
Abstract
Study Design:
Broad narrative review.
Objectives:
Translaminar screw (TLS) fixation was first described as a salvage technique for fixation of the axial spine. Better understanding of the spine anatomy allows for advancement in surgical techniques and expansion of TLS indications. The goal of this review is to discuss the anatomic feasibility of the TLS fixation in different region of the spine.
Methods:
A review of the current literatures on the principles, biomechanics, and clinical application of the translaminar screw technique in the axial, subaxial, and thoracolumbar spine.
Results:
Anatomic feasibility and biomechanical studies have demonstrated that TLS is a safe and strong fixation methods for fusion beyond just the axial spine. However, not all spine segments have wide enough lamina to accept TLS. Preoperative computed tomography scan can help ensure the feasibility and safety of TLS insertion. Recent clinical reports have validated the application of TLS in subaxial spine, thoracic spine, hangman’s fracture, and pediatric population.
Conclusions:
TLS can be used beyond axial spine; however, TLS insertion is only warranted when the lamina is thick enough to avoid further complications such as breakage. Preoperative computed tomography scans can be used to determine feasibility of such fixation construct.
Introduction
Posterior upper cervical screw instrumentation has become the most widely used technique as it provides high fusion rates without a prolonged external immobilizer. For subaxial cervical spine, lateral mass screws (LMS) have been used among a vast majority of spine surgeons because LMS have shown to provide excellent stability with high fusion rates. 1 –4 Pedicle screws in the subaxial cervical spine have also been used with strong biomechanical properties. 5 Pedicle screws are especially useful if patients need any cervical deformity correction. 6 However, the usage of pedicle screws in subaxial cervical spine can be limited by the small size of the cervical pedicle and its close proximity to vertebral artery and spinal cord. 7,8 That is probably the reason LMS are still more widely used in the subaxial cervical spine.
Stabilization of the atlantoaxial spine can be challenging because of its unique anatomy. Early methods involving posterior cervical wiring of the C1 and C2 lamina were pioneered by Gallie. 9 Despite providing adequate stability in flexion and extension, this technique resulted in poor stabilization of rotational movements and was associated with high nonunion rates. 10 Several modifications have been proposed to improve posterior wiring, including the wedge compression method developed by Brooks and Jenkins 11 and the interior spinous method developed by Dickman et al. 12 Although these techniques are relatively simple procedures, the unsatisfactory fusion rate and need for rigid external immobilization prompted the need for a new approach. 13 Transarticular screw fixation, first described by Jeanneret and Magerl, 14 provides complete immobilization of rotational movement about the atlantoaxial joint. 14 However, this method poses great technical challenges with potential serious complications such as vertebral artery injury if it is high riding. Therefore, Goel et al 15 first described the use of a C1 lateral mass screw (LMS) and C2 pedicle screw construct. Early attempts using this method provided high rates of fusion with a low incidence of complications. 16 However, with any anatomical variation, C2 pedicle screws or pars screws are not always feasible. Given these constraints, Wright 17,18 developed a novel technique using a screw-rod construct with C2 translaminar screws (TLS) for atlantoaxial fixation. This approach has gained increasing use, especially when used as a salvage technique as it reduces the risk of vertebral artery injury, eliminates the need of navigational instruments, and achieves comparable stability and fusion compared to other traditional means of fixation. 18 –21
Most recently, there have been trials to expanding the use of translaminar screws in subaxial cervical as well as thoracolumbar spine. 22 –24 The main challenge with TLS outside the axial spine exists because of the longer length yet narrower width of lamina in these regions. However, with advanced imaging and improved understanding of the spinal anatomy, TLS has been shown to be a feasible option. With many individual reports of new advancement in TLS, there is paucity in current literature providing comprehensive overview of TLS utility in the entire spine. The purpose of this review is to discuss the principles, biomechanics, and clinical application of the TLS in the axial, subaxial, and thoracolumbar spine.
Methods
A PubMed search was conducted on December 9, 2017, using the key words “translaminar screw” and “spine.” A total of 166 records were found (Figure 1). References of the relevant articles were checked for additional articles and all bibliographies of the included articles were hand-searched to identify further relevant literature. Two investigators (JJC, NS) screened studies independently for eligibility, summarized key findings, and synthesized a comprehensive review of the current literatures on the principles, biomechanics, and clinical application of the TLS technique in the axial, subaxial, and thoracolumbar spine.
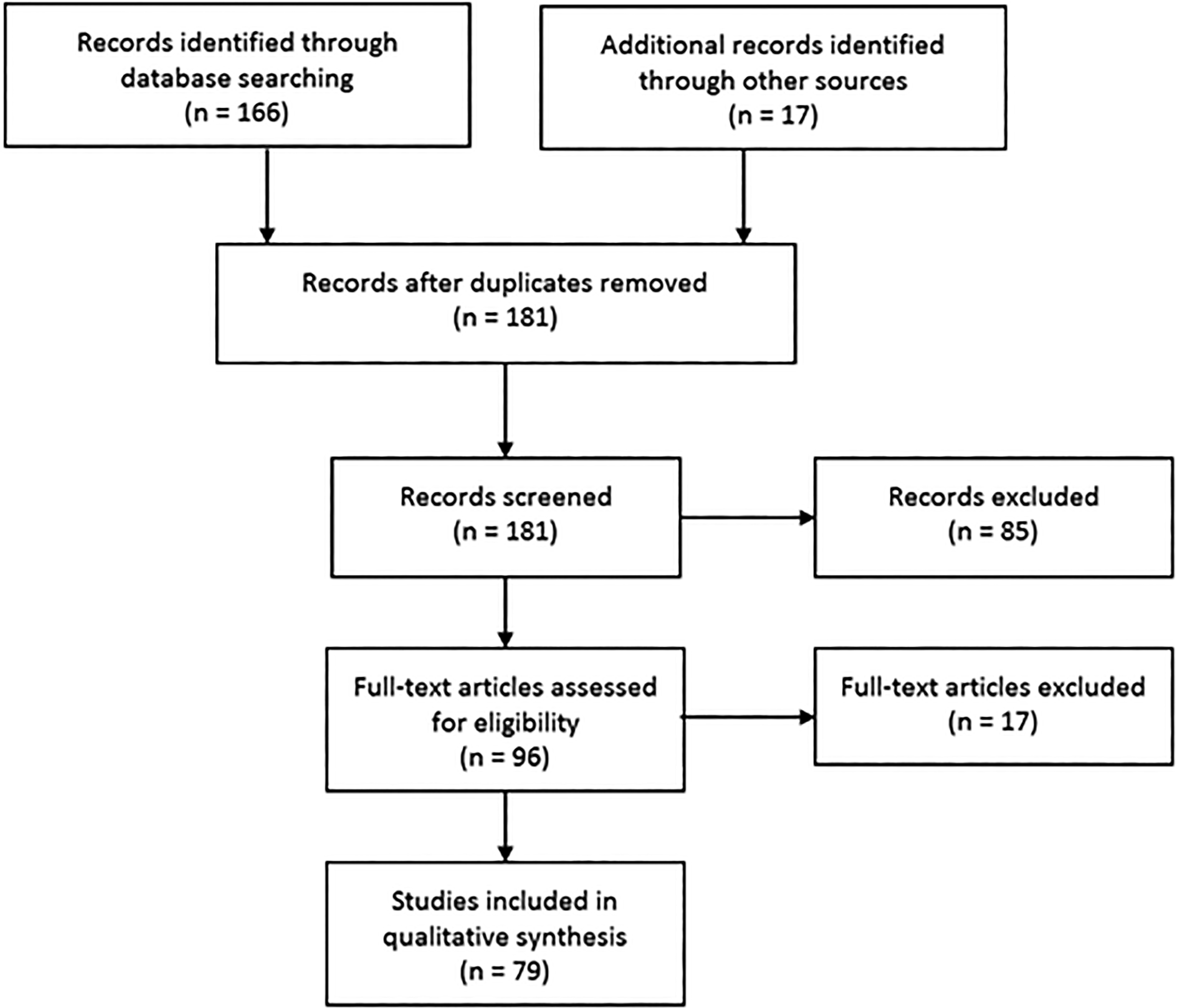
Flowchart using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Principles of TLS Fixation
Anatomic Feasibility
Axial Spine
An understanding of laminar anatomy, including size, trajectory, and relation to surrounding structures is crucial to ensure safe screw placement. An early study by Xu et al 25 examined the lamina from C2-L5 in 37 spines. At C2, the authors found a mean laminar thickness of 4.3 ± 0.9 mm; however, their measurements that were based on the mid-portion of the spinous process to the medial border of the facet were not particularly applicable for laminar screws, in which a minimum thickness is critical to determine whether the lamina can safely accept screw placement.
Further studies following popularization of TLS using cadaveric specimens have addressed this issue with regards to anatomic applicability. In a study of 420 C2 lamina, Cassinelli et al 19 found a mean thickness of 5.77 ± 1.31 mm, with 92.6% and 71% having a thickness of ≥4.0 mm and ≥5.0 mm, respectively. While their data suggests high rates of screw acceptance, lamina thickness exhibited a wide range (1.35-9.77 mm), indicating considerable anatomic variability. Wang 26 reported similar morphologic variability of C2 lamina in his smaller study of 38 cadaveric specimens. While the mean cross sectional laminar area was 75.2 mm2, only 79% and 48% of lamina had a mean thickness of 5.5 and 6.0 mm, respectively, which corresponded to a 3.5 or 4.0 mm screw with 1-mm tolerance on either side. Again, the cranial-caudal dimension consistently exhibited a greater mean thickness compared to that of the ventral-dorsal diameter, suggesting an increased risk of dorsal, or worse ventral breakthrough during screw insertion. Given this variability, Wang 26 advocated for the use of preoperative computed tomography (CT) imaging to characterize the desired lamina and ensure feasibility prior to using TLS technique.
Another important consideration to minimize the risk of ventral breakthrough is the laminar inclination angle that guides screw trajectory. It is often defined by the angle at the spinolaminar junction formed by the lamina and spinous process in an axial plane. 19 Reported values have ranged from 41° to 49° with less variation compared with that of laminar thickness. 19,26 –29
To accommodate bilateral screws the cranial-to-caudal distance of the spinous process, or spinal height, must also be sufficient to serve as the screw entry point. While it is rarely a limiting factor with unilateral screws, it is an important consideration when using bilateral TLS that must transect in the coronal plane. In a cadaveric study of 120 C2 vertebrae, Ma et al 29 reported that only 2.5% of samples had a spinous process height of ≤9 mm, which is the distance needed for two 3.5-mm screws with 1-mm tolerance in each direction. 29
This does not hold true in the pediatric population where anatomic acceptance of bilateral screws appears to be age dependent. Using CT, Chern et al 30 studied cervical lamina in relation to translaminar screws in 69 pediatric patients aged between 1.5 and 16 years. 30 The authors found that similar to adults, the C2 is one of the largest lamina in the cervical region. However, rates of bilateral TLS acceptance based on a minimum laminar height of ≥9 mm and thickness of ≥4.5 mm were significantly lower at 30.4%. When stratified by age, acceptance rates increased to 45.9% in those patients aged 8 years and older, suggesting significant age-related changes. Others have supported this age dependent relationship, and specifically variations in laminar thickness with differing ages in the pediatric population that precludes the use of bilateral TLS in very young patients but are favorable for unilateral screws. 27,31
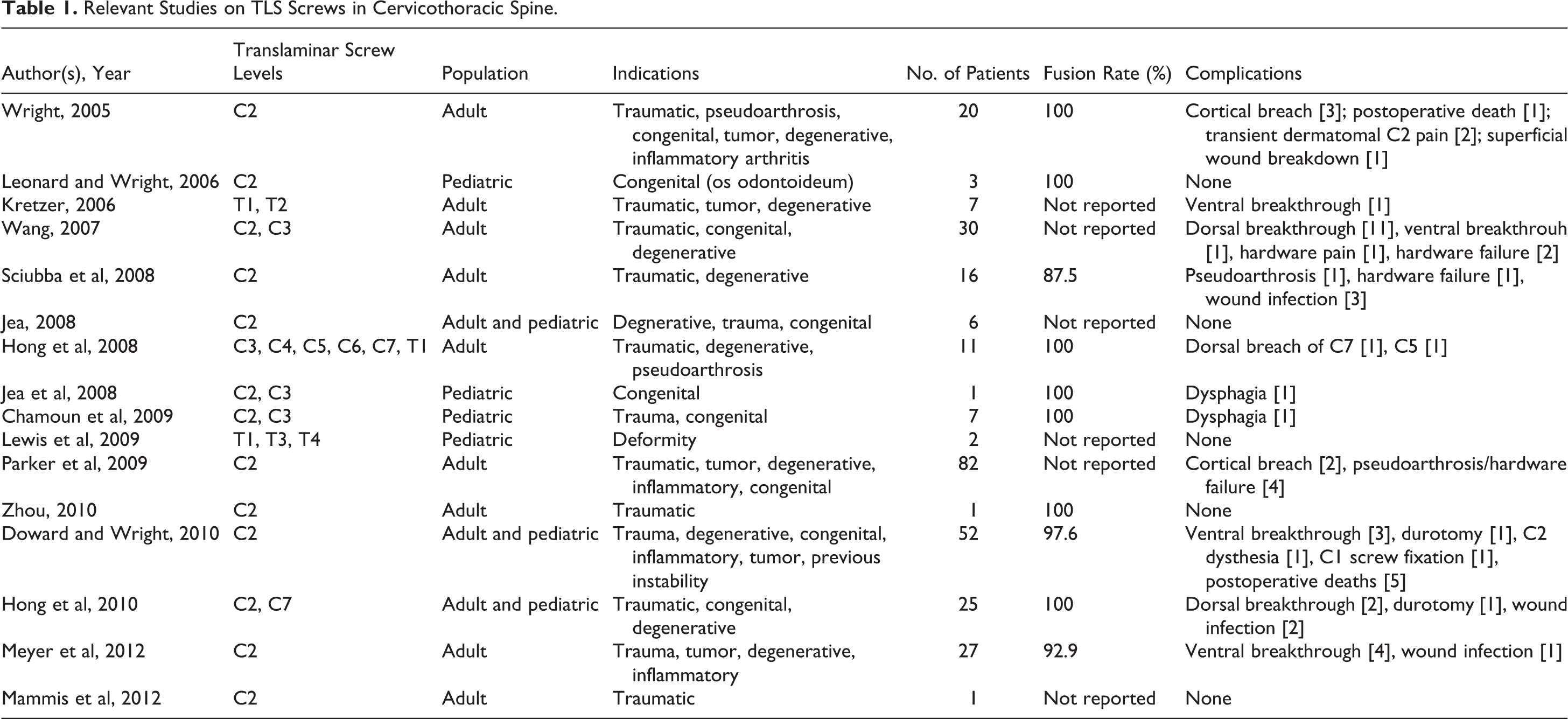
One proposed benefit of TLS is that it decreases the risk of neurovascular injury, and specifically that to the vertebral artery compared with other methods of posterior fixation. Since gaining popularity, there have been no reported complications related to perioperative vertebral artery injury, but careful preoperative planning is still necessary to decrease the risk of vertebral artery injury (Table 1). Riesenburger et al 32 evaluated 100 C2 laminae using CT angiography with simulated screw trajectories in which the screws transversed the entire lamina and entered the lateral mass achieving maximal bony purchase. The authors reported a potential risk for vertebral artery injury in 55% of these cases, with an average of 5.6 mm between the screw tip and vertebral artery in high-risk instances. While this risk increased with increasing screw length, they noted that screws less than 28 mm were safe in all samples. 32
Relevant Studies on TLS Screws in Cervicothoracic Spine.
Subaxial Spine
Compared with C2, the laminar anatomy of the subaxial spine with the exception of C7 often limits the use of translaminar screws as a reliable and safe method of fixation without careful preoperative planning. Using CT analysis, Yusof et al. studied a total of 1,176 lamina from C2-C7. 33 The authors reported a decrease in mean laminar thickness from C2 to C4/5, which had the smallest diameters of 3.1 mm, before increasing caudally toward C7. This translated to acceptance rates less than 50% for C3-C6 using a diameter cutoff of ≥4.0 mm, and less than 16% when the cutoff was increased to ≥5.0 mm. This is compared with the high rates of screw acceptance for C2 and C7, which were 94/75% and 100/79%, respectively. Alvin et al 34 reported similar results in their extensive study of laminar anatomy from C3-C7 in 50 patients using CT morphometric and volumetric analysis. Again, dimensions were noted to decrease to C5, which was shown to have the smallest laminar thickness and shortest laminar height and increase toward C7. While unilateral acceptance rates were slightly higher, ranging from 12% to 84% from C3-C6, both C5 and C6 could not accept bilateral translaminar screws due to insufficient laminar thickness. Cho et al 35 conducted CT morphologic analysis of subaxial lamina correlated with simulated screw trajectory in 18 cadaveric spines and reported the anatomy of the lamina of subaxial cervical spines. Most cervical spine segment did not allow insertion of 2 screws except in C7. Most recently, the same authors conducted feasibility study of TLS in the subaxial spine. They found that 13% of 1° screws and 33% of 2° screws violated medial cortex. The authors concluded that TLS in subaxial cervical spine is feasible only with thick lamina or C7, and they do not recommend routine use except in certain salvage situations. If translaminar screws are only available option for the fixation of subaxial cervical spine, they advised to pursue preoperative CT scan to ensure safety. 36
Thoracic Spine
With the increasing use of translaminar screws beyond the axial spine, consideration is being given to other segments that can safely accommodate screw placement. 37 Compared with the pedicles in the upper thoracic spine, which are relatively short and intimately related to exiting nerve roots, thoracic lamina may offer less anatomic limitations. 38,39 Cho et al 40 inserted TLS screws into thoracic spine in 15 cadaveric spines using 4-mm dimeter screws from T1-T6 and 3.5-mm diameter screws from T7-T12. 40 All screws were successfully inserted in separated spine group (total of 147 vertebral levels) and confirmed with CT image. In nonseparated group, 4 inner cortex breakages and 3 outer cortex breakages were found on CT scan. The authors concluded that TLS can be safely inserted into the thoracic spine (Figure 2).
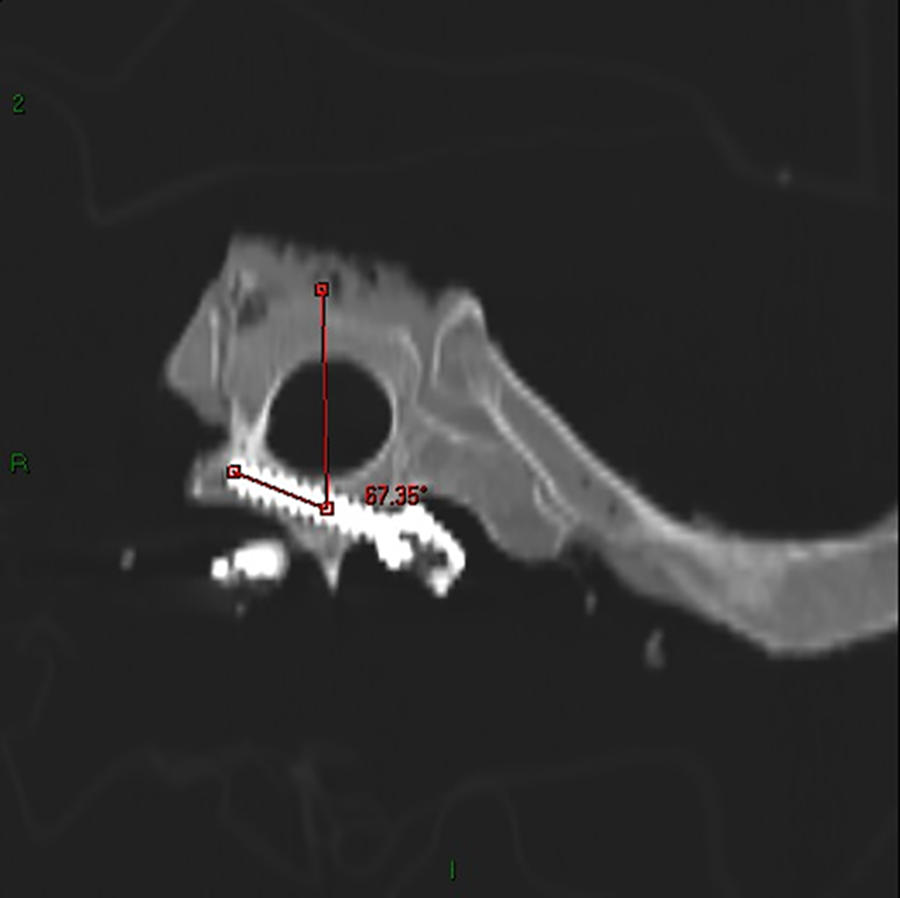
Computed tomography scan of thoracic spine demonstrating safe placement of translaminar screw.
Kretzer et al 41 used CT-based analysis to characterize the width, screw length, and screw trajectory in 100 upper thoracic spines. They found that both T1 and T2 had surprisingly high acceptance rates of 97% and 99%, respectively, which were similar to those for pedicle screw acceptance rates at the same level (99% and 94%). The authors did note an increase in laminar length and decrease in laminar width in T1 versus T2, which is an important consideration when determining the optimal screw size at each level. Additionally, the spinolaminar angle used for screw trajectory was noted to be slightly greater than that in the cervical spine.
Patel et al 42 reported that TLS fixation was also a feasible option for upper thoracic fixation in the pediatric population. Using CT morphometric analysis, the authors studied lamina from T1-T4 in children aged 3 months to 17 years. As appears to be the case with the subaxial spine, laminar dimensions including height, width, and length differed significantly with age with a 100% bilateral TLS acceptance rate at T1-T4 in patients aged 4 years and older compared with roughly 50% in patients 1 to 3 years and less than 50% in patients younger than 1 year. Again, T1 was noted to have the greatest length necessitating a longer TLS screw with spinothlamic angles ranging from 47° to 53°.
Lumbar Spine
Although TLS has been placed in lumbar spine, limited feasibility data exists in this region. Sasso et al 43 performed 10 percutaneous computer-assisted TLS insertion in a human cadaver. Post-CT examination demonstrates 5 grade-0 placement and 5 grade-I breeches with less than half the screw through the lamina. No screws violate the spinal canal or the exiting nerve root. 43 Kang et al 44 safely inserted TLS in 17 patients as a supplement to anterior lumbar interbody fusion that was performed several days earlier. No screws violated the spinal canal and no complication was recorded. 44 There is currently an ongoing randomized controlled trial comparing 3-dimensional navigation template for guiding unilateral lumbar pedicle screw with contralateral TLS in lumbar spine. 45 Future studies like these will help further characterize the feasibility of TLS in lumbar spine.
Biomechanics
With multiple options available for atlantoaxial fixation, several studies have been conducted to determine TLS biomechanical properties in relation to other commonly used methods of fixation in both primary and salvage techniques. 46,47 Gorek et al, 48 in their biomechanical analysis using six C0-C4 cadaveric specimens, compared the stability afforded using a screw-rod construct with C1 lateral mass–C2 TLS to the Harms technique using C1 lateral mass–C2 pedicle screws. They found that intralaminar and pedicle screws, or a combination of both, provide equivalent acute stabilization at C2 with similar reductions in flexion/extension, lateral bending, and axial rotation. In a similar study, Claybrooks et al 46 analyzed the same 2 constructs, C1 lateral mass–C2 TLS and C2 lateral mass–C2 pedicle screws, in 8 C1-C3 cadaveric spines. TLS were found to provide equivalent resistance to flexion/extension and anterior-posterior translation but had inferior stiffness in both lateral bending and axial rotation compared with pedicle screws. The authors attributed this difference to the use of shorter spine segments that reduced adjacent level motion during testing and focused the motion at the elastic zone of C1-C2. Impaired resistance to lateral bending was also reported by Lapsiwala et al, 47 who compared 4 C2 fixation constructs, including TLS, anterior/posterior transarticular screws, and pedicle screws with and without supplemental sublaminar cable fixation. Again, TLS provided comparable stability with the other methods of fixation in flexion/extension and axial rotation; however, while TLS resistance to lateral bending was greater than an uninstrumented intact spine it was less than other constructs, indicating decreased stiffness in the coronal plane.
While early studies demonstrated comparable stability between laminar screws and other methods of posterior fixation, many disregards possible wear characteristics and screw properties such as pullout strength (POS) and insertional torque (IT). Lehman et al 49 addressed these issues in their in vitro biomechanical analysis of pedicle screws, TLS, and pars screws as primary and salvage techniques at C2. After simulating primary failure with either a pedicle or pars screw, the type not used in the index procedure was tested as a salvage technique followed by the use of TLS as a “backup” salvage technique. The authors observed that pedicle screws generated greater IT and POS when used for primary fixation compared to pars screws and TLS and a trend toward greater IT and POS when used as a salvage technique. Meanwhile, TLS exhibited consistently, though not statistically significantly higher POS compared with pars fixation when used as a salvage technique, suggesting superiority of TLS over pars screws should primary fixation with pedicle screws fail.
Similar work was done to demonstrate the biomechanical stability of laminar screws in the subaxial, thoracic, and lumbar spines. Reddy et al 50 used cadaveric specimens to compare the stability of C2-3 constructs containing either C2 TLS or pedicle screws in conjunction with C3 lateral mass screws. Both the transpedicular and translaminar constructs exhibited increase stability compared with an intact spine, but there was a trend toward greater motion allowed by TLS that may have resulted from the use of longer rods in the TLS constructs that produced a greater moment about C2-3.
As demonstrated in anatomic feasibility studies, C7 is also another candidate for TLS constructs. Cardoso et al 51 used in vitro analysis of cadaveric C7 specimens to evaluate the bone-screw interface strength of TLS following simulated failure of index pedicle screws. The authors found no statistical difference in POS between TLS and pedicle screws, but reported a 57% decrease in TLS IT, which they attributed to the large C7 laminar thickness relative to that of the pedicle. These results were reaffirmed by Hong et al, 23 who tested the biomechanical and kinematic properties of lateral mass screws, TLS, and pedicle screws in C6-7 segments of cadaveric spine. All 3 constructs provided greater stability relative to intact spines, though lateral mass screws had statistically inferior POS compared with TLS and pedicle screws. Similar to results seen in the axial spine, TLS also provided equivalent resistance to motion in flexion/extension and axial rotation at C7, but decreased stiffness in lateral bending.
McGirt et al 52 examined 10 human cadaver spines and compared the biomechanical properties of TLS versus pedicle screw fixation at T1-T2. They found that both constructs significantly decreased motion during flexion, extension and lateral bending compared with preinstrumented spines. Rotation at the cervicothoracic junction was increased after 40 000 cycles of loading in both constructs, but TLS group has slightly greater change. 52 Similarly, Kretzer et al 41 also found that TLS offers similar stability to pedicle screw in the upper thoracic spine with slight increase in motion in flexion and extension.
In the lumbar spine, Liu et al 53 compared the biomechanical properties of 3 posterior constructs, unilateral pedicle screw (UPS) versus UPS with contralateral TLS versus bilateral pedicle screw. They concluded that UPS with contralateral TLS has superior flexion-extension and lateral bending compared with UPS but inferior lateral bending compared with bilateral pedicle screw. 53 However, Zhan et al 54 tested 12 fresh human cadavers, and found that both pedicle screw and TLS significantly reduced range of motion and increased stiffness compared with intact spine, and there is no significant difference in stability between the 2 constructs.
Clinical Application and Safety
Several authors have reported on their experience with TLS in the axial, subaxial, and thoracic spine over the past decade (Table 1). The earliest studies by Wright et al 18 followed a cohort of 10 patients in 2004 that was expanded to 20 patients in 2005. 18 Using a C2 TLS and C1 lateral mass screw construct, the authors placed forty 4.0-mm C2 TLS with a 100% fusion rate. While there were 3 instances of cortical breach, the authors had no difficulty placing the screws and reported no cases of ventral cortical disruption or neurovascular complications following screw insertion. To minimize this potential complication of ventral disruption with penetration into the canal, Jea et al 55 proposed a modified Wright’s technique to assure bicortical screw purchase by creating an exit window on the dorsal aspect of the lamina. A total of 6 patients underwent this modified Wright’s technique with satisfactory fixation of the axis and no significant complications.
Following the initial success of C2 TLS by Wright, Wang 26 conducted a similar study with smaller 3.5-mm screws. The authors placed 59 TLS in 30 patients and noted several complications. 26 Compared with earlier reports, the authors observed higher rates of instrumentation failure (6.7%) and laminar disruption including one case of ventral breakthrough identified on postoperative imaging. Wang and colleagues attributed the instrumentation failure to the smaller screw size and proposed that larger screws should be used to withstand greater mechanical stress. Sciubba et al 56 also used 3.5-mm screws in their study, in which 32 laminar screws were placed in 16 patients. No neurologic or vascular complications were observed; however, 1 case of pseudoarthrosis and 1 case of fixation fracture were reported, both of which required revision surgery. Regardless of the screw size, the bony fusion rate of translaminar screws has been excellent, ranging from 92.9% to 97.6%. 57,58
In 2009, Zhou et al 59 described a case of a 37-year-old patient with atlantoaxial dislocation and prior C2-C3 fusion who underwent primary fixation via C2 TLS with C1 lateral mass screws. Prior to this report, Wright’s method of C2 TLS for atlantoaxial fixation was only used as a salvage technique in cases where pedicle or transarticular screw implantation had failed or were prohibited by unilateral vertebral artery occlusion. In this instance, the patient had small axis pedicles following C2-C3 fusion, making her a poor candidate for transarticular or pedicle screw insertion. The authors noted clinical success with no neurovascular complications and complete fusion at 6 months.
TLS gained international popularity with Hong’s group in Korea, who reported on their earlier experience using TLS in the subaxial spine. The authors studied fixation of the subaxial cervical spine in 11 patients using thirty-four 3.5-mm TLS with few complications noted including 2 cases of dorsal breakthrough. 23 In a subsequent study, the group compared intralaminar screws placed at C2 with those placed at C7, which can be used in the fixation of the upper thoracic spine in patients with intact posterior elements. Again, all patients achieved successful fusion with no neurovascular complications or ventral breakthrough, but there was one instance of C2 dorsal breach that did not require revision. The authors noted that using this method may potentially decrease the risk of vascular injury in the subaxial spine, as the vertebral artery enters the C7 transverse foramen in 5.4% of cases and is therefore at increased risk with the insertion of C7 pedicle screws. In contrast, TLS allow mobilization of C7 and eliminates the aforementioned risks.
In addition to its use as salvage technique in the axial and subaxial spine, TLS have also been shown to be effective in the thoracic spine and with hangman’s fractures. 60 Following their reported use in the axial spine by Wright, Kretzer et al 41 demonstrated successful placement of 13 intralaminar screws at T1 and 6 intralaminar screws at T2 in 7 patients. The risk for ventral breakthrough was still present with one reported ventral laminar disruption that required subsequent revision.
Similarly, lumbar spine is still a relatively under-explored region for TLS fixation. 61 Grob et al 62 compared the results of 57 patients undergoing TLS versus pedicle screw in 63 patients. TLS group has significant lower blood loss and operating time, while the multidimensional CORE Outcome Measure Index and complication at 2 years was equivocal between the 2 groups. They concluded that extensive 3-point stabilization is a requirement for optimizing patient outcomes. 62 TLS has also been implicated in use with pedicle screw in lumbar spine. Huang et al 63 treated 60 single level lumbar degenerative disease patients with minimal invasive TLIF using a unilateral pedicle screw and a TLS. Patient had significant improvement in visual analogue scale and Oswestry Disability Index with 88% grade I fusion at 30 months follow-up. 63
While multiple studies have compared TLS versus other methods of fixation in vitro, few have focused on their clinical application in vivo. In a landmark study, Parker et al 64 compared the efficacy of 152 C2 TLS with 161 C2 pedicle screws in 167 patients. The authors found that both techniques were equally efficacious for axial cervical fusions and that C2 translaminar screws had significantly less risk of radiographic breach compared with C2 pedicle screws (1.3% vs 7%, respectively) with no significant difference in overall morbidity, including surgical site infection, incisional cerebrospinal fluid leak, iatrogenic neurological injury, and vertebral artery injuries. However, the 1-year durability of TLS were found to be inferior to pedicle screws for subaxial fusions and were associated with higher rates of revision surgery at 1 year (6.1% vs 0%, respectively). The authors concluded that although C2 translaminar screws might have an inferior 1-year durability for subaxial fusions, it is equally efficacious for axial cervical fusion with no increase in morbidity.
Although the use of TLS in the pediatric population is not as extensive as in adults, multiple studies have demonstrated their successful application in younger patients. Leonard and Wright 65 described the use of C2 TLS in 3 patients aged between 3 and 16 years with successful axial fusion and no complications. In the subaxial spine, Jea et al 24 reported the use of unilateral C3 TLS in a child with occipitoatlantoaxial instability. While the patient had temporary cranial nerve dysfunction, successful fusion was observed by 3 months with no evidence of instability on either flexion or extension. Chamoun et al 22 was also able to successfully insert subaxial and thoracic TLS in 7 pediatric patients from C3 to T1 with a 100% fusion rate and no instances of cortical breach or instrument failure. These results were similar to those reported by Lewis et al, 66 who used laminar screws as a salvage technique in the thoracic spine.
Conclusion
TLS was originally described as a salvage method of fixing the axial spine. It has the advantage of lower vertebral artery injury without use of navigational instruments, yet achieving similar fusion rate as other constructs. It uses the anatomy of atlantoaxial in which the lamina was short and wide. Usage of TLS has since then expanded to the entire spine. Advancement in imaging has allowed preoperatively planning for appropriate sizing of TLS as well as guidance of the insertion trajectory. Biomechanical studies have also corroborated the integrity of TLS stability compared to traditional pedicle constructs. Good clinical outcomes with TLS, either alone or in conjunction with pedicle screws, have also been reported in the spine communities around the world. TLS has certainly become a viable alternative option that spine surgeons should be aware of. Although this review article only used one search engine (PubMed), the overall yield of records was sufficient with supplementation of hand searching through all relevant citations and included all recent and relevant literatures up to time of publication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.