
Abstract
Study Design:
The authors performed a retrospective controlled study of patients diagnosed with lumbar degenerative disc disease who received surgical intervention (either total disc replacement [TDR]/Activ-L or anterior lumbar interbody fusion [ALIF]) at a single tertiary-care hospital from 2007–2010.
Objectives:
To investigate the clinical outcomes after TDR in comparison with ALIF for surgical treatment of lumbar degenerative disc disease (DDD).
Methods:
Analyzed data included intra-operative blood loss, time to return to work, and clinical outcomes as evaluated through the Oswestry Disability Index (ODI) and the Visual Analog Scale (VAS) pain questionnaires pre-operatively and at 6 weeks, 3 months, 6 months, and 1 year postoperative follow-up.
Results:
At the univariate analysis, patients submitted to TDR presented significantly lower VAS pain scores than patients who received ALIF starting at 6 weeks (P < .001) and continuing through one year postoperatively (P = .007). Patients submitted to TDR also presented significantly lower ODI disability scores at all time points. There was a significant difference in the number of days to return to work, with TDR patients returning to work on average 65 days sooner than ALIF patients (P = .011). There was no significant difference in the total blood loss between both groups.
Conclusions:
The results of this retrospective controlled study suggest that, in comparison with patients submitted to ALIF, patients submitted to TDR present quicker return to work, less back pain, and lower disability scores at 1 year follow-up.
Keywords
Introduction
Chronic lower back pain (CLBP) is a very prevalent symptom which has been shown to constitute one of the most debilitating and economically costly medical problems worldwide. 1,2 It has been estimated that more than 26 million Americans aged between 20 and 64 years experience CLBP at least once during the year and that 30 to 50 billion dollars are spent annually by the health care system for the treatment of CLBP. 3
The etiology of CLBP is essentially multifactorial, and it is often challenging to determine with precision in each individual case the most important component. Degenerative disc disease (DDD) has been implicated in the etiology of CLBP through many pathophysiologic pathways that attempt to correlate the histological fragmentation and fibrosis observed in degenerated intervertebral discs as well as the abnormal signal and loss of disc height observed in magnetic resonance imaging with some type of impairment of the normal biomechanics at the affected level that may generate pain. 4 –7 Nevertheless, the exact details as well as the true causal relationships among the several factors that have been implicated to be involved in the pathophysiology of DDD are still controversial. 5 In fact, recent studies have demonstrated high rates of DDD in asymptomatic patients. 8 Furthermore, the incidence of DDD in asymptomatic individuals has been shown to increase with age (with signs of DDD seen in 34% of asymptomatic individuals between 20 and 39 years of age, in 59% of individuals between 40 and 59 years of age, and in 93% of individuals between 60 and 80 years of age), suggesting that the radiological criteria that have been used to diagnose DDD may actually represent the natural history of the magnetic resonance imaging signal changes with age, thus posing several important questions, such as the real value of abnormal radiological findings in elderly patients with CLBP.
Management of CLBP in the presence of radiological signs of DDD is, therefore, a long and complex medical process in which conservative measures are still the mainstay of treatment. First-line therapy often consists of nonsteroidal anti-inflammatories in conjunction with muscle relaxants, thermal analgesia, ultrasound, transcutaneous electrical nerve stimulation (TENS), and spinal manipulation. 9 Physical therapy is often recommended to maintain or improve paravertebral muscle strength and restore range of motion, and structured evidence-based validated protocols have already been proposed with such goals. 10 Although the majority of patients with CLBP and DDD find significant relief with noninvasive therapies, some of them ultimately fail such nonoperative measures. This small subgroup, which present persistent and refractory axial lower back pain even after 6 months to 1 year of conservative treatment, may be considered candidates for surgical interventions. 11 Although classical studies in the surgical literature suggested that lumbar fusion in a well-informed and selected group of patients with severe CLBP and DDD may decrease pain disability more efficiently than nonsurgical treatment, 6 some more conservative groups have not only increased the time length of conservative treatment (for up to 2 years) but also suggested that intensive standardized programs including cognitive intervention and psychological support should be offered before considering the surgical intervention. 12,13
Despite the fact that several surgical techniques have been proposed for the treatment of CLBP in the presence of DDD (such as intradiscal electrothermal therapy and nucleoplasty), 14 the current gold-standard surgical intervention is still spinal fusion. 5,15 Multiple techniques are currently employed by surgeons for such goals, most of them relying on instrumented posterolateral fusion with pedicle screws either in isolation or with some form of interbody fusion, which may be performed with the following approaches: anterior (anterior lumbar interbody fusion [ALIF]), posterolateral (posterior lumbar interbody fusion [PLIF]), transforaminal (transforaminal lumbar interbody fusion [TLIF]), and, more recently, extreme-lateral (extreme-lateral interbody fusion [XLIF]).
Although fusion has been considered the traditional procedure for surgical treatment of DDD associated with CLBP, there are serious drawbacks to such techniques, including a nonnegligible incidence of postoperative complications (such as infection and hematomas), adjacent level disease, hardware failure, as well as a high incidence of patients with chronic, debilitating and persistent postoperative back pain, which even lead to the formulation of a specific term in order to describe such condition—the so-called failed-back syndrome. In such a scenario, it has been estimated that the overall clinical success (as defined by the US Food and Drug Administration) of lumbar fusion for treatment of CLBP in the setting of DDD is achieved in only 51% of patients at the 5-year follow-up. 16
Although for a long-time total joint replacement has been considered an effective and validated therapeutic modality for treatment of chronic pain associated with anatomical degeneration of hips, knees, and shoulders, 5 the development of successful strategies for spinal joint replacement has faced several challenges including the development of biomechanically sound and long-term durable prosthesis as well as the marked anatomical changes associated with spinal degeneration.
Previous studies have demonstrated that total disc replacement (TDR) seems highly effective in relieving pain, limiting disability, and decreasing time off work in the setting of DDD of the cervical spine. 17 Nevertheless, the data regarding the clinical outcomes of TDR in the lumbar spine is still controversial because most retrospective cohort series lack a control group 18 –27 and all prospective randomized trials up to now focused on a noninferiority comparison between TDR and the standard therapy (fusion). 3,28,29
The current study was designed in order to provide further scientific evidence for the hypothesis of superiority of TDR in relation to the anatomically similar surgical intervention involving fusion (ALIF) in terms of improving clinical outcomes.
Methods
The authors performed a retrospective controlled study of patients with DDD who received surgical intervention, either fusion (ALIF) or TDR, at a single tertiary care hospital (Illinois Neurological Institute at the OSF-Saint Francis Medical Center from 2007 to 2010). The study was approved by the local institutional review board.
TDR patients meeting the inclusion and exclusion criteria (Table 1) were recruited during routine clinic visits and consented for participation in the study prior to surgery as part of a larger prospective multicenter trial for the National Institutes of Health approval of an investigational device (Activ-L/Aesculap). 30 The number of surgeries performed in the trial context during the analyzed time frame determined the study size. Subjects for the control group were selected from the main neurosurgeon’s practice using the same inclusion and exclusion criteria during the same period.
Inclusion and Exclusion Criteria for the Experimental (TDR) and Control (ALIF) Groups.
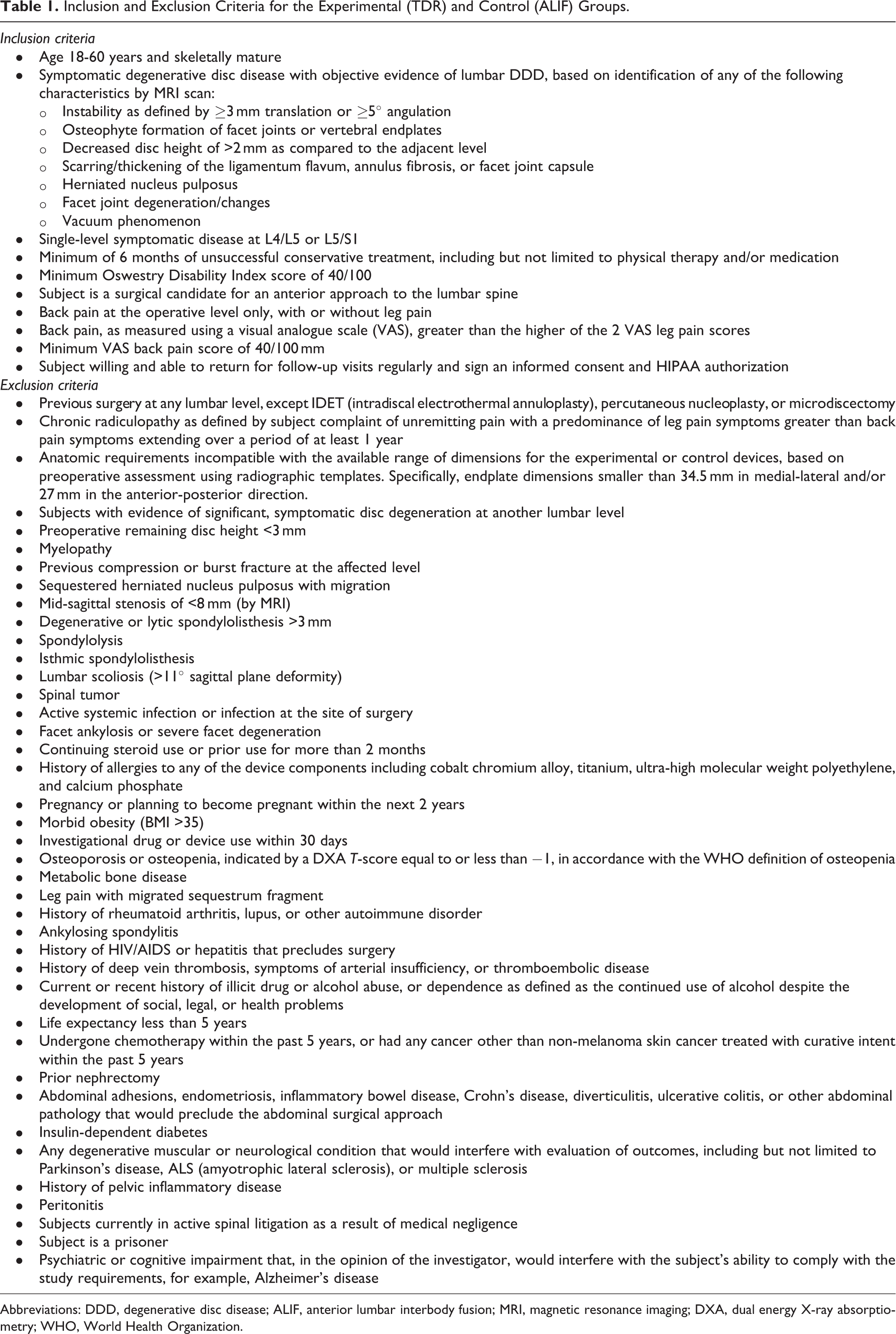
Abbreviations: DDD, degenerative disc disease; ALIF, anterior lumbar interbody fusion; MRI, magnetic resonance imaging; DXA, dual energy X-ray absorptiometry; WHO, World Health Organization.
Surgical bias was controlled through the use of the same general access surgeon and the same neurosurgeon for all procedures in both groups. Such standardization attempted to eliminate any possible technical differences related to surgical technique or personal expertise that might have affected the measured outcomes. Furthermore, all procedures were performed at one institution at the same operating room and with the same anesthesiology staff.
Patients’ data was collected in a prospective fashion at outpatient clinic visits using the Oswestry Disability Index (ODI) and the Visual Analogue Scale (VAS) for back pain questionnaires applied preoperatively and at 4 standard subsequent follow-up time points: 6 weeks, 3 months, 6 months, and 1 year postoperatively.
Basically the VAS is a 10-cm linear scale in which patients indicate their current level of pain by a hash mark, which is measured and converted to a numerical score out of 100. The ODI consists of 10 sections that address different aspects of disability for patients with chronic back pain: pain intensity, personal care, lifting, walking, sitting, standing, sleeping, sex life, social life, and traveling. The patient’s score for each section (ranging from 0 to 5) are sequentially added and converted to a total score scale of 100.
Patient demographics, operative blood loss, employment status, and return to work data were also obtained from patients’ charts and physician’s notes. Clinical outcomes were evaluated through the total ODI score and the total VAS score for back pain. As the present study was designed to evaluate the effects of TDR and ALIF in terms of DDD and CLBP, only VAS axial back pain data was taken into account while VAS values for leg pain were disregarded.
The data was entered into an Excel spreadsheet with the analysis having being completed using PASW Statistics V17.0 (SPSS Inc, an IBM Company, Chicago, IL). Both the ODI and VAS scores were tested for normality of the analyzed variables according to the appropriate statistical tools. A significance level of P ≤ .05 was used.
To test the differences between the 2 groups at baseline, the χ2 test was used for nominal variables, the Mann-Whitney U test for ordinal variables, and t tests for interval variables. A mixed effect regression model was used in order to test differences in the VAS and ODI scores for the experimental (TDR) and control (ALIF) groups at baseline, 6 weeks, 3 months, 6 months, and 1 year postoperatively. To test differences in time to return to work, a univariate general linear model was employed.
Results
Eighty patients were included in the final data analysis for this study. Thirty patients met the inclusion criteria for TDR and were consented for study participation prior to surgery (Figure 1). No patients were lost during the study period. Data from all subjects at all time intervals was available for analysis.
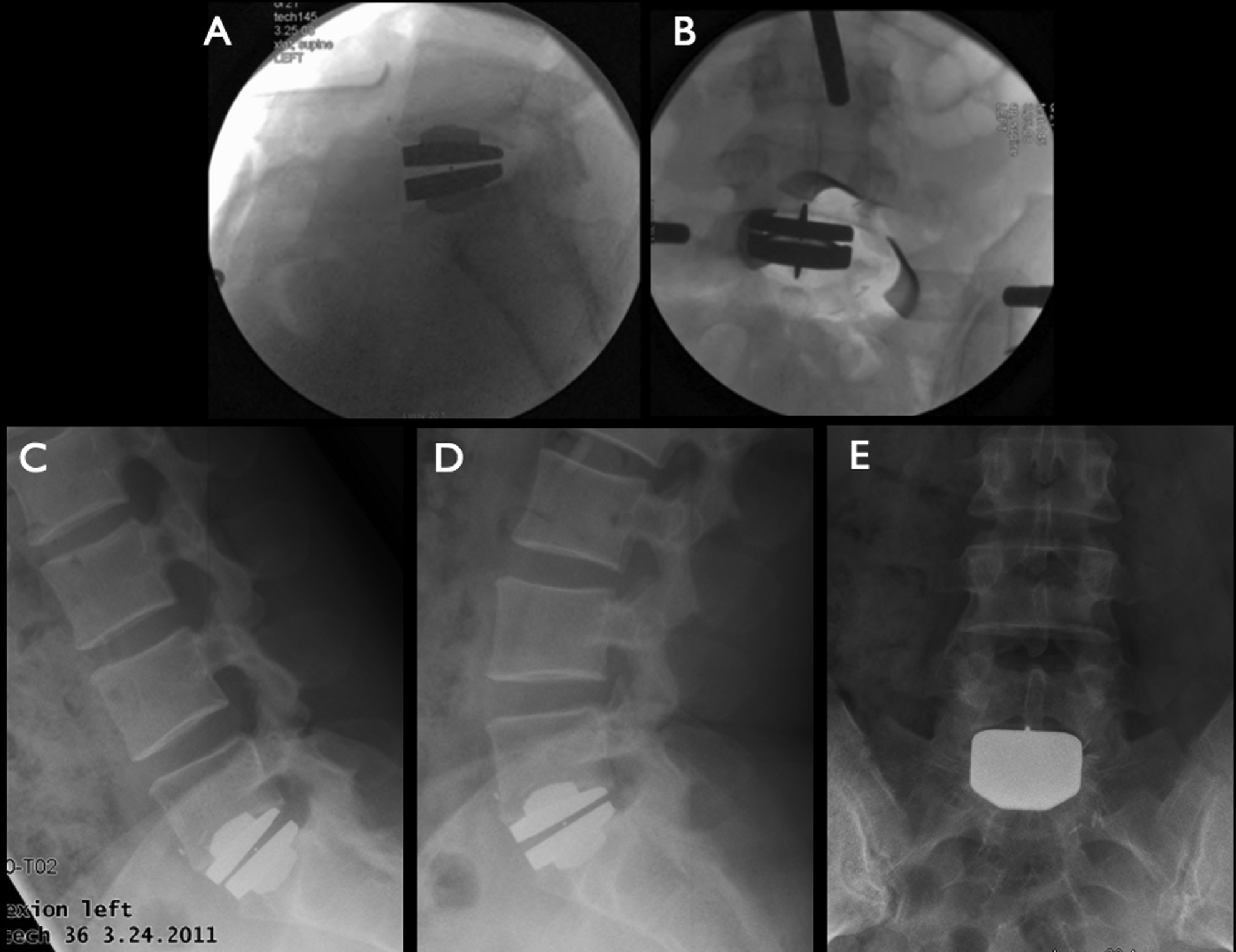
Intraoperative X-rays (A, lateral; B, AP) demonstrating TDR with Activ-L at the L5/S1 level. Note the preserved motion at the operated level as demonstrated by dynamic postoperative X-rays at 6-month follow-up (C, flexion; D, extension). E = AP radiograph.
Control cases (N = 67) were selected based on operative billing codes from a single hospital database from patients from the main neurosurgeon for the same period (2007-2010). Subjects were eliminated based on age criteria (18-60 years), and with respect to previous spinal surgery or surgery involving more than one spinal level, with a final control group of 50 subjects. Two subjects with missing available objective data were also eliminated. One subject with fusion at spinal level L5-L6 (transitional vertebrae) was considered as part of the L5-S1 group for statistical analysis.
Baseline Characteristics
Regarding the baseline epidemiological characteristics there was no significant gender difference between the 2 groups (Table 2). There was a significant difference in the mean age between the experimental and control groups (P = .012), with patients who received TDR presenting a lower mean age (40.47 ± 8.12 years) than patients who received spinal fusion (45.30 ± 7.97 years). There was also a significant difference in the spinal levels with the ALIF group presenting a higher proportion of patients with DDD at L5-S1 (88% of the cases) than the control group (63.3%), P = .020.
Baseline Demographic Characteristics of Case and Control groups as Well as VAS/Back Pain and ODI Scores.
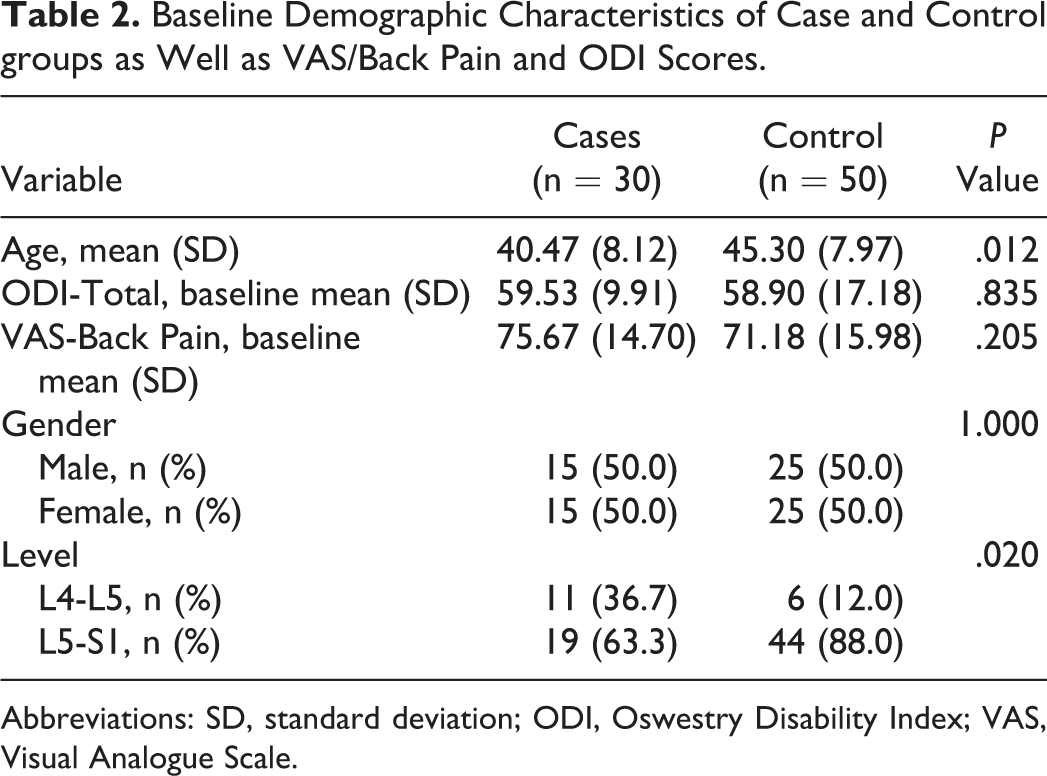
Abbreviations: SD, standard deviation; ODI, Oswestry Disability Index; VAS, Visual Analogue Scale.
There were no significant differences between the 2 groups with respect to preoperative back pain (VAS) and disability (ODI) scores at baseline (Table 2). The mean VAS score was 75.67 (±14.70) for the TDR group and 71.18 (±71.18) for the ALIF group (P = .205), while the mean ODI score was 58.90 (±17.18) for the TDR group and 59.93 (±9.91) for the ALIF group (P = .835).
Follow-up
Back Pain
In the univariate analysis there were significant differences in back pain scores (VAS) between the experimental (TDR) and control (ALIF) groups at all time intervals except at baseline (Table 3), with patients in the TDR group presenting significantly less back pain than patients who received spinal fusion starting at 6 weeks and continuing through 1 year postoperatively.
Outcome Measures for Cases and Controlsa.
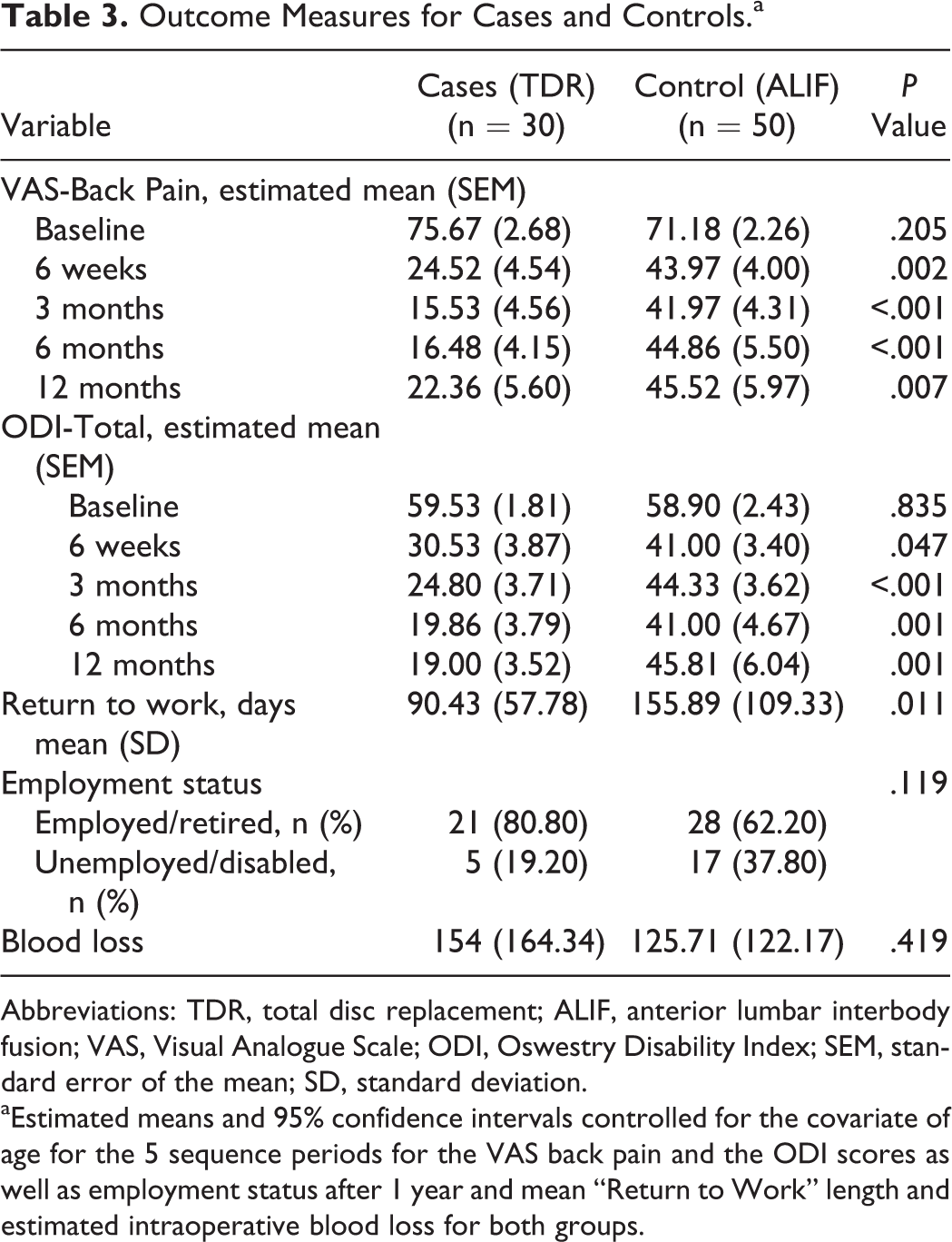
Abbreviations: TDR, total disc replacement; ALIF, anterior lumbar interbody fusion; VAS, Visual Analogue Scale; ODI, Oswestry Disability Index; SEM, standard error of the mean; SD, standard deviation.
aEstimated means and 95% confidence intervals controlled for the covariate of age for the 5 sequence periods for the VAS back pain and the ODI scores as well as employment status after 1 year and mean “Return to Work” length and estimated intraoperative blood loss for both groups.
Disability
According to the univariate analysis, there were significant differences in disability scores (ODI) between the experimental and control groups at all time intervals except at baseline (Table 3). Disability scores were significantly lower in the TDR group at all time points when compared with patients in the ALIF group, demonstrating that patients submitted to TDR achieved higher levels of daily function with less disability starting at 6 weeks and continuing through 1 year postoperatively.
Employment and Return to Work
Although the observed difference in employment rates between the TDR group (80.80%) and the ALIF group (62.2%) at 1-year follow-up was not statistically significant (P = .119), there was a significant difference in the number of days to return to work between the TDR group (90.43 ± 57.78 days) and the ALIF group (155.89 ± 109.33), P = .011. The fact that TDR patients returned to work on average 65 days sooner than patients who received ALIF suggests that arthroplasty, which, at least theoretically, restores the normal biomechanical physiology, may be associated with greater clinical improvement and quicker return to baseline professional activities.
Blood Loss
There was no statistically significant difference in the total amount of intraoperative blood loss between the TDR group (154 ± 164.34 mL) and the ALIF group (125.71 ± 122.17 mL), P = .419.
Disability and Back Pain at 1 Year
Linear mixed models were performed to test for differences in the data between both groups over the 5 time measures, with the outcome (VAS-back pain or ODI) at baseline, 6 weeks, 3 months, 6 months, and 1 year. The predictor variable of “control/experimental” and sequence (5 time measures) were included as factors and age as a covariate. The affected spinal level (either L4-L5 or L5-S1) was also included in the initial equation but was eliminated as it has been shown not to be significant. The 2-way and 3-way interactions were entered individually and only the interaction of case/experimental by age was significant and retained in the equation. Table 4 gives the level of significance for each of these variables.
Linear Mixed Effect Models for Disability and VAS-Back Scoresa.
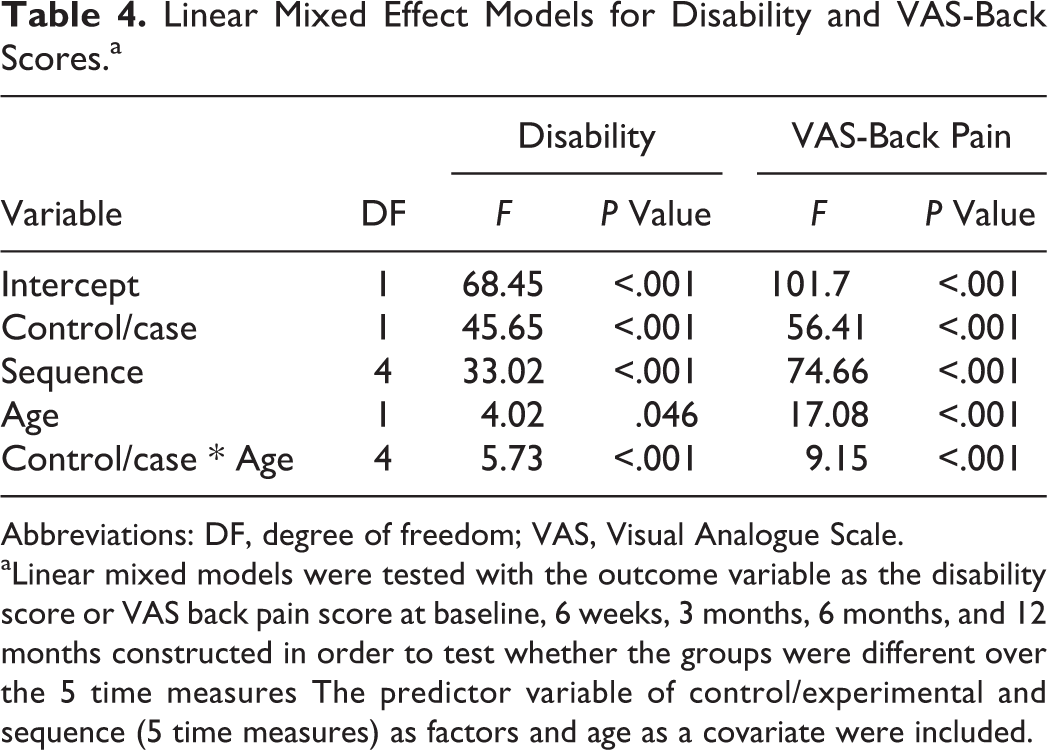
Abbreviations: DF, degree of freedom; VAS, Visual Analogue Scale.
aLinear mixed models were tested with the outcome variable as the disability score or VAS back pain score at baseline, 6 weeks, 3 months, 6 months, and 12 months constructed in order to test whether the groups were different over the 5 time measures The predictor variable of control/experimental and sequence (5 time measures) as factors and age as a covariate were included.
The grand estimated mean of the variables under study (ODI and VAS) controlled for age of the patients at the control group was higher than that of the experimental group for both disability (ODI/ALIF: 46.88 ± 1.70 vs ODI/TDR: 29.97 ± 1.76) as well as for back pain (VAS/ALIF: 50.97 ± 2.00 vs VAS/TDR: 29.27 ± 2.02 years). Table 4 illustrates the estimated means and 95% confidence intervals controlled for the covariate of age for the 5 sequence periods for both ODI and VAS back pain. While both ODI and VAS back pain scores were similar at baseline, the postoperative values of both measures declined more rapidly in the TDR group than in the ALIF group.
Discussion
Initial cohort studies examining the potential benefits of TDR have suggested improvement in multiple clinical outcome measures. 18 –27 These studies suggest the clinical benefits of TDR in relation to the natural history of DDD and supported its potential role as an effective alternative to spinal fusion. Nevertheless, the lack of control groups in most of these studies promptly lead the scientific community to a search for further evidence from comparative studies of TDR in relation to lumbar fusion. Our retrospective controlled study demonstrated superiority of TDR compared with ALIF in patients with single-level DDD in terms of pain and disability reduction.
The results of previous controlled studies on clinical outcomes of TDR versus fusion for treatment of CLBP in the setting of DDD have been controversial. 28,29,31 –42 For example, the Charité trial, which was designed as a noninferiority multicenter, prospective, randomized investigational device exemption (IDE) study, randomized 375 patients to either TDR with the Charité III disc or ALIF with BAK cage with a follow-up of 2 and 5 years. 28 The 5-year report, which is consistent with the 2-year initial data, found no statistical differences in clinical outcomes between both groups as measured by ODI questionnaire as well as VAS, SF-36, and patient satisfaction surveys, demonstrating that TDR with the Charité device provides at least as good outcomes as fusion with ALIF. Moreover, this study demonstrated that TDR patients reached a statistically greater rate of part-time and full-time employment and a statistically lower rate of long-term disability when compared with fusion patients.
Another prospective, randomized, multicenter, clinical trial compared the safety and effectiveness of TDR with the ProDisc-L (Synthes Spine/West Chester, PA) to circumferential spinal fusion at one vertebral level between L3 and S1. 39 This study was able to demonstrate that TDR patients presented significantly higher SF-36 Health Survey scores than the control group at 6 weeks and 3 months follow-up time points (P = .018 and P = .0036, respectively). In this study VAS pain score showed statistically significant improvement from preoperative levels regardless of the treatment (P < .0001). Nevertheless the VAS patient satisfaction score showed a statistically significant difference favoring TDR over the fusion group at 6 weeks and 3 months follow-up time points (P = .015). Nevertheless, according to a recent meta-analysis on the issue, although the Prodisc artificial disc trial (which was designed as a noninferiority study) found TDR to be more effective than circumferential fusion on the composite outcome of “clinical success,” with a statistically significant difference (53.4% vs 40.8%), the risk of bias of this study was considered high. Therefore, it provides very low quality evidence for the superiority of TDR over anterior lumbar circumferential fusion. 40
Other studies focusing on other quality-of-life outcomes related to CLBP demonstrated a significant improvement in sexual activities after both TDR and lumbar fusion which was positively correlated to a reduction in LBP. 41 Nevertheless the results of this study suggested that sexual function, evaluated as the achievement of orgasm, deteriorated in men in the fusion group postoperatively, despite the reduction in CLBP after 2 years, and that TDR performed through an anterior retroperitoneal approach was associated with less sexual dysfunction compared with instrumented lumbar fusion performed either as an PLF or as a PLIF. According to such a study, 26% of all men in the fusion group, compared with 3% in the TDR group, reported postoperative deterioration in the ability to achieve orgasm. 41
Interestingly, although the TDR technique has been criticized by some due to its higher costs in comparison with standard fusion procedures, the results of a recent retrospective study that compared surgical and hospitalization charges of TDR and circumferential lumbar fusion demonstrated that this may not actually be the case. 42 In this analysis the authors were able to show that patients undergoing TDR not only spent significantly less time in the operating room (OR) (mean OR minutes averaged 344 minutes for the fusion group and 185 minutes for the TDR; P < .05) and had less intraoperative blood loss than controls (averaged 794 mL in the fusion group vs 412 mL in the TDR group; P = .0058), but also that the total charges for one-level surgery (including implant costs, OR charge, and surgeon and anesthesiologist fees) were significantly lower for TDR when compared with circumferential fusions (mean charge for the TDR of $35 592 vs $46 280 for the fusion group; P = .0018).
In relation to our series, the following considerations should be taken into account during the interpretation of the obtained results. Although the difference in the mean age between the TDR group (40.47 ± 8.12 years) and ALIF group (45.30 ± 7.97 years) seems small and would not be expected to significantly influence in the obtained results, the unmatched characteristics of the experimental and control groups may raise the possibility of other unknown selection bias. Also, the differences in levels operated are inherent drawbacks to the study design.
Furthermore, this was a retrospective study. Therefore, further prospective randomized trials are warranted to confirm the observed results. Furthermore, as the study focused on the clinical outcomes (as measured by both pain and disability scores) as well as on the employment status of the patients, and did not evaluate further imaging follow-up, there is no data available for comparison of adjacent segment degeneration and its possible relation to the observed worst outcome in the surgical group, an important factor which may favor the use of TDR over fusion.
Nevertheless, despite the aforementioned limitations, the present study constitutes one of the few controlled cohorts that has been able to demonstrate a clear superiority of TDR when compared to fusion in terms of both clinical outcomes (both in pain and disability scores) as well as time to return to professional activities. In fact, in a recent literature review on the issue, 40 all 16 identified prospective cohort studies that assessed pain relief, improvement in functional status, and patient satisfaction after TDR lacked a control group. 9 –27,30 Moreover, because the only 3 randomized controlled multicenter trials that assessed the effectiveness of TDR were designed as Food and Drug Administration investigational device exemption studies, they only attempted to demonstrate noninferiority between TDR and fusion. 18,28,39 Because of the contradictory results of such studies the authors of a recent systematic review on the issue concluded that, up to now, there is very low quality evidence even for proving noninferiority of TDR in comparison to standard fusion procedures in terms of clinical outcome measures at the 5-year follow-up. 40
Conclusions
In this retrospective controlled study, TDR patients demonstrated significantly less back pain (as measured by VAS) starting at 6 weeks and continuing through 1 year postoperatively as well as lower disability scores (as measured by ODI) at all time intervals when compared to patients who received spinal fusion (ALIF). Although there were no significant statistical differences between either intraoperative blood loss or employment rates at 1-year follow-up, the time to return to work after TDR was significantly lower than after ALIF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.