
Abstract
Only a few cases of iatrogenic lumbar injury have been reported in the literature. A 58-year-old male with severe back pain was admitted to our department. The patient was qualified for the transpedicular stabilization with interbody fixation at L4/L5 and L5/S1 levels. On the first day after surgery, the patient was mobile and reported significant pain relief. He was discharged the same day. After 2 weeks, the patient returned with severe right lower abdominal pain and radicular pain in his right leg. He was administered to the Neurology Department where the presence of a lumbar muscle hematoma and lumbar artery pseudoaneurysm were discovered. He was transferred to the Vascular Surgery Department where aortography was performed and the pseudoaneurysm was embolized. After few days, the patient’s overall condition improved significantly. Eight weeks after surgery, he was pain-free. Our case shows how initially innocuous symptoms may be the result of serious complications.
Keywords
Introduction
The use of transpedicular screws in spine surgery began in the 1950s and 1960s, 1 and they are currently a widely used standard fixation technique in both traumatic and degenerative spine surgery. Intraoperative navigation in combination with the C-arm or O-arm is often used to improve screw position accuracy. In the last few years, to reduce intraoperative X-ray radiation, many spine surgeons are returning to the free-hand screw insertion technique, using anatomical points.2–4 Vascular complications of spinal surgery are rare, with the incidence ranging from 0.01% to 0.22%5,6 and the mortality rate ranging from 15% to 65%. 6 The most commonly damaged vessels are the aorta, the common iliac vein, and the internal iliac vein.5,6
Case report
A 58-year-old male with severe back pain was admitted to our department. He had already undergone L5/S1 microdiscectomy surgery on the left side 5 years earlier. For several months, he felt recurrence of back pain that radiated to both legs. His Core Outcome Measures Index (COMI) 7 back questionnaire score was 6.20. Magnetic resonance imaging (MRI) showed a central stenosis with discopathy and significant hypertrophy of the intervertebral joints at the L4/L5 and L5/S1 levels. The patient qualified for the following surgical treatment: transpedicular stabilization with interbody fixation-posterior lumbar interbody fusion (PLIF) at these levels.
A classic midline approach was used. Transpedicular fixation was initially performed using the free-hand technique, and then facetectomy was performed on both sides at the level of L4/L5 and L5/S1. Two intervertebral implants were placed at both levels. The intraoperative X-ray control image was satisfactory (Figure 1), and the surgery seemed to be performed without any complications to this point.

Post operation X-ray, lateral view.
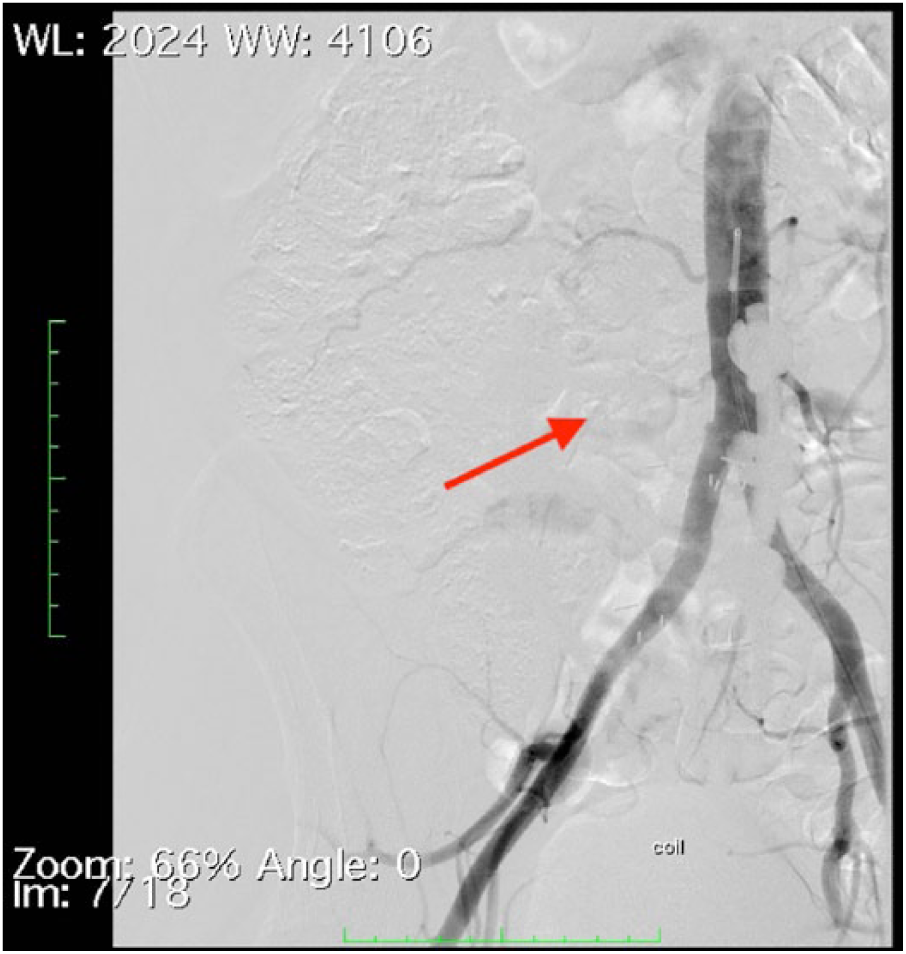
On the first day after surgery, the patient was mobile and he reported significant pain relief. He was hemodynamically stable. The blood test showed a slight decrease in hemoglobin adequate to the surgery. He was discharged the same day. After a week, he came back to have his stitches removed and reported a single episode of short-lasting severe back pain radiating to the right groin and abdomen. The symptom seemed not to be related to the surgery, and it was suggested that he contact an internal medicine specialist. After another week, the patient returned with exacerbation of symptoms. He had severe right lower abdominal pain and pain radiating into his right leg that prevented self-movement. He was admitted to the Neurology Department where after a ultrasonograpy (USG) and computed tomography (CT) scan, the presence of a lumbar muscle hematoma and lumbar artery pseudoaneurysm was discovered (Figure 2). The patient was transferred to the vascular surgery department where aortography was performed. Contrasted anastomotic pseudoaneurysm was embolized using a VortX Diamond-18 coil 4 × 3.7 mm2 and 5 × 5.5 mm2 (Figures 3 and 4) (Boston Scientific, USA). Nearly complete closure of the infiltration to the aneurysm was obtained.

CT scan, iatrogenic aneurysm in lumbar muscle before embolization.

Angiography, iatrogenic aneurysm in lumbar muscle before embolization.
Angiography, iatrogenic aneurysm in lumbar muscle after embolization.
After a few days, the patient’s overall condition improved significantly; he started walking by himself with walking stick and was discharged. On the first follow-up after surgery, he was walking stick-independent. Eight weeks after surgery, he was pain-free and his COMI 7 back score was 8.4.
Discussion
Vascular complications can be divided into those detected intraoperatively, early (a few hours after surgery), or late (after a few months).5,6 Lumbar arteries are small branches of the abdominal aorta, iliac lumbar artery, or medial artery, which has a diameter of up to 2.9 mm. 8 Only a few cases of iatrogenic lumbar injury have been reported and most of them have a rapid course with hemodynamic shock. Lee et al. 9 described one case of a 23-year-old patient who underwent surgery to correct scoliosis. Thereafter, she had a massive hemorrhage of the lumbar artery, which led to cerebral ischemia and death of the patient several hours after surgery. Sandri et al. 10 describes the case of a 39-year-old patient whose lumbar artery was damaged as a result of rear screw fixation. The complication was detected a few hours after surgery because of the occurrence of sudden hemodynamic disorders requiring blood and plasma transfusions. Similar to our patient, endovascular coiling was provided and the patient was discharged without any distant complications.
Delayed progression with gradual neurological deterioration without hemodynamic disturbances such as in our patient is very rare. Nijenhuis et al. 11 describe the case of a lumbar artery pseudoaneurysm in the space after L4 laminectomy, which caused dural sac pressure and neurological deficits in the patient 3 months after the surgery. After endovascular embolization, the symptoms were resolved.
Stevens et al. 12 describe the occurrence of a lumbar artery pseudoaneurysm after needle biopsy of L4 vertebral body. As in our patient, this was a late complication that was discovered 6 months after the original procedure. The patient was also treated endovascularly and discharged neurologically intact.
Conclusion
An increasing number of reports of iatrogenic lumbar spine injury suggest that it may not be such a rare complication. 13 Given the possible effects such as pain, increased neurological deficits, and hemodynamic instability, it is important to take into account the possibility that these effects can occur. Our case shows how initially innocuous symptoms, which are often ignored, may be the result of serious complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.