
Abstract

The optimal treatment for thoracolumbar (TL) burst fractures without neurological deficits has remained a controversial topic with different schools of thought worldwide advocating for surgical management or non-surgical management. The many efforts in determining best treatment have faced many challenges. Conducting pragmatic randomized controlled trials in surgery to produce highest level of evidence has been quite challenging thus far for multiple reasons. Treating surgeons understandably have a fear of providing suboptimal treatment to patients contrary to their local expertise. Traumatic spinal pathologies often require urgent decision. Blinding and allocation concealment is difficult for surgical treatment. Ultimately, patient’s accrual can be quite arduous. In medicine, high-quality evidence should be obtained prior to the integration of fracture management practices into clinical practice. Paramount to the impact of these studies is the outcome measure chosen to evaluate the superiority of once treatment strategy over another. Outcome selection is a complex and challenging process notably due to wide spectrum of outcome measures used in orthopedics and spinal trauma.1,2 Final outcome selection should reflect an understanding of the disease or injury as well as benefits and harms of the proposed intervention. 3
Many different outcome measures have been utilized in TL burst fractures research with many other studies attempting to settle the debate between nonoperative management and surgical management and producing inconclusive and mixed results.4,5 A Cochrane review of available research published in 2013 showed a wide range of different clinical outcome parameters. 6 Two trials were included and reported on pain (NAS), Roland and Morris disability questionnaire, disability, return to work, complications, subsequent surgery, kyphosis and length of stay. Ultimately, the contradictory evidence was insufficient to conclude whether surgical or non-surgical treatment yields superior pain and functional outcomes.
The recently published prospective international multicenter AO A3A4 study by Dvorak et al has attempted to answer many burning questions regarding best treatment of neurologically intact patients with TL burst fractures. 7 The primary outcome chosen was time to achieve an improvement in minimally clinically important difference in Oswestry Disability Index at 1 year. Results showed that surgically and non-surgically treated patients do not differ in terms of ODI improvement. With inconclusive results, investigators reflected on whether ODI was an appropriate measure in spinal trauma. This tool has been developed for degenerative chronic low back pain. It has not been created or validated for acute spinal injury. The emphasis of this tool may be misplaced in long term. In trauma, there is lower incidence of back pain after the acute phase vs worsening in degenerative back pain.
Using the data collected from the AO A3A4 prospective study, a health economic analysis by Dandurand et al was also conducted and has recently been published. 8 This study was conducted from a societal perspective including direct and indirect costs notably patient and caretaker productivity loss. The cost-utility analysis revealed that surgery is the dominant approach at 2 years and through working lifetime horizon. Surgery was cost-effective largely due to the greater productivity loss of patients and caregivers within the non-surgical group. Additionally, the non-surgical group had more frequent physician and allied health visits with higher utilization of medication including opioids. This finding should encourage a shift in how we measure outcomes following spinal trauma. The investigator’s mindset should shift towards returning patient to their pre-injury productivity levels as the ultimate goal. Doing so will optimize a patient’s life as well as society where caregiver burden and healthcare utilization will be decreased. Health economics should become an essential part of the investigations attempting to determine the superiority of one treatment over another.
There is a lack of consensus in which instruments should be used when measuring spinal trauma outcomes. Many different types of outcomes have been used such as quality of life physical and mental measures, disability indices, functional and spinal cord injury measures. A systematic review identified the outcome measures used in evaluating adults sustaining cervical spine fractures. 9 The most popular outcomes measured radiological parameters such as fusion and stability as well as mortality or complications. Less than 30% of studies reported on patient reported outcomes or functional assessment. However, the review identified an increasing use overtime in patient reported outcomes and functional assessment. In the 1980s, only 13.3% of studies reported such outcomes compared to about 35% in 2020s. Another systematic review identified pain and neurological deficits at the most common outcome measures used in spine trauma research using International Classification of Functioning, Disability, and Health (ICF) as a reference10. A bibliometric analysis reviewed outcome instruments in spinal trauma surgery. Interestingly, functional or QoL outcomes were more commonly used in cervical trauma compared to TL trauma. 11 Overall, instruments used in spinal trauma research have been designed for chronic conditions, not acute trauma. Very few outcome instruments used in spinal trauma have been validated. A review by Stadhouder et al in 2010 showed that only the Walking Index for Spinal Cord Injury has been validated in spinal trauma, specifically in spinal cord injury patients. 12 When evaluating the wide spectrum of outcome measures selected in the literature, it becomes clear that the heterogeneity of instruments evaluating the same domain as well as the lack of validated instruments is creating multiple levels of complexity.
Of note, in the orthopedic scientific literature, an increasing usage of PROMs has been observed which are guiding clinical decision-making as well as health policies and reimbursement decision.3,13,14 The usage of these tools has the advantages of reflecting impacts of interventions on important health-related quality of life (HRQoL). However, limitations remain with the data relying on validity, responsiveness and recall. A recent systematic review on outcome measures in orthopaedic trauma trials revealed that 41.6% of the trials did not clearly define what the primary outcome was or how it was measured. 1 Nearly half of the studies had a primary outcome focused on function following fracture care. Most common primary outcome used were patient or clinician reported function in 47.3% of studies, followed by adverse events in 11.9%, radiologic parameters in 11.1% and assessment of pain in 8.6%. The most common primary outcome measure was the Visual Analogue Scale (VAS) followed by radiographic bone-union. PROMs were used in majority of trials (68.5%). Oswestry disability index was used in 11.9% of studies. Overall, the capture of levels of capability, productivity levels or functional status is often lacking in the spinal trauma literature with few surgeons accounting for social well-being. 15
This brings us to reflect on the nature of spinal trauma and its impact on the patient and society. Spinal trauma is an acute event with acute loss of functioning compared to a pre-injury baseline status that has not been recorded. This disease characteristic is unique and different compared to degenerative spinal pathology. Best treatment should aim to return the patient to their preinjury state in the shortest amount of time (Figure 1). There are clear limitations that exist with the current outcome measures used. First, the lack of baseline makes comparative analysis or recovery trends difficult. Trauma patients express health in relation to their pre-injury status compared to degenerative disorders or diseases where health is expressed compared to perfect health. Pre-injury status and level of productivity differs between patients. It is likely inaccurate and methodologically unsound to assume that all patients have the same baseline. Future outcome measures could attempt to use each individual patient’s level of functioning as baseline for comparative studies or trend analysis. Treatment trajectories based on return to pre-injury level of functioning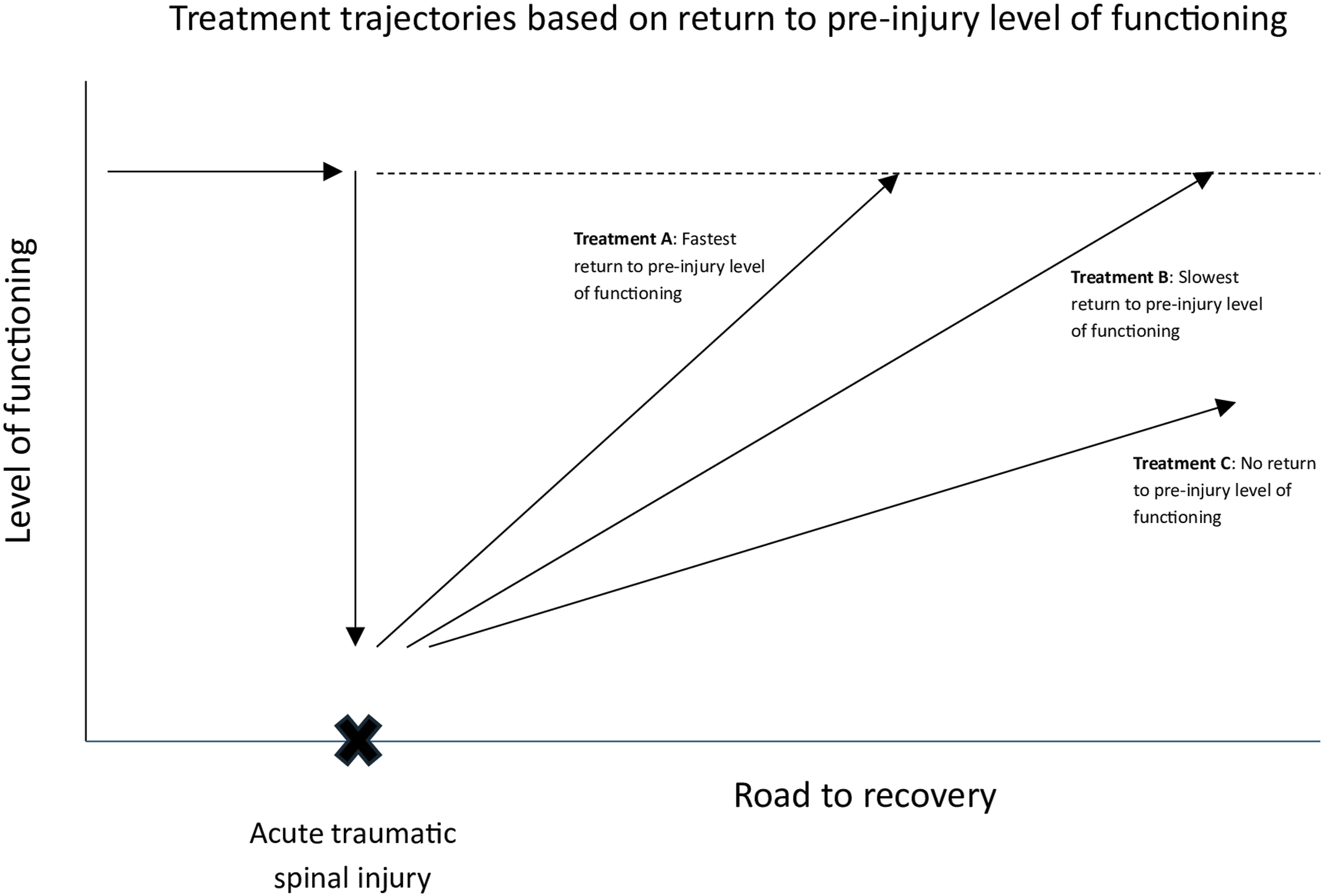
In the pursuit of determining best treatment, it is essential to be aligned with what is most important and meaningful for patients. For patients with spinal column injury without complete paralysis, loss of functioning and limitations in daily living is more important than pain. 10 This seemed to be true among all world regions studied. This shows that measuring recovery from trauma based on pain or radiographic characteristics may not be the best choice in TL burst fractures without neurological deficits. The ODI used in the AO A3A4 study relied on the impact of pain as a measure of disability. 16 In the hopes of solving the dilemma of outcome selection in spinal trauma research, the AOSpine Knowledge Forum Trauma initiated a project to develop and validate a disease-specific outcome instrument for spine trauma patients including both the patient’s and health professionals’ perspectives.17,18 The AO Spine PROST was designed to assess a broad range of aspects of functioning (eg, household activities, urinating, sexual function) on a 0 to 100 numeric rating scale with 0 indicating no function at all and 100 corresponding to the pretrauma functional level. Multivariate analysis showed significant independent determinants for a worse AO Spine PROST score: having one or more comorbidities, later return to work and no return to work. This evidence adds weight to the fact that the key is to assess if and when patients return to their prior level of functioning.
A real challenge in spinal trauma research is the unknown and unmeasured pre-injury baseline status. It then becomes inevitable to rely on recall to determine pre-injury level of functioning. Despite the AOSpine PROST being a validated and valuable tool, some limitations must be kept in mind with performing retrospective collection of PROMs in this format. This tool is subjected to recall bias like most retrospective collection, which can be subjective by nature and affected by mood, expectations, time and sentiments. External factors also come into play with treatment context, interactions with healthcare providers and patient’s socioeconomic status. Additionally, another barrier lies in finding appropriate and standardized time points for measurement amid the range of nonsurgical and surgical pathways. PROMs have demonstrated the prevalence of psychological distress and social concerns present in the trauma population, which account for the variation in symptom intensity and HRQOL scores. 15 When completing the AO PROST, patients are asked to rate on a scale whether they function as well as before their accident. The creation of future outcome tools should be based on assessing the time and the degree of return to preinjury baseline. Beyond this, efforts towards eliminating relying on subjective recall and shifting towards objective data collection regarding preinjury functional status is warranted. However, patient reported outcomes play an imperative role in evaluating the superiority of a treatment strategy. Their usage will continue to increase as healthcare standards and policies are increasingly being driven by patient satisfaction, engagement and shared decision-making.
Ultimately, epidemiological challenges remain in spinal trauma research. In 1948, the World Health Organization (WHO) defined health as “a state of complete physical, mental and social well-being and note merely the absence of disease or infirmity”. 19 This supports the proposed direction of outcomes selection towards measuring the path to recovery and solving the lack of baseline. Learnings from the AO A3A4 study should guide future investigations. The paucity of validated outcome tools in trauma is a problem that the academic spinal surgery community should tackle. An important and valuable first step has been taken with the AO PROST tool. Trauma represents an acute life-threatening event leading to loss of function, which is significant given the majority of spinal trauma occurring in the young and working population. Best treatment should return the patient to their preinjury state in the shortest amount of time. The next step in spinal trauma research is to solve how to best measure recovery in terms of return to pre-injury functional status.
Footnotes
Acknowledgements
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma, a focused group of international spinal trauma experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research. We would like to acknowledge Dr. Marcel Dvorak and his decade long dedication to this topic as the Principal Coordinating Investigator of the Thoracolumbar Burst Fracture Study Comparing Surgical Versus Non surgical Treatment (AO Spine TLA3–A4 Study).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma. Study support was provided directly through AO Network Clinical Research.