
Abstract
Study Design:
Retrospective case-control study.
Objectives:
Few studies have compared the costs of single-level (1) posterior instrumented fusion alone (PSF), (2) posterior interbody fusion with PSF (PLIF), and (3) lateral interbody fusion with PSF (circumferential LLIF). The purpose of this study was to compare costs associated with these procedures.
Methods:
Charts were reviewed and patients followed-up with a telephone questionnaire. Medicare reimbursement data was used for cost estimation from the payer’s perspective. Multivariate survival analysis was performed to assess time to elevated resource use (greater than 90% of study patients or $68 672).
Results:
A total of 337 patients (PSF, 45; PLIF, 222; circumferential LLIF, 70) were included (63% follow-up at 6 years). PSF and circumferential LLIF patients were 3 times more likely to reach the cutoff value compared with PLIF patients (P = .017).
Conclusions:
Circumferential LLIF and PSF patients were more likely to have higher resource use than PLIF patients and thus incur greater costs at 6-year follow-up.
Introduction
The economic burden of spine-related health care in the United States has been estimated to top $100 billion annually. 1 –4 Despite a 65% increase in spine-related medical expenditures from 1997 to 2005, measures of physical function, work, and social limitations did not improve during the same interval. 4 These numbers emphasize the importance of economic evaluation of surgical procedures given the finite nature of health care resources.
In contrast to previous studies, 5,6 Glassman et al recently reported that posterior instrumented fusion of the spine is a cost-effective intervention. 7 Results published by Bydon et al suggest that interbody fusion might add to the long-term cost-effectiveness and functional outcomes compared with instrumentation alone. 8 Several authors have found that minimally invasive spinal surgery can result in lower direct costs, while a recent systematic review concludes that this remains controversial. 9 –11 While Soegaard et al found a greater cost-utility per quality-adjusted life year (QALY) of circumferential over posterolateral fusion, 12 this study was conducted from the societal perspective of cost. Furthermore, a recent study was able to demonstrate that QALYs can be an invalid measure for cost-analysis leading to inconsistent recommendations. 13 This is particularly true in the elderly population.
To the best of our knowledge, there have been no studies comparing the costs of lateral interbody fusion with open posterior instrumented lumbar fusion (circumferential LLIF), open posterior interbody fusion with instrumentation (PLIF), or open posterior instrumented fusion alone (PSF) from the payer’s (ie, insurance’s) perspective. As such, we aimed to examine whether the addition of an interbody device is beneficial to instrumented fusion alone and whether lateral placement of the cage provides any additional benefits. The purpose of this study was to perform a financial analysis from the payer’s perspective, comparing the costs associated with these 3 different techniques for single-level lumbar fusion.
Material and Methods
Patient Selection
After institutional review board approval was obtained, adult patients undergoing single-level lumbar fusion by 1 of 6 senior, fellowship-trained surgeons at a single spine center between November 2008 and 2011 were identified through Current Procedural Terminology codes. Patients were divided into 3 groups: (1) PSF, (2) PLIF, and (3) circumferential LLIF. 14 Spinal decompression was performed in every patient. The choice of procedure was based on the surgeon’s preference. The indications for surgery included degenerative disc disease, spinal and foraminal stenosis, and spondylolisthesis. Patients with a history of prior lumbar fusion surgery and those with missing medical charts were excluded.
A total of 538 patients were eligible, of which 7 (1%) were deceased, 46 (9%) had incorrect contact details, 17 (3%) declined participation, 125 (23%) did not respond to phone calls, and 6 (1%) had missing charts. This left 337 (63%) patients for the analysis. The average follow-up time was 5.3 years, 4.8 years, and 4.4 years in the PSF, PLIF, and circumferential LLIF groups, respectively (Table 1). Compared with patients lost to follow-up, patients included in the study were older (57 ± 13, 53 ± 15 years, P = .003), more likely to have undergone circumferential LLIF (21%, 11%, P = .008), and more likely to be Caucasian or Asian (P < .001).
The Cost Estimates Used to Determine the Time to the Cutoff Value of $68 672 in Survival Analysis, for Index Procedure, Reoperation Procedure, and Epidural Injectionsa.
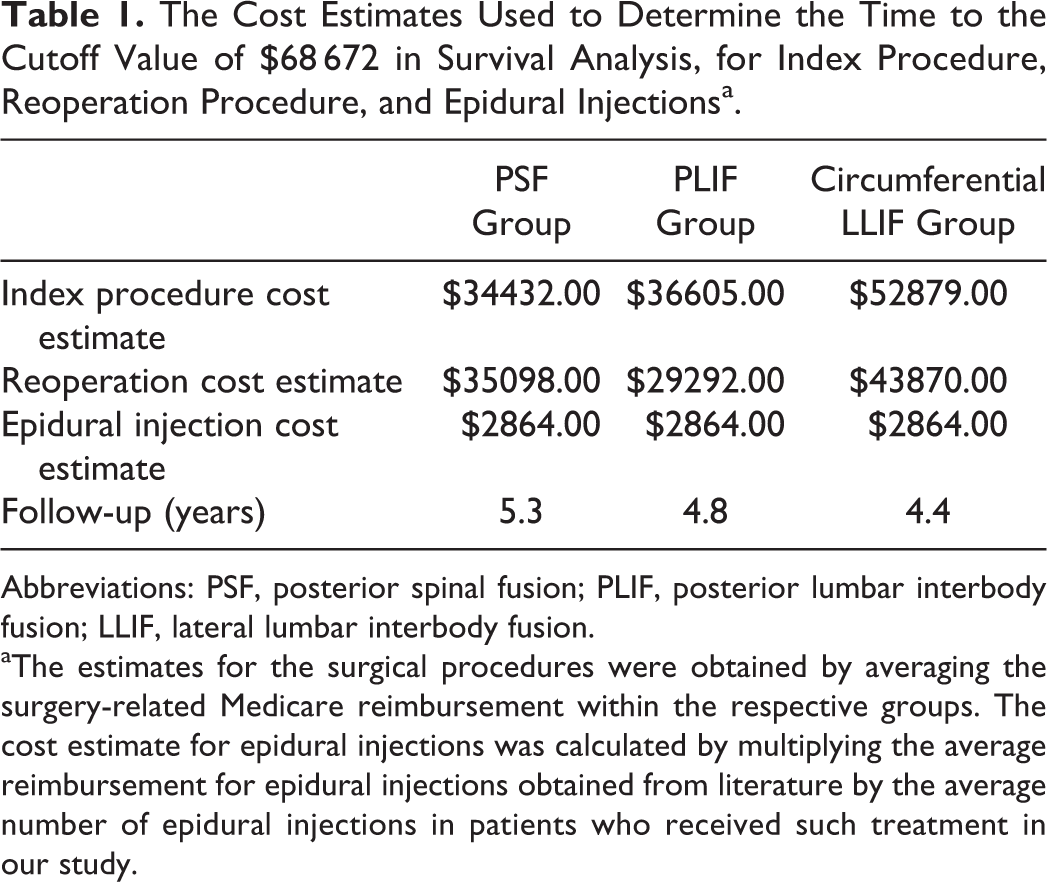
Abbreviations: PSF, posterior spinal fusion; PLIF, posterior lumbar interbody fusion; LLIF, lateral lumbar interbody fusion.
aThe estimates for the surgical procedures were obtained by averaging the surgery-related Medicare reimbursement within the respective groups. The cost estimate for epidural injections was calculated by multiplying the average reimbursement for epidural injections obtained from literature by the average number of epidural injections in patients who received such treatment in our study.
Data Collection
Data was collected and analyzed by 6 independent observers not involved in patient care. Patient charts were reviewed retrospectively, and eligible patients were contacted by telephone to complete a questionnaire on reoperation status, epidural injections, and overall satisfaction. Overall satisfaction was graded on a 5-point Likert scale from “Very satisfied” to “Very dissatisfied” (see the appendix). To minimize chance bias and nonresponse rates, the study investigators attempted calls to study candidates on at least 3 separate occasions at different times of the day with a minimum of 1 week between the first call and the final call.
Actual inpatient hospital reimbursement and physician reimbursement were obtained from the hospital’s finance department for each index and reoperation surgery performed on Medicare patients. This data was not available for privately insured patients. All values were adjusted to 2015 dollars using the consumer price index data from 2008 to 2016. 15
Cost Estimation
In this study, Medicare reimbursement was used as a proxy for cost. Medicare is the US federal insurance program covering all Americans aged 65 years or above, or suffering from certain disabilities. In order to extrapolate Medicare reimbursement values to the larger group of privately insured patients, the average surgery-related Medicare reimbursement (ie, hospital plus physician) for the index surgery in each group was calculated (PSF, $34 432; PLIF, $36 605; circumferential LLIF, $52 879). The average surgery-related Medicare reimbursement for reoperation surgeries in each group was determined likewise (PSF, $35 098; PLIF, $29 292; circumferential LLIF, $43 870; Table 1). These averages were then applied to the index and reoperation procedures for all patients within each treatment group as cost estimate. For example, every PLIF index surgery was assigned the cost estimate of $36 306. Similarly, any reoperation surgery in the PLIF group was assigned the cost estimate of $29 292, irrespective of the type of reoperation in the lumbar spine.
Next, reimbursement data for epidural injections in the years 2008 to 2015 was obtained from the literature, 16 adjusted to 2015 dollars and averaged to arrive at a single reimbursement figure of $659 ± 67 per injection. Telephone follow-up was used to identify the subset of patients who underwent epidural injection, and the average number of such injections in this subgroup was found to be 4 ± 4 injections. Thus, the estimation for the mean cost for epidural injections in this subgroup was $2864 (Table 1). As the exact date of injections was not routinely available, this cost estimate of $2864 was added as a baseline value in this subgroup.
Finally, the estimated total reimbursement for each patient was calculated by summing the estimate for the particular index surgery; the number of reoperations times the estimate for reoperation cost in the respective treatment group; and the cost estimate for injections. The 90th percentile of the total reimbursement at the time of the follow-up telephone call was determined ($68 762) and defined as a cutoff value for high resource utilization. This was preferred over using the mean overall cost for cost-analysis to account for the complex nature of cost data and skewing.
Statistical Analysis
Statistical analysis was performed using SAS version 9.3 (SAS Institute Inc, Cary, NC). All tests were 2-sided and the significance level was set at .05 for all comparisons. Descriptive statistics were generated for the demographic and clinical characteristics of each treatment group. Continuous variables are expressed as mean ± standard deviation and categorical variables as counts and percentages. Comparisons of treatment groups were performed using one-way ANOVA for continuous variables, the Kruskal-Wallis test for ordinal variables (satisfaction questions) and χ2 test for categorical variables. Reoperation rate was defined as the percentage of patients requiring at least one reoperation.
Cost Analysis using Survival Analysis
The primary endpoint was high resource utilization. The time from the index surgery until the time the cost per patient exceeded the cutoff value for high resource utilization ($68 762, see above) was calculated and analyzed using Kaplan-Meier methods and Cox proportional hazards model to account for censoring, as described and discussed extensively in the literature. 17 –21 The time to high resource utilization was compared between the treatment groups using the log-rank test. Multivariate Cox proportional hazards analysis, stratified by insurance status, was used to compare the time to high resource utilization. Models were adjusted for age, gender, body mass index, race, and American Society of Anesthesiologists (ASA) Physical Status score. Stratified analysis was performed to address the difference in distribution of insurance type among the 3 treatment groups.
Satisfaction
Outcome satisfaction was dichotomized into 2 categories: “Very satisfied” and all other responses. Multiple logistic regression analysis was performed to evaluate the influence of the 3 surgical techniques on satisfaction. Models were adjusted for age, body mass index, gender, race, ASA score, and time of follow-up.
Results
Comparison of Patient Characteristics and Surgical Outcomes
There were 337 patients available for analysis. Patients in the PSF group were significantly older (PSF, 72 ± 12; PLIF, 59 ± 13; circumferential LLIF, 65 ± 10 years, P < .001), as such the percentage of PSF surgeries covered by Medicare was highest (PSF, 43%; PLIF, 17%; circumferential LLIF, 19%; P < .001; Table 2).
Demographic, Surgical, and Financial Details for the 3 Treatment Arms, Posterior Instrumented Fusion (PSF), Posterior Interbody Fusion With Posterior Instrumentation (PLIF), and Lateral Interbody Fusion With Posterior Instrumentation (Circumferential LLIF).
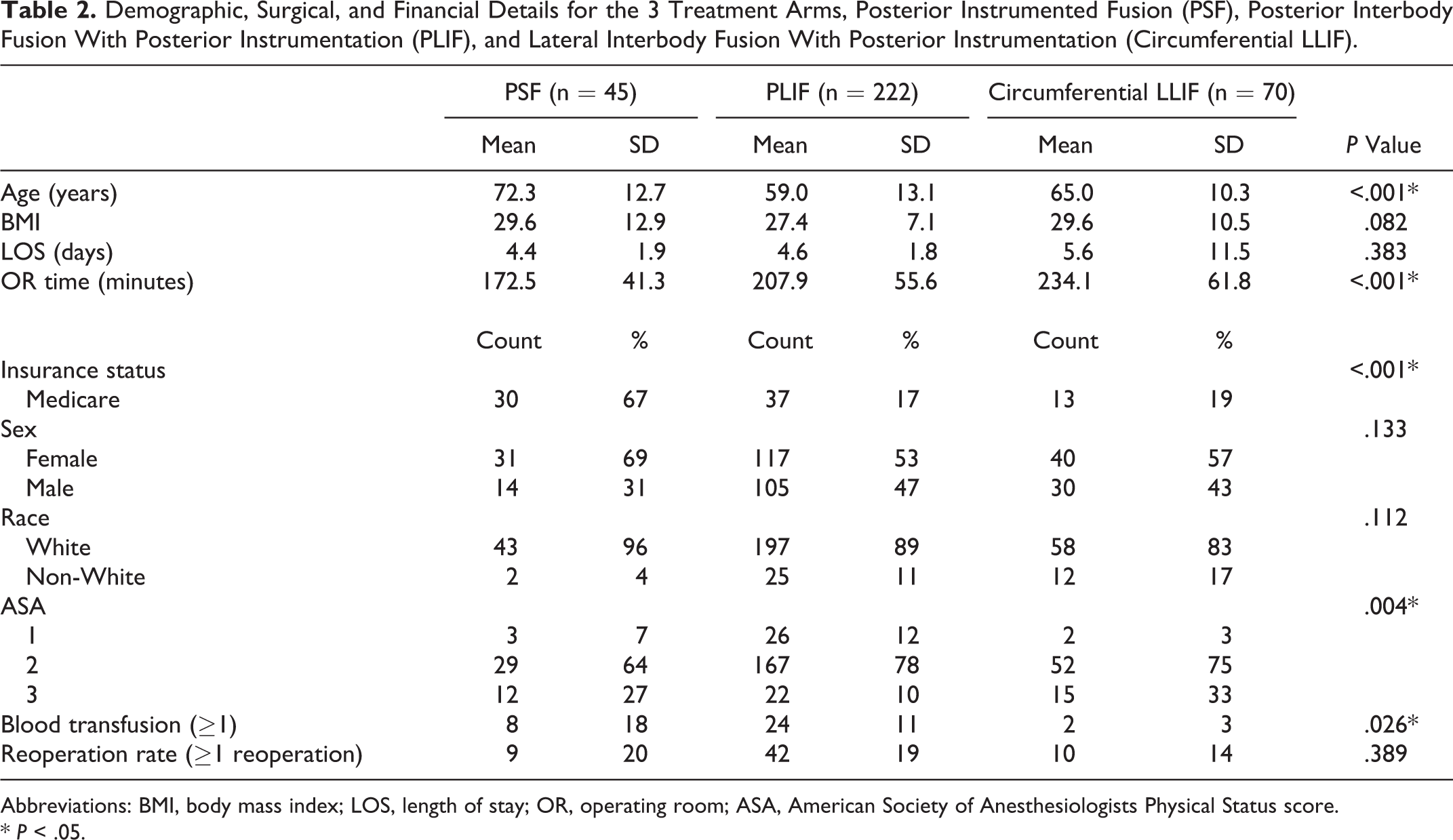
Abbreviations: BMI, body mass index; LOS, length of stay; OR, operating room; ASA, American Society of Anesthesiologists Physical Status score.
* P < .05.
On average, surgical time at the index procedure was lowest in the PSF group (PSF, 172 ± 41; PLIF, 208 ± 56; circumferential LLIF, 234 ± 62 minutes; P < .001; Table 2). The percentage of patients with an ASA score of 1 at index procedure was highest in the PLIF group (PSF, 7%; PLIF, 12%; circumferential LLIF, 3%; P = .004). The use of allogeneic blood transfusions during index procedure was lowest (PSF, 18%; PLIF, 11%; circumferential LLIF, 3%; P = .002) in the circumferential LLIF group. The length of stay after the index procedure was not significantly different between groups (PSF, 4 ± 2; PLIF, 5 ± 2; circumferential LLIF, 4 ± 2 days; P = .369; Table 2).
Cost Analysis
The mean time to the cutoff value of $68 672 was significantly longer in PLIF patients (PSF, 4.6 ± 1.9; PLIF, 4.7 ± 1.6; circumferential LLIF, 4.1 ± 1.0 years; P = .027). A log-rank test comparison showed that the survival distributions of the treatment groups were significantly different (P = .002). PLIF patients were less likely to reach the cutoff value compared with PSF (P = .002) and circumferential LLIF (P = .006) patients, at a mean follow-up of 5.8 years. The reoperation rate (percentage of patients requiring at least one reoperation) was highest in the PSF group, but this was not statistically significant (PSF, 20%; PLIF, 19%; circumferential LLIF, 14%, P = .389).
Cox proportional hazard regression models revealed that patients in the PSF group were 3.3 times more likely to reach the cutoff value of $68 762 compared with PLIF patients (hazard ratio [HR] = 3.280, P = .017). Similarly, patients in the circumferential LLIF group were 3.4 times more likely to reach the cutoff value than PLIF patients (HR = 3.370, P = .017; Table 3).
Results of the Cox Proportional Hazard Regression Analysisa.
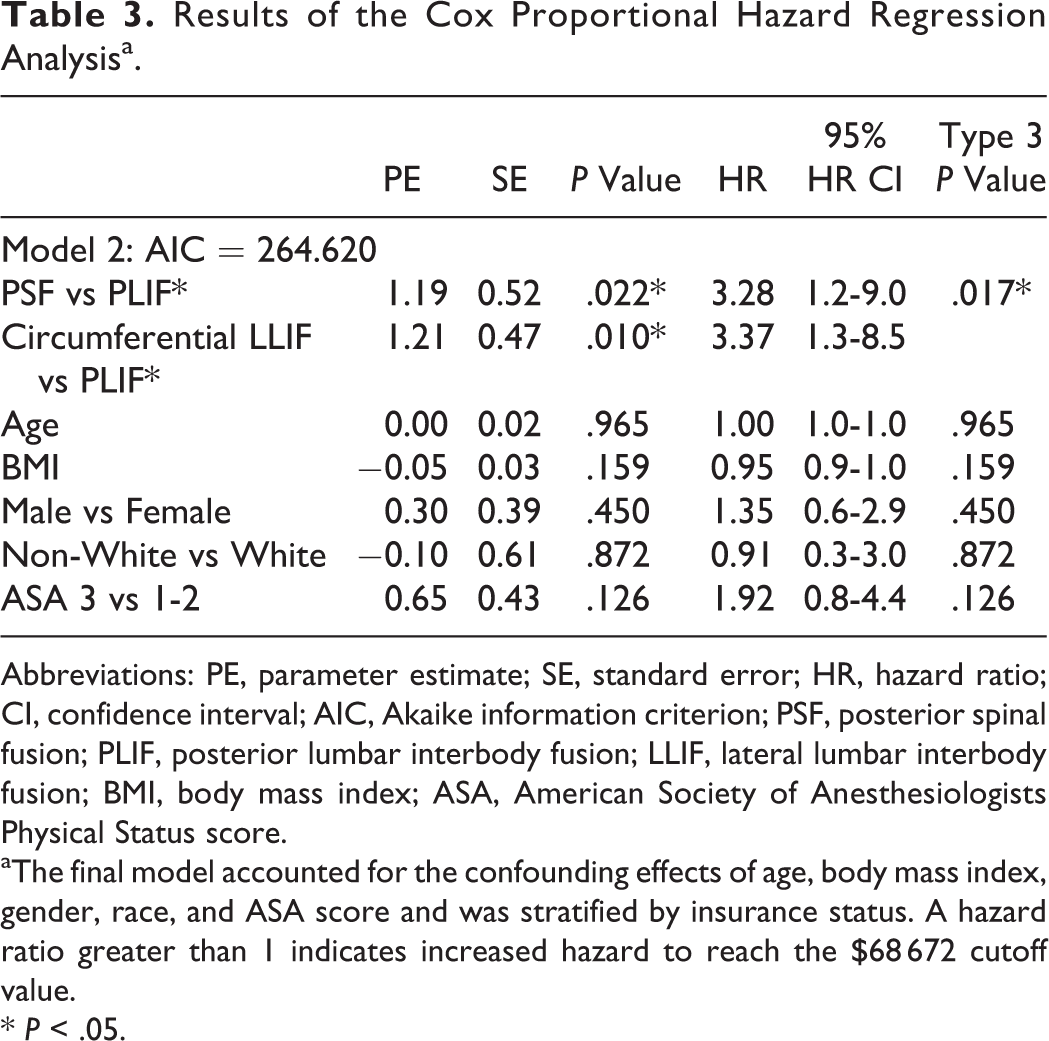
Abbreviations: PE, parameter estimate; SE, standard error; HR, hazard ratio; CI, confidence interval; AIC, Akaike information criterion; PSF, posterior spinal fusion; PLIF, posterior lumbar interbody fusion; LLIF, lateral lumbar interbody fusion; BMI, body mass index; ASA, American Society of Anesthesiologists Physical Status score.
aThe final model accounted for the confounding effects of age, body mass index, gender, race, and ASA score and was stratified by insurance status. A hazard ratio greater than 1 indicates increased hazard to reach the $68 672 cutoff value.
* P < .05.
Satisfaction
There was no statistically significant difference in the percentage of “Very satisfied” patients in bivariate analysis (PSF, 56%; PLIF, 55%; circumferential LLIF, 61%; P = .463). Multivariate logistic regression, however, showed that patients in the circumferential LLIF group were more likely to be satisfied compared with the PLIF group (odds ratio = 3.320, P = .002), while no significant difference was found between the PSF and PLIF groups (odds ratio = 0.560, P = .402; Table 4).
Results of Binary Logistic Regression for Overall Satisfaction With the Outcomea.
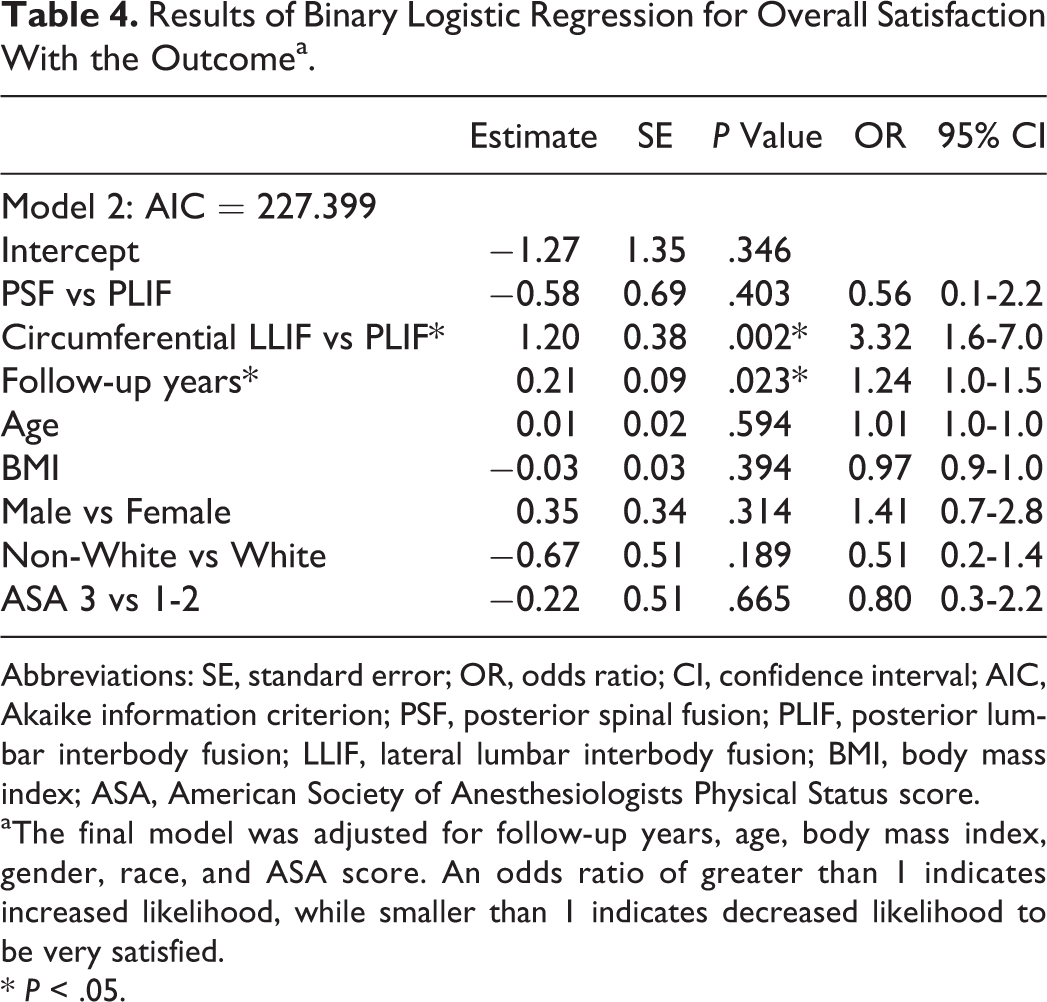
Abbreviations: SE, standard error; OR, odds ratio; CI, confidence interval; AIC, Akaike information criterion; PSF, posterior spinal fusion; PLIF, posterior lumbar interbody fusion; LLIF, lateral lumbar interbody fusion; BMI, body mass index; ASA, American Society of Anesthesiologists Physical Status score.
aThe final model was adjusted for follow-up years, age, body mass index, gender, race, and ASA score. An odds ratio of greater than 1 indicates increased likelihood, while smaller than 1 indicates decreased likelihood to be very satisfied.
* P < .05.
Discussion
In this study, a cost comparison of PSF, PLIF, and circumferential LLIF was performed using survival analysis to assess the differences in time to resource utilization exceeding that of 90% of patients in this study. Multivariate Cox analysis revealed that circumferential LLIF or PSF patients were more likely to have higher resource utilization and thus to incur greater costs to payers at an average follow-up of 6 years. The high cost estimate for index and reoperation procedures in the circumferential LLIF group and for reoperations for PSF patients led to greater costs compared with the PLIF group. In addition, multivariate logistic regression demonstrated that patients in the circumferential LLIF group were more likely to be satisfied with the overall result of their surgery when compared with PLIF patients.
Comparison of Baseline Characteristics and Surgical Outcomes
The PSF group had a significantly higher percentage of Medicare beneficiaries. As Medicare eligibility is based on age (65 years and older) among others, it follows that the average PSF patient in this study was significantly older and had a higher ASA score than those in the circumferential LLIF and PLIF groups. With the possible perception of being the least invasive procedure group examined in the study, PSF was most likely preferentially chosen for these older, sicker patients in most cases.
Our finding of 234-minute operative time for circumferential LLIF at index procedure is consistent with reports ranging from 277 to 477 minutes. 22 Contrary to other studies, 23,24 it was highest in circumferential LLIF in our study, which can be explained by the need for intraoperative repositioning. Our results indicate no statistically significant difference in hospital length of stay (PSF, 4 ± 2; PLIF, 5 ± 2; circumferential LLIF, 4 ± 2; P = .369). This conflicts with other reports in which percutaneous screws were used, however. 23,25
Comparison of Cost and Cost Analysis
The cost estimates for the index procedure used in our study are comparable to the results reported by Nunley et al. Regardless of levels fused, posterior fusion was reimbursed $41 404 and combined anterior and posterior fusion $47 992 by Medicare. 26
Multivariate Cox regression analysis showed that patients in the PSF and circumferential LLIF groups were 3.3 and 3.4 times more likely to incur high costs (ie, more than $68 762) to payers compared with PLIF. While the reoperation rate was highest in the PSF group, this was not statistically significant. This, as well as high cost estimates for index and reoperation procedures in the circumferential LLIF group and for reoperation in the PSF group, explains why PSF and circumferential LLIF patients were more likely to have high resource utilization in our study. In 2012, Lucio et al compared the cost incurred to the hospital within 45 days of 2-level open PLIF to that of circumferential LLIF in 210 patients. 23 The study found that circumferential LLIF was significantly less expensive both in terms of the index procedure ($23 687, $25 272) and total costs at 45-day follow-up ($24 230, $27 055). While Lucio et al examined costs incurred to the hospital during a 45-day period, our study defined cost as reimbursement paid by Medicare over an average follow-up of 6 years.
Bydon et al conducted a cost-effectiveness study comparing patients undergoing single- and multilevel posterior or transforaminal lumbar interbody fusion (PLIF or TLIF) to patients undergoing posterior instrumented fusion (PSF). The average cost for interbody fusion was $54 827 compared with $47 822 for posterior instrumented fusion. The cost-effectiveness ratio, including index surgery and first reoperation, favored PSF. When including 2 PSF patients requiring a second reoperation, the total cost-effectiveness ratio of an interbody fusion relative to an instrumented fusion was $9 884 per QALY. The authors conclude that these findings suggest moderate long-term cost-effectiveness and better functional outcomes with interbody fusion, supporting our findings. 8
Contrary to our results, Soegaard et al concluded that circumferential fusion was more cost effective than instrumented posterolateral fusion. 12 This study performed a cost-utility analysis per QALY from a societal perspective. Thus, all costs, such as surgical costs, reoperations and rehospitalizations, service in the primary health care sector, medication, and productivity loss, were included in the study. Some of these costs, such as productivity loss, were based on estimations and thus introduce variability to the data especially when considering older, retired patients. While Soegaard et al found that circumferential fusion was less expensive from a societal perspective, 12 our data revealed from a long-term payer’s perspective that PLIF incurs less cost than LLIF. Furthermore, the cost-utility analysis performed by Soegaard et al is based on the concept of QALYs, which were recently shown to be a questionable measure that can lead to inconsistent recommendations. Thus, for this study a different approach to cost analysis (using Cox regression to analyze time to high resource utilization) was chosen instead of a QALY-based cost-analysis in order to minimize varying cost estimates.
Comparison of Overall Satisfaction
Multivariate analysis showed that a longer follow-up period (odds ratio = 1.2), as well as circumferential LLIF (odds ratio = 3.3) compared with PLIF, were predictors of greater overall satisfaction. This might be related to better functional outcomes as reported previously. Pawar et al showed that circumferential LLIF patients compared to PLIF patients had a significantly better improvement in Oswestry Disability Index scores after an average follow-up of 16 months. 24
Limitations
(1) This study was conducted as a retrospective case-control study. Data was collected from chart review and telephone follow-up. (2) While the present study benefits from the use of actual Medicare reimbursement data, similar information from private payers was not available. Reimbursement was extrapolated to procedures covered by private insurers. For this study reoperation costs were calculated based on the actual reoperation surgery performed utilizing available cost data from Medicare patients. Furthermore, it is important to note that American reimbursement data was used for this study and thus the findings from this study may not be applicable to other countries. (3) This cost-analysis was performed from the payer’s perspective. It does not account for direct costs to the insurer related to physical therapy, medication, and physician office visits. These expenses are typically negligible when compared with those of surgical procedures, would not differ largely, and are difficult to ascertain via telephone follow-up. (4) Patient satisfaction at a single time point, while important, should not be viewed as a surrogate of health-related quality of life measurements. (5) The overall follow-up rate in this study was 63%, which is comparable to a follow-up of 66% in a study with similar design. 27 Older patients, circumferential LLIF patients, and white and Asian patients were more likely to complete this survey. Thus, a response bias cannot be excluded. This must be considered when interpreting the results of this study.
Conclusion
This study compared costs associated with single-level PSF, PLIF, and circumferential LLIF at a tertiary spine center with a mean follow-up of 6 years. Cost analysis, using survival analysis, indicated that PLIF incurred fewer costs than PSF and circumferential LLIF, but circumferential LLIF patients were more likely to be satisfied than PLIF patients. In the setting of higher index cost for circumferential LLIF, longer follow-up may be required to show a cost benefit over PSF or PLIF. Considering the high costs associated with spinal surgery and the goals of a value-based health care system (highest quality of care at minimal cost), this study provides valuable evidence for surgeons to draw upon in their decision making regarding lumbar fusion surgery. Ongoing research is required for definitive conclusions.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Huong Do has received research support from the National Center for Advancing Translational Sciences. Federico P. Girardi declares conflict of interest with the following companies not related to this study: Lanx, Nuvasive, Orthodevelopment Crop, Depuy Spine, Small Bone Innovations, Pioneer Surgical Technology, LifeSpine, Centinel Spine, Spinal Kinetics, Paradigm Spine, Gerson Lehrman Group, SpineArt USA, Pharmawrite, Scient’x USA, HealthPoint Capital, and MiMedx. Andrew A. Sama declares conflict of interest with the following companies not related to this study: Ortho Development Corportation, Depuy Spine, Sentio, Paradigm Spine, Clariance, MiMedx, Spinal Kinetics, Aesculap, AO Spine. Alexander P. Hughes declares conflict of interest with the following companies not related to this study: Altus Spine, MiMedx, Nuvasive. Frank P. Cammisa declares conflict of interest with the following companies not related to this study: Nuvasive, Alphatec Spine, Paradigm Spine, Small Bone Innovations, Scient’x USA, Spinal Kinetics, Vertebral Technologies, Vertical Spine, BI Members, BioAssets Development Corp., Healthpoint Capital Partners, Ivy Healthcare I and II, Promethean Surgical Devices, Liventa BioScience, Royer BioMedical, Viscogliosis Brothers, Woven Orthopedic Technologies, 4 Web Medical, Spine Partners III, Bacterin, Novobone, Integra, NuTech, Depuy.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.