
Abstract
The Institute of Medicine defines clinical practice guidelines as “statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options.” Guidelines help clinicians implement best evidence into practice and encourage informed shared decision making with patients. Guidelines are intended to enhance the quality of patient care by discouraging ineffective and potentially harmful interventions and standardizing practice. Standards for the development and appraisal of guidelines, such as those proposed by the Institute of Medicine and other organizations, help assure guideline quality and credibility. Primary standards include establishing transparency, managing conflicts of interest, forming a multidisciplinary guideline development group, conducting methodologically sound systematic reviews, developing evidence-based recommendations, balancing risks and harms, and rating the strength of recommendations based on the confidence in the evidence. Furthermore, the guideline document must be appraised internally and externally and updated when new evidence arises. The Grading of Recommendation, Assessment, Development and Evaluation process helps appraise the existing body of evidence as well as provide an interactive framework for weighing the benefits and harms of treatment options and translating evidence to recommendations. This article summarizes the methodology used to develop clinical practice guidelines for the management of degenerative cervical myelopathy and acute spinal cord injury.
Keywords
Introduction
The Institute of Medicine (IOM) defines clinical practice guidelines as “statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options.” 1 Guidelines (1) are a way of implementing evidence into practice; (2) focus on improving quality of care; (3) reduce health care variations, improve diagnostic accuracy, promote effective therapies, and discourage ineffective and potentially harmful interventions; (4) represent the best judgement of a team of experienced clinicians and methodologists; (5) can potentially form the basis for measuring performance; and (6) can be implemented into practice if well designed. In contrast, guidelines are not intended to be the sole source for treatment decisions, supersede professional judgement, or be used for reimbursement policies, performance measures, legal precedents, comprehensive management, or as measures of certification or licensing. 2
Well-conducted clinical practice guidelines can substantially improve patient care as well as treatment outcomes by standardizing management strategies, and encouraging clinicians to make evidence-informed decisions. The methodology used for their development, however, must be rigorous. In the past 2 decades, substantial variation in the quality of clinical practice guidelines prompted the implementation of standards and more rigorous processes for guideline development. 3 –7 Such standards have helped improve the credibility of guidelines, are required for publication in the Agency for Healthcare Research and Quality’s National Guideline Clearinghouse, 8 and are increasingly used by policy makers to assess guideline quality.
There is substantial overlap between standards published by the IOM
1
and the Guidelines International Network
6
for the development and reporting of high-quality and trustworthy guidelines. Primary tenets include the following: Establish transparency by disclosing funding sources, achieving editorial independence, and following a protocol. Manage conflict of interests, including intellectual and financial conflicts. Create a multidisciplinary guideline development group (GDG) that includes a patient or patient advocate. Conduct methodologically sound systematic reviews that appraise the evidence and contain an appropriate balance between systematic review and guideline development teams. Create clear and actionable recommendations that explicitly link critically appraised and synthesized evidence to rationale of recommendations. Balance risks and harms. Rate the strength of recommendations based on confidence in the evidence and effect sizes. External review by a multidisciplinary group. Update as new evidence becomes available and as practice changes.
The Grading of Recommendation, Assessment, Development and Evaluation (GRADE) process is the most widely used method for assessing the overall quality (strength) of evidence for a specific outcome. The quality of evidence is described as high, moderate, low, or very low, based on the confidence that the observed effect sizes reflect the true effect. 9,10 The GRADE process for guideline development implements standards and provides a step-wise process that considers the following factors: the overall certainty and quality of evidence with respect to both benefits and harms; the value and importance of specific outcomes to various stakeholders, including patients, clinicians, and payers; the relative effect sizes of anticipated desirable and undesirable effects; resource use and cost-effectiveness; impact on health inequities; applicability; and feasibility. Recommendations are then formed based on these considerations as well as a formal balance of the desirable and undesirable consequences; the overall confidence in the evidence ultimately determines the strength of the recommendation. The GRADE framework also provides a process for articulating the evidence, judgements, and rationale (including the role of expert opinion) used to support the recommendation, and for identifying gaps in the evidence. 10 This article summarizes the methodology used to develop a clinical practice guideline for the management of degenerative cervical myelopathy (DCM) and acute spinal cord injury (SCI).
Methods for Guideline Development
Overview of the Process
There are critical knowledge gaps and variability in the care of patients with DCM and acute SCI. Following a series of meetings and webinars, the leadership group agreed there was a need to develop clinical practice guidelines to address key questions and resolve existing controversy surrounding the management of DCM and acute SCI. Multidisciplinary systematic review teams and a GDG were formed based on input from the leadership group and were required to disclose potential conflicts of interest. These disclosures were self-reported by members of the group; there may be some inherent conflicts of interest as all participants were experienced in the treatment of patients with DCM and/or acute SCI (see the appendix). There was some overlap between groups. Expert methodologists, with no important financial or intellectual conflicts of interest, conducted several systematic reviews to synthesize the evidence required to formulate recommendations. These methodologists were experienced in the application of GRADE and also directed the guideline development process. The Conference on Guideline Standardization (COGS) Checklist for Reporting Clinical Practice Guidelines, 7 with reference to IOM Standards, 1 was used to establish transparency, apply development standards, and refine the scope and intention of the guidelines. GRADE methods were used to assess the overall quality of evidence and document GDG discussions that guided the formation of the recommendations. 10 In-person meetings and webinars were used throughout the process. The guidelines were internally and externally appraised; results of these reviews, a summary of the final voting, as well as any substantial changes to the guidelines were documented.
Developer
DCM Guidelines
The guideline for the management of DCM was developed under the auspices of AOSpine North America (AOSNA) and the Cervical Spine Research Society (CSRS). AOSNA is an academic spine surgeon professional society and 1 of the 5 global regions of AOSpine International, a Clinical Division of the AO Foundation based in Davos, Switzerland. AOSpine is a “leading global academic community for innovative education and research in spine care, inspiring lifelong learning and improving patients’ lives.” Furthermore, it is “an international community of spine surgeons generating, distributing, and exchanging knowledge to advance science and the spine care profession through research, education, and community development. With this collaborative approach, AOSpine continues to advance spine care worldwide.” The CSRS is an organization of spine care professionals interested in clinical and research problems related to the cervical spine.
SCI Guidelines
The guideline for the management of acute SCI was sponsored by AOSpine North America, AOSpine International, and the Section on Neurotrauma and Critical Care of the American Association and Congress of Neurological Surgeons. The American Association of Neurological Surgeons (AANS) is a scientific and educational association that focuses on advancing the specialty of neurological surgery. There are approximately 10 500 members worldwide. They have a joint section with the Congress of Neurological Surgeons (CNS; total membership, 9100); together the AANS and CNS aim to define the use of spinal neurosurgical methods for the treatment of diseases of the spinal neural elements, the spine, and peripheral nerves. Their overall objectives include to advance spinal neurosurgery and related sciences, improve patient care, support meaningful basic and clinical research, and provide leadership in undergraduate and graduate education.
Composition of Guideline Development Group
DCM Guidelines
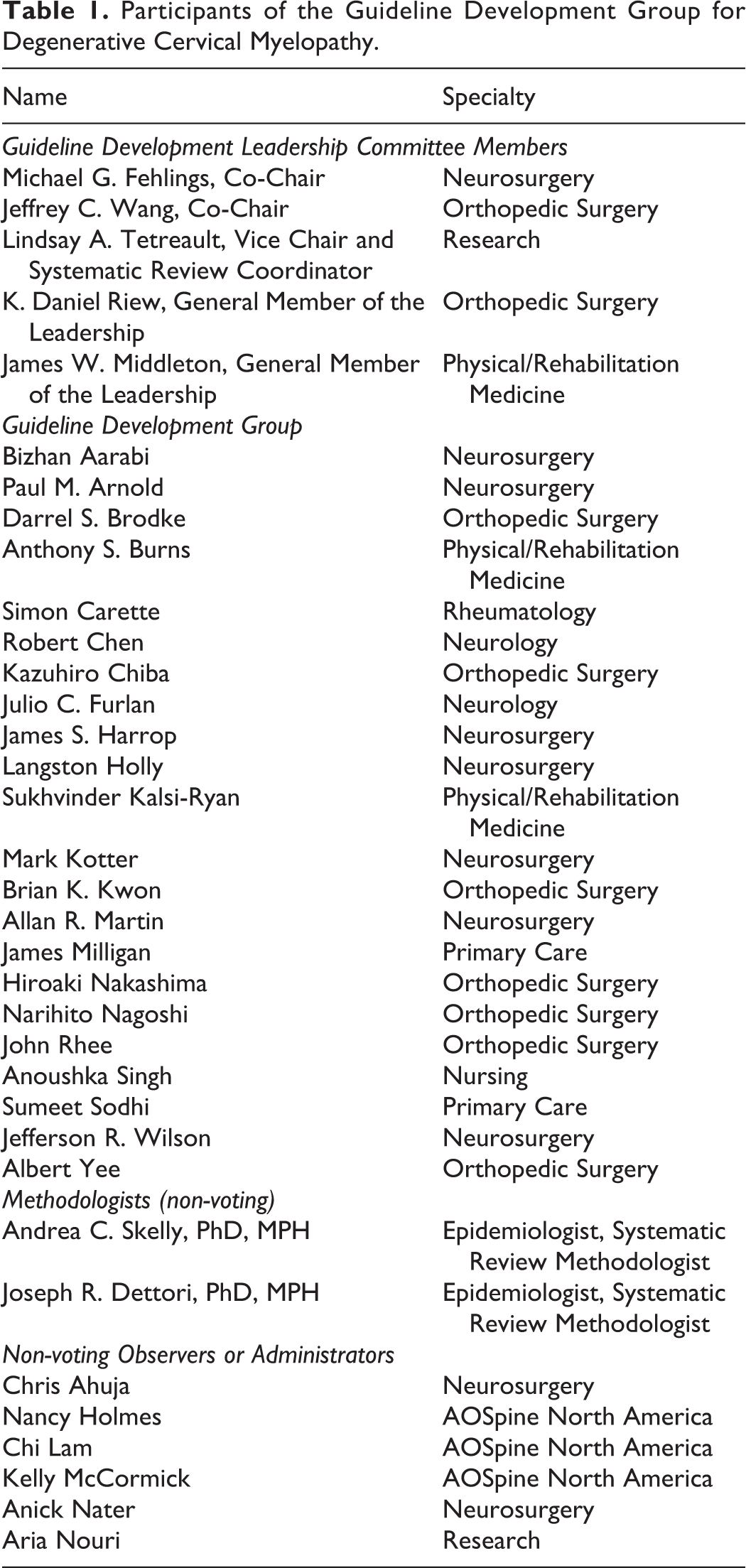
Our multidisciplinary GDG consisted of 17 spine surgeons (neurosurgeons, orthopedic surgeons), 2 neurologists, 1 rheumatologist, 3 physical medicine/rehabilitation specialists, 2 primary care physicians, 1 nurse, and 1 clinical researcher (Table 1). The GDG did not include a patient representative or a member from the public.
Participants of the Guideline Development Group for Degenerative Cervical Myelopathy.
SCI Guidelines
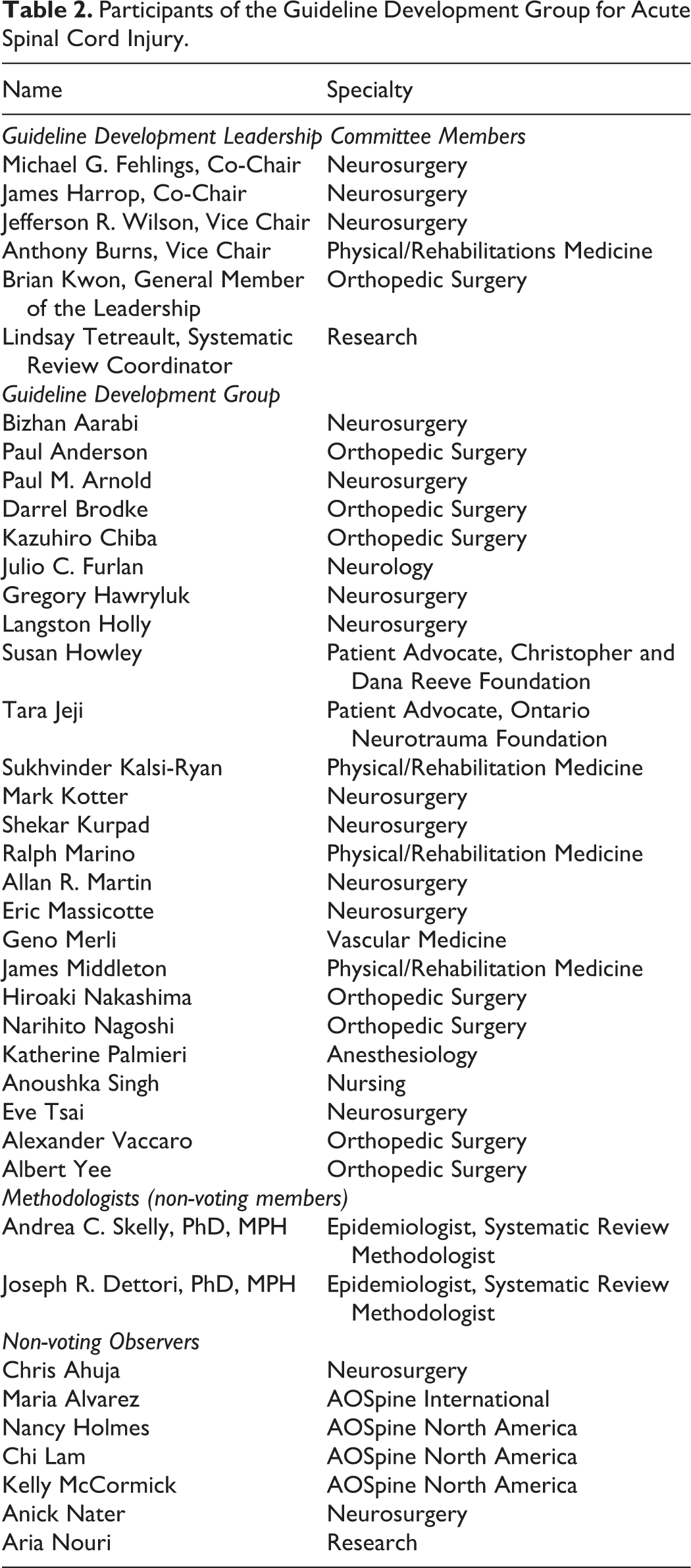
Our multidisciplinary GDG consisted of 20 spine surgeons (neurosurgeons, orthopedic surgeons), 1 neurologist, 4 physical medicine/rehabilitation specialists, 1 vascular medicine specialist, 1 anesthesiologist, 2 patient advocates, 1 nurse, and 1 clinical researcher (Table 2).
Participants of the Guideline Development Group for Acute Spinal Cord Injury.
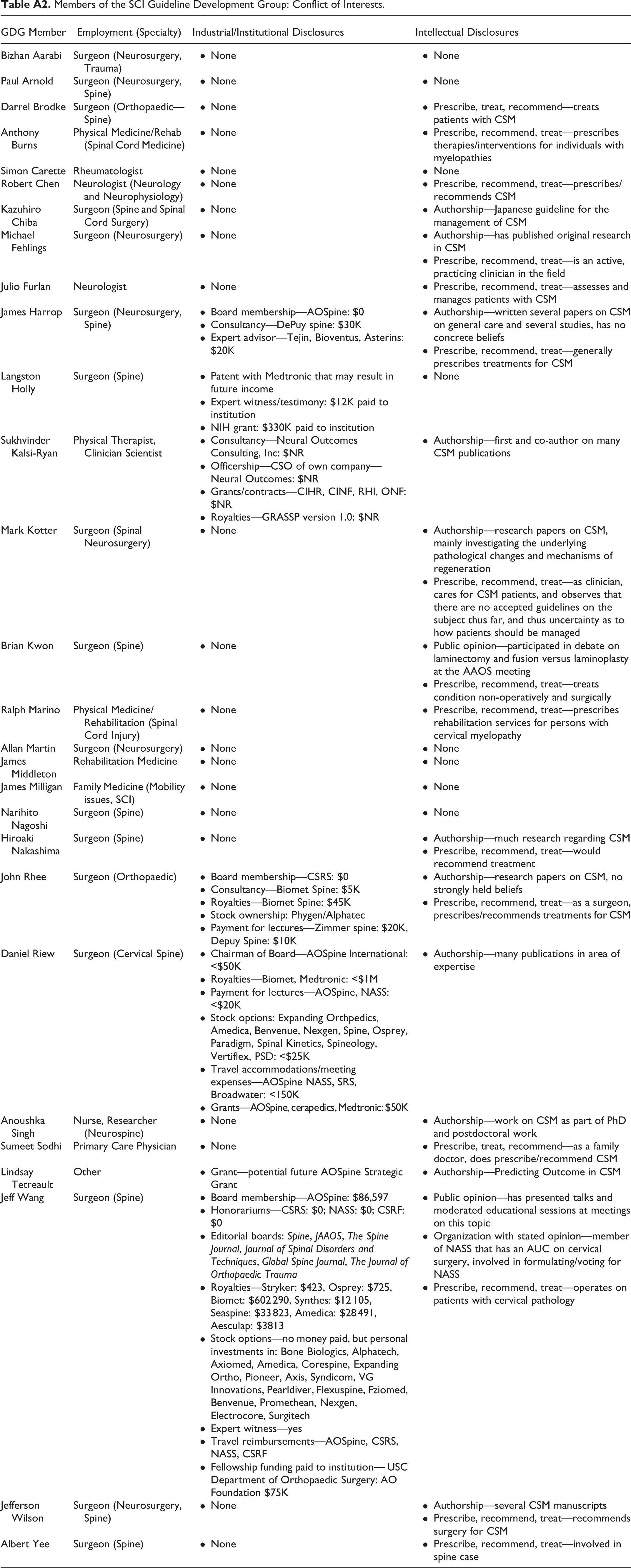
For both guidelines projects, the GDG had full editorial independence from the sponsors and included stakeholders who were not members of these organizations. Two methodologists from Spectrum Research, Inc, experienced in the accepted methodology for systematic reviews and guideline development, served as nonvoting participants and coordinated the process as a neutral party. Members of the GDG were required to complete a disclosure form detailing financial, personal, and intellectual conflicts of interests (summarized in the appendix) and verbally indicate relevant conflicts prior to each meeting. Before voting, individuals with relevant conflicts of interest were asked to recuse themselves from voting. Advice on conflict of interest management was provided by the methodologists at a number of stages throughout the development process. The leadership teams, however, were ultimately responsible for managing relevant conflicts.
Systematic Review of the Evidence
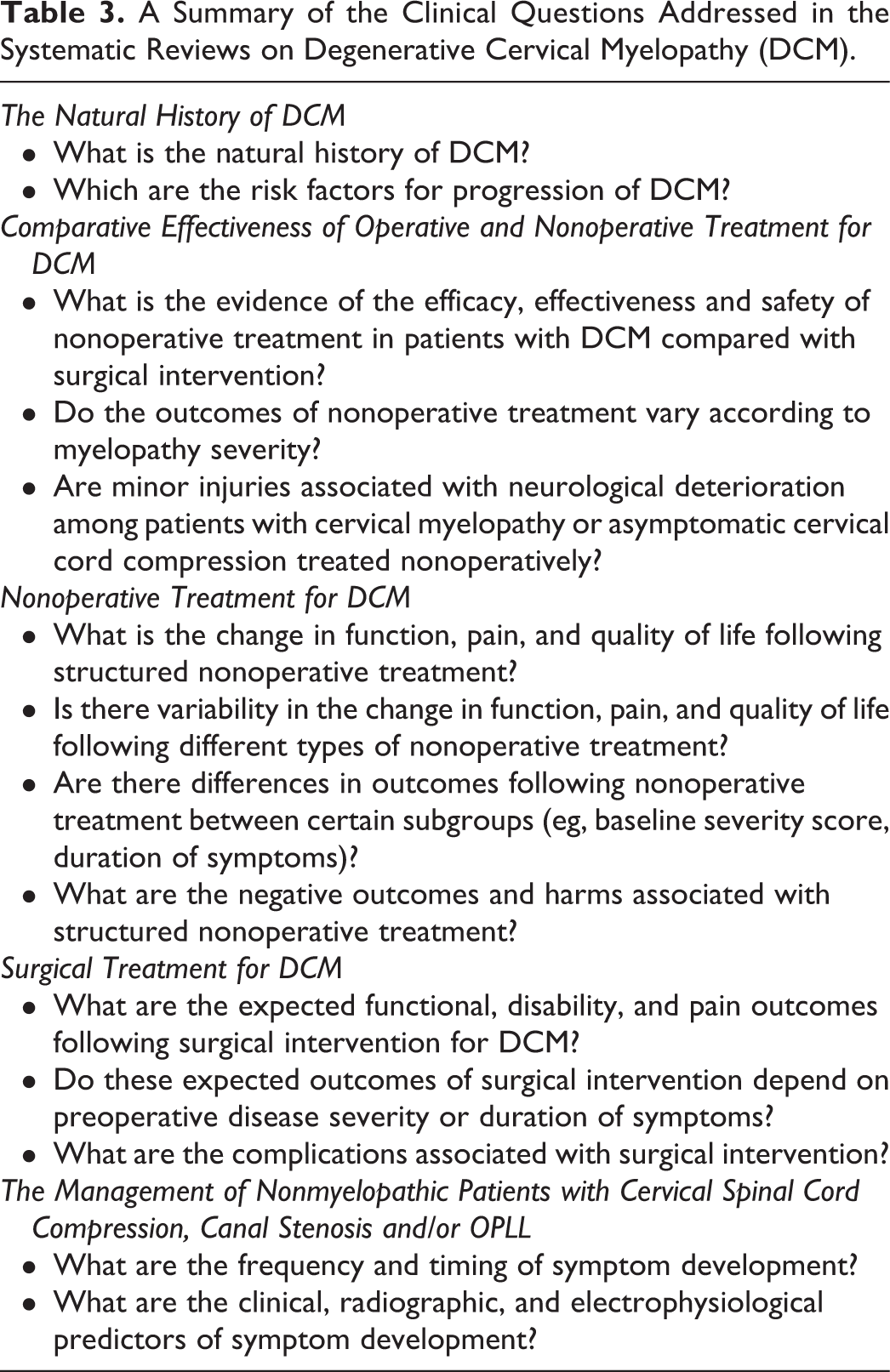
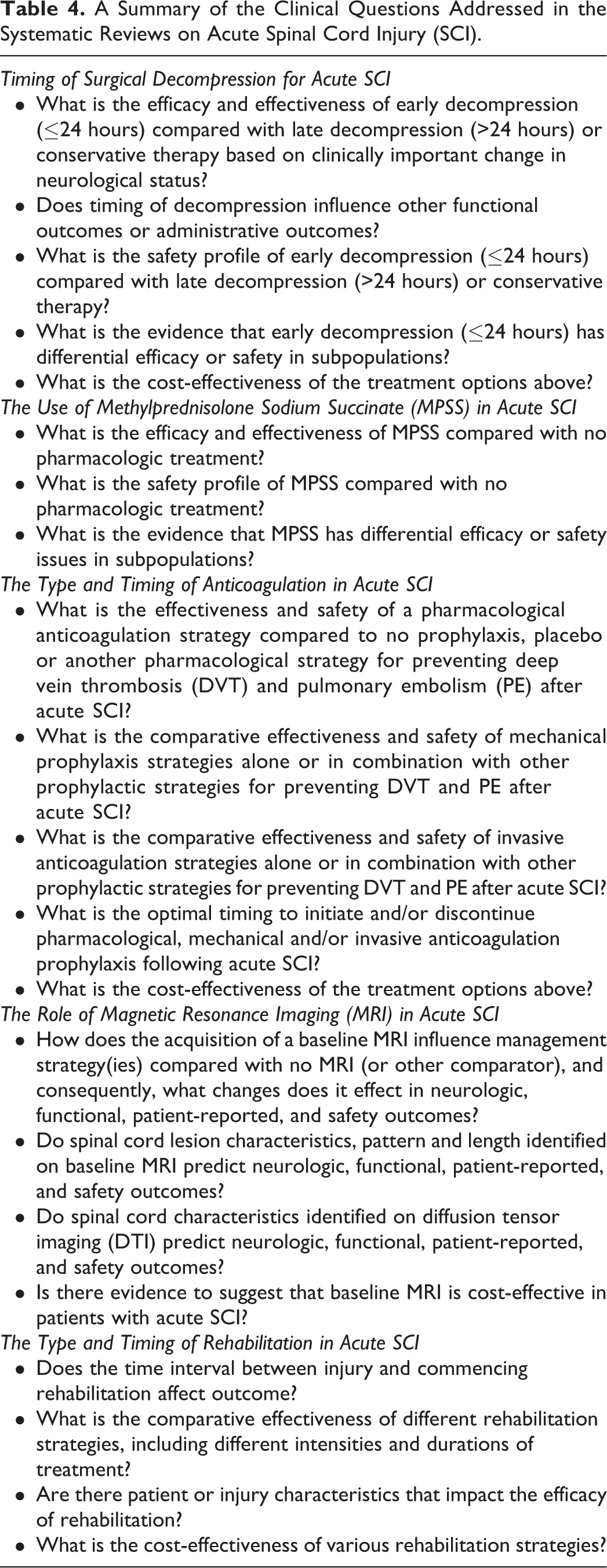
Systematic reviews were performed to summarize and synthesize the evidence required for the DCM and SCI guidelines. These reviews are published separately in this focus issue. The primary clinical questions addressed in these systematic reviews are summarized in Tables 3 and 4.
A Summary of the Clinical Questions Addressed in the Systematic Reviews on Degenerative Cervical Myelopathy (DCM).
A Summary of the Clinical Questions Addressed in the Systematic Reviews on Acute Spinal Cord Injury (SCI).
Spectrum Research, Inc, an independent evidence-based practice center, provided the methodological expertise needed to perform these systematic reviews. Reviews were conducted according to accepted methodological standards 8,11,12 (eg, Institute of Medicine, Agency for Healthcare Research and Quality, and Patient-Centered Outcomes Research Institute) and used similar methods as previously published systematic reviews. 13 Spectrum methodologists worked with clinical experts to ensure that the results were accurate and clinically appropriate. Specifically, the methodologists were responsible for conducting the systematic search, determining the inclusion/exclusion of retrieved articles, synthesizing results, and grading the evidence. Clinical authors were primarily responsible for developing the key questions and writing the introduction and discussion sections of these reviews.
Systematic review teams were selected by the leadership groups and included members from the GDG as well as clinicians that were not part of the GDG. Detailed methods are described in each individual review, including search strategies, search dates, inclusion/exclusion criteria (set a priori), data analysis/synthesis methods, risk of bias assessment, and evaluation of the overall quality (strength) of evidence. Electronic databases searched included PubMed, ClinicalTrials.gov, EMBASE, The Cochrane Library, and others deemed relevant by the review team. Spectrum methodologists prepared standardized evidence summaries and syntheses of the current evidence and key results; they presented these findings to the full GDG on several occasions to obtain input from clinical experts and to convey the overall quality of the evidence.
Previous systematic reviews on the topics were evaluated using the AMSTAR (A Measurement Tool to Assess Systematic Reviews) Checklist. 14 This system scores a systematic review out of 11 based on the following criteria: (1) was an a priori design provided; (2) was there duplicate study selection and data extraction; (3) was a comprehensive literature search performed; (4) was the status of publication used as an inclusion criteria; (5) was a list of studies (included and excluded) provided; (6) were the characteristics of the included studies provided; (7) was the scientific quality of the included studies assessed and documented; (8) was the scientific quality of the included studies appropriate for formulating conclusions; (9) were the methods used to combine the findings of studies appropriate; (10) was the likelihood of publication bias assessed; and (11) were conflicts of interest included.
Grading of Evidence
The overall quality of evidence was determined using methods outlined by the GRADE Working Group. 9,10 Spectrum methodologists, experienced in the application of GRADE, presented syntheses of the overall strength (quality) of evidence for specific outcomes. Details are provided in the individual systematic reviews. In general, the risk of bias, consistency, directness, precision, and publication bias were assessed across included studies for each critical or important outcome. The initial quality (strength) of the overall body of evidence was considered “High” for randomized controlled trials and “Low” for observational studies in most instances. The body of evidence may be downgraded 1 or 2 levels based on the following criteria: (1) risk of bias (study limitations), (2) inconsistency of results, (3) indirectness of evidence, (4) imprecision of the effect estimates (eg, wide confidence intervals), or (5) failure to provide an a priori statement of subgroup analyses. 10 If there are no downgrades, the body of evidence may be upgraded 1 or 2 levels based on the following criteria: (1) large magnitude of effect, (2) dose-response gradient, or (3) if all plausible biases would decrease the magnitude of an apparent effect. The final overall quality (strength) of evidence expresses the confidence that the effect estimate lies close to the true effect: high (high confidence that the estimate reflects the true effect), moderate (moderate confidence), low (low confidence), or very low (very little confidence; the true effect is likely to be substantially different from the estimated effect).
Recommendation and Guideline Development
A core group of individuals from the GDG constructed the key questions to be addressed by these guidelines.
DCM Guidelines
Should operative management be used to treat patients with severe DCM?
Should operative management be used to treat patients with moderate DCM?
Should nonoperative management be used to treat patients with mild DCM?
Should operative management be used to treat patients with mild DCM?
Should operative management be used to treat nonmyelopathic patients with imaging evidence of cord compression without signs or symptoms of radiculopathy?
Should operative management be used to treat nonmyelopathic patients with imaging evidence of cord compression and clinically/electrophysiologically diagnosed radiculopathy?
SCI Guidelines
Timing of surgery: Should we recommend early decompressive surgery (≤24 hours after injury) for adult patients with an incomplete pattern of neurological injury consistent with central cord syndrome, no radiological evidence of mechanical instability, and radiological evidence of spinal cord compression? Should we recommend early decompressive surgery (≤24 hours after injury) for adult patients with acute SCI regardless of neurological level of injury at hospital admission?
The use of methylprednisolone sodium succinate (MPSS): Should a 24-hour infusion of high-dose MPSS be administered to adult patients with acute SCI after 8 hours after injury? Should a 24-hour infusion of high-dose MPSS be administered to adult patients with acute SCI within 8 hours of injury? Should a 48-hour infusion of high-dose MPSS be administered to adult patients with acute SCI?
The type and timing of anticoagulation: Should prophylactic pharmacological strategies be employed to minimize the risk of thromboembolic events in the acute period after SCI? What prophylactic pharmacological strategy should be employed to minimize the risk of thromboembolic events in the acute period after traumatic SCI? Should prophylaxis be initiated within 72 hours (vs after 72 hours) of SCI? Should prophylactic pharmacologic strategies be used alone or in combination with mechanical approaches?
The role of magnetic resonance imaging (MRI): Should baseline MRI be performed to facilitate clinical management decisions in adult patients with acute SCI? Should baseline MRI be performed in adult patients with acute SCI to facilitate improved prognostication of neurologic and functional outcomes?
The type and timing of rehabilitation: Should early (vs late) rehabilitation be recommended for individuals with acute or subacute SCI? Should body weight supported treadmill training (vs conventional rehabilitation) be recommended for patients with acute or subacute SCI? Should functional electrical therapy (vs conventional rehabilitation) be recommended for patients with acute or subacute SCI? Should training unsupported sitting (vs control/standard in-patient therapy) be recommended for patients with acute or subacute SCI?
Input was obtained from other members of the GDG via a series of teleconferences and incorporated into a guideline development protocol, based on the COGS checklist. 3,7 This protocol included the general focus, purpose and rationale of the guideline, relevant definitions, the aspects of care covered by the guideline, users and settings, and implementation strategies. GDG members were required to review and provide written approval of the protocol.
Recommendations were developed using the process outlined by the GRADE Guideline Development Tool (GDT, Version 1) and the related “evidence-to-recommendation” framework. The GDT process consists of examining and weighing the evidence, formulating evidence-based recommendations, assessing the overall certainty of evidence and determining the strength of recommendation 15 –18 for each clinical question. The framework provides a systematic process to document the certainty of evidence, how stakeholders value the main outcomes, the size of anticipated desirable and undesirable effects (and the size of desirable effects relative to undesirable effects), resource use/cost-effectiveness, acceptability of options to key stakeholders, impact on health inequities, and feasibility of implementation. It also facilitates formal discussion on the balance of consequences and the type of recommendation. The framework was used by members of the GDG Leadership Team (Chairs, Vice Chair(s), and at least one general GDG member) to draft “strawman” recommendations (Table 5).
GRADE Guideline Development Evidence to Recommendation Framework: Questions and Response Options.
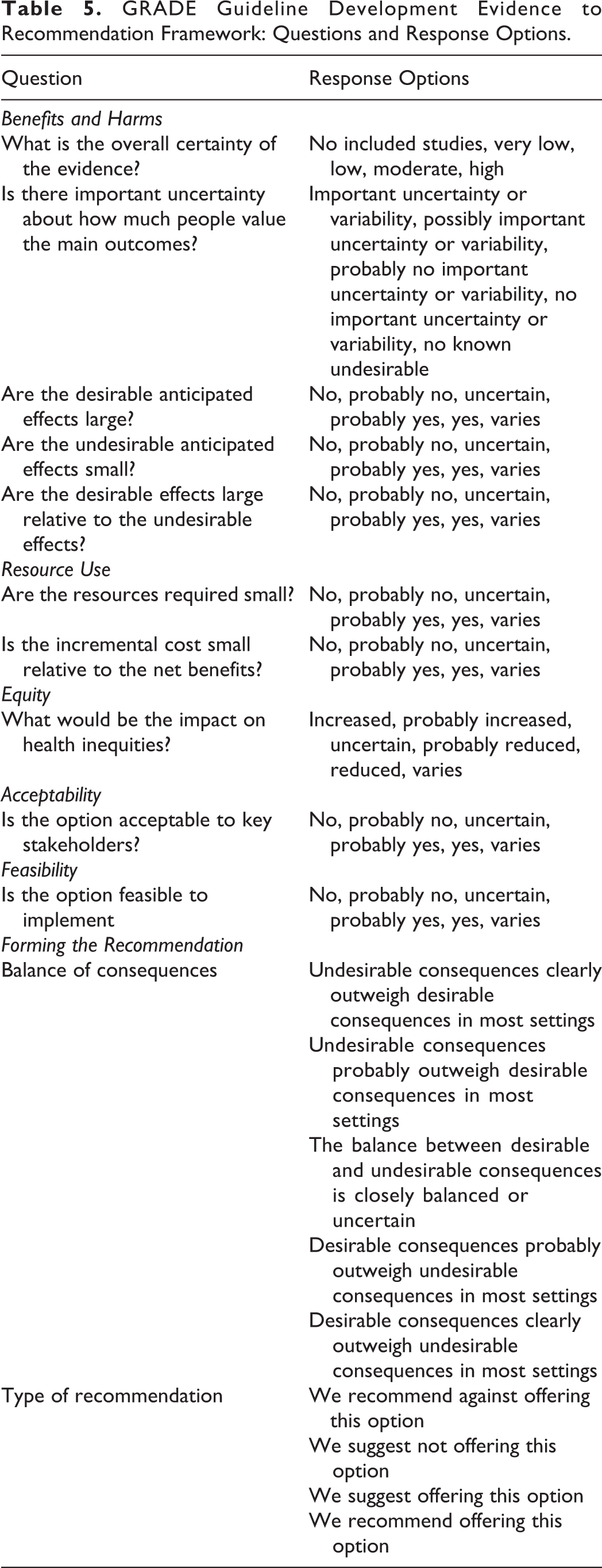
Some of the questions included in the GDT required discussion and interpretation. For the question on the overall certainty of the evidence, the quality of evidence across all critical outcomes, including desirable and undesirable effects, was considered as described in the GRADE Handbook. 10 With respect to the question on anticipated desirable effects, the importance of desirable effects and the number of people affected were considered. Prior to drafting the “strawman” recommendations, the GDG leadership group identified and ranked outcomes by their relative importance. Specific outcomes were classified as (1) critically important in determining treatment options and decision making, (2) important but not critical for decision making, and (3) of limited importance. Finally, for the question on health inequities, the GDG group agreed to assume that the recommendation would inform a change in policy.
Evidence from the systematic reviews was presented to the full GDG at in-person and follow-up webinar meetings by methodologists from Spectrum Research, Inc. The GDG discussed the available evidence, including important knowledge gaps, and presented relevant perspectives based on their clinical experiences. Perspectives from patients and advocates were also considered; in the absence of representation from these stakeholders, clinical experts were asked to provide the patient perspective based on their experience. The “strawman” recommendations facilitated initial discussion at in-person and webinar meetings involving the full GDG. The GDT (Version 1) was used in real-time to refine and finalize recommendations, document key discussion points, and summarize voting results. An audience response system was used for voting during in-person meetings to ensure anonymity; only methodologists were aware of the voting patterns based on discipline. In cases of voting discrepancies, the GDG discussed alternative perspectives and refined the wording of the recommendation if necessary.
Additional anonymous votes were completed electronically using SurveyMonkey; one vice chair and one methodologist were aware of these voting results. A modified Delphi process was used to reach consensus; however, for some elements and recommendations, there were varying perspectives and opinions, and consensus was not achieved. Votes were recorded and are presented in the “rationale for recommendation” sections when a consensus was not reached or when there was not a large majority. In the absence of strong evidence, the GDG was required to document their consideration of preferences and values and the role of clinical expertise in formulating the final recommendation.
Types and Interpretation of Recommendations
The 4 factors that influence the strength of a recommendation are the balance between desirable and undesirable outcomes, the confidence in the magnitude of the estimate of effect, the confidence in values and preferences, and resource use. 10 For example, the larger the difference between the desirable and undesirable consequences, the more likely a strong recommendation is warranted. In contrast, the smaller the net benefit of an option, and the lower the certainty for that benefit, the more likely a weak recommendation is warranted. Furthermore, the higher the quality of evidence, the more likely a strong recommendation is justified, and the greater the variability or uncertainty in values and preferences, the more likely a weak recommendation is warranted. Finally, in terms of resource use, the higher the cost of an intervention, the less likely a strong recommendation is justified.
The wording of the recommendation indicates whether it is “strong” or “weak;” the word “suggest” indicates a weaker recommendation, whereas the word “recommend” indicates a stronger statement. 10 For a strong recommendation, (1) most patients would want the recommended course of action and only a small proportion would not; (2) the recommendation would apply to most individuals; formal decision aids are not likely to be needed to help individuals make decisions consistent with their values and preferences; and (3) the recommendation can be adopted as a policy in most situations. In contrast, for a weak recommendation, (1) the majority of patients would want the recommended course of action, but many would not; (2) clinicians should support each patient in reaching a management decision consistent with his or her values and preferences; decision aids may support individuals in reaching such decisions; and (3) policymaking will require substantial debate and involvement of stakeholders.
In general, GRADE discourages guideline panels from making strong recommendations when their confidence in estimates of effect for critical outcomes is low or very low. GRADE has identified 5 paradigmatic situations in which strong recommendations may be warranted despite low or very low quality of evidence. These include the following: When low-quality evidence suggests benefit in a life-threatening situation (evidence regarding harms can be low or high) When low-quality evidence suggests benefit and high-quality evidence suggests harm or a very high cost When low-quality evidence suggests equivalence of 2 alternatives, but high-quality evidence suggests less harm for one of the competing alternatives When high-quality evidence suggests equivalence of 2 alternatives and low-quality evidence suggests harm in one alternative When high-quality evidence suggests modest benefits and low/very low quality of evidence suggests possibility of catastrophic harm
Internal Appraisal
A draft of the full guideline was distributed to GDG members for feedback and approval using electronic voting. GDG leadership reviewed these comments and incorporated them in a revised guideline prior to external review. Substantive changes were subject to re-vote of the GDG. GDG Vice-Chairs independently appraised the final guideline using Appraisal of Guidelines for Research & Evaluation II (AGREE II) criteria 19 to assess the validity of the guideline and the development process and to determine major areas of deficiency. Results were reviewed within the GDG leadership and any necessary corrections were made. Areas requiring substantive changes were presented to the full GDG and subject to re-vote.
External Review
A multidisciplinary group of clinicians and patient advocates were invited by the leadership group to externally review the guideline document. These individuals were selected based on their clinical expertise in a specific area and their willingness to participate. Comments and feedback were assessed by the GDG leadership and methodologists and incorporated into the final draft. Invited external reviewers included a broad spectrum of potential stakeholders (primary care physicians, neurosurgeons, orthopedic surgeons, critical care physicians, vascular medicine specialists, rheumatologists, and neurologists) and were asked to disclose financial and intellectual conflicts of interest. The Joint Guideline Committee at the AANS/CNS also externally reviewed all documents contributing to these guidelines. Reviewer comments were summarized by the GDG leadership and methodologists and made available to the full GDG together with the revised guideline. Substantial changes were subjected to re-vote by the full GDG and are reflected in the final guideline. The final guideline documents were distributed to AOSNA, AOSpine International, and CSRS for their approval.
Update Planning
The guidelines will be reviewed by the primary sponsor at 3 years to a maximum of 5 years following publication. A working group, consisting of a chair, a vice chair, an independent methodologist, and 2 to 5 content experts will follow a structured process to review the body of literature and search for new evidence that may influence the proposed recommendations. The working group will discuss the need to update the guideline with the leadership of the sponsoring organization. An update will be considered if there are changes in (1) the evidence related to harms and benefits, (2) outcomes which would be considered important for decision making, (3) ranking of current critical and important outcomes, and (4) available interventions and resources. 20
Footnotes
Appendix
Members of the SCI Guideline Development Group: Conflict of Interests.
| GDG Member | Employment (Specialty) | Industrial/Institutional Disclosures | Intellectual Disclosures |
|---|---|---|---|
| Bizhan Aarabi | Surgeon (Neurosurgery, Trauma) |
None |
None |
| Paul Arnold | Surgeon (Neurosurgery, Spine) |
None |
None |
| Darrel Brodke | Surgeon (Orthopaedic—Spine) |
None |
Prescribe, treat, recommend—treats patients with CSM |
| Anthony Burns | Physical Medicine/Rehab (Spinal Cord Medicine) |
None |
Prescribe, recommend, treat—prescribes therapies/interventions for individuals with myelopathies |
| Simon Carette | Rheumatologist |
None |
None |
| Robert Chen | Neurologist (Neurology and Neurophysiology) |
None |
Prescribe, recommend, treat—prescribes/recommends CSM |
| Kazuhiro Chiba | Surgeon (Spine and Spinal Cord Surgery) |
None |
Authorship—Japanese guideline for the management of CSM |
| Michael Fehlings | Surgeon (Neurosurgery) |
None |
Authorship—has published original research in CSM Prescribe, recommend, treat—is an active, practicing clinician in the field |
| Julio Furlan | Neurologist |
None |
Prescribe, recommend, treat—assesses and manages patients with CSM |
| James Harrop | Surgeon (Neurosurgery, Spine) |
Board membership—AOSpine: $0 Consultancy—DePuy spine: $30K Expert advisor—Tejin, Bioventus, Asterins: $20K |
Authorship—written several papers on CSM on general care and several studies, has no concrete beliefs Prescribe, recommend, treat—generally prescribes treatments for CSM |
| Langston Holly | Surgeon (Spine) |
Patent with Medtronic that may result in future income Expert witness/testimony: $12K paid to institution NIH grant: $330K paid to institution |
None |
| Sukhvinder Kalsi-Ryan | Physical Therapist, Clinician Scientist |
Consultancy—Neural Outcomes Consulting, Inc: $NR Officership—CSO of own company—Neural Outcomes: $NR Grants/contracts—CIHR, CINF, RHI, ONF: $NR Royalties—GRASSP version 1.0: $NR |
Authorship—first and co-author on many CSM publications |
| Mark Kotter | Surgeon (Spinal Neurosurgery) |
None |
Authorship—research papers on CSM, mainly investigating the underlying pathological changes and mechanisms of regeneration Prescribe, recommend, treat—as clinician, cares for CSM patients, and observes that there are no accepted guidelines on the subject thus far, and thus uncertainty as to how patients should be managed |
| Brian Kwon | Surgeon (Spine) |
None |
Public opinion—participated in debate on laminectomy and fusion versus laminoplasty at the AAOS meeting Prescribe, recommend, treat—treats condition non-operatively and surgically |
| Ralph Marino | Physical Medicine/Rehabilitation (Spinal Cord Injury) |
None |
Prescribe, recommend, treat—prescribes rehabilitation services for persons with cervical myelopathy |
| Allan Martin | Surgeon (Neurosurgery) |
None |
None |
| James Middleton | Rehabilitation Medicine |
None |
None |
| James Milligan | Family Medicine (Mobility issues, SCI) |
None |
None |
| Narihito Nagoshi | Surgeon (Spine) |
None |
None |
| Hiroaki Nakashima | Surgeon (Spine) |
None |
Authorship—much research regarding CSM Prescribe, recommend, treat—would recommend treatment |
| John Rhee | Surgeon (Orthopaedic) |
Board membership—CSRS: $0 Consultancy—Biomet Spine: $5K Royalties—Biomet Spine: $45K Stock ownership: Phygen/Alphatec Payment for lectures—Zimmer spine: $20K, Depuy Spine: $10K |
Authorship—research papers on CSM, no strongly held beliefs Prescribe, recommend, treat—as a surgeon, prescribes/recommends treatments for CSM |
| Daniel Riew | Surgeon (Cervical Spine) |
Chairman of Board—AOSpine International: <$50K Royalties—Biomet, Medtronic: <$1M Payment for lectures—AOSpine, NASS: <$20K Stock options: Expanding Orthpedics, Amedica, Benvenue, Nexgen, Spine, Osprey, Paradigm, Spinal Kinetics, Spineology, Vertiflex, PSD: <$25K Travel accommodations/meeting expenses—AOSpine NASS, SRS, Broadwater: <150K Grants—AOSpine, cerapedics, Medtronic: $50K |
Authorship—many publications in area of expertise |
| Anoushka Singh | Nurse, Researcher (Neurospine) |
None |
Authorship—work on CSM as part of PhD and postdoctoral work |
| Sumeet Sodhi | Primary Care Physician |
None |
Prescribe, treat, recommend—as a family doctor, does prescribe/recommend CSM |
| Lindsay Tetreault | Other |
Grant—potential future AOSpine Strategic Grant |
Authorship—Predicting Outcome in CSM |
| Jeff Wang | Surgeon (Spine) |
Board membership—AOSpine: $86,597 Honorariums—CSRS: $0; NASS: $0; CSRF: $0 Editorial boards: Spine, JAAOS, The Spine Journal, Journal of Spinal Disorders and Techniques, Global Spine Journal, The Journal of Orthopaedic Trauma Royalties—Stryker: $423, Osprey: $725, Biomet: $602 290, Synthes: $12 105, Seaspine: $33 823, Amedica: $28 491, Aesculap: $3813 Stock options—no money paid, but personal investments in: Bone Biologics, Alphatech, Axiomed, Amedica, Corespine, Expanding Ortho, Pioneer, Axis, Syndicom, VG Innovations, Pearldiver, Flexuspine, Fziomed, Benvenue, Promethean, Nexgen, Electrocore, Surgitech Expert witness—yes Travel reimbursements—AOSpine, CSRS, NASS, CSRF Fellowship funding paid to institution— USC Department of Orthopaedic Surgery: AO Foundation $75K |
Public opinion—has presented talks and moderated educational sessions at meetings on this topic Organization with stated opinion—member of NASS that has an AUC on cervical surgery, involved in formulating/voting for NASS Prescribe, recommend, treat—operates on patients with cervical pathology |
| Jefferson Wilson | Surgeon (Neurosurgery, Spine) |
None |
Authorship—several CSM manuscripts Prescribe, recommend, treat—recommends surgery for CSM |
| Albert Yee | Surgeon (Spine) |
None |
Prescribe, recommend, treat—involved in spine case |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by AOSpine, the Cervical Spine Research Society (CSRS) and the AANS/CNS Section on Neurotrauma and Critical Care. Dr Fehlings wishes to acknowledge support from the Gerald and Tootsie Halbert Chair in Neural Repair and Regeneration and the DeZwirek Family Foundation. Dr Tetreault acknowledges support from a Krembil Postdoctoral Fellowship Award.