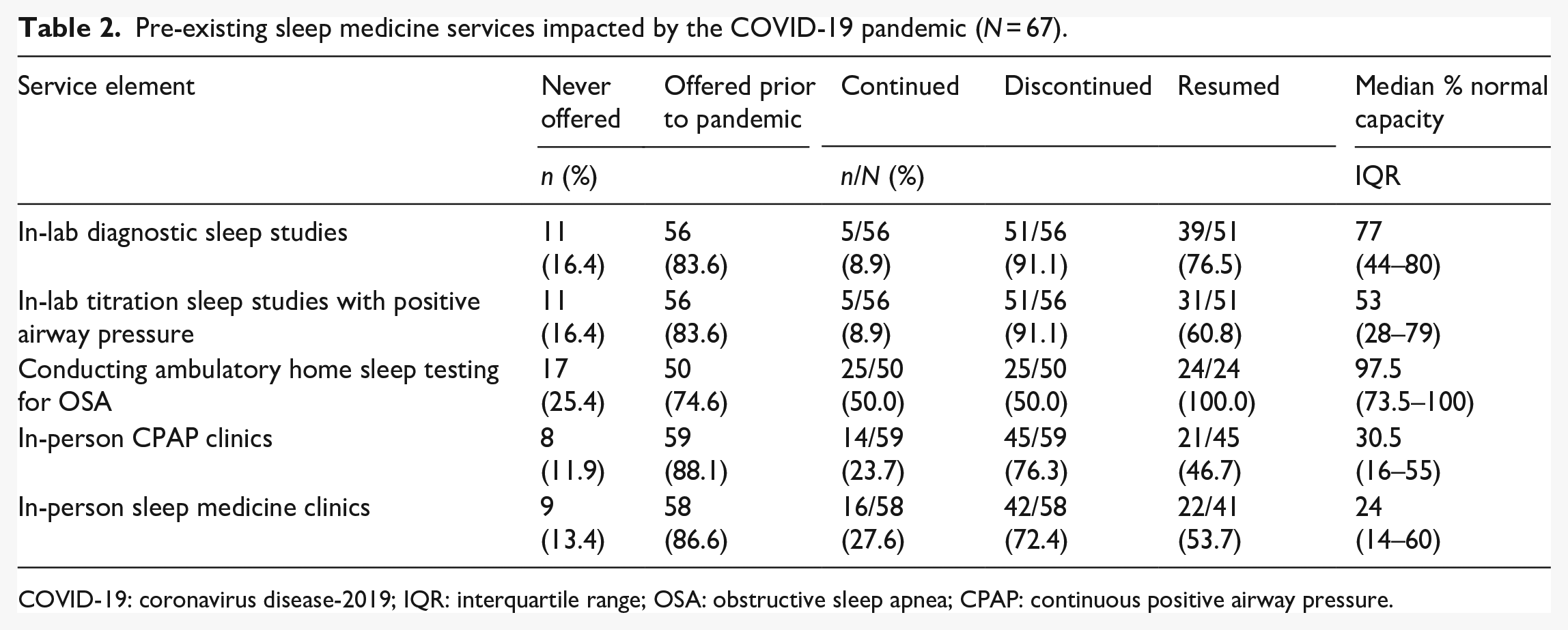
COVID-19: coronavirus disease-2019; IQR: interquartile range; OSA: obstructive sleep apnea; CPAP: continuous positive airway pressure.
Regarding in-person sleep medicine clinics, 58 (72.4%) VHA facilities discontinued this service; however, 22 (53.7%) facilities restarted these services during the pandemic. VHA facilities reported operating well below their pre-pandemic capacity (median of 24%). PAP clinics were similarly reduced during the pandemic: 45 (76.3%) of VHA facilities reported halting in-person PAP clinics, with 21 (46.7%) of these facilities reporting that they restarted this service, albeit at a reduced capacity (median of 30.5%).
Compared with the disruption of in-lab and in-person services, VHA facilities which offered ambulatory home sleep testing prior to the pandemic reported lower rates of discontinuation for conducting ambulatory home sleep testing during the pandemic. Among the 50 (50.0%) of facilities that discontinued its use of ambulatory home sleep testing for OSA, all facilities had resumed this service. VHA facilities reported that their ambulatory home sleep testing programs were operating close to pre-pandemic capacity (median of 97.5%).
Increased utilization of telehealth strategies and eConsults to deliver sleep services
As seen in Table 3, expansion of telehealth services delivered through either VHA VVC or CVT commonly occurred during the pandemic. More than a third of facilities continued VVC Sleep Clinics which existed prior to the pandemic; more than 40% reported they had created VVC Sleep Clinics whereas nearly 8% had these clinics under development. Similarly, more than a quarter of facilities continued preexisting CVT clinics, another 16.4% had created new CVT clinics, and 10.4% had CVT clinics under development. No facility reported discontinuation of telehealth clinics. In considering the growth of eConsults for Sleep services, 67.2% (45/67) of facilities reported they had developed an eConsult program during the pandemic while another 7.5% (5/67) were actively developing this service.
Use of telehealth to maintain the delivery of sleep services (N = 67).

VVC: VA video connect; CVT: clinical video telehealth; VA: Veterans Affairs.
Backlog of sleep studies as a result of the COVID-19 pandemic
Consistent with the cessation of sleep testing, 62.1% of VHA facilities reported in the pandemic survey that their patient backlog (i.e., accumulation of pending consults) for sleep studies increased. A median sleep study backlog of 150 patients (interquartile range (IQR): 67.5–455.5) was reported.
Precautions taken during the COVID-19 pandemic for patients and sleep medicine personnel
Table 4 provides the data about the use of pandemic-related precautions among facilities who responded that they were providing in-person services during the pandemic (68.7%; 46/67). One hundred percent of these facilities offered at least 1 safety precaution to reduce the transmission of SARS-CoV-2 when conducting in-lab diagnostic studies whereas nearly half of respondents indicated taking additional precautions with in-lab titration studies. Masks were reported to be more often used by sleep medicine personnel (100%) than by patients (89.1%). Face shields were also commonly used by technicians (87.0%). Precautions were taken more often when in-person demonstration and education of home sleep testing equipment was disseminated (46.3%) rather than only discussed (17.9%).
COVID-19 precautions taken for patients and sleep medicine personnel (N = 67).a

COVID-19: coronavirus disease-2019; PAP: positive airway pressure; PCR: polymerase chain reaction.
Qualitative thematic analysis
As seen in Table 5, five major themes emerged from responses to the open-ended prompt: “How has COVID-19 affected staff within your sleep lab?”:
Staff in the sleep lab developing COVID-19 themselves, with negative personal repercussions both for the infected individuals and for the emotional and functional well-being of the lab.
Spiking employee stress and anxiety related to the COVID-19 pandemic and its effects on the workplace and in the community.
Shifting to more telework and an uptick in the remote delivery of sleep services.
Working in new physical circumstances due to the newly mandated use of PPE.
Redeploying existing staff to other duties based on evolving needs of the VHA facilities, often inpatient respiratory therapy.
Of note, very few respondents reported that the COVID-19 had little to no impact on their sleep lab.
Open-ended written comments illustrating major themes related to “How has COVID-19 affected staff within your sleep lab?.”

COVID-19: coronavirus disease-2019; RT: respiratory therapist; MD: medical doctor; ICU: intensive care unit; RPSGT: registered polysomnographic technologist; HST: home sleep testing; PAP: positive airway pressure; PSG: polysomnogram; FTE: full-time equivalent; CPAP: continuous positive airway pressure; f/u: follow-up; VVC: VA video connect; PPE: personal protective equipment; VA: Veterans Affairs.
Two additional broad themes emerged in responses to the open-ended questions: “Once your VA facilities and Sleep Program reopens, what types of services do you envision resuming first?” and “Once your VAMC (VA Medical Center) and Sleep Program reopens, what types of services do you envision resuming last?”
Sleep services resuming first included in-person sleep services (i.e., Home Sleep Testing (HST) and CPAP set-ups, mask fit checking, standard PSG, in-lab studies [including baseline testing], CPAP walk-in clinics, desensitization therapy), home sleep testing, and VVC CPAP appointments.
Sleep services resuming later included PAP titration studies, in-person services (i.e., face to-face clinic appointments, in-person sleep lab, CPAP clinic, durable medical equipment return to clinic, overnight sleep testing in full capacity, CVT in Community-Based Outpatient Clinics, mask fitting, as well as “full beds without PPE and testing of Veterans”) and group visits (i.e., face-to-face group classes and group PAP set-up clinics).
Many respondents noted having plans to increase utilization of virtual care options even after in-person visits increased.
Discussion
The COVID-19 pandemic has impacted the delivery of sleep services throughout VHA as well as VHA-based sleep medicine service providers in important professional and personal ways. This large-scale assessment, which also included qualitative analyses of front-line sleep medicine providers and those responsible for clinical operations, demonstrates several key findings. The most commonly disrupted sleep services as well as those with the lowest rates of being restarted were those which required a provider and patient to be in close physical proximity to one another (e.g., in-lab sleep services, in-person PAP clinics). Home sleep testing services were impacted less than in-person sleep services, with an overwhelming majority of VHA facilities restarting their home sleep testing programs and reporting that they were operating near their pre-pandemic capacity. Although the VHA was an early adopter of telehealth (well before the pandemic), telehealth use increased substantially during the pandemic, with the greater growth in VVC use likely attributable to the convenience and safety which comes with patients receiving healthcare in their homes. VHA facilities adopted many of the routinely available and recommended COVID-19 precautions, which included use of PPE and temperature checks. Finally, the pandemic has negatively impacted the physical and mental health of sleep medicine personnel. Respondents reported either getting COVID-19, their colleagues becoming infected, and increased fear, stress, and anxiety related to infection with the SARS-CoV-2 virus. Furthermore, increased stress and challenges were reported with changes in workflow in delivering sleep services (e.g., shifting to telework, wearing PPE, increased time between in-person visits because of room cleaning, respiratory therapists (RTs) and RPSGTs shifted to work in parts of the sleep program which were bolstered to offset reduction in other parts of the sleep program), not being able to deliver sleep services because sleep medicine personnel were detailed to work in intensive care units and hospital wards, and general angst as it related to how the pandemic was increasing stress levels and increasing burnout.
Several of our findings are consistent with other investigations into how the pandemic has disrupted sleep medicine care delivery. In an online survey of 379 sleep medicine providers across 297 sleep centers outside of the VHA conducted between April 29, 2020, and May 8, 2020, 90.4% of responding centers reported reducing in-laboratory sleep testing by 90% or more, whereas 60.3% of centers endorsed reducing their HST programs. 8 Furthermore, symptom screening and temperature checks occurred within 77.1% and 64.3% of sleep programs, respectively. The higher rates of these COVID-19 safeguards reported in our current work may reflect that the survey period for our work began three and a half months after the survey period of the work by Johnson et al., 8 thus allowing for more time for these precautions to be implemented, and differences in the healthcare systems surveyed.
A novel contribution of the findings of our survey and noting that the survey period for the current work was August 2020 to November 2020, is that we are able to report on which halted sleep services were resumed during the survey period. In-person clinics, including sleep medicine clinics and CPAP clinics, had the lowest rates of being reinstituted; however, approximately half of sites reported bringing these services back during the survey period. Furthermore, all sites reported resuming HST and operating near pre-pandemic capacity. Trends for services that have restarted mirror the guidance offered by the AASM and other organizations and may also reflect a combination of an increasing trend toward using disposable HST equipment, reduced number of COVID-19 in the geographic region of given VHA facilities, increased availability of PPE, even more widespread use of other COVID-19 mitigation strategies (e.g., COVID-19 screening), and sleep medicine personnel becoming more used to changes in workflow.14 -16 Increasing the delivery of sleep medicine services may be associated with improved patient outcomes given the evidence that OSA is independently associated with developing severe COVID-19, 27 infection rates are higher for those with OSA compared to similar persons without OSA, 28 and that use of and greater adherence to PAP therapy is associated with reduced rates of developing COVID-19. 28
In order to provide continued access to sleep services, a majority of VHA facilities continued, expanded, or were in the process of implementing new telehealth services. Respondents also noted that telehealth services for sleep may continue at higher levels than at pre-pandemic moving forward. The use of telehealth has become widely considered as a means of improving access to experienced sleep medicine providers.29,30 Telehealth has also been found to be a safe and effective means of setting up CPAP and promoting adherence. 31 Our survey, as well as other work 8 conducted earlier in the course of the pandemic, indicates increased use of telehealth as a means of delivering sleep care.31,32
Sleep medicine providers have been affected by the pandemic in multiple ways. Given how the diverse skill sets of VHA sleep medicine providers matched the respiratory care needs of Veterans admitted to VHA facilities with COVID-19, many sleep lab personnel were detailed throughout the VHA facilities, including intensive care units, emergency departments, hospital wards, and to a lesser degree, to assist in home sleep testing programs. Noting the expertise of many sleep medicine providers, particularly those with training in pulmonary medicine, RPSGTs and pulmonologists were deployed to the front lines, at times contracting COVID-19 and/or being quarantined for COVID-19 exposure. The pandemic also increased stress and anxiety levels among sleep medicine personnel, many noting concerns and even fear for their safety and the safety of their families and patients. Fear was reported specifically in the context of being involved in PAP administration. COVID-19-related fear experienced by physicians has been reported outside of sleep medicine, with most physicians surveyed between March and April 2020 reporting fear of infecting family members (79.7%), rapid spread of COVID-19 (63.0%), and COVID-19-related complications (60.3%). 33 It is notable that fear continued to be a pervasive theme of healthcare providers between the latter study and our current work despite the survey periods being months apart.
High rates of burnout were reported. Contributing to the enhanced stress, anxiety, and burnout were stressors related to the pronounced changes in workflow and care delivery, specifically increased utilization of telehealth and providing in-person care while wearing PPE. Work done outside of sleep medicine has similarly demonstrated pronounced physical and mental health impact of COVID-19 on healthcare workers, especially among providers who have close contact with patients (i.e., ⩾12 times/day), have 15 h or more of continuous patient contact, and work in a high-risk department. 3 Additionally, distress, insomnia, anxiety, and depression were commonly reported. 3
Our study has important strengths. First, the “pre-pandemic” sleep survey was completed just prior to the beginning of the COVID-19 pandemic. Combining data from a “pre-pandemic” survey conducted with the intention of understanding VHA-wide sleep capacity within VHA facilities with data from a survey conducted to understand the variety of ways in which the COVID-19 pandemic has affected the same sleep programs may have lessened the effect of recall bias. Second, this study was conducted within an integrated healthcare system, where dissemination of guidance and best practice may occur more readily than across individual sleep clinics and health care systems. Third, by sampling a period several months into the pandemic, which includes a time period after the April 27, 2020, release of AASM guidance regarding COVID-19 mitigation strategies, we were able to examine not only which sleep services were stopped but also which were restarted. Finally, to our knowledge this study is the first to conduct a qualitative analysis regarding how the pandemic has affected individuals delivering sleep medicine services, with these results highlighting feelings toward pronounced changes in workflow and work responsibilities, which oftentimes put them at increased risk of becoming infected with the SARS-CoV-2.
There are also limitations to this work. First, data from both surveys were self-reported; when reported, less than half of VHA medical centers responded to the pandemic survey. Second, although all participants were involved in sleep medicine, each may have varying degrees of knowledge regarding changes in sleep services offered during the pandemic, especially as recommendations evolved and were disseminated. Furthermore, the unit of the survey analysis was at the facility-level, rather than the provider-level. Hence, demographics of survey respondents were not collected. Next, the survey was conducted after the first wave and during the second wave of the pandemic, and thus, does not reflect how the delivery of sleep services may have changed after the development and dissemination of COVID-19 vaccinations. As both surveys were disseminated broadly throughout the VHA sleep medicine community, a power calculation was not conducted. Furthermore, as we used all available qualitative responses in the COVID-19 pandemic survey questionnaire at the end of the survey period, and hence, did not examine qualitative data prospectively, we do not have information regarding whether thematic saturation was or was not obtained. Finally, there were statistically significant differences in VHA facilities between respondents and non-respondents, such that respondents were more likely to have been delivering sleep medicine services within higher complexity VHA facilities. Additionally, responding VHA facilities were more likely to offer almost all sleep services surveyed except for CVT. These differences raise the concern of selection bias, and hence, the findings may be more applicable to more complex VHA facilities with a greater array of sleep services.
Conclusions
Sleep medicine services offered throughout VHA have undergone several pronounced changes during the COVID-19 pandemic. VHA facilities shifted away from in-person clinics and studies, especially those where CPAP was involved, and pivoted toward expanding HST and telehealth programs, with a preference for telehealth in the home (i.e., VVC). Anxiety, increased stress, fear, and burnout exists among sleep medicine providers, regardless of whether they were detailed to care for patients in COVID wards, work longer hours to compensate for increased absenteeism or loss of other healthcare personnel, were adapting to using PPE, or shifted to remote delivery of sleep medicine services. The use of telehealth will likely continue to grow as a provision under sleep services in the COVID-19 era and beyond.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231169388 – Supplemental material for Impact of the coronavirus disease-2019 pandemic on Veterans Health Administration Sleep Services
Supplemental material, sj-docx-1-smo-10.1177_20503121231169388 for Impact of the coronavirus disease-2019 pandemic on Veterans Health Administration Sleep Services by Jason J Sico, Brian B Koo, Anthony J Perkins, Laura Burrone, Ali Sexson, Laura J Myers, Stanley Taylor, W Claibe Yarbrough, Joanne K Daggy, Edward J Miech and Dawn M Bravata in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121231169388 – Supplemental material for Impact of the coronavirus disease-2019 pandemic on Veterans Health Administration Sleep Services
Supplemental material, sj-docx-2-smo-10.1177_20503121231169388 for Impact of the coronavirus disease-2019 pandemic on Veterans Health Administration Sleep Services by Jason J Sico, Brian B Koo, Anthony J Perkins, Laura Burrone, Ali Sexson, Laura J Myers, Stanley Taylor, W Claibe Yarbrough, Joanne K Daggy, Edward J Miech and Dawn M Bravata in SAGE Open Medicine
Footnotes
Acknowledgements
The views expressed in this article are those of the authors and do not necessarily represent the view of the Department of Veterans Affairs.
Author contributions
JJS (male, physician/clinician-scientist), BBK (male, physician/clinician-scientist), EJM (male, research scientist), and DMB (female, physician/clinician-scientist) contributed to the design of the work, including survey and manuscript preparation. AJP (male, analyst) and EJM conducted analyses on survey data. LB (female, research assistant), ST (male, data manager), and LJM contributed to data acquisition. JJS, BBK, LB, AS (female, research assistant), LJM (female/data scientist), ST, WCY (male, physician/clinician-scientist), JKD (female, research scientist), EJM, and DMB contributed to data interpretation.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have read this manuscript and approve of its submission. This work was produced at VA Connecticut Healthcare System, West Haven, CT and Richard L Roudebush VA Medical center in Indianapolis, IN. All authors, except for Dr W Claibe Yarbrough, MD, received salary support from the Addressing Sleep Apnea Post-Stroke/TIA clinical trial (NCT04322162). All authors have no conflicts of interest in the publication of this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Veterans Affairs Office of Research and Development, Health Services Research and Development Addressing Sleep Apnea Post-Stroke/TIA (ASAP) clinical trial (grant number: 1I01HX002324-01A2). Clinical trial data obtained directly from ASAP clinical trial (NCT04322162), as a facility-level randomized controlled trial, was not used in this manuscript. Rather, both surveys predated the beginning of the active implementation phase of ASAP. The funding body did not take a role in the design of the study and collection, analysis, and interpretation of data or in writing the manuscript.
Ethics approval and consent to participate
Ethics approval for this study was waived by the VA Connecticut Healthcare System (VACHS) Institutional Review Board (IRB) as it was deemed to be a quality improvement (QI) project rather than research (Ethics Waiver Number JS0001). Similarly, informed consent was not sought for the present study because the VACHS IRB deemed the study to be a QI project rather than research. Hence, the project was granted a QI waiver and the need to obtain informed consent was waived by the IRB.
Informed consent
Informed consent was not sought for the present study because the VA Connecticut Healthcare System Institutional Review Board (IRB) deemed the study to be a quality improvement (QI) project rather than research. Hence, the project was granted a QI waiver and the need to obtain informed consent was waived by the IRB.
Preprint submission
A preprint of the manuscript, “Impact of the COVID-19 Pandemic on Veterans Health Administration Sleep Services” was submitted elsewhere.
Data sharing statement
Due to Veterans Health Administration (VHA) regulations and our ethics agreements, the analytic data sets used for this study are not permitted to leave the VHA firewall without a Data Use Agreement. This limitation is consistent with other studies based on VHA data. However, VHA data are made freely available to researchers with an approved VHA study protocol. For more information, please visit ![]() or contact the VHA Information Resource Center at
or contact the VHA Information Resource Center at
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.