
Abstract
Study Design:
Prospective observational cohort study.
Objectives:
To analyze clinical and economic results in patients with degenerative disc disease in the lumbar area for patients who received combined anterior and posterior fusion or total disc replacement (TDR).
Methods:
The study included 75 patients, 38 in the fusion group and 37 in the TDR group, who received either anterior/posterior fusion or TDR for lumbar disc disease from January 2005 to December 2008 with a minimum follow-up of 24 months. We collected data with regard to clinical parameters, demographics, visual analogue scale scores, Oswestry Disability Index scores, SF-36 and SF-6D data, surgery time, amount of blood loss, transfusion of blood products, number of levels, duration of hospital stay, and complications. For cost analysis, general infrastructure, theatre costs, as well as implant costs were examined, leading to primary hospital costs. Furthermore, average revision costs were examined, based on the actual data. Statistical analysis was performed using t tests for normal contribution and Mann-Whitney test for skew distributed values. The significance level was set to .05.
Results:
There was a higher surgery time, more blood loss, and longer hospital stay for the fusion group, compared with the TDR group. In addition, the hospital costs for the primary procedure and revision were 35% higher in the fusion group. The clinical data in terms of SF-36 and SF-6D showed no difference between these 2 groups.
Conclusions:
TDR is a good alternative to anterior and posterior lumbar fusion in terms of short follow-up analysis for clinical data and cost analysis. General advice cannot be given due to missing data for long-term costs in terms of surgical treatment of adjacent level or further fusion techniques.
Keywords
Introduction
World health care expenditure (percentage of gross domestic product) is currently reported to be 9.9%. 1 Musculoskeletal disorders account for a significant part of health care costs in Western countries due to the aging population. The overall costs for treatment of acute and chronic low back pain (LBP) account for 17% of total health care costs in Sweden. 2 -4 Only 10% to 20% of this is related to direct medical costs, 5 while 80% comprise indirect costs due to loss of productivity. 4 Direct costs for surgical treatment of LBP account for a relatively small but increasing part of total hospital costs. 5 The number of surgical procedures for LBP in adults increased from 147 500/year in 1979 to 279 000/year in 1990 in the United States, according to Taylor et al, 6 accounting for an increase in yearly prevalence from 109 to 158/100 000 adults. Over the same period, a 100% increase in the number of lumbar fusion procedures has been reported (from 13 to 26/100 000 adults per year). 6
Degenerative disc disease (DDD) is considered the most frequent cause of chronic LBP in adults. If conservative treatment fails, surgery is generally indicated. 4 Spinal fusion is the most common treatment for DDD-related LBP as it is historically considered the gold standard treatment for this condition. 4,7 -9 Nevertheless, several studies have reported significant rates of perioperative complications as well as prolonged postoperative recovery times. Furthermore, lumbar fusion has been shown to accelerate adjacent segments degeneration, which, in turn, can lead to persistent or new pain and disability. All these factors have led to the development of motion-preserving technologies for surgical treatment of LBP. 10
Artificial total disc replacement (TDR) is a relatively new technology that has been adopted by many institutions over the years as an alternative treatment strategy for LBP. 11 -13 Potential advantages of TDR over fusion are shorter recovery period and lower rates of adjacent segments degeneration, which can, in turn, decrease the number of revision procedures. Although these advantages are often cited by advocates of TDR, they have been more difficult to prove in the literature, and indications for TDR versus fusion are still highly debated among surgeons. 14 -18 Furthermore, several cost-comparison studies have been attempted in the past, but none of these is available for patients within the National Health Service in the United Kingdom to the best of our knowledge.
The aim of this study is to conduct a prospective cost-analysis comparing lumbar TDR and circumferential fusion surgery for discogenic LBP in adults in a tertiary referral spinal surgery center in the United Kingdom.
Material and Methods
Following institutional board review approval (as part of service evaluation and adhering to the Helsinki Declaration), we did a prospective, nonrandomized data collection of patients treated in our institution for anterior-posterior circumferential fusion as well as anterior TDR in the lumbar area and lumbosacral junction (L5/S1) in the years 2005 to 2008.
The study population was divided into 2 groups: a group of patients (fusion group) with anterior and posterior fusion with allograft and lamina screws or titanium cage and pedicle screws and a second group with TDR (TDR group). The primary endpoint of the study was the 24-month follow-up examination.
For clinical data, the visual analogue scale (VAS), Oswestry Disability Index (ODI), and National Health Service hospital parameters such as age, sex, body mass index (BMI), length of symptoms as well as time for surgery, given blood products, number of levels, and inpatients days were included. Furthermore, for the period between the primary discharge date and the 24-month follow-up, revision surgeries and costs, as well as further inpatients stays due for injections were noted.
The treating consultant together with the patient decided the type of surgery. Usually more than 6 months of chronic discogenic LBP, failure of conservative treatment, 1- or 2-level positive discographically proven discogenic LBP was seen as the indication. Meyerding grade II or greater spondylolisthesis, active or systemic infection, osteoporosis, higher graded spinal stenosis, major deformity pregnancy, negative discogram, or the presence of active malignancy was seen as exclusion criteria.
For the fusion group, 2 techniques of posterior fixation were performed in the study, namely, translaminar screw fixation or pedicle screw fixation. Translaminar screws are placed via stab incisions as described by Montesano (Figure 1), 19,20 and pedicle screws are placed in the standard technique. 21
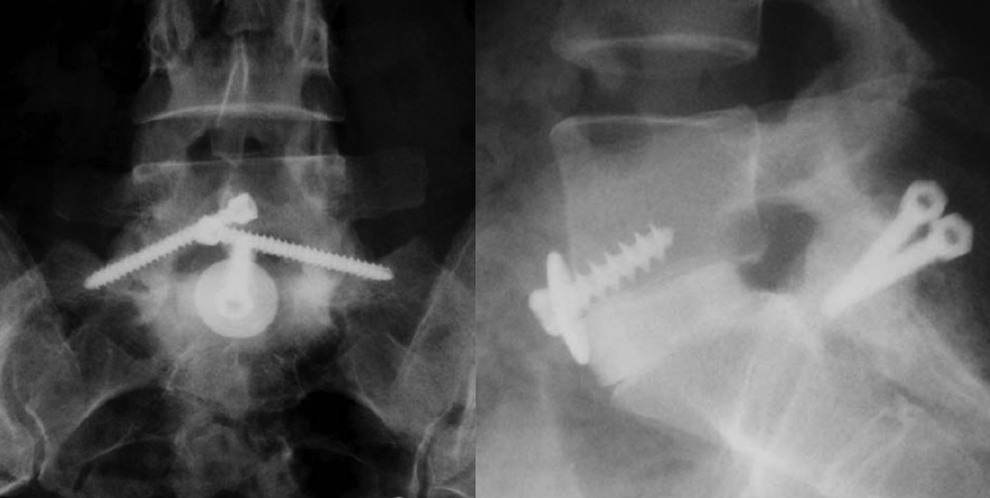
Illustration of a case of posterior Magerl screws and femoral ring allograft.
After that, the patient is turned supine and re-draped. The lumbar spine was exposed via a retroperitoneal approach, and for the visualization of the disc, Steinmann pins or Synframe retractors (Synthes, Zuchwill, Switzerland) were inserted. The surgical level was identified using intraoperative radiographs and a complete discectomy was carried out. The vertebral body endplates were prepared by curetting until point bleeding was seen as described by McKenna et al. 19 After trial implants, a femoral ring allograft (see Figure 1) larger than the measured disc space was inserted and secured with a 6.5-mm large fragment cancellous screw and a washer. 19 For other patients, a titanium cage (Syncage; Synthes, Zuchwill, Switzerland; see Figure 2) was used instead of the allograft.
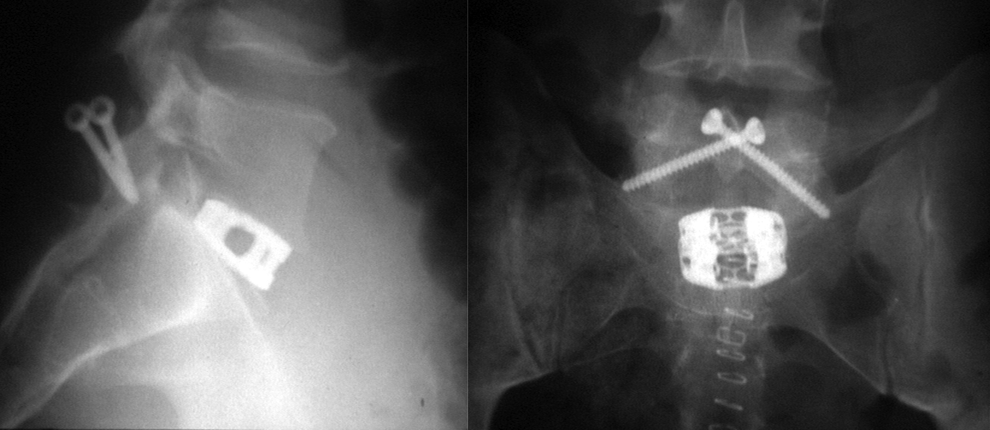
Illustration of a patient treated with screws, anterior discectomy, and implantation of a titanium cage.
For the treatment with TDR, the technique follows the anterior retroperitoneal approach, as a disc replacement, ProDisc (Synthes, Zuchwill, Switzerland; see Figure 3) was used in all cases.
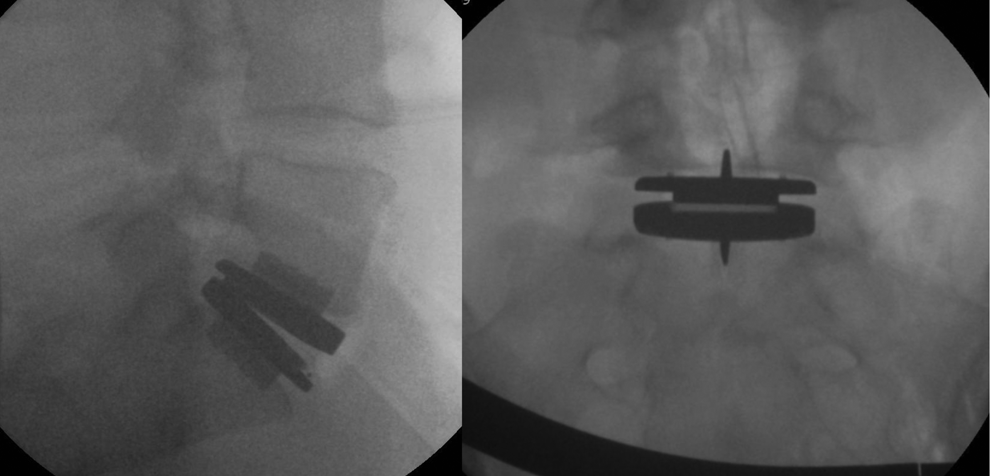
Illustration of a case with anterior total disc replacement.
For both patient groups, no patient received immobilization by brace postoperatively. Postoperative physiotherapy was initiated in hospital and further extended with local sessions and a home exercise protocol for 5 to 6 months after surgery.
For further clinical aspects, all patients completed the Short Form-36 (SF-36) health survey 22 at baseline, 6, 12, and 24 months. In order to derive a preference-based measure of health, the SF-36 data were revised into a 6-dimensional health state classification, the SF-6D as described earlier. 21 -24
For cost analysis between these 2 procedures, costs aspects from a previous publication of our institution was used and adapted to our calculation. 21 For the primary cost analysis, operation theatre costs as well as costs for blood units and preservation, ward costs, and implant costs were analyzed. Further necessary procedure costs for treatment of ongoing pain or complication, which included surgical interventions, were analyzed. Surgery time was calculated as the time the patients spend in the operation theatre with anesthesia time, surgical preparation, surgical procedure, and aftercare in the operation room. In our analysis, medical staff was assumed not to vary between patients. 21 The operation theatre costs include overhead costs and building charge as well as spinal surgery and theatre equipment besides implants costs.
Statistical Analysis
For statistical analysis, utilizing GraphPad Prism (GraphPad Software, San Diego, CA) and Microsoft Excel (Microsoft, Redmond, WA), Student’s t test was performed in case of normal distribution; in skew distributed data the Mann-Whitney U test was used. The significance level was set to .05.
Results
Overall, 75 patients were included in the prospective study from 2005 to 2008, 38 in the fusion group and 37 patients receiving TDR (TDR group). All patients were seen at 24-month follow-up.
The average age at time of surgery was 41.9 ± 8.2 years, while the age distribution did not differ. Furthermore, in the preoperative assessment, BMI and length of symptoms did not differ between the 2 groups, as well as the VAS score for leg pain and ODI values. However, there were significant differences for preoperative back pain between the 2 cohorts. Detailed values for preoperative assessment can be found in Table 1.
Demographics and Preoperative Data.
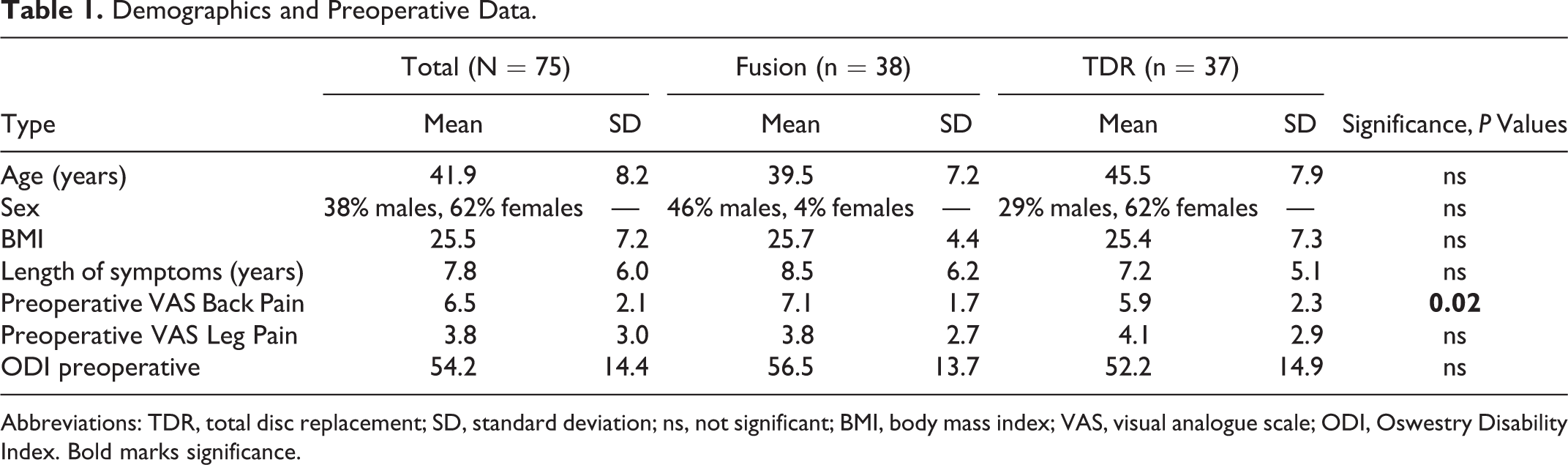
Abbreviations: TDR, total disc replacement; SD, standard deviation; ns, not significant; BMI, body mass index; VAS, visual analogue scale; ODI, Oswestry Disability Index. Bold marks significance.
In the postoperative analysis (see Table 2), we found higher values for time of surgery, blood units used, number of levels treated, and inpatients days for the fusion group compared with the TDR group. However, clinical follow-up scores as measured with the VAS and ODI did not differ between the 2 groups. Even though in every patient the L5/S1 junction was included in the fusion group, the average number of levels treated was higher in the fusion than in the TDR group.
Postoperative Data of Both Patient Cohorts.
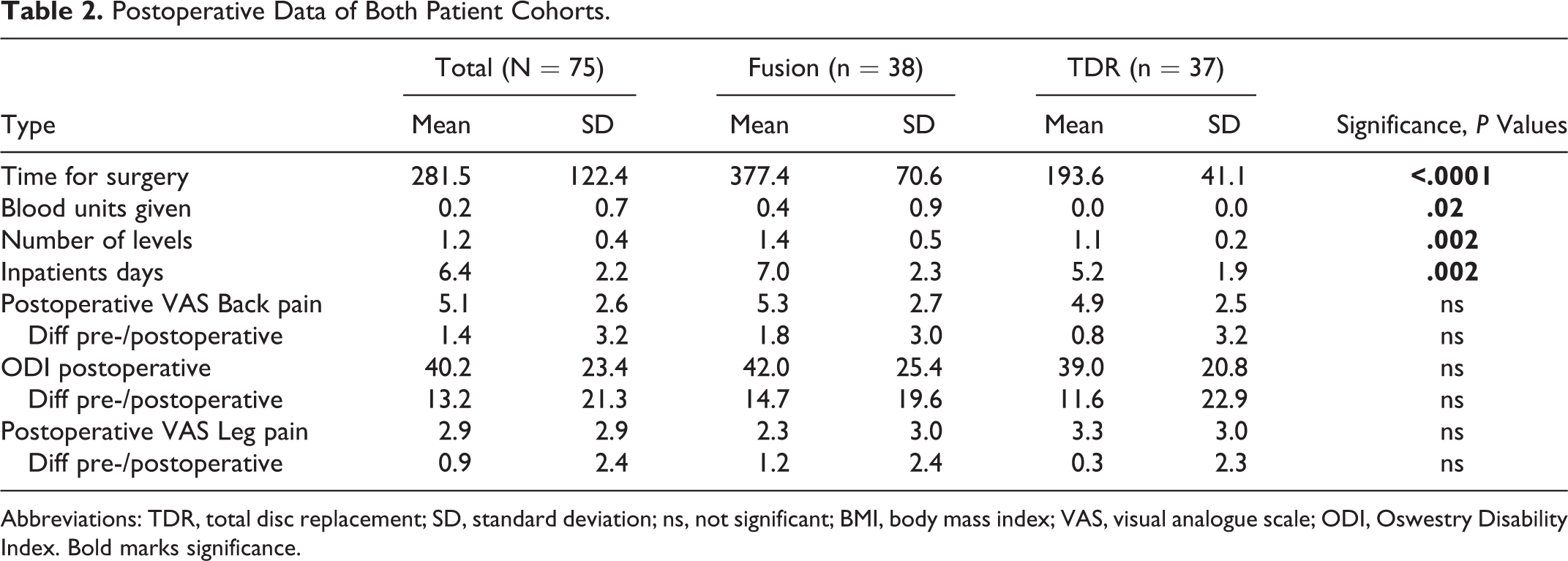
Abbreviations: TDR, total disc replacement; SD, standard deviation; ns, not significant; BMI, body mass index; VAS, visual analogue scale; ODI, Oswestry Disability Index. Bold marks significance.
For the TDR group, 7 patients received injection therapy with a median time of 214 ± 134 days after first procedure and a total stay in hospital of 18 days; no patient received surgical revision in the first 24 months.
In the fusion group, 5 patients received an injection therapy with a mean time of 12 ± 6 days to the first index procedure and hospital stay of further 6 days; furthermore, in 8/38 patients (21.1%) postoperative complication occurred, which needed further surgical intervention, leading to a total of 78 inpatient days. The complications included 4 debridements due to hematoma or infection, 1 removal of a translaminar screw, 1 repair of a meningomyeolocele, and 2 patients needing further posterior 2-level posterolateral fusions (L4 to S1); all complications contributed to 1447 additional operating theatre minutes and 2 more blood units.
The SF-6D analysis showed significant improvements for physical function, general health, bodily pain, vitality, and social function for both groups in the preoperative and 24-month examination as well as for mental health in the fusions group. Nevertheless, the comparison of SF-6D between preoperative and 24 months showed no difference in the subvalue analysis. Details are shown in Table 3.
SF-6D, Calculated From SF-36 Questionnaire Data of the 2 Patient Cohorts.
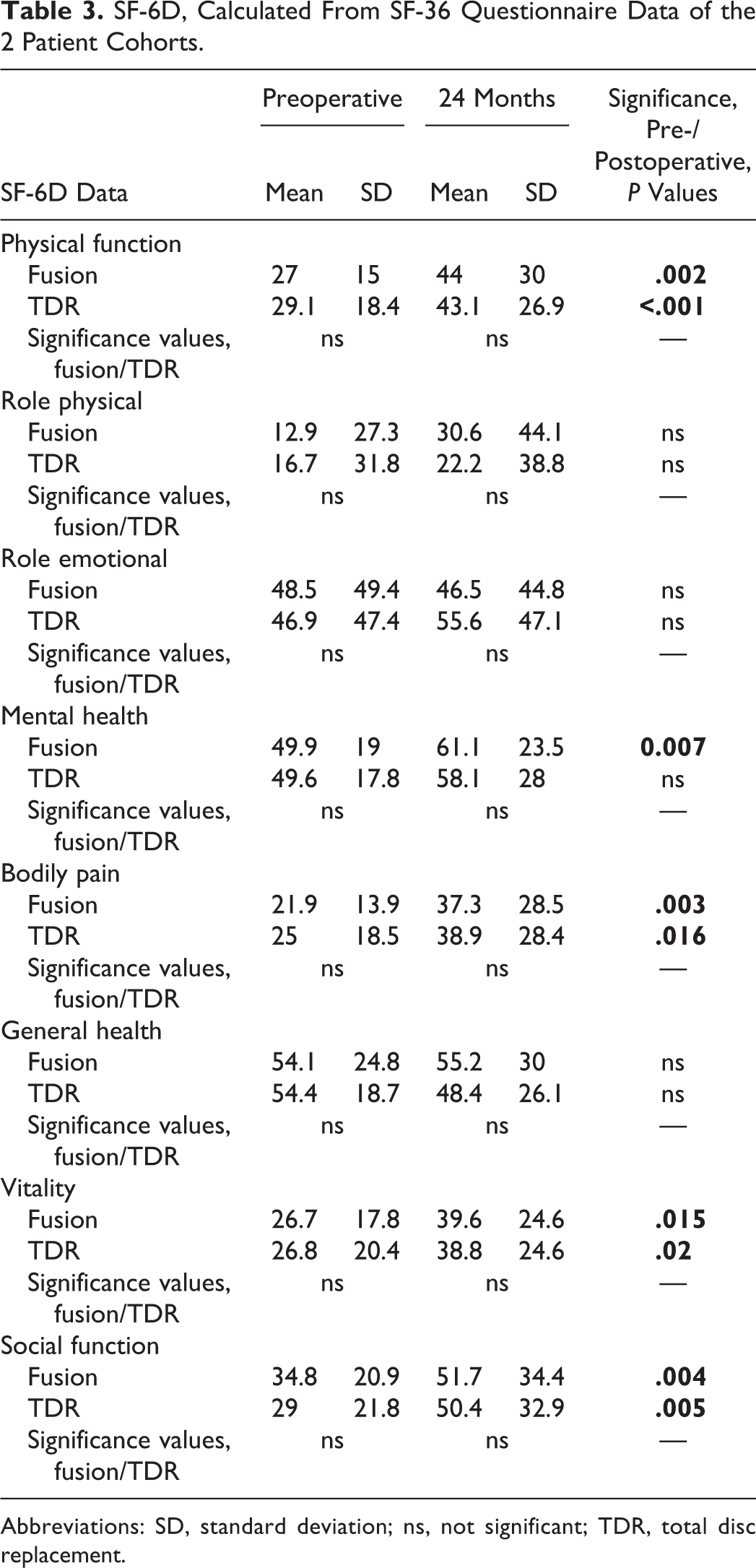
Abbreviations: SD, standard deviation; ns, not significant; TDR, total disc replacement.
The cost analysis for primary surgery revealed mean primary costs of £9012.7 for the fusion group and £7057.0 for the TDR group. While for the fusion group, in 25 patients and 36 levels, pedicle screws and a titanium cage was used, in 13 patients and 15 levels, a femoral allograft and Magerl screws were used. Detailed calculation of the expenses can be found in Table 4.
Primary Hospital Costs.
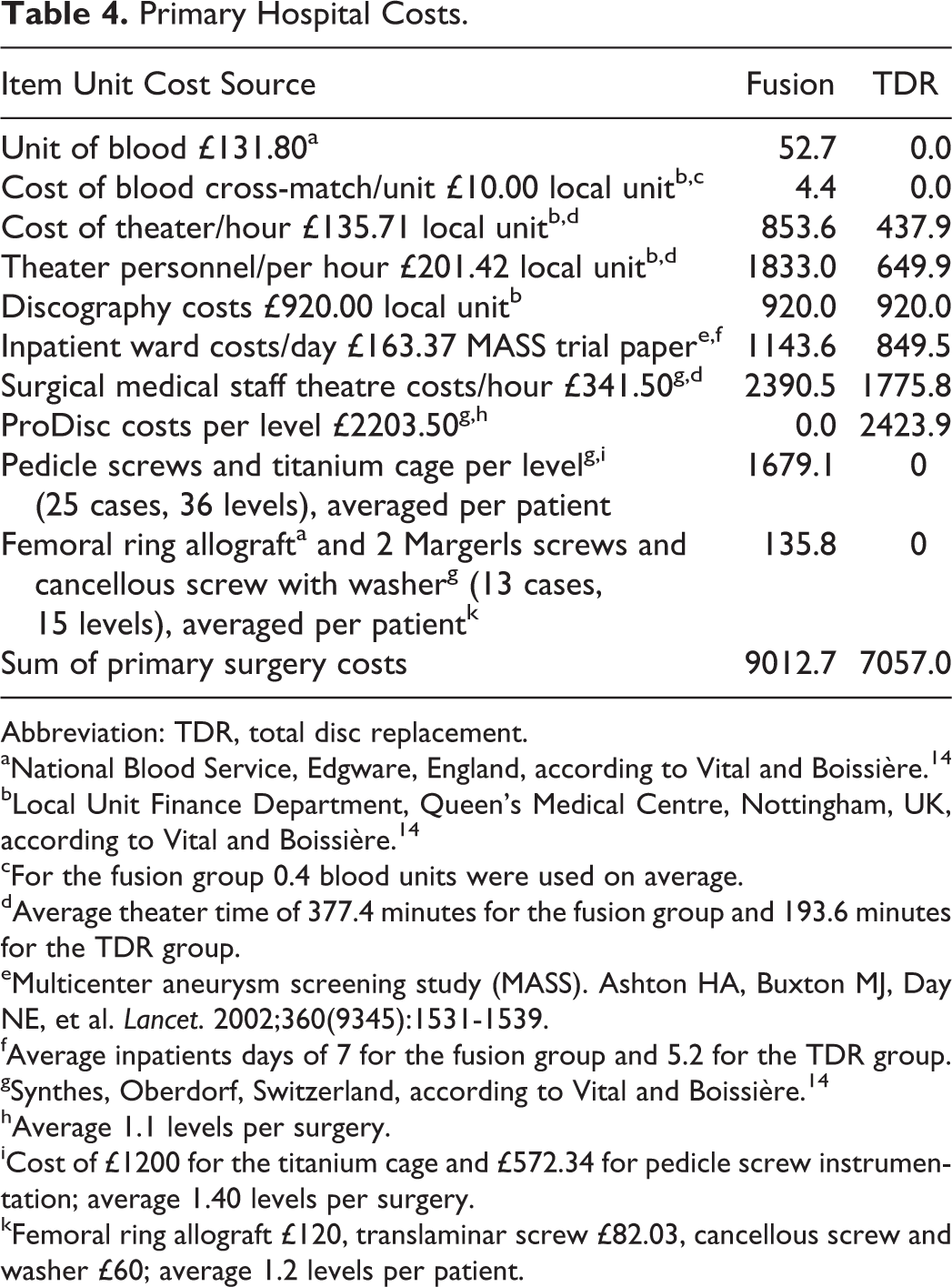
Abbreviation: TDR, total disc replacement.
aNational Blood Service, Edgware, England, according to Vital and Boissière. 14
bLocal Unit Finance Department, Queen’s Medical Centre, Nottingham, UK, according to Vital and Boissière. 14
cFor the fusion group 0.4 blood units were used on average.
dAverage theater time of 377.4 minutes for the fusion group and 193.6 minutes for the TDR group.
eMulticenter aneurysm screening study (MASS). Ashton HA, Buxton MJ, Day NE, et al. Lancet. 2002;360(9345):1531-1539.
fAverage inpatients days of 7 for the fusion group and 5.2 for the TDR group.
gSynthes, Oberdorf, Switzerland, according to Vital and Boissière. 14
hAverage 1.1 levels per surgery.
iCost of £1200 for the titanium cage and £572.34 for pedicle screw instrumentation; average 1.40 levels per surgery.
kFemoral ring allograft £120, translaminar screw £82.03, cancellous screw and washer £60; average 1.2 levels per patient.
Altogether, in the TDR group 1.1 levels were addressed, while in the fusion group, there were 1.34 levels on the average patient, which received anterior-posterior surgery.
The costs per level, averaged to the patient and adjusted for hospital, personnel, implant, and blood costs and was £7098.2 for the fusion group and £6756.3 for the TDR group, concerning primary costs.
The costs for revision surgery and procedures was calculated on the actual incidence of needed surgery, injection, and inpatient days in our patient cohort, as described above. The costs for surgical revision were calculated using actual parameters for implants, operation theatre, and blood products as well as inpatient days, while for injection procedures, despite the inpatient days, each injection was calculated with 30 minutes of operation theatre time, but with only 50% surgical staff and 50% medical personnel costs.
A detailed cost analysis for revision surgery is shown in Table 5. Overall, TDR costs are about 33.35% lower in comparison to the fusion group.
Revision and Total Hospital Costs for 24 Months.
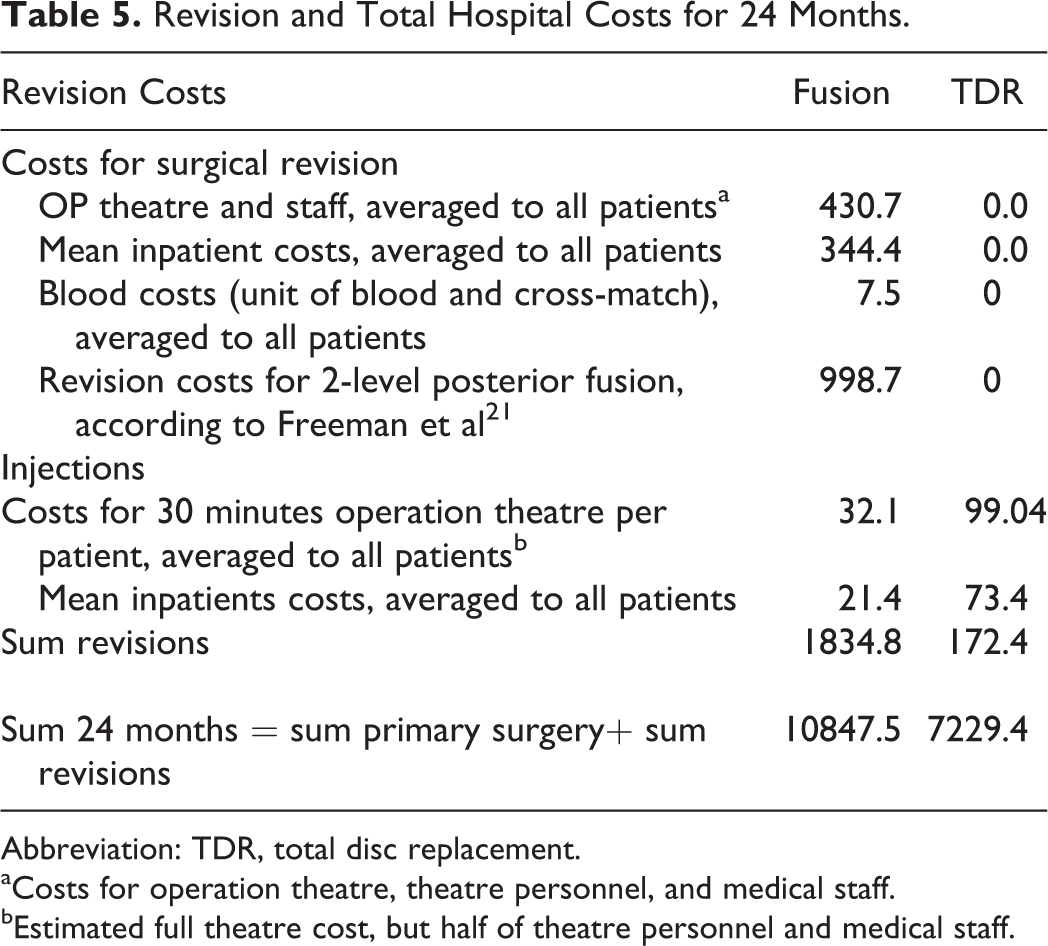
Abbreviation: TDR, total disc replacement.
aCosts for operation theatre, theatre personnel, and medical staff.
bEstimated full theatre cost, but half of theatre personnel and medical staff.
Discussion
Our prospective study demonstrated comparable clinical result in patients treated with lumbar circumferential fusion versus TDR but 33% lower total costs in the TDR group.
Chronic back back has a lifetime prevalence >70% and an annual prevalence of 15% to 45% in the adult population. 25 While most of the patient tend to have intermittent episodes of LBP, up to 10% of patients will develop chronic LBP with a slow and unpredictable recovery. 26 Etiology of chronic LBP is poorly understood. DDD refers to a process whereby normal biomechanical function of the disc nucleus-annulus complex is altered, resulting in chronic pain and disability. 26
The socioeconomic impact of LBP in Western countries is huge. In the United States, back pain is one of the leading causes for hospital admission and the third most common indication for surgery. Short-term studies have demonstrated comparable clinical outcomes between TDR and lumbar fusion, 27,28 but economic aspects of disc arthroplasty in the United Kingdom have not been published or studied before. Fusion surgery is still considered the gold standard for treatment of DDD, although TDR is a common alternative method of treatment. Both procedures are aimed at reducing pain, decreasing disability, allowing early return to work, and increasing quality of life. Nevertheless, patient selection remains a critical factor to achieve good results. 29 Data from the Swedish spine register have shown an average patient satisfaction after fusion surgery of 70%. 30 TDR has gained in popularity in recent years, although the technique has been known since the early 1980s. 31 Restoring and preserving mobility in the motion segment(s) could theoretically minimize risk of relapse of symptoms caused by progressive degenerative changes in adjacent motion segments. 32,33 However, cost-effectiveness for either of the procedures may have an impact on the frequency each procedure is performed.
The average age at time of surgery in our 2 cohorts was comparable, and the sex distribution was comparable to other studies. 18 Furthermore, in the preoperative assessment, BMI and length of symptoms did not differ between the 2 groups, as well as the VAS score for leg pain and ODI values. This shows a homogeneous distribution of patients within the 2 groups. Nevertheless, the 2 cohorts showed significant higher back pain preoperative, which in our opinion did not have any impact on the choice of either of the procedures by the patient. This is supported by the results of other studies, where authors described a significant higher amount of leg pain preoperative in the fusion group, 5,18 whereas the postoperative comparison could not reveal any differences in terms of pain. These findings are confirmed in our study.
Operative time in the fusion group was almost double when compared with the TDR group. This may be explained by the fact that the average patient in the fusion group received a 1.34-level surgery versus 1.1 levels for the patients in the disc replacement group.
Further explanations are that a 2-stage procedure was used in the fusion group. This can also explain the increased blood loss and higher transfusion rate in the fusion group. 18 Vascular complications during anterior spinal surgery are reported as high as 15%. 34,35 Postoperatively, hospital admission was longer in the fusion group than in the TDR group, and this finding is also confirmed by other studies due to longer wound healing times for fusion surgery, as well as more pain and delayed mobilization as reported by Blumenthal et al. 15 The postoperative VAS and ODI scores at the 2-year follow-up did not show any difference in the 2 groups. This is also consisted with previously reported studies. 5,18,19,22
Overall, the clinical assessment via the SF-36 questionnaire revealed significant postoperative improvements in both groups in terms of physical health, mental health, bodily pain, vitality, and social function. We did not find any difference between the 2 study groups at any time point. Zigler et al 28 and Delamarter et al 36 have reported significant differences for the SF-36 between the fusion and TDR groups in their studies. On the other hand, Berg et al found no differences in the SF-36 and EQ5D questionnaires’ comparison at 24-month follow-up. 18 Nevertheless, a significantly higher number of patients in the TDR group was reported to be totally pain free after 2 years (30% vs 15%). Other authors have described comparable clinical outcomes after 2 years. 37
In our study, none of the patients in the TDR group underwent further surgery over the 24-month follow-up, whereas 21.3% of patients in the fusion group needed surgical revisions. Our overall complication rates are similar to those reported by Zigler et al. 28 Berg et al 18 reported a complication rate of 21% in the fusion group and 18% in the TDR group but only a 10% complications rate in both groups that needed revision surgery. According to the same authors, the most common complication in the fusion group was adjacent-level degeneration, while in the TDR group patients needed fusion due to persisting pain at the level of the operated disc. 18 In our study, 7 patients in the TDR group received injection therapy with a median time of 214 ± 134 days after first procedure and a total stay in hospital of 18 days. In the fusion group, only 5 patients received an injection therapy with a mean time of 12 ± 6 days to the first index procedure and hospital stay of further 6 days. Nevertheless, the VAS scores at the 24-month follow-up showed no difference between the groups.
Our cost analysis for the primary procedure showed higher costs for theatre, medical staff, and blood products for the fusion group. These findings can be easily explained by the longer duration of the fusion surgery and more levels per patient. On the other hand, implant costs were higher for TDR, as also confirmed by other studies. 5,6,26,38 In a similar study, Fritzell et al did not observe any difference between TDR and fusion surgery in terms of cost-effectiveness. 5 Other authors used a comparable approach in their studies and reported similar findings. 39,40
The revision costs further increased the differences between the 2 study groups, leading to up to 34% higher costs for fusion surgery in our study. These costs are driven by the high rate of revision surgery in the patient group with fusion surgery and may differ for other cohorts with different revision rates.
There are several limitations in our study that may have had impact on the results and interpretation.
Our study focused on hospital charge costs only, and external costs (need for physiotherapy), ongoing pain treatments, as well as lifetime costs were not included in our analysis. Furthermore, for revision costs, we did not account for opportunity costs. 41 Opportunity costs are those that could have been generated if another patient received surgery in the same timeframe with higher reimbursements and could have an even higher impact in the cost calculation for revision surgery. Furthermore, inflation costs were not included in the analysis.
Additionally, it must be noted that our study compared posterior-anterior circumferential fusion to anterior-only disc replacement. Single-stage anterior fusion surgery (anterior lumbar interbody fusion), which might be the common fusion procedure for DDD in other departments, might have led to different findings.
The study had a prospective design; nevertheless, the patients were not randomized for one or another operative procedure, resulting in 3 different procedures and may have led to selection bias, where patients with multilevel DDD may have been advised for fusion more often.
Finally, while our patients’ cohort was followed up for a minimum of 24 months, and some studies 42 have shown that significant changes in clinical outcome and also further surgical revisions still occur more than 2 years after surgery.
Conclusion
TDR may be an alternative to anterior and posterior lumbar fusion in terms of short follow-up analysis for clinical data and cost analysis. General advice cannot be given due to missing data for long-term costs in terms of surgical treatment of adjacent level or further fusion techniques.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.