
Abstract
Study Design:
Systematic review.
Objectives:
Management of stable traumatic thoracolumbar burst fractures in neurologically-intact patients remains controversial. Conservative management fails in a subset of patients who require subsequent surgical fixation. The aim of this review is to (1) determine the rate of conservative management failure, and (2) analyze predictive factors at admission influencing conservative management failure.
Methods:
A systematic review adhering to PRISMA guidelines was performed. Studies with data pertaining to traumatic thoracolumbar burst fractures without posterior osteoligamentous injury (e.g. AO Type A3/A4) and/or the rate and predictive factors of conservative management failure were included. Risk of bias appraisal was performed. Pooled analysis of rates of failure was performed with qualitative analysis of predictors of conservative management failure.
Results:
16 articles were included in this review (11 pertaining to rate of conservative management failure, 5 pertaining to predictive risk factors). Rate of failure of conservative management from a pooled analysis of 601 patients is 9.2% (95% CI: 4.5%-13.9%). Admission factors predictive of conservative management failure include age, greater initial kyphotic angle, greater initial interpedicular distance, smaller initial residual canal size, greater Load Sharing Classification (LSC) score and greater admission Visual Analog Scale (VAS) pain scores.
Conclusion:
A proportion (9.2%) of conservatively managed, neurologically-intact thoracolumbar burst fractures fail conservative management. Among other factors, age, kyphotic angle, residual canal area and interpedicular distance should be investigated in prospective studies to identify the subset of patients prone to failure of conservative management. Surgical management should be carefully considered in patients with the above risk factors.
Introduction
Management of stable traumatic thoracolumbar burst fractures in the neurologically-intact patient remains a controversial aspect of spinal trauma. Both conservative and surgical management are utilized for similar fracture morphologies. 1 Studies comparing non-operative to surgical management have largely found equivalence in terms of treatment outcomes. 2 Studies on orthotic versus non-orthotic management of burst fractures similarly demonstrate no difference in clinical outcomes. 3 However, conservative management fails in a subset of patients who require subsequent surgical stabilization. Many studies on conservative management of neurologically-intact burst fracture patients deliberately exclude patients with significant immediate post-injury kyphotic deformity, anterior loss of vertebral height, and/or traumatic canal stenosis.4,5 This serves in part to exclude patients with occult posterior ligamentous injury. Admission variables have not been rigorously examined in terms of their predictive value for failure of conservative management.
The aim of this systematic review is to 1) determine the rate of failure of conservative management, and 2) analyze prognostic factors (at the point of admission) influencing failure of conservative management in neurologically-intact patients with traumatic thoracolumbar burst fractures without posterior osteoligamentous injury (e.g. AO Type A3, A4).
Methods
This systematic review is conducted in accordance to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (PROSPERO Registration: CRD42020181008).
Definitions and Eligibility Criteria
“Failure” of conservative management was defined as the need for surgical management within 6 months of injury after initial conservative management. “Conservative management” included all non-operative interventions. This includes any combination of mandatory bed rest, early ambulation, physiotherapy, body casting, orthotic devices and closed reduction. In studies that included more than one conservative treatment modality (e.g. orthotic and non-orthotic conservative therapy), all patients were considered as a single (conservative) cohort.
To maintain homogeneity of included subjects, only neurologically-intact adult subjects (≥18 years old) with traumatic burst-only fractures (without posterior osteoligamentous injury, distraction, rotational or translational injuries) were included. Burst fractures are defined as vertebral body fractures involving/extending to the posterior border of the vertebral body. This includes, but is not limited to, AO Spine Type A3, A4 fractures, 6 Magerl AO Type A3.1/A3.2/A3.3 fractures, 7 or Denis burst-type fractures. 8 Studies on compression-only fractures (e.g. AO Type A1/A2), distraction fractures (e.g. AO Type B), translational and rotational fractures (e.g. AO Type C) were excluded. Both retrospective and prospective studies (with N of at least 10) of consecutive patients were included. Only studies that reported on the rates of conservative management failure, and/or statistically significant (P < 0.05) predictors of conservative management failure were included. Included studies have a minimum duration of 6 months mean follow-up. For the purpose of determining rate of failure of conservative management, the authors included fractures at the levels of T10-L3. For the purpose of analyzing admission factors predictive of conservative management failure, the authors included fractures at the levels of T10-L5. This decision was due to the presumed scarcity of literature on predictive admission factors.
Studies on osteoporotic or pathological fractures were excluded. Further, studies on fractures in patients with ankylosing spondylitis or diffuse idiopathic skeletal hyperostosis were excluded. Studies on multiple fracture types were included if they provided information on subgroup analysis of the burst-type fractures.
Information Sources and Search Strategy
Medline/PubMed, EMBASE and the Cochrane Database were systematically searched from 1st January 1995 to 29th May 2021. Combinations of the following medical subject headings (MeSH) or key words were used in the search strategy: “Spinal fractures,” “Burst fractures,” “Conservative treatment,” “Treatment outcome,” “Treatment failure,” “Orthotic devices,” “Prognosis.” Titles and/or abstracts were screened and full texts of potential articles assessed for final inclusion. Bibliographic references and citations of all included articles were further screened to identify additional eligible articles.
Data Collection and Analysis
An electronic spreadsheet (Microsoft Excel, Redmonds, WA, USA) with required data fields was created a priori. Data regarding authorship, publication year, title, study design, fracture classification, demographics, type of conservative management, rate and nature of conservative management failure, clinical and radiographic predictors of conservative management failure was extracted from included articles.
Qualitative and quantitative analysis of conservative management failure was performed. Pooled analysis of conservative management failure rate was calculated with a random-effects model (OpenMetaAnalyst, Providence, Rhode Island, USA). Statistical heterogeneity among included articles was reflected by Forest plots and the I 2 index. Predictors of conservative management failure were recorded and assessed if their derivation was borne from univariate or multivariate logistic regression analysis. Results are described on a qualitative basis.
Study Risk of Bias Assessment
Risk of bias for randomized trials was performed in accordance to the Cochrane Handbook for Systematic Reviews of Interventions. Risk of bias for observational studies was performed according to Agency for Healthcare Research and Quality (AHRQ) recommendations, with modifications made to accommodate studies pertaining to prognostic factors. 9 Studies not accounting for other prognostic factors were automatically graded as at least of moderately high risk.
Results
Study Selection
The search algorithm returned a total of 1404 articles. 152 articles were selected for full text review after initial screening of titles and/or abstracts. Manual searching of included articles’ citations and bibliography generated a further one article for inclusion (Figure 1). Thus, a total of eleven4,5,10-18 studies had data on conservative management failure rate, and a total of 512,14,17,19,20 studies had data on predictive factors of conservative management failure.
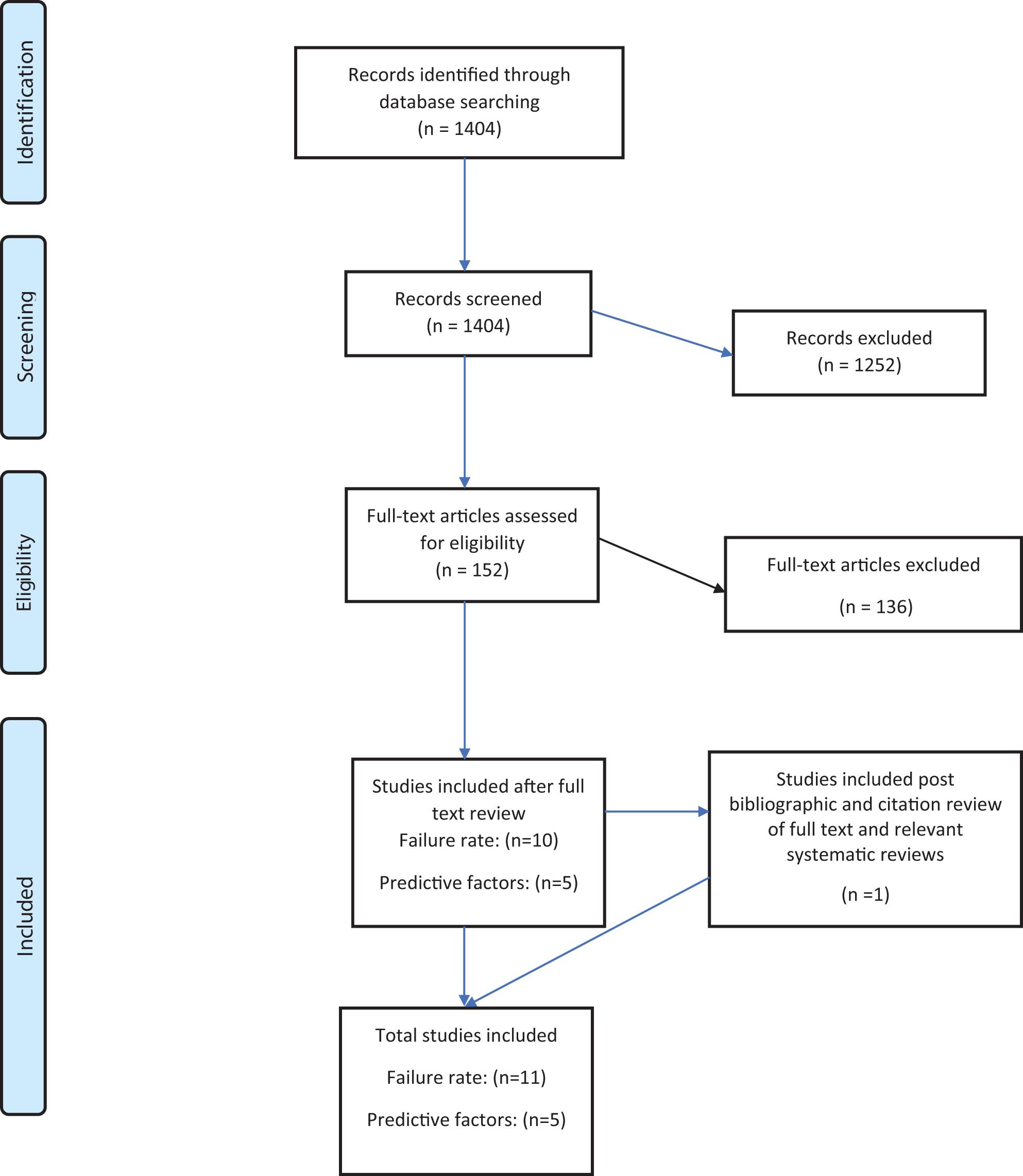
PRISMA flow diagram of study inclusion.
Rate of Conservative Management Failure
Study characteristics and outcomes
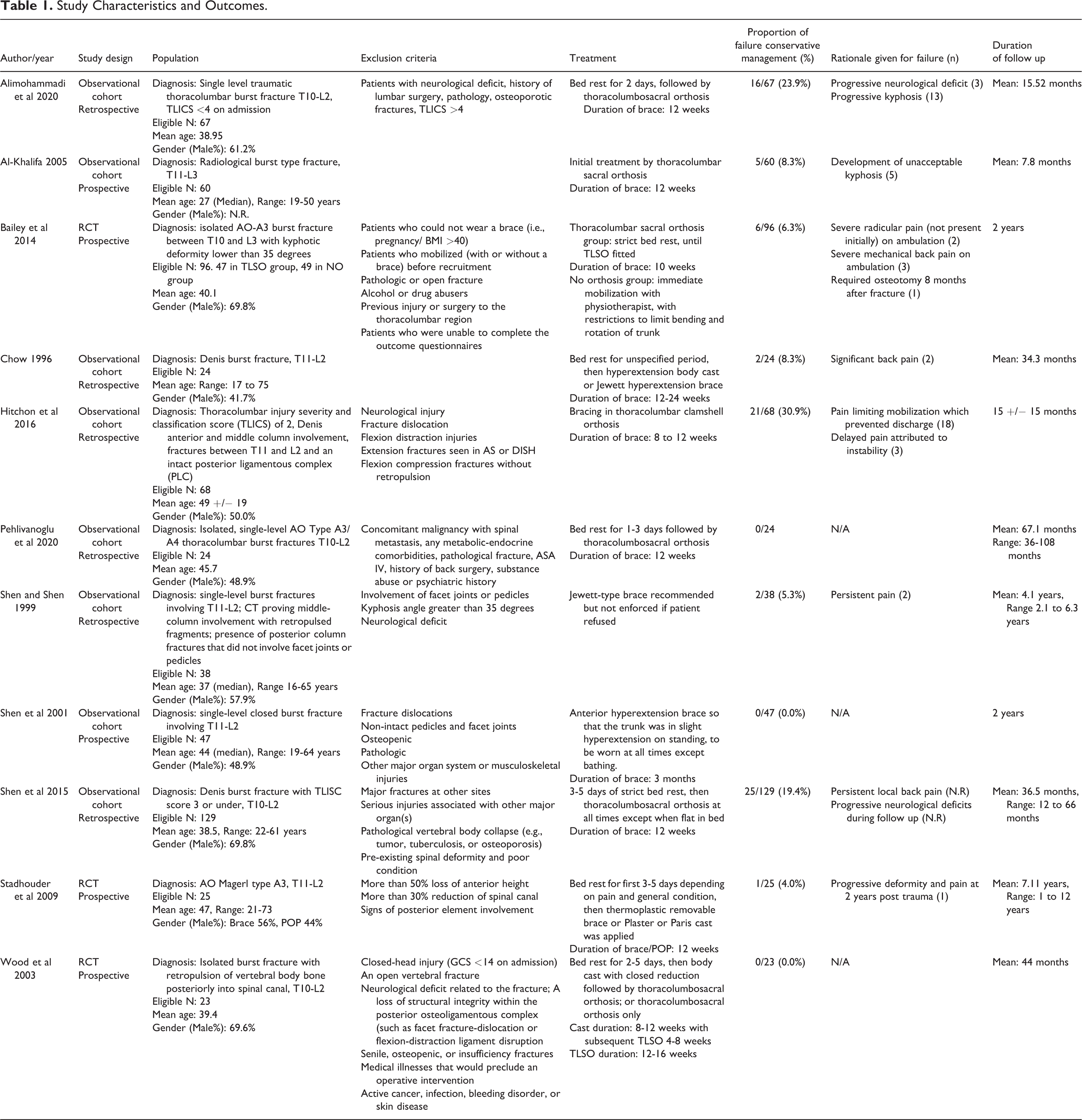
11 Studies, including 34,15,16 randomized controlled trials (RCTs) and 8 cohort studies (2 prospective,10,13 6 retrospective5,11,12,14,17,18) were included. There was a total of 601 patients (Range of patients per study: 23 to 129) included (Table 1).
Study Characteristics and Outcomes.
One of the 3 RCTs compared outcomes in thoracolumbar burst fractures in patients with orthosis versus no orthosis. Bailey et al 4 enrolled 96 patients with AO Spine Type A3 fractures and randomized patients to receive a thoracolumbar sacral orthosis (TLSO) for 10 weeks or non-brace therapy. Patients were included only if they had an isolated burst fracture and post-injury kyphotic deformity of less than 35 degrees. Six patients had failure of conservative management and required surgery for radicular pain (n = 2), severe mechanical back pain on ambulation (n = 3), or severe kyphotic deformity during follow up (n = 1). Four were from the TLSO group, and 2 were from the non-braced group.
Stadhouder et al 15 randomized 25 patients with AO Magerl A3.1/3.2/3.3 thoracolumbar burst fractures to receive either an orthotic brace or Plaster of Paris cast for 12 weeks. Only patients with less than 50% loss of anterior vertebral body height and less than 30% reduction of spinal canal were included. There were no significant radiologic or functional difference between the 2 treatment arms. One patient in the orthotic brace group required surgical fixation due to progressive deformity with pain at follow up.
Wood et al 16 randomized 47 patients with isolated thoracolumbar burst fractures to receive operative fixation versus conservative management (body casting or orthosis). 23 patients were randomized to the conservative arm. There was no exclusion of patients based on post-injury kyphosis, canal encroachment or anterior vertebral body height loss. There were no significant functional outcomes between treatment arms. No patient from the conservative arm had failure of conservative management on follow up.
Of the remaining 8 studies included, the majority (7 studies) were single-arm observational cohort studies. All studies except for one 5 included an anti-flexion orthosis for periods of 8 weeks to 24 weeks as part of their conservative management regimen. Table 1 summarizes the characteristics of the included studies.
Descriptive analysis
Overall, 78 of 601 (13.0%) patients required surgical fixation due to failure of conservative management. Development of neurological deficits during conservative management is uncommon. Two patients, in the study by Bailey et al, 4 developed severe radiculopathy on ambulation requiring surgical fixation and decompression. Three patients, in the study by Alimohammadi et al, 17 developed “progressive neurological deficit.” It is not clear if these deficits refer to radiculopathy or spinal canal compression. Three studies13,16,18 reported no patients requiring surgical fixation after employing a conservative approach. Patients underwent surgical fixation due to reasons of mechanical back pain on ambulation, development of radiculopathy on ambulation or progression of kyphotic deformity.
Of the 7 studies (n = 378)4,5,10-12,15,17 that reported specific reasons for 53 patients who failed conservative management, 28 (52.8%) failed conservative measures due to back pain, 19 (35.8%) failed due to development of kyphotic deformity, 1 (1.9%) failed due to combination of pain and kyphosis, and 5 (9.4%) failed due to occurrence of neurological deficit (n = 2 due to new radicular pain, n = 3 type of deficit not recorded). Recorded data from individual studies is shown in Table 1.
Pooled analysis
Pooled analysis of all 601 patients from the 11 included studies showed that the rate of failure in the conservative management of thoracolumbar burst fractures is 9.2% (95% CI: 4.5%-13.9%) (Figure 2). The I 2 statistic of 83.9% demonstrates substantial heterogeneity within the included studies. The retrospective study by Hitchon et al 12 was an outlier with a conservative management failure rate of 30.9% (21 of 68 patients). Sensitivity analysis using leave-one-out meta-analysis demonstrated that no single study had a significant influence on the overall effect size (forest plot not shown).
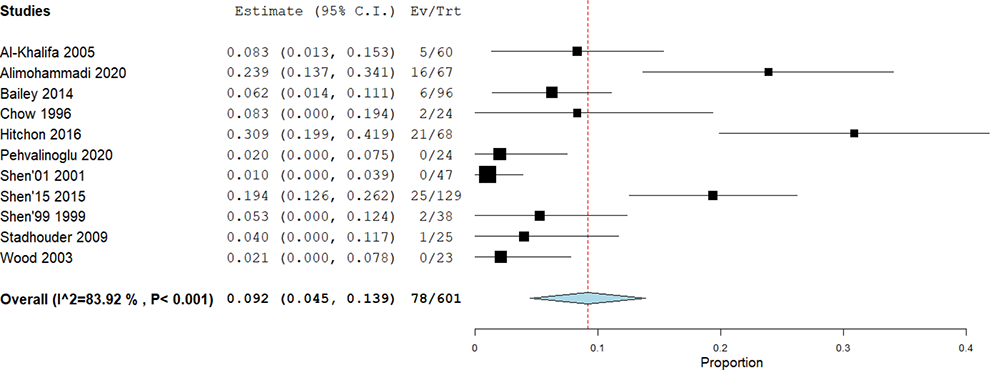
Pooled analysis of overall failure rate of conservative management.
Pooling of the included RCTs and prospective cohorts only (n = 251) demonstrated a conservative management failure rate of 3.6% (95% CI 0.8%-6.4%, I 2 = 32.4%) (Figure 3).
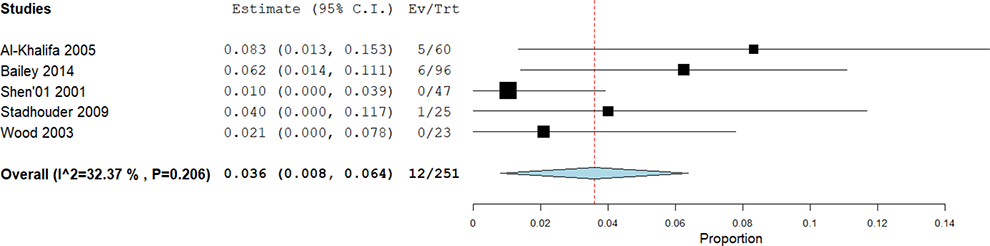
Pooled analysis failure rate of conservative management from included prospective studies.
Predictors of Conservative Management Failure
Study characteristics
Five studies (1 prospective, 19 4 retrospective12,14,17,20) with a total of 448 (Range: 60 to 129) patients analyzed factors predictive of failure of conservative management (Tables 2 and 3). Four12,14,17,20 of 5 studies employed multiple logistic regression as part of their statistical analysis to identify significant predictive factors. The remaining study by Azhari et al 19 relied on testing of means between groups (Student’s t test) only. Table 3 details type of statistical tests used and results from individual studies.
Demographic predictors
Age was studied in all 5 studies with inconsistent results. Of 4 studies using multivariate regression, 2 studies found that older age was significantly predictive of failure of conservative management,17,20 while another 2 found older age to not be a factor in failure of conservative management.12,14 In the study by Azhari et al 19 younger age was found to be associated with conservative management failure on univariate analysis (Failure group: 33.4 +/− 11.4 years, Successful group: 51.4 +/− 13.5 years, P = 0.003).
Gender (2 studies14, 20), Body Mass Index (one study 12 ) and Smoking status (one study 17 ) were found to not be significantly predictive of failure of conservative management.
Clinical predictors
In one study, 14 higher VAS pain score at admission was significantly predictive of failure of conservative management. Patients who failed conservative management had higher admission VAS pain scores compared to those who were successfully managed conservatively (6.5 ± 1.9 points versus 3.6 ± 1.3 points respectively, OR = 2.91, 95% CI: 1.103-8.059, P = 0.031).
McCormack’s Load Sharing Classification (LSC) score was studied in one study 12 and found to be a significant predictor of failure of conservative management. Patients requiring surgery have a higher initial LSC score compared to those managed successfully with conservative therapy (LSC: 6.9 +/− 1.1 points versus LSC: 5.8 +/− 1.3 points respectively, P = 0.006).
Radiographic predictors
Kyphotic angulation at admission was studied in 4 studies. In 2 studies,14, 17 increased kyphotic angulation at admission as measured by Cobb angle was not significantly predictive of failure of conservative management. In the remaining 2 studies where kyphotic angulation was measured as the angle subtended between adjacent intact endplates, one study 12 found increased kyphotic angulation significantly predictive of failure of conservative management (P = 0.017), while the second study 20 demonstrated a trend toward being a significant predictor of conservative management failure (P = 0.056, OR = 1.131, 95% CI 0.997-1.283).
Residual canal area at admission was studied in 4 studies. In 3 studies,12,19,20 smaller residual canal area at admission (47-52% residual canal area in the failure group, versus 63-67% residual canal area in the conservatively successful group) was predictive of failure of conservative management. In one study, 14 residual canal area at admission was found to be non-predictive.
Interpedicular distance at admission was investigated in 2 studies.14,17 Increased interpedicular distance at admission was found to be significantly predictive of conservative management failure in both studies. A similar degree of post-injury interpedicular distance (29.18% 17 and 29.7% 14 respectively) was found in the group of patients who failed conservative management.
Table 2 summarizes predictive factors studied in the above studies, and Table 3 details factors identified from individual studies.
Summary of Predictive Factors Studied.a
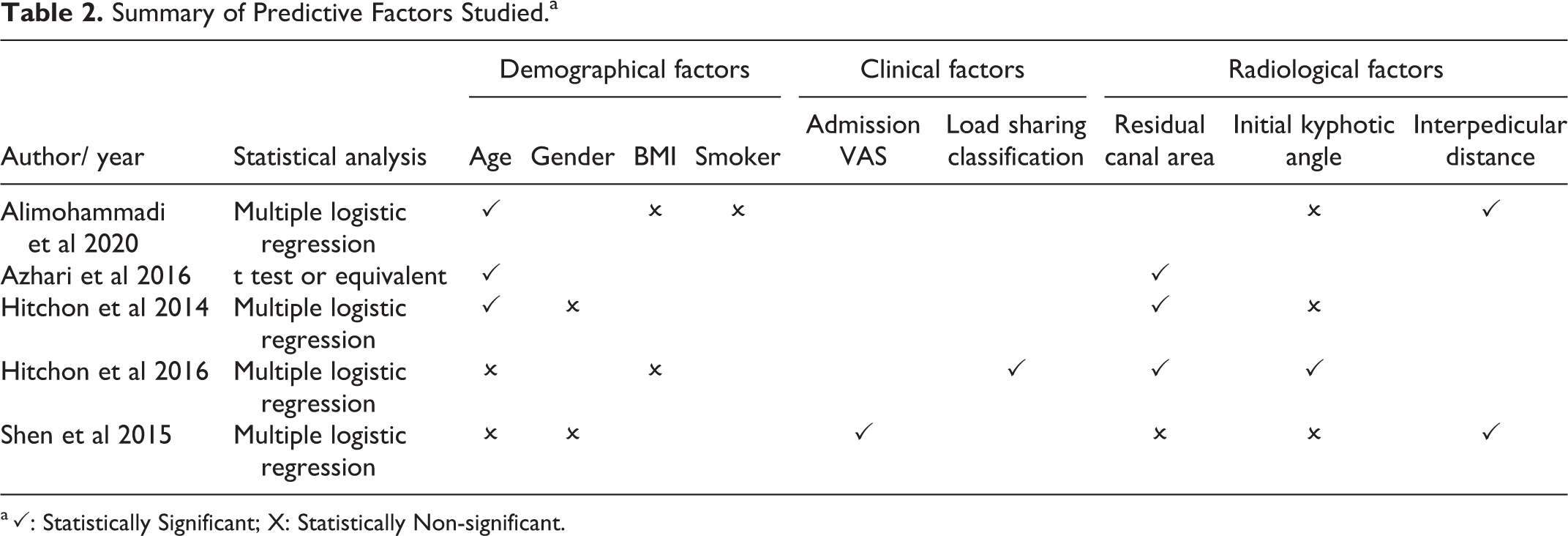
a ✓: Statistically Significant; X: Statistically Non-significant.
Detailed Synopsis of Predictive Factors Studied.
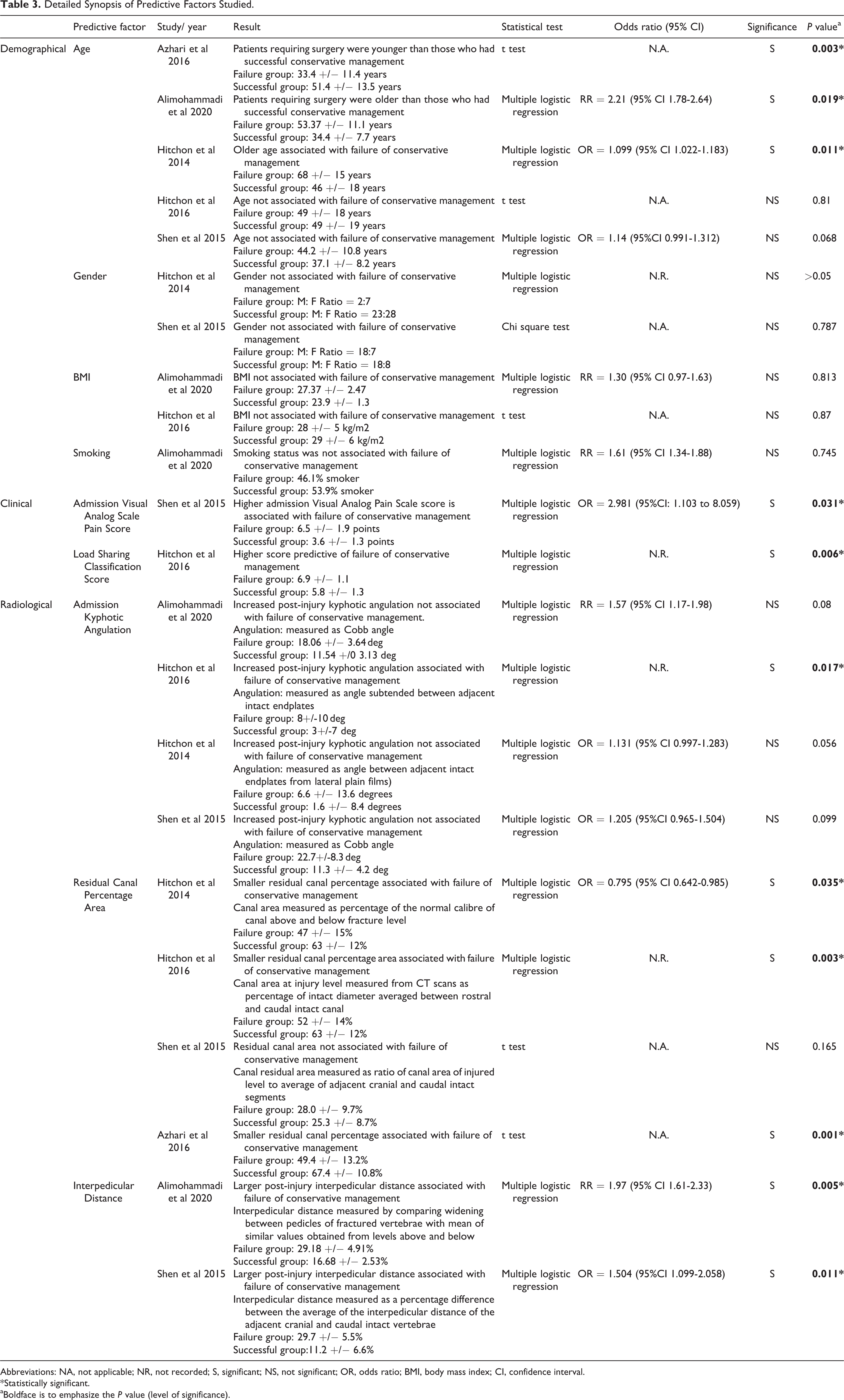
Abbreviations: NA, not applicable; NR, not recorded; S, significant; NS, not significant; OR, odds ratio; BMI, body mass index; CI, confidence interval.
* Statistically significant.
aBoldface is to emphasize the P value (level of significance).
Risk of Bias Assessment
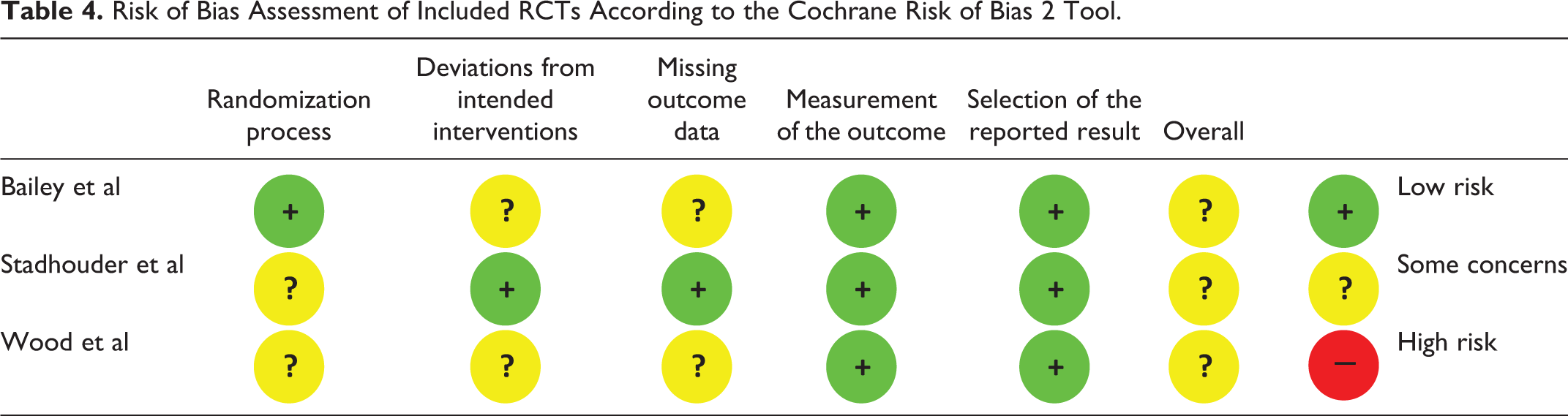
Using the Cochrane Handbook for Systematic Reviews of Interventions Risk of Bias 2 tool, all 3 included RCTs were assessed as having some concerns (Table 4). Stadhouder et al 15 had no description of allocation sequence for their randomization process, nor of subsequent blinding prior to implementation of interventions and hence was graded as having some concerns. Bailey et al 4 was downgraded due to reported lack of compliance to brace intervention, and unclear reasons behind missing data; potentially contributing to bias. Wood et al used computer-generated randomization to randomize 53 individuals, however noted a statistically significant difference (P < 0.01) in baseline characteristics for smoking, where 16/24 (67%) of the operative group compared to 4/23 (17%) of the non-operative smoked. Furthermore, 6 patients were lost to follow up in total, including 2 deaths, and hence this study was also rated as having some concerns.
Risk of Bias Assessment of Included RCTs According to the Cochrane Risk of Bias 2 Tool.
Risk of bias for cohort studies of prognosis was performed using the Agency for Healthcare Research and Quality (AHRQ)’s domains (Table 5). 5 studies were of high5,11,18 or moderately high10,13 risk, due primarily to lack of accounting for other prognostic factors. The remaining 3 studies12,14,17 were found to be of moderately low risk.
Risk of Bias Assessment for Cohort Studies, Using the Agency for Healthcare Research and Quality (AHRQ)’s Domains.
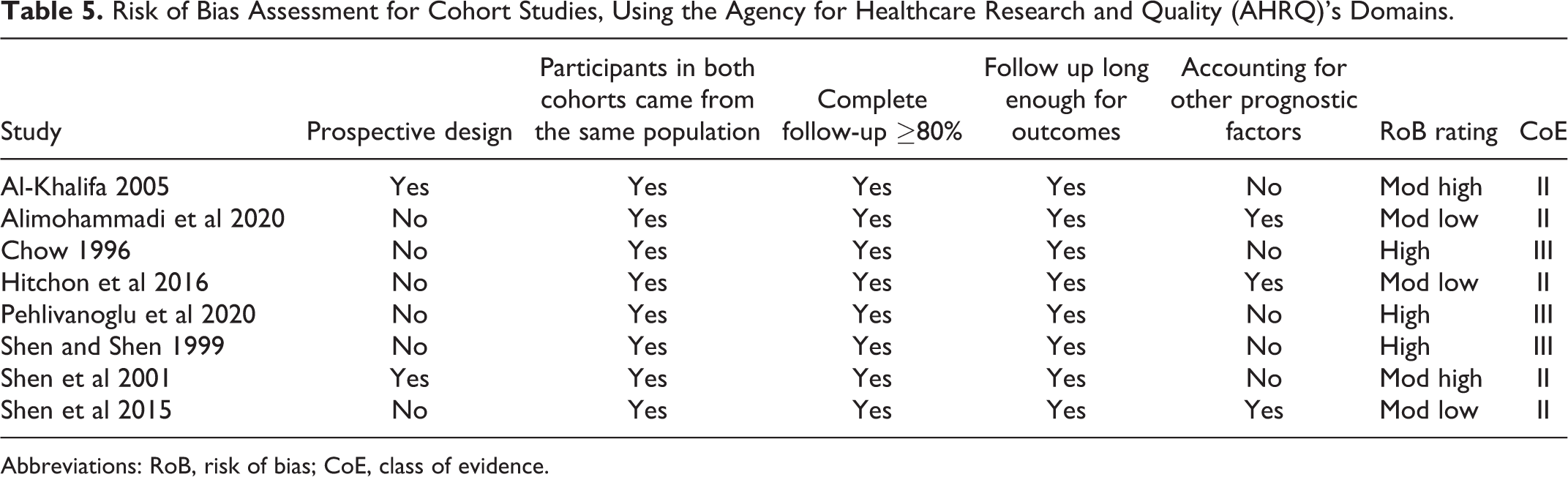
Abbreviations: RoB, risk of bias; CoE, class of evidence.
Discussion
Despite multiple thoracolumbar classification systems and associated decision-making aids e.g. TLICS, AOSpine injury score (TL AOSIS), 1 the optimal management of a thoracolumbar burst fracture in the neurologically-intact patient without any disease modifiers (TLICS = 2, AOSpine A3N0M0, AOSpine A4N0M0) remains controversial. While conservative management with, or without orthosis is well-recognized, well-accepted and safe, there is a subset of AOSpine A3/4N0M0 who fail conservative management and require surgical fixation for progressive pain, deformity, or rarely, neurological injury.
The management of these thoracolumbar fractures is highly variable. In a survey of 483 spinal surgeons in 6 different continents, there was marked differences in the management of neurologically-intact burst fractures, especially AOSpine A4 fractures. 1 In this survey, 51.7% of South American surgeons and 46.0% of European surgeons will recommend surgical intervention for AOSpine A4N0M0 fractures, compared to 0% of North American surgeons.
From our review, 9.2% of neurologically-intact patients with thoracolumbar burst fractures fail non-operative management and require subsequent surgical fixation. Conversely, 90.8% of patients were successfully managed in a conservative fashion. In this review, conservative management is a catch-all strategy encompassing all non-operative treatment. In particular, we included all patients with or without orthotic bracing as a single cohort. Multiple reviews on the use of orthosis3,21 have resulted in a prevalent literature consensus on the equivalency of orthosis and non-orthotic use in the treatment of these thoracolumbar fractures.
Besides regional variability, institutional, surgeon-specific, patient-based factors all undoubtedly play a role in deciding upon conservative or surgical treatment. The main impetus driving spinal surgeons to opt for surgical management are to 1) alleviate mechanical pain, 2) prevent long-term kyphotic deformity, and 3) prevent development of neural injury. In order to prevent any of these outcomes from occurring, it is important to be able to identify the subset of patients who will benefit from upfront surgery using variables available during the initial hospital admission. The admission risk factors identified in this manuscript serves as a starting point for spine surgeons to consider the need for up-front surgical management in patients with AO Type A3/A4 thoracolumbar fractures.
As demonstrated in this review, the available literature is sparse on factors predictive of failure of conservative management. In terms of demographical variables, age is the variable that has been most often investigated. However, inconsistent results have been reported in terms of this predictive factor. Azhari et al, 19 using univariate statistics, found younger patients more likely to fail conservative management. In contrast, Hitchon et al 20 and Alimohammadi et al, 17 using logistic regression analysis, found older patients more likely to fail conservative management. It is not immediately clear how this discrepancy of results between studies have come about but could possibly be due to heterogeneity in terms of subjects between studies, or institutional differences in surgical decision-making. However, if older age does predict conservative management failure, spinal surgeons will have to take this into account prior to embarking on surgical management.
Regarding clinical predictors of conservative management failure, higher admission VAS pain score was the only clinical factor found to be associated with failure in one study. 14 It is not specified at what point after admission the VAS pain score was measured i.e. at the point of initial emergency department admission, versus when the patient is allowed to ambulate in the upright position.
Radiographic appearances are key in decision-making for surgical management of thoracolumbar fractures. Kyphotic deformity at admission, smaller residual canal area, substantial loss of vertebral body height, vertebral body comminution are factors which spinal surgeons consider during their decision-making. As demonstrated by the current review, the quantity and strength of the current evidence is limited. In this review, kyphotic deformity at admission was a significant predictive factor for conservative failure in one study and showed a strong trend toward significance in one study. Presence of kyphotic deformity at admission, especially at the thoracolumbar junction, has been shown to portend a greater degree of kyphosis on follow up. However, degree of eventual kyphosis is not necessarily minimized by surgical fixation, 22 and increasing kyphotic angle at follow has not been consistently shown to result in worsening functional outcomes. 23 Additional research is required to delineate the contributory effect of admission kyphotic deformity to a patient’s need for eventual surgery.
Residual canal area was identified as a significant predictive factor in 3 of 4 studies (2 using logistic regression, one using univariate analysis). Degree of canal compromise is reflective of vertebral body involvement and retropulsion, and could correspond to mechanical pain. Similarly, increased interpedicular distance could be a correlate of degree of vertebral body involvement. A dreaded outcome of conservative management of AOSpine A3/4 fractures in neurologically intact patients is the subsequent development of neurological injury. However, this is a uncommon phenomenon. In this review, 5 of 601 patients developed new neurological symptoms. It is well-known that remodeling of the spinal canal occurs post burst fracture injuries with subsequent improvement in residual canal area. 24
The McCormack Load Sharing Classification (LSC) incorporates vertebral body comminution, apposition of fracture fragments, and degree of deformity correction into a 9-point classification system. It was devised as a classification to predict the need for anterior stabilization in addition to posterior instrumented fixation. 25 The LSC was investigated in one study and found to be a significant predictive factor of conservative management failure. Vertebral body comminution and spread could portend eventual kyphotic deformity and should be investigated in future studies.
Limitations
Whilst failure of conservative management of thoracolumbar burst fractures is clearly defined as the conversion to surgical management in this review, the reasons underlying this conversion is less well-defined from the included studies. The clinical indications for conversion to operative management are often obvious and include mechanical pain on ambulation precluding discharge, development of radicular pain, or significant increases in kyphosis on erect posture. Nonetheless, in the absence of pre-determined clinical thresholds/scores to determine conservative management failure, individual, institutional and regional variances in management necessarily influences the number of patients who are converted to surgical management.
As seen from the I 2 statistic in the pooled analysis, there is significant heterogeneity between studies. This has been mitigated by 1) the strict and homogeneous inclusion of adult patients with defined burst-only thoracolumbar fractures without neurological injury, and 2) the subgroup analysis using only the prospective included studies. For the purposes of investigating admission factors for failure of conservative management, the authors included fractures from the levels T10-L5 due to the expected paucity of literature on this topic. The inclusion of low lumbar fractures reduces applicability to junctional thoracolumbar fractures. The included data (not shown) from individual studies is insufficient to perform subgroup analysis for this outcome.
Conclusion
A proportion (9.2%) of conservatively managed, neurologically-intact thoracolumbar burst fractures fail conservative management. Among other factors, age, admission kyphotic angle, admission residual canal area and interpedicular distance should be further investigated in prospective studies to identify the subset of patients prone failure of conservative management. Surgical management should be carefully considered in patients with the above risk factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.