
Abstract
Study Design:
Propensity score matched retrospective cohort study.
Objectives:
Obesity is a major confounder in determining the independent effect of metabolic syndrome (MetS) on complications after spinal surgery. The purpose of this study is to differentiate MetS from obesity as an independent influence on perioperative outcomes after elective lumbar spine fusion.
Methods:
One- to 3-level posterior spinal fusion cases were identified from the 2011-2014 American College of Surgeons’ National Surgical Quality Improvement Program. To determine the effects of MetS outside of obesity itself, patients with MetS were first compared to a no-MetS cohort and then to an obese-only no-MetS cohort. Two propensity score matches based on demographics, comorbidities, surgical complexity, and diagnosis were used to match patients in 1:1 ratios and compare outcomes. Logistic regression with propensity score adjustment was further utilized as a secondary method of reducing selection bias.
Results:
Out of 18 605 patients that met criteria for inclusion, 1903 (10.2%) met our definition of MetS. Patients with MetS had a higher rate of wound complications (3.8% vs 2.7% obese no MetS, P = .045; vs 2.6% no MetS, P = .035), readmissions (7.4% vs 2.2% obese no MetS, P < .001; vs 4.6% no MetS, P < .001), and extended length of stay (29.1% vs 23.9% obese no MetS, P < .001; vs 23.5% no MetS, P < .001). Patients with MetS were more likely to experience a wound complication (odds ratio = 1.47, 95% confidence interval = 1.02-2.12) or readmission (odds ratio = 1.48, 95% confidence interval = 1.22-1.80).
Conclusions:
Even after controlling for obesity, MetS is an independent risk factor for adverse short-term outcomes. These findings have various implications for preoperative risk stratification and reduction strategies.
Introduction
Metabolic syndrome (MetS) is unique state of hormonal dysregulation that puts patients at risk for multiple disease processes. The exact definition of MetS is a subject of debate, 1 but it is generally agreed that the 4 components of the phenotype can be described as visceral obesity, insulin resistance, hypertension, and dyslipidemia. Multiple population-based studies have shown that MetS is associated with osteoarthritis (including involvement of the spine) and intervertebral disc disorders. 2 –7 Osteoarthritis and MetS are pathophysiologically connected through imbalances in proinflammatory cytokines, increased oxidative stress, endothelial dysfunction, and dysregulation of common metabolites. 1,8
Rather than the consequence of a high body mass index (BMI), MetS is a distinct state of hormonal dysregulation and must be treated as an independent risk factor when accounting for complications after elective surgery. 1,9 The Centers for Medicare and Medicaid Services has increased legal and financial pressure on providers 10 to reduce adverse outcomes after orthopedic surgery, motivating researchers to quantify the impact of MetS on complications, readmissions, and length of stay. 9,11 –13 The impact of MetS is confounded by its relationship with obesity, as visceral adiposity is one of the key components of the disease. Chung et al 14 and Memtsoudis et al 15 both utilized national surgical databases to show that MetS is a risk factor for complications after surgery; however, neither study isolated obesity as a confounder. Thus, it is unclear whether obesity or MetS is the culprit behind inferior short-term outcomes in this population.
The purpose of our study is to control for the effect of obesity in quantifying the relationship of MetS with 30-day medical complications, wound complications, readmissions, and prolonged hospital stay after elective posterior lumbar fusion surgery. Through the use of propensity score matching, a statistically rigorous method that approximates randomization of known covariates, we hope to define whether obesity or MetS is the greater predictor of poorer short-term outcomes after elective spine surgery. 16 This information is essential for knowledgeable patient counseling, medical optimization, and risk-adjusted reimbursement models.
Materials and Methods
Data Acquisition and Definitions
Data was acquired from the American College of Surgeons’ National Surgical Quality Improvement Program (NSQIP). NSQIP encompasses a wide variety of centers ranging from small community practices to large urban hospitals and utilizes a validated third-party data collection method. 17,18 The reliability of the data has allowed for the production of generalizable orthopedic surgery outcomes research. 9,19,20
One- to 3-level posterior lumbar fusion cases were identified from the 2011-2014 NSQIP datasets using the primary Current Procedure Terminology (CPT) codes 22 612, 22 630, or 22 633. The number of levels fused and fusion technique (posterior/transforaminal vs anterior) were identified using any additional CPT codes assigned to each case. The presumed indication for surgery was referenced using the ICD9 surgical diagnosis codes: 724, spinal stenosis; 722, intervertebral disc disorder; 721, spondylosis; 737, scoliosis; and 738.4, acquired spondylolisthesis. Emergency and revision cases were excluded. Using a previously operationalized definition, 9,21 patients were classified as having MetS if they had a BMI of greater than or equal to 30 kg/m2, diabetes mellitus, and hypertension requiring medication.
Primary outcomes of interest included wound complications, medical complications, unplanned readmission, and prolonged postoperative stay. Precise definitions of each complication may be found in the NSQIP Participant Use File Guide. 22 Wound complications included superficial surgical site infection, deep surgical site infection, and wound dehiscence. Medical complications included pulmonary embolism, deep venous thrombosis/thrombophlebitis, pneumonia, unplanned intubation, ventilation >48 hours, acute renal failure, progressive renal insufficiency, urinary tract infection, stroke or cerebrovascular accident, coma, bleeding transfusion, myocardial infarction, cardiac arrest, sepsis, and septic shock. Bleeding transfusion was defined as “at least 1 unit of packed or whole red blood cells given from the surgical start time up to and including 72 hours postoperatively.” 22 Unplanned readmission was defined as any readmission at the same or another hospital for a problem likely related to the principal surgical procedure. Prolonged postoperative stay was defined as a stay longer than 5 days, the top quartile in our dataset. All outcomes were recorded for up to 30 days after the index procedure.
Statistical Analysis
To control for confounding and approximate randomized conditions in the estimation of effect size, a predetermined propensity score algorithm was used to match patients with MetS to controls in a 1:1 ratio. Patients were matched using the follow factors: gender, race, age class, smoking status over the past year, chronic obstructive pulmonary disease, dyspnea, congestive heart failure in the past 30 days, chronic steroid use, bleeding disorder, anterior interbody fusion, posterior interbody fusion, number of levels fused, and surgical diagnosis. Of note, American Society of Anesthesiologist (ASA) class, a well-known correlate with postoperative complications after spine surgery, 23 was not used as a cofactor because of confounding concerns—diseases used in the assignment of ASA class overlap with those used in our definition of MetS (eg, diabetes). Last, in order to distinguish the impact of MetS from the effect of morbid obesity itself, a second propensity score algorithm was utilized to allow for comparisons with a control group that was obese. Patients with MetS were matched on all of the aforementioned comorbidities, demographics, and surgical factors, but to an obese-only cohort using BMI class (Obese I, 30-35 kg/m2; Obese II, 35-40 kg/m2; Obese III, ≥40 kg/m2) as the additional algorithm covariate.
Outcomes were compared between the matched cohorts using Pearson’s χ2 test for categorical variables and Mann-Whitney U test for continuous variables. Logistic regression was used to generate propensity score–adjusted odds ratios to determine the independent association of patient demographics, comorbidities, and surgical factors with each outcome of interest. Covariates were screened for inclusion in the model using a significance of P < .200 and event occurrence of 10. 24 Hosmer-Lemeshow tests were used to assess the goodness-of-fit for each model. 25 All analyses were performed using IBM SPSS version 22 (Armonk, NY).
Results
Out of the 18 605 patients identified as having undergone 1- to 3-level posterior lumbar fusions, 1903 (10.2%) met criteria for MetS. Table 1 displays the rates of demographic characteristics, comorbidities, and surgical factors in patients with and without MetS. Compared to those without MetS, patients with MetS were more likely to be older (31% vs 26% >70 years old, P < .001), black (12% vs 6%, P < .001), and suffer from higher rates of dyspnea and chronic obstructive pulmonary disease (11% vs 5% and 7% vs 5%, respectively, P < .001 for both). With regard to surgical factors, patients with MetS had higher rates of spinal stenosis (35% vs 29%, P < .001) and underwent surgery for 2 or more levels at a higher rate (37% vs 34%, P < .009). Propensity score matching the MetS patients to a representative group of patients without MetS was successful in eliminating significant differences between the cohorts (P > .05 for all demographics, comorbidities, and surgical factors). As expected, BMI differed between the cohorts due to the inclusion of BMI in the definition of MetS (35.7 kg/m2 [32.6-39.6] vs 29.0 kg/m2 [25.7-33.3]).
Patient Sample Characteristics.
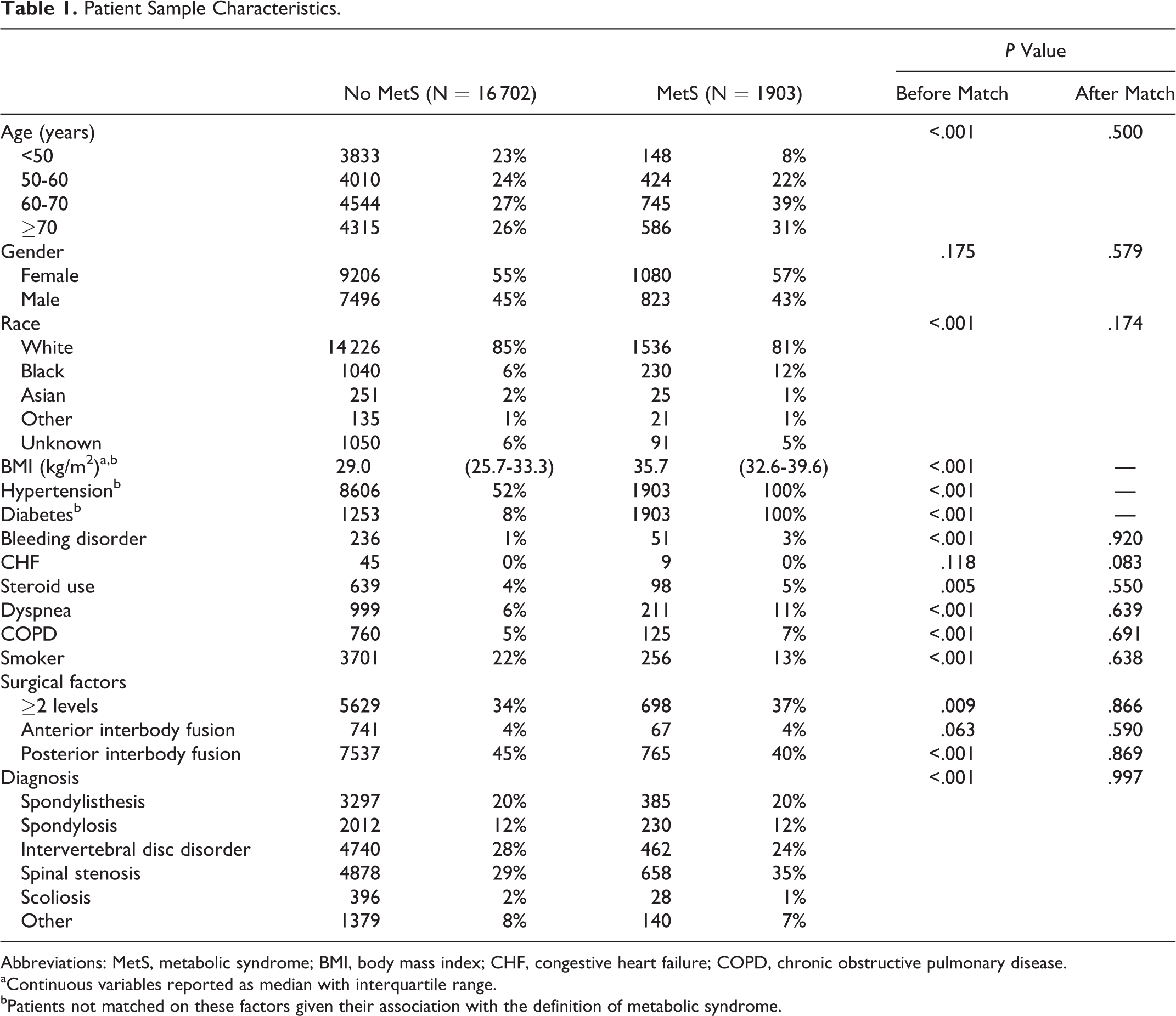
Abbreviations: MetS, metabolic syndrome; BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease.
aContinuous variables reported as median with interquartile range.
bPatients not matched on these factors given their association with the definition of metabolic syndrome.
After matching, the rate of wound complication (Table 2) was significantly higher among patients with MetS (3.8% vs 2.6%, P = .035). Logistic regression (Table 3) revealed that patients with MetS were one-and-a-half times more likely to experience a wound complication after lumbar fusion surgery (odds ratio [OR] = 1.5, 95% confidence interval [CI] = 1.0-2.1, P = .04).
Complication Rates in the Matched Cohortsa.
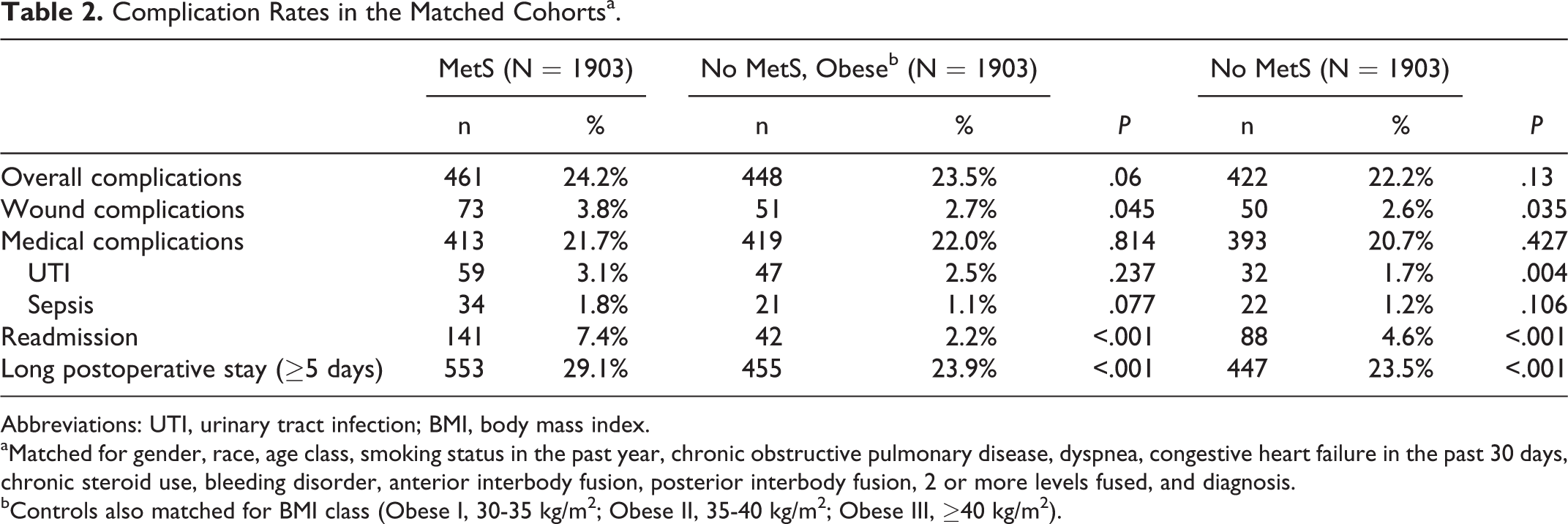
Abbreviations: UTI, urinary tract infection; BMI, body mass index.
aMatched for gender, race, age class, smoking status in the past year, chronic obstructive pulmonary disease, dyspnea, congestive heart failure in the past 30 days, chronic steroid use, bleeding disorder, anterior interbody fusion, posterior interbody fusion, 2 or more levels fused, and diagnosis.
bControls also matched for BMI class (Obese I, 30-35 kg/m2; Obese II, 35-40 kg/m2; Obese III, ≥40 kg/m2).
Association of Metabolic Syndrome With Outcomes of Interest.
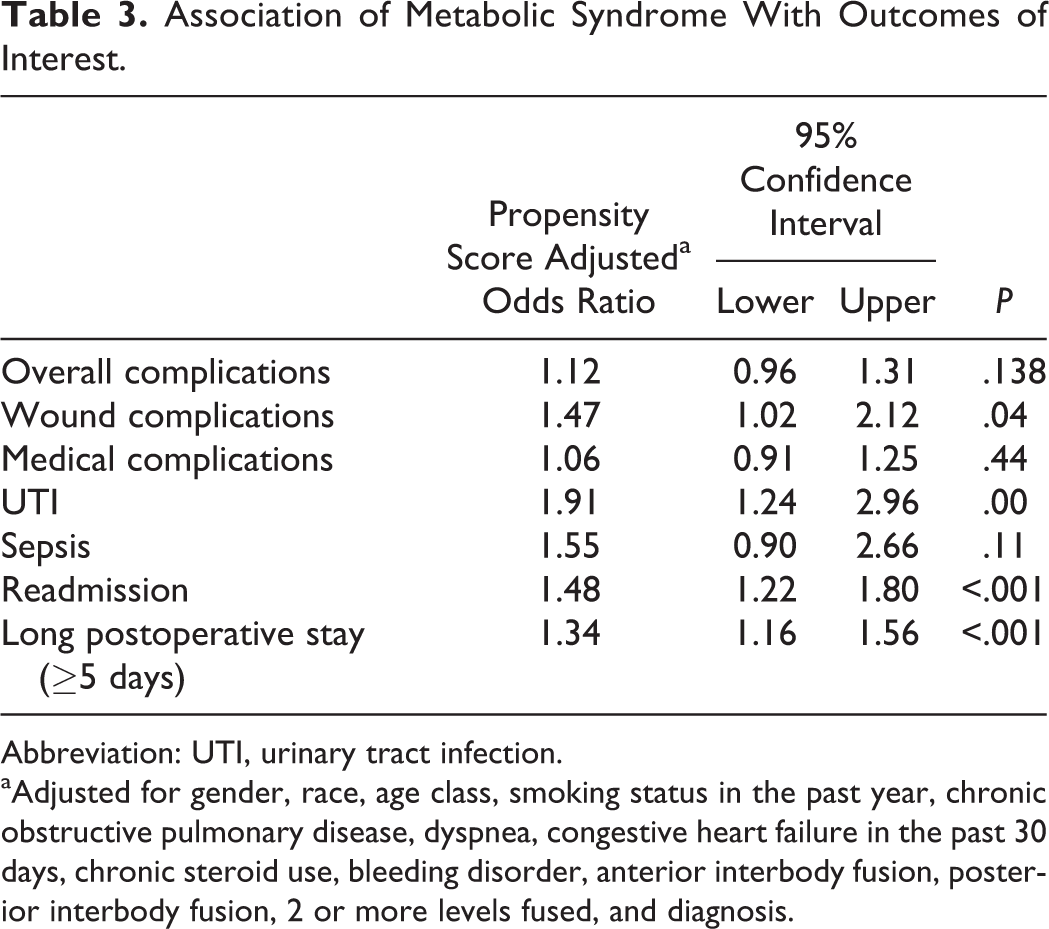
Abbreviation: UTI, urinary tract infection.
aAdjusted for gender, race, age class, smoking status in the past year, chronic obstructive pulmonary disease, dyspnea, congestive heart failure in the past 30 days, chronic steroid use, bleeding disorder, anterior interbody fusion, posterior interbody fusion, 2 or more levels fused, and diagnosis.
Though medical complications were not increased (21.7% MetS vs 20.7% No MetS, P = .427), analysis of individual complications revealed that patients with MetS experienced urinary tract infections (UTIs) at higher rates (3.1% vs 1.7%, P = .004). The odds of having a postoperative UTI were doubled in patients with MetS (OR = 1.9, 95% CI = 1.2-3.0, P < .001). Sepsis occurred at a higher but insignificant rate between the cohorts (1.8% MetS vs 1.2% no-MetS, P = .106), trending toward an association with MetS (OR = 1.6, 95% CI = 0.9-2.7, P = .11). Of note, sepsis occurred at a very low rate in this dataset. Other individual medical complications, such as myocardial infarction and cerebrovascular accident, occurred at comparable rates (P > .05 for all; data not shown in table).
Metabolic syndrome was also associated with a prolonged postoperative hospital stay, as 29.1% of patients with MetS stayed longer than 5 days, compared to 23.5% in those without MetS (P < .001). This association was validated in the logistic regression model (OR = 1.34, 95% CI = 1.2-1.6, P < .001). Last, patients with and without MetS were readmitted at a higher rate (7.4% vs 2.2%, P < .001). Logistic regression supported this association of MetS with readmission (OR = 1.48, 95% CI = 1.22-1.80, P < .001).
The secondary propensity score match was successful in matching the MetS patients with obese controls by BMI class (Obese I, II, III; 44%, 34%, and 22% No MetS vs 44%, 33%, 23% MetS, P = .751). Compared to obese controls (Table 2), MetS patients had higher rates of wound complications (3.8% vs 2.7%, P = .045) and longer postoperative stays (29.1% vs 23.9%, P < .001). Readmission was also increased (7.4% vs 4.6%, P < .001). Urinary tract infections were slightly higher, but this difference was not significant (3.1% MetS vs 2.5% No MetS, Obese, P = .237). Medical complications among patients with MetS were comparable to the obese controls (P > .05 for all).
Discussion
The number of patients with MetS undergoing lumbar spinal fusion has trended upward over the past 2 decades, tripling in prevalence between 2000 and 2008. 15 The trend is not surprising, as there are multiple proposed pathophysiologic connections between spinal osteoarthritis and MetS. 1,7 Reactive oxidative species, found in high levels in patients with MetS, accelerate chondrocyte aging and apoptosis. 26 However, the most recognized connection between osteoarthritis and MetS lies in systemic inflammation. Visceral fat (adipose tissue surrounding abdominal organs) is metabolically active, increasing pro-inflammatory factors. In both osteoarthritis and MetS, there are low-grade elevations in systemic inflammatory markers such as interleukin (IL)-1, IL-6, and IL-10. 27 Thus, it is unclear whether obesity is the true factor influencing surgical outcomes associated with the MetS.
Central obesity is a common criteria used in defining MetS 1 ; and the connection between obesity and wound infections after spine surgery is well studied. 28 –33 Though many surgeons believe that obese patients are at high risk for wound infections, there are conflicting data stating otherwise. 28 –33 To explain this discrepancy, some authors have proposed that the link between obesity and infection lies in the distribution of body fat, not the BMI itself. 33 A large amount of subcutaneous fat over the posterior spine requires vigorous prolonged retraction to adequately visualize the surgical site. The resultant tissue necrosis, combined with an increased surface area of subcutaneous tissue exposed to the environment, may increase the likelihood of bacterial infection. 28,29,33
The conflicting data in the relationship between obesity and infection may also be explained by considering that past studies have not distinguished patients with MetS within their obese study groups. In our study, we were able to show that the rate of wound infections is higher in patients with MetS even when compared to their obese counterparts. Patients with MetS are not only obese but also in a state of hormonal dysregulation and low-grade inflammation, likely contributing to a propensity for infections. Similar to how the low-grade inflammatory state predisposes these patients to arthritis, it may also predispose them to infections. Hormonal mediators have been proposed as mechanisms connecting chronic inflammation with immune dysfunction and a subsequent susceptibility to infection. 34,35 Thus, certain obese patients with MetS are especially at risk, subject to the local effects of thick subcutaneous fat at the wound combined with a systemic vulnerability to infection. The fact that the rate of wound complications among patients with MetS was increased even when compared with obese controls suggests that the hormonal dysregulation is separate from, or possibly additive to, the effect of obesity alone. This theory that MetS patients are predisposed to infection through systemic factors is supported by the finding that UTIs were also associated with the disease. Last, sepsis was also increased in patients with MetS, though the infrequency of this complication likely left the study underpowered to detect any significant difference (1.8% vs 1.2%, P = .11).
To our knowledge, this is the first study demonstrating that patients with MetS undergoing 1- to 3-level posterior lumbar fusion also have an increased risk for wound complications. Chung et al also used the NSQIP database to analyze the relationship between MetS and short-term outcomes, finding that MetS was not related with wound complications. 14 However, there are several key differences between our studies. First, the statistical methods were quite different. Chung et al did not employ a multivariate analysis of wound complications, choosing only to use uncontrolled univariate analyses, which did not account for the impact of obesity in the non-MetS cohort, a plausible explanation for why wound complications were comparable. Second, the populations were different, as their cohort included data from 2006 to 2013 and all levels fused, while we used the more recent 2011 to 2014 files and only included 1- to 3-level fusions. The initial NSQIP user files in the earlier years of the program often included missing or null data. We specifically chose to use the files after the addition of a readmission variable in 2011 in order to account for earlier discrepancies in coding. Third, while they report “wound complications” in their table, this is not a variable in the NSQIP User Guide, 22 and the authors do not define what specific NSQIP variables this term includes in their materials section, making it difficult to interpret the conclusion.
Medical complications were found at comparable rates between the 2 cohorts, likely as a result of a nonparsimonious propensity score match. The patients were matched for a wide variety of demographics and medical comorbidities, among them age, chronic obstructive pulmonary disease, and congestive heart failure within 30 days, all well-known risk factors for medical complications and readmission after spine surgery. 36 –40 In an analysis of the National Inpatient Sample from 2000 to 2008, Memtsoudis et al 15 found that patients with MetS experienced higher rates of cardiac and pulmonary complications; however, they were not able to control for procedural complexity. In our study, patients were matched by the number of levels fused and type of interbody fusion, to account for the higher rate of medical complications that may be seen in anterior/posterior fusions or in those greater than 2 levels. 41 Chung et al also found that patients with MetS had higher rates of pulmonary complications after lumbar fusion and attributed this to obesity-related pulmonary disease. 14 However, their study population included patients undergoing extensive posterior fusions while ours was confined to 1 to 3 levels. Furthermore, they did not control for anterior/posterior cases in their analysis. We believe that the comprehensive propensity score match and narrowly defined patient population better approximates the real risk of medical complications in the MetS cohort.
Though we did not have direct data on expenditures, several comments may be made regarding the potential impact of MetS on increasing spinal surgery costs. Through its association with long postoperative stays (≥5 days), complications, and readmissions, MetS directly drives up expenditures. However, recent regulatory efforts by the Centers for Medicare and Medicaid Services add another factor to the complication-cost equation. Though the current legislation focuses on reducing costs after hip and knee replacements, posterior lumbar fusion, a somewhat “infamous” procedure for its costs and wide range of use, 41 will likely be targeted in the future. Hospitals incur a fee if they exceed standard rates of reportable postoperative outcomes after total joint replacement—among them myocardial infarction, pneumonia, sepsis, surgical site bleeding, pulmonary embolism, wound infection, and 90-day readmission. 10 Administrators can expect patients with MetS to experience higher rates of wound infections, and possibly sepsis. Furthermore, MetS was associated with 30-day readmissions, which incur additional financial penalties for hospitals outside of the direct increases in expenditures. As reimbursement models move toward payments for defined episodes of care over a certain time period, this will become even more relevant. Thus, aside from the impact on surgeon-patient counseling and preoperative medical optimization, quantifying the association of MetS and risk of complications becomes necessary for the creation of properly risk-adjusted reimbursement and penalization models. As the models are created, it is essential to distinguish MetS from obesity as its own independent risk factor.
Metabolic syndrome is a modifiable risk factor. Accordingly, all patients with the disease should be counseled on taking measures to optimize their health before undergoing elective surgery. Through exercise, patients with the MetS may temper the various metabolic risk factors that define the disease. 42 For those in whom exercise and dietary modifications fail, bariatric surgery has also been shown to improve the disease state. 43 However, gastric bypass is not an easy solution—patients who undergo gastric bypass have been shown to have decreased bone mineral density, 44 which could theoretically affect the strength of some constructs.
This analysis suffers from a number of limitations inherent to database research. First, to account for the lack of certain parameters in the NSQIP database, such as lipids and waist circumference, we employed a definition of MetS previously utilized in the orthopaedic literature. 9 Due to our inability to capture these parameters, we may have underestimated the number of patients with conventionally-defined MetS. 1 Such a limitation would have biased the results toward the null hypothesis, underestimating the disease’s effect. Thus, it is possible that patients with MetS have an even greater propensity toward wound infections, urinary tract infections, and long postoperative stays. Most importantly, the use of our definition allowed for the analysis of MetS within a nationwide, multicenter database, maximizing the generalizability of the findings for use in risk-adjusted reimbursement schemes. Second, the limits of using NSQIP for orthopedic research must be noted; in the context of this investigation, the lack of data on antibiotic practices, perioperative disease optimization strategies, and outcomes past 30 days are pertinent when interpreting the results. Third, though the study encompassed a large number of patients with MetS, certain complications, such as sepsis, myocardial infarction, and pneumonia, occur at such rare rates after 1- to 3-level lumbar fusion surgery that detecting significant differences in outcomes requires an extraordinary number of patients. Last, data such as hemoglobin A1c and perioperative glucose levels are not available in NSQIP, factors known to influence infection rate. 45,46 A logical next step for further research would be an attempt to isolate such factors from MetS as a confounder.
In summary, MetS is a unique state of hormonal dysregulation, putting patients at risk for a host of secondary cardiovascular, metabolic, and musculoskeletal diseases. The low-grade chronic inflammation characteristic of the disease is a plausible mechanism connecting the disease with spinal osteoarthritis and a propensity toward infection. Using a national, validated database, we have demonstrated that patients with MetS are at an increased risk of wound complications, readmissions, and long postoperative hospital stays after 1- to 3-level posterior lumbar fusion. This risk is increased even when accounting for obesity as a confounder. As quality-based health care becomes the norm, we recommend that this data be used in the creation of risk-adjusted reimbursement models. Surgeons may want to be particularly vigilant with infection-prevention strategies when operating on patients with MetS. The increased risk of complication should be explicitly stated in patient counseling and utilized in decision making for elective lumbar fusion surgery.
Footnotes
Authors’ Note
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS-NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
De-identified patient information is freely available to all institutional members who comply with the ACS-NSQIP Data Use Agreement. The Data Use Agreement implements the protections afforded by the Health Insurance Portability and Accountability Act of 1996 and the ACS-NSQIP Hospital Participation Agreement. This study conforms to the Helsinki Declaration.