
Abstract
Study Design
Systematic literature review.
Objective
The management of traumatic thoracolumbar burst fractures (TLBF) remains challenging, and analyzing the levels of evidence (LOEs) for treatment practices can reform the decision-making process. However, no review has yet evaluated the operative management of traumatic thoracolumbar burst fractures with particular attention placed on LOE from an established methodology. The objective of the present study was to characterize the literature evidence for TLBF, specifically for operative management.
Methods
A comprehensive search of the English literature over the past 20 years was conducted using PubMed (MEDLINE). The inclusion criteria consisted of (1) traumatic burst fractures (2) in the thoracic or lumbar spine. Exclusion criteria included (1) osteoporotic burst fractures, (2) pathologic burst fractures, (3) cervical fractures, (4) biomechanical studies or those involving cadavers, and (5) computer-based studies. Studies were assigned an LOE and those meeting level 1 or 2 were included.
Results
From 1,138 abstracts, 272 studies met the criteria. Twenty-three studies (8.5%) met level 1 (n = 4, 1.5%) or 2 (n = 19, 7.0%) criteria. All 23 studies were reported.
Conclusions
The literature contains a high LOE to support the operative management of traumatic thoracolumbar burst fractures. For patients who are neurologically intact, a high LOE demonstrated similar functional outcomes, lower complication rates, and less costs with conservative management when compared with surgical management. There is a high LOE for short- or long-segment pedicle instrumentation without fusion and less invasive (percutaneous and paraspinal) approaches. Furthermore, the posterior approaches are associated with lower complications as opposed to the anterior or combined approaches.
Introduction
Traumatic spinal fractures can cause spinal instability with neurologic deficits. The majority of such fractures occur at the thoracolumbar junction (T11–L2), largely due to regional biomechanics in which the rigid, kyphotic thoracic spine is juxtaposed with the more mobile, lordotic lumbar spine. 1 Burst fractures account for 30 to 64% of the thoracolumbar spinal fractures. 1 , 2 Historically, burst fractures have been defined as involving the anterior and middle spinal columns based on the Denis three-column spinal model. 3 However, the more current classification of burst fractures utilizes the load-sharing classification. 4 Under the Magerl fracture classification system, burst fractures are designated as type A3 compression fractures. 2 The etiology is typically related to powerful axial compression forces, such as in falls from heights (34 to 54%), 1 , 5 motor vehicle accidents (51 to 65%), 1 , 5 or high-intensity sports (9%). 5 , 6 , 7 , 8 , 9
Despite an overwhelming amount of descriptive and clinical studies addressing traumatic thoracolumbar burst fractures, a significant controversy surrounds the optimum management strategies. This is reflected by the lack of uniformity in the treatment modalities. Typically, the management can be either operative or conservative: the former involves a combination of spinal fixation and fusion that may include interbody devices, with or without decompression, 1 , 10 , 11 , 12 , 13 , 14 , 15 , 16 , 17 and the latter incorporates the use of braces/casts, bed rest, analgesics, or observation with no bed rest or casts. 12 , 13 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 By extension, the algorithms to guide management decisions are limited, with one example being the Thoracolumbar Injury Classification and Severity Score. 25
With ambiguity regarding the best management, compiling and analyzing the levels of evidence (LOEs) for treatment practices can reform the decision-making process. The practice of evidence-based health care has gradually become more prevalent in modern medicine, as the pay-for-performance interventions with high LOE lead to greater reimbursements. 26 , 27 , 28 , 29 , 30 , 31 Systematic reviews (SRs) and meta-analyses provide the means to rapidly analyze a study's quality, ultimately facilitating the introduction of recommendation grades and providing a foundation for establishing practice guidelines. 32 To the author's best knowledge, there are currently seven SRs involving various aspects of traumatic thoracolumbar burst fractures. 13 , 16 , 33 , 34 , 35 , 36 , 37 However, no review has yet evaluated the operative management of traumatic thoracolumbar burst fractures with particular attention placed on the LOE from an established methodology. The current LOE for the operative management of traumatic thoracolumbar burst fractures remains unknown. Therefore, the objective of the present study was to characterize the literature evidence for traumatic thoracolumbar burst fractures, specifically by detailing the studies involving the operative management, with an LOE of 2 or greater.
Methods
A systematic literature review was conducted according to the Cochrane guidelines to capture all studies pertaining to traumatic thoracolumbar burst fractures over the past 20 years. 38 This time frame was arbitrarily predetermined, as the surgical management of burst fractures has greatly evolved during this period. An electronic search of PubMed (MEDLINE) was done on April 17, 2014 with permutations of the following terms: (“spine AND burst”) or “burst fracture” or (“burst and fracture”) or (A3 and fracture and spine). The inclusion criteria included: (1) burst fractures resulting from traumatic mechanism and (2) fractures of the thoracic or lumbar spine. The exclusion criteria were: (1) osteoporotic burst fractures, (2) pathologic burst fractures, (3) cervical fractures, (4) biomechanical studies or those involving cadavers, and (5) computer-based studies such as finite element analyses. Search results were blinded such that only the titles and abstracts were reviewed. When inclusion or exclusion was unclear, full texts were retrieved; if doubt remained, a decision was made through discussion and addition of a third reviewer if needed. Following the search, only those involving operative management were selected to be reviewed in the present study. They were categorized as operative versus nonoperative or as treatment/technique studies.
LOEs were assigned using criteria from the Journal of Clinical Orthopaedics and Related Research, 30 which is adapted from the Oxford Centre of Evidence Based Medicine LOEs. 39 , 40 The LOE scale ranges from 1 being the highest to 5 the lowest. Studies with level 1 or 2 LOE were classified as high LOE. Ambiguities regarding LOE were resolved through discussion and addition of a third reviewer if needed. Once all the studies were assigned a LOE, only those rated as level 1 and 2 were included. All data were stored in Microsoft Excel 2013 (Microsoft Corp., Redmond, Washington, United States).
Results
Overall Composition of the Literature
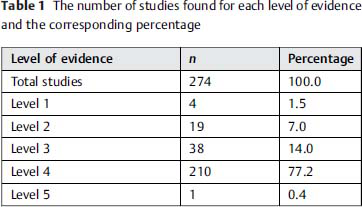
The search yielded a total of 1,138 abstracts, of which 272 met the criteria, involved operative management, as well as were published between January 1, 1992, and April 17, 2014. Twenty-three of the studies (8.5%) met level 1 (n = 4, 1.5%) or 2 (n = 19, 7.0%) criteria (Table 1).
The number of studies found for each level of evidence and the corresponding percentage
Operative versus Nonoperative Management
Fifteen of the studies (5.5%) investigated the differences between operative versus nonoperative treatment. Of these, seven qualified as high LOE (two level 1, five level 2; Table 2). All others were classified as level 3 (n = 6) and level 4 (n = 2).
Studies (n = 23) with high level of evidence
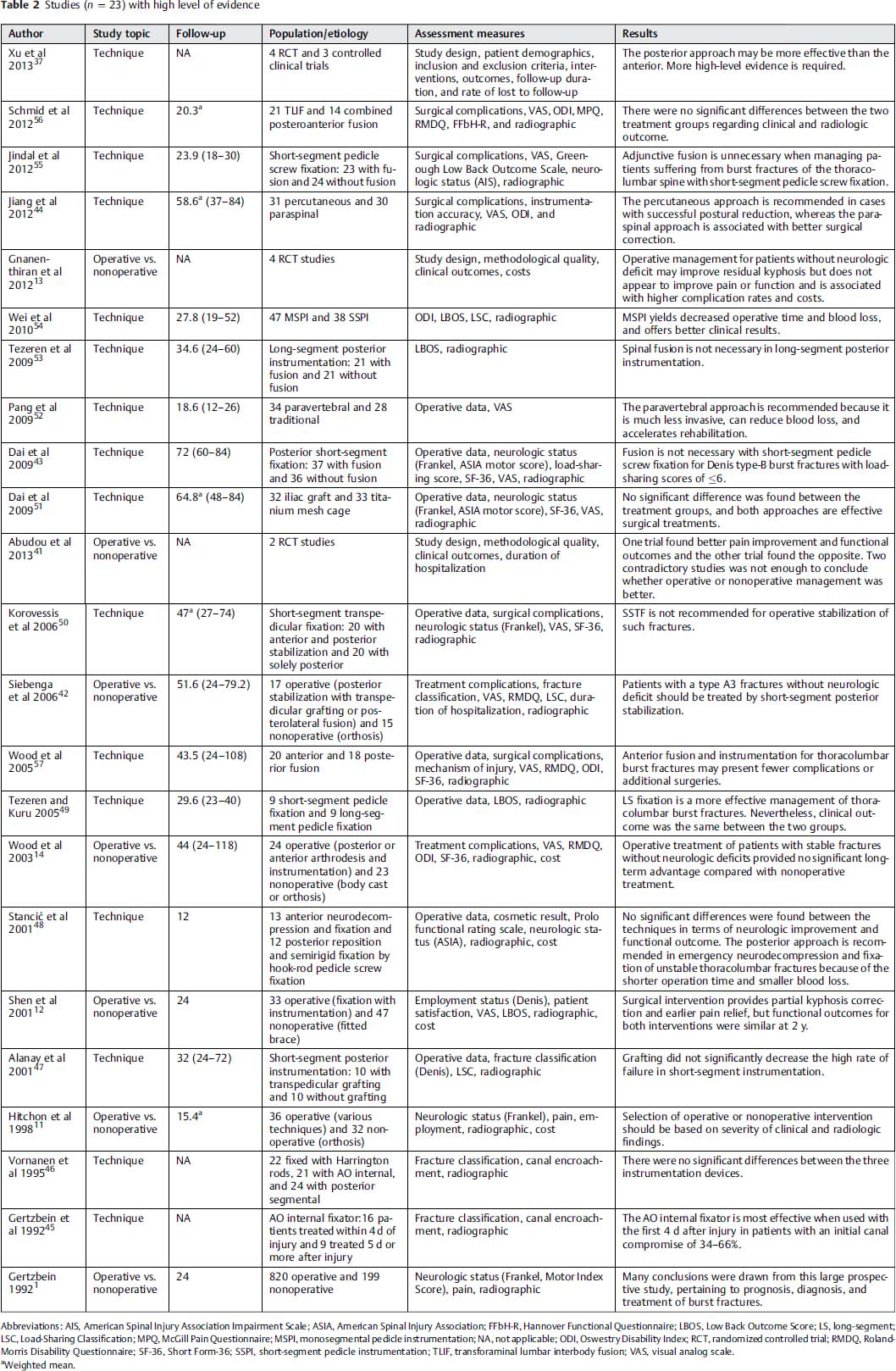
Abbreviations: AIS, American Spinal Injury Association Impairment Scale; ASIA, American Spinal Injury Association; FFbH-R, Hannover Functional Questionnaire; LBOS, Low Back Outcome Score; LS, long-segment; LSC, Load-Sharing Classification; MPQ, McGill Pain Questionnaire; MSPI, monosegmental pedicle instrumentation; NA, not applicable; ODI, Oswestry Disability Index; RCT, randomized controlled trial; RMDQ, Roland-Morris Disability Questionnaire; SF-36, Short Form-36; SSPI, short-segment pedicle instrumentation; TLIF, transforaminal lumbar interbody fusion; VAS, visual analog scale.
Weighted mean.
Two studies—one SR and one randomized controlled trial (RCT)—met level 1 criteria. Abudou et al reported an SR through the Cochrane collaboration in which they searched for RCTs comparing operative and nonoperative treatment in patients without neurologic deficit. 41 Due to strict inclusion and exclusion criteria, only two studies with contrasting results were identified (Siebenga et al and Wood et al, discussed below), 14 , 42 leading the authors to conclude that there is insufficient evidence to conclude whether surgical or conservative treatment yields superior functional outcomes. 41 The second study was an RCT reported by Siebenga et al that compared the radiographic and functional outcomes in neurologically intact patients with burst fractures. The operative cohort underwent short-segment posterior pedicle screw fixation above and below the fracture level with an autologous fusion; the nonoperative treatment involved rehabilitation and bed rest for ≥5 days following the injury. All patients wore a Jewett hyperextension orthosis for 3 months. Although both the patient groups had similar baseline local and regional sagittal angles and visual analog scale scores, the surgery resulted in significantly lower angles and less pain at the final follow-up. Further, the authors reported that the conservative treatment led to higher Roland Morris Disability Questionnaire-24 (RMDQ-24) scores at the final follow-up, with fewer patients capable of returning to work. 42
Five studies met the level 2 criteria. In 1992, Dr. Gertzbein and the Scoliosis Research Society prospectively analyzed spinal fractures in 1,019 patients across 12 countries. Operative intervention was administered to 545 patients and 96 received conservative therapy. The results revealed a statistically significant, albeit weak, relationship between the initial canal compromise and the neurologic deficit in burst fractures. However, there were no differences in the rates of the neurologic improvement between the treatment groups. Of the operative patients, the neurologic outcomes were equivalent for anterior versus posterior surgery. Among patients with preoperative neurologic deterioration, surgical management, particularly anterior surgery, led to greater improvement. At 2-year follow-up, a higher proportion of patients managed conservatively complained of “severe/moderate” pain compared with “none/mild” pain. 1 Hitchon et al performed a prospective study to outline the indications, benefits, and costs of bed rest compared with surgical stabilization with pedicle screws, rods, and plates; Luque or Harington rods with sublaminar wiring; or an “anterior spinal device.” All patients were immobilized in thoracolumbar orthoses for 3 to 5 months. Although both cohorts improved neurologically, a progressive angular deformity was present, with rates twice as high in the surgery group. 11
Shen et al conducted an RCT to examine nonoperative treatment (a hyperextension brace for 3 months without fracture reduction) versus short-segment posterior fixation. Although the surgical group had better pain and clinical outcomes in the early postoperative period (3 to 6 months), these differences were not observed at final follow-up (2 years). Regarding kyphosis correction, the operative group had an initial correction of 17 degrees, which was lost over time, and the nonoperative group had a loss of 4 degrees. Also, hospital charges were 4 times greater with surgery. 12 Wood et al reported another RCT in which nonoperative patients underwent a fracture reduction supplemented by a body cast or a thoracolumbar orthosis for 3 months. The operative patients underwent either a posterolateral spinal arthrodesis with pedicle screw and hook instrumentation and autologous bone grafting or an anterior two-level fibular and rib-strut construct arthrodesis with local autologous bone grafting and instrumentation. Both groups were similar at final follow-up with respect to the radiographic and clinical outcomes. 14 A level 2 meta-analysis reported by Gnanenthiran et al pooled the results from the four aforementioned trials. No differences in the clinical outcomes of pain and function were seen. The surgical group, however, did show better correction radiographically at follow-up, albeit this came with higher complication rates and costs. 13
Treatment and Technique
Two hundred fifty-seven studies (9.5%) examined the operative treatment and technique of thoracolumbar burst fractures. There were 16 high LOE studies (two level 1, 14 level 2; Table 2), and the rest were level 3 (n = 32), level 4 (n = 208), and level 5 studies (n = 1).
Both level 1 studies were prospective RCTs. Dai et al investigated posterolateral fusion in combination with short-segment posterior pedicle screw instrumentation into the levels cephalad and caudad to the fractured vertebra. A total of 37 patients underwent fusion and36 did not, and no differences in the radiographic or clinical outcomes were seen. 43 In the second study, two muscle-sparing surgical approaches—the percutaneous and paraspinal approaches for pedicle screw and rod fixation—were compared by Jiang et al for efficacy and safety. The percutaneous approach led to lower intraoperative blood loss, shorter surgical time, and shorter hospitalization. In the short-term postoperative period, this approach also yielded less pain and greater improvements in the functional scores. In contrast, the paraspinal approach resulted in better correction of the kyphosis and restoration of the vertebral height. The long-term clinical outcomes were equivalent. 44
The first level 2 study was published by Gertzbein and colleagues, in which 25 patients were treated with the AO internal fixator before or after the first 4 days postinjury. Earlier intervention led to greater improvement in canal encroachment. 45 Vornanen et al compared three methods of internal fixation (Harrington rods, AO internal fixators, posterior segmental fixators) with respect to improvement in canal encroachment. All methods improved encroachment, with Harrington rods providing the best reduction. 46 Next, Alanay et al reported an RCT comparing short-segment pedicle instrumentation with or without transpedicular grafting. No differences in the radiographic, operative, pain, or functional outcomes were seen. 47
Stancić et al compared anterior and posterior surgical approaches for overall clinical outcomes and operative efficacy. Of the 25 patients enrolled, 13 received anterior neurodecompression and fixation and 12 underwent posterior fixation by hook and rod and pedicle screw fixation. Neither the neurologic outcomes nor economic/functional outcomes proved to be different. However, the posterior group suffered less blood loss and had shorter operative times, better aesthetic outcomes, and lower costs, complications, and donor site pain. 48
Tezeren and Kuru performed a prospective study in which patients were treated with short- or long-segment pedicle fixation. 49 The short-segment fixation involved fixation one level above and below the fracture; long-segment instrumentation involved hook fixation two or three levels above plus pedicle fixation two levels below the fracture. At final follow-up, patients in the long-segment group showed significantly better correction of the sagittal index and anterior body compression. 49 Wood and colleagues compared anterior reconstruction, fusion, and instrumentation to posterior fusion with instrumentation. 57 Although the posterior approach had significantly less blood loss, no differences in radiographic, clinical, and functional outcomes were observed. In a prospective randomized trial by Korovessis et al, patients received a combined anterior and posterior stabilization technique or standard posterior short-segment transpedicular fixation. Both resulted in radiographic improvement but the combined group faced greater blood loss, operative time, complications, and duration of hospital stay. Furthermore, visual analog scale and SF-36 scores did not correlate with the anatomical correction in either treatment group. 50
Dai et al prospectively evaluated the outcomes following anterior-only stabilization with either structural autografts or titanium mesh cages. Apart from the differing instrumentation, the surgical approaches were similar between the groups. In the autograft group, the operative times were longer but no other differences were observed. Both the treatment groups improved postoperatively and there were no significant differences. 51
In 2009, Pang et al prospectively compared the outcomes and surgical efficiency/safety between an approach via the paravertebral muscle or the traditional posterior approach. The paravertebral muscle approach led to significantly better outcomes in terms of blood loss, drainage, duration of recumbency, and clinical outcome scores. 52 Tezeren et al prospectively investigated long-segment instrumentation with or without fusion. The average operation time and blood loss were significantly lower in the nonfusion group, but the two groups were otherwise similar in terms of the radiologic and clinical assessment measures that were analyzed. 53
Wei and colleagues published a clinical trial in 2010 comparing the clinical and radiologic outcomes between monosegmental transpedicular fixation and short-segment pedicle instrumentation. Patients were analyzed based on the operative data, Low Back Outcome Score (LBOS), Oswestry Disability Index, Load-Sharing Classification, sagittal index, and percentage of anterior body height compression. Monosegmental fixation resulted in lower operative times and blood loss but did lead to higher LBOS scores. 54 The groups were also similar at final follow-up for the sagittal index, local kyphosis, and average correction loss. Following this, in 2012, Jindal et al assessed the benefits of short-segment pedicle fixation with or without fusion in an RCT. Ultimately, the fusion did not improve the radiographic or functional outcomes but did increase the operative time and necessity for blood transfusion. 55 Schmid et al prospectively compared thoracoscopy or transforaminal lumbar interbody fusion (TLIF) in the anterior reconstruction of burst fractures. The TLIF group received a monocortical strut graft and the thoracoscopy included tricortical strut grafts or titanium vertebral body-replacing implants. Satisfactory outcomes were achieved in both groups, and no differences were seen in the radiographic or clinical outcomes. Surgical decompression, however, was higher with TLIF. 56
In 2013, Xu et al performed a meta-analysis of RCTs, quasi-RCTs, or controlled trials investigating anterior versus posterior approaches in attempt to identify the optimal approach. 37 The authors analyzed seven studies comparing 179 and 152 patients in the anterior and posterior groups, respectively. No significant differences were found between the approaches for neurologic recovery, return to work, complications, and deformity correction. However, the anterior group was associated with longer operative time, greater blood loss, and a higher cost than the posterior approach.
Discussion
Traumatic thoracolumbar burst fractures remain a challenge to treat, and optimal operative and nonoperative techniques have not yet been established. The goals of treatment are to obtain early patient mobilization and a painless, balanced, stable vertebral column with maximum spine mobility and optimal neurologic function. To achieve these goals, numerous studies have investigated different diagnostic, prognostic, and management approaches, with a greater emphasis in the latter. The present study attempted to characterize the high LOE studies pertaining to the operative management of traumatic thoracolumbar burst fractures and found that the overall literature contained 23 studies (8.5%) in PubMed that met an LOE of 1 or 2.
When treating neurologically intact patients with thoracolumbar burst fractures, there is no difference in the clinical outcomes when comparing a conservative or open operative approach. This is supported by five of the seven high-level studies investigating this cohort. Although better correction of the spinal deformity can be achieved surgically, three level 2 clinical studies demonstrated higher rates of complications and costs with this approach. Two high-level SRs confirmed no difference in the functional outcomes when the approaches were compared. These studies utilized different operative and conservative approaches, follow-up times, and inclusion/exclusion criteria. It is worth noting that there are limited numbers of patients in these studies and thus their results are inherently limited.
There is a high LOE for short- or long-segment pedicle instrumentation without fusion. Tezeren and Kuru compared short- versus long-segment pedicle fixation in a level 2 study and concluded that better correction can be achieved with the long construct, and LBOS outcomes were similar. 49 Longer constructs provide the necessary rigidity to decrease failure rates, but they also decrease patient mobility due to the more rigid fixation, which may impact quality-of-life parameters that were not assessed. Four high-level studies questioned the necessity of additional fusion to posterior short-segment pedicle instrumentation. Dai et al (level 1), Alanay et al (level 2), and Jindal et al (level 2) demonstrated that bone grafting was not necessary in short-segment pedicle instrumentation in RCTs. 43 , 47 , 55 Tezeren et al (level 2) also demonstrated that fusion did not change the radiologic or clinical outcomes in long-segment instrumentation. 53 The operative time would decrease by forgoing fusion, and because bone graft is not needed, this would collectively decrease the risk of infections. As mentioned previously with studies involving neurologically intact patients, the discussed RCTs also have small sample sizes and the conclusions from these studies should be considered within the context of that limitation.
Open approaches to spine surgery are associated with higher morbidity, and there has been a recent trend toward preserving thoracolumbar muscle attachments. The percutaneous and paraspinal approaches to thoracolumbar burst fractures are supported by level 1 and 2 studies. Pang et al (level 2) demonstrated that the paravertebral approach results in better clinical outcome scores than the traditional posterior approach. 52 Jiang et al (level 1) demonstrated that shorter hospitalization time and equal 3-year clinical outcomes can be achieved with the percutaneous versus paraspinal approach in pedicle screw and rod fixation. 44 However, better deformity correction can be achieved with the paraspinal approach.
When investigating an anterior, posterior, or combined approach in instrumentation, four level 2 studies reported similar radiographic, clinical, and functional outcomes. 37 , 48 , 50 , 57 Furthermore, when compared with the anterior or combined approach, the posterior approach correlated with fewer complications and operative risks. When considering anterior reconstruction, Dai et al demonstrated no significant differences in the use of titanium or autologous grafting for fusion. 51 Furthermore, Schmid et al demonstrated that transforaminal lumbar interbody fusion may provide further surgical decompression than thoracoscopy. 56 And finally, Xu et al performed a meta-analysis and found similar results with the exception that the anterior approach also had a higher cost associated with it. 37 The choice of the operative approach can be decided by the preference of the surgeon and patient, while acknowledging that greater risks and possible higher costs are associated with the anterior approach.
Additional considerations in the operative management of traumatic thoracolumbar burst fractures include both the correction of a kyphotic deformity and the potential loss of a kyphotic correction over time. The results regarding whether operative management maintained the correction more successfully than nonoperative management are mixed. 12 , 14 , 42 All studies show a significant improvement postoperatively; however, in the study by Siebenga et al (level 1), 42 the operative group maintained the correction and the kyphosis was significantly less than in the nonoperative group at final follow-up (a mean of 4.3 years). On the other hand, Shen et al (level 2) and Wood et al (level 2) did not show any differences in the deformity correction between operative and nonoperative management at the final follow-up (2 years). 12 , 14 The clinical implication of kyphotic correction is questionable, as Wood et al (level 2) and Korovessis et al (level 2) both did not find any correlation between the degree of kyphosis at the final follow-up and the degree of pain or disability. 14 , 50 Operative management does improve pain and stability. 12 , 13 , 14 , 16 , 42 Most studies had similar radiographic results between the various operative techniques. 37 , 43 , 47 , 51 , 53 , 54 , 55 , 56 , 57 Specifically, fusion does not appear to affect the maintenance of radiographic correction as demonstrated by four high LOE studies. 43 , 47 , 53 , 55 However, Jiang and colleagues (level 1) found better long-term local kyphosis correction with a paraspinal approach versus a percutaneous. 44 Similarly, Tezeren and Kuruet (level 2) found better kyphotic correction at final follow-up for patients who underwent long-segment pedicle fixation compared with short-segment fixation. 49
The heterogeneity nature of burst fractures due to the different mechanisms of injury results in a variety of clinical presentations, and makes it difficult to formulate a universal approach. Other SRs were limited to select studies by the strict inclusion/exclusion criteria and therefore did not include most of the literature covered in this report. This report was conducted in accordance with the Cochrane Collaboration Handbook on SRs; it highlights the current evidence and provides further insight into future investigations needed. This review is limited by studies found only in the PubMed database (MEDLINE). However, the MEDLINE database is well accepted as the comprehensive source of relevant literature.
Conclusion
The literature contains a high LOE to support the operative management of traumatic thoracolumbar burst fractures. The highest degree of controversy involves the decision whether to operate on neurologically intact patients. For patients who are neurologically intact, a high LOE demonstrated similar functional outcomes and lower complication rates and costs with conservative management when compared with surgical management. However, the evidence is unclear when there is a neurologic deficit. If a patient is determined to require surgery, there is no general consensus on the appropriate technique to be used. There is a high LOE for short- or long-segment pedicle instrumentation without fusion and less invasive (percutaneous and paraspinal) approaches. Furthermore, posterior approaches are associated with fewer complications as opposed to anterior or combined approaches.
Funding
No funding was used for this study.
Disclosures
Justin K. Scheer, none
Joshua Bakhsheshian, none
Shayan Fakurnejad, none
Taemin Oh, none
Nader S. Dahdaleh, none
Zachary A. Smith, none