
Abstract
Study Design:
Retrospective study.
Objective:
To analyze the various anatomical parameters that influence segmental stability in patients suffering from lumbar intra spinal cysts (LISCs) and to determine the outcome of microscopic unilateral laminotomy and cystectomy.
Methods:
All patients that were surgically managed for a LISC between 2007 and 2013 with more than 3 years of follow-up were reviewed. Those without associated instability were evaluated for segmental mobility, segmental angulation, facet inclination, stage of disc degeneration, and level of involvement on MRI and dynamic radiographs. Outcomes of unilateral laminotomy and cystectomy were evaluated using VAS (Visual Analogue Score), ODI (Oswestry Disability Index), and Macnabs criteria. Dynamic radiographs were performed in all cases pre- and postoperatively and at the last follow-up.
Results:
Thirty patients were operated for a LISC between 2007 and 2013. The levels involved were L4-5(23), L3-4(4) and L5-S1(3). The mean facet angle was 42.6 (± 6.1) degrees. The stage of disc degeneration was scattered haphazardly across all the cases (Gr 2[17]; Gr 3[1]; Gr 4[8]; Gr 5[4]). VAS and ODI scores improved significantly in all patients. Mean follow-up was 46.5 months (36-96 months). No patient developed postoperative instability at the last follow-up.
Conclusions:
The coronal inclination of the facet joints, absence of radiological instability, and poor co-relation with stages of disc degeneration suggests the presence of adequate residual stability. In this study, stand-alone decompression for LISCs without instability had well sustained good/excellent outcomes. Fusion is recommended for LISCs with associated instability.
Introduction
Lumbar intraspinal synovial cysts (LISCs) are a well-documented cause of spinal stenosis and radiculopathy. 1 Degeneration, instability, and repetitive microtrauma are often implicated as the cause of these cysts. 2 –6 The belief that LISCs may share an association with microinstability has shaped the way this condition is managed. Not surprisingly, many authors recommend primary fusion for the surgical management of LISCs. 2,3,7 –11 Furthermore, the fear that a stand-alone decompression could unmask latent instability or even lead to a recurrence of cyst, has also justified fusion. The aim of this study was to analyze various anatomical parameters that influence segmental stability and to determine the outcome of microscopic unilateral laminotomy and cystectomy in patients suffering from LISCs without associated instability.
Material and Methods
This retrospective study was conducted in a single tertiary-care institution. All patients that were operated for a LISC between 2007 and 2013 were reviewed.
The inclusion criteria were the following: Patients operated for a LISC with all pre- and postoperative radiological data available. Minimum 3 years’ follow-up.
The exclusion criteria were the following: Associated segmental instability as determined by pre-operative radiological assessment. Association of any other pathological process at that spinal segment such as congenital deformities, previous infections and surgery of the lumbar spine, tumors, or trauma.
Segmental instability was defined as more than 3.5-mm translation and more than 11° of angulation on dynamic standing lateral radiographs as defined by Panjabi and White. 12 Patients were evaluated for segmental mobility and angulation on preoperative dynamic x-rays, facet inclination and level of involvement on the axial magnetic resonance imaging (MRI) and stage of disc degeneration (Modified Pfirrmann’s Grading System) on the sagittal MRI. Facet inclination was defined as the angle generated by connecting the 2 end-points of each facet on a preoperative axial lumbar MRI (mid-section through the disc) and a line connecting the 2 ventral points of each facet joint. The term sagittal orientation of a facet joint was used for a facet inclination of more than 50°. All patients underwent a stand-alone midline sparing, microsurgical resection of the cyst.
Technique Used for Stand-Alone Decompression
Microscopic resection of the cyst was done via the micro-endoscopic decompression (med) technique with the 18-mm METRx tubular retractor system (Medtronic Sofamor Danek, Memphis, TN, USA). The surgeon stood on the contralateral side of the cyst and performed a laminotomy and accessed the cyst using the “over the top” technique. This was made possible by wanding of the tubular retractor and tilting the table. Once the cyst was adequately exposed, it was ruptured using the Kerrison or a spinal needle under vision. The walls were then removed. End-point of the procedure was complete resection of the cyst, adequate decompression of the thecal sac and contralateral nerve root with visualization of contralateral caudal pedicle.
Patients overall outcomes were evaluated using visual analogue scale (VAS) for back and leg pain and Oswestry Disability Index (ODI). Satisfaction with the surgical procedure was assessed using Macnabs’s criteria (excellent/good/average/poor). Dynamic radiographs were performed for all cases at the last follow-up. Postoperative MRI scan was done in 5 randomly selected patients to document the successful excision of LISC and preservation of the facet joint. All statistical analyses were performed using SPSS version 22.0 (IBM Corp, Armonk, NY, USA). A P value was set at <.05 for significance.
Results
A total of 36 patients with LISCs were operated between 2007 and 2013. Three patients had associated instability and were excluded from the study. Another 3 patients were lost to follow-up, with undeterminable surgical outcomes and were also excluded from the study. The remaining 30 patients that underwent a stand-alone microdecompression were evaluated. There were 18 males and 12 females with age ranging from 55 to 78 years and a mean age of 67 years. Eight patients had a grade I stable degenerative spondylolisthesis (no mobility on flexion-extension x-rays). The levels involved were L4-5(23), L3-4(4) and L5-S1(3). The mean facet angle was 42.6° (±6.1°) indicating a coronal inclination (Table 1; Figure 1a and b). The stage of disc degeneration in the decompression group was scattered randomly [Gr 2(17); Gr 3(1); Gr 4(8); Gr 5(4)] (Figure 2). The average follow-up was 46.5 months (range 36-96 months). With regard to the clinical outcomes, 1 patient with a bilateral foot-drop preoperatively showed complete neurological recovery at 1-years follow-up. The mean VAS score for leg pain at 1-year follow-up improved from 7.6 ± 0.9 to 1.6 ± 1.04 (P < .05) while that for back pain changed from 2.56 ± 0.98 to 1.87 ± 0.70 pre- and postoperative, respectively. The mean ODI scores improved from 61.50 ± 8.4 to 13.16 ± 5.14 (P < .05). Overall satisfaction with the surgical procedure was rated as excellent by 23 patients and good by 7. There were no “average” or “poor” results. None of the patients experienced a recurrence of symptoms at the last follow-up. There was a single case of incidental durotomy in the series which was managed successfully by squirting fibrin glue over the defect and watertight closure. There were no other complications or reoperations. Patients with stable, fixed degenerative spondylolisthesis fared as well as the rest of the patients with no statistically significant difference between the 2 groups (Table 2).
Facet Orientation of All the 30 Patients.a
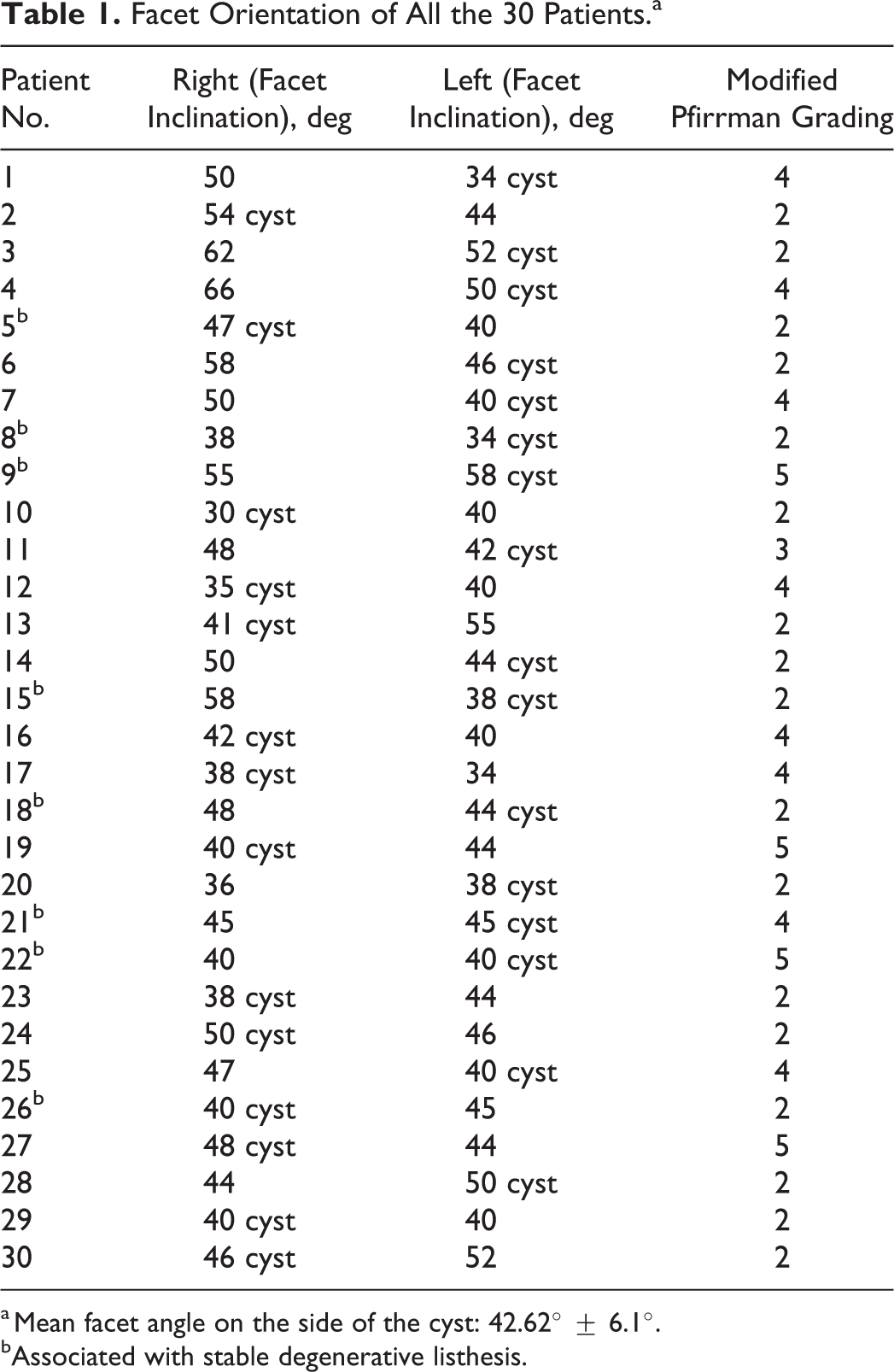
a Mean facet angle on the side of the cyst: 42.62° ± 6.1°.
bAssociated with stable degenerative listhesis.
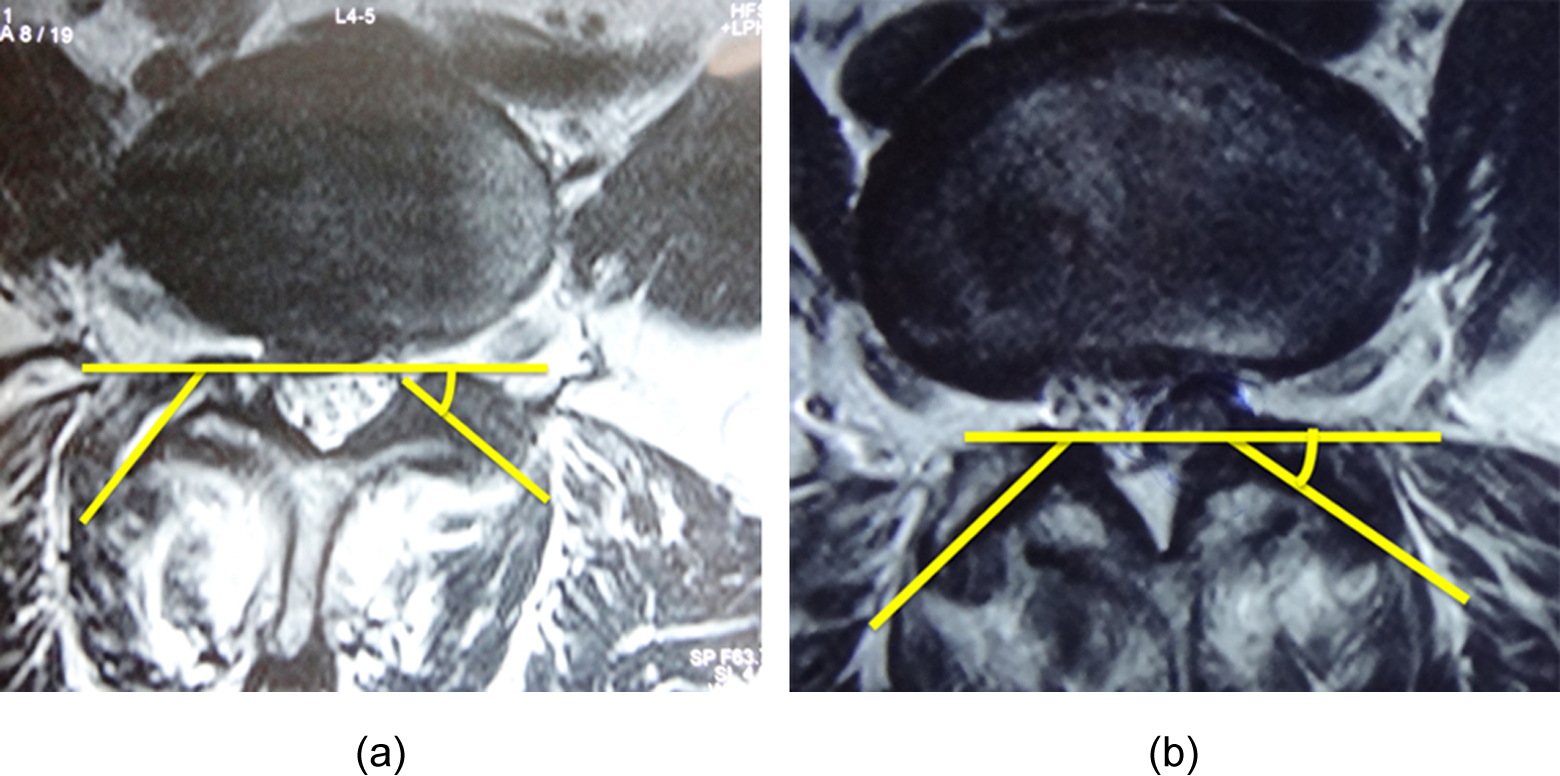
(a, b) Axial magnetic resonance imaging scan showing coronal orientation of facet joint in lumbar intraspinal synovial cysts.
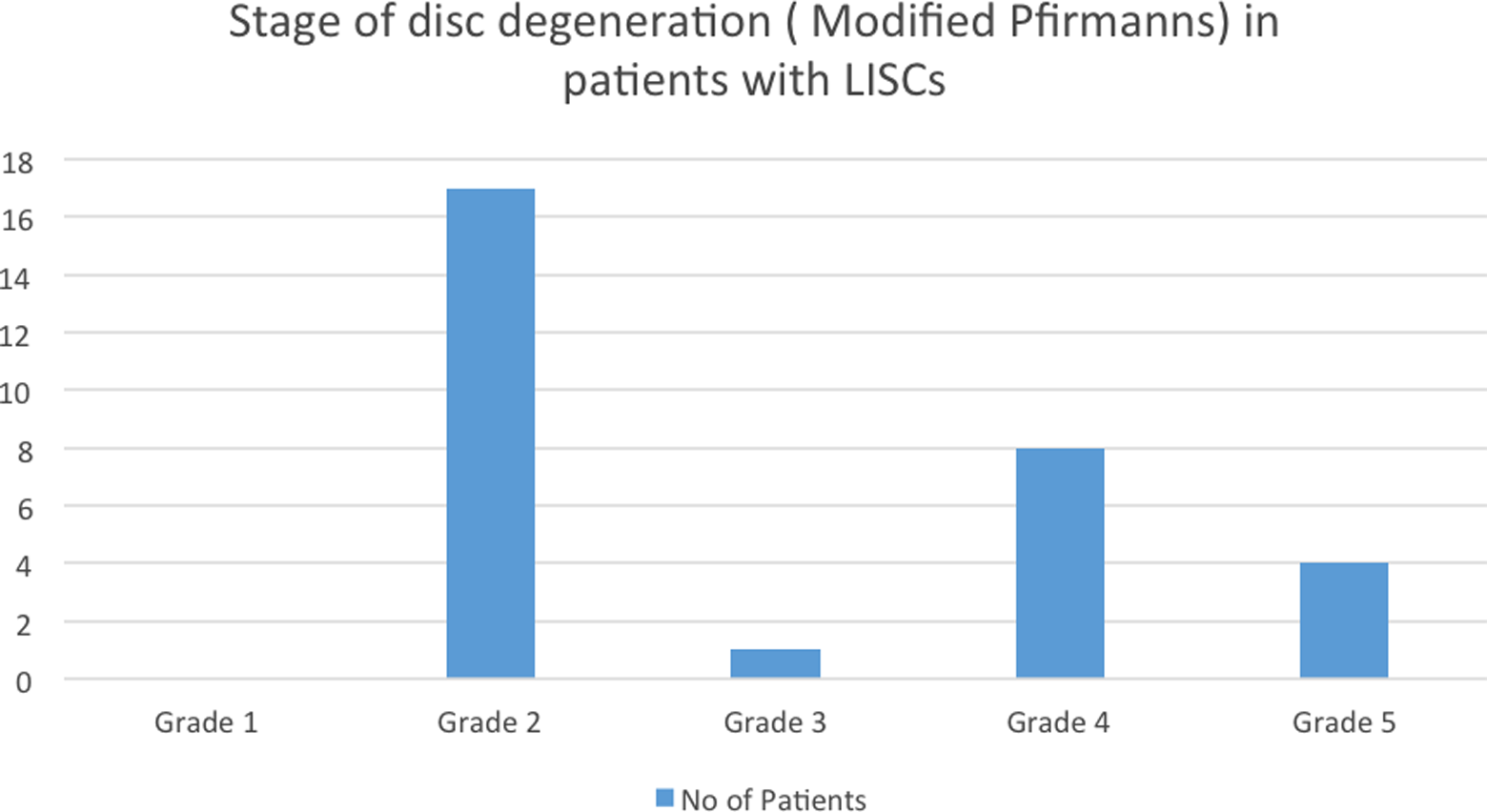
Distribution of Lumbar intraspinal synovial cysts according to the stage of disc degeneration (modified Pfirmann staging).
Subgroup Analysis of Patients With Stable Degenerative Listhesis and Those Without Any Listhesis.
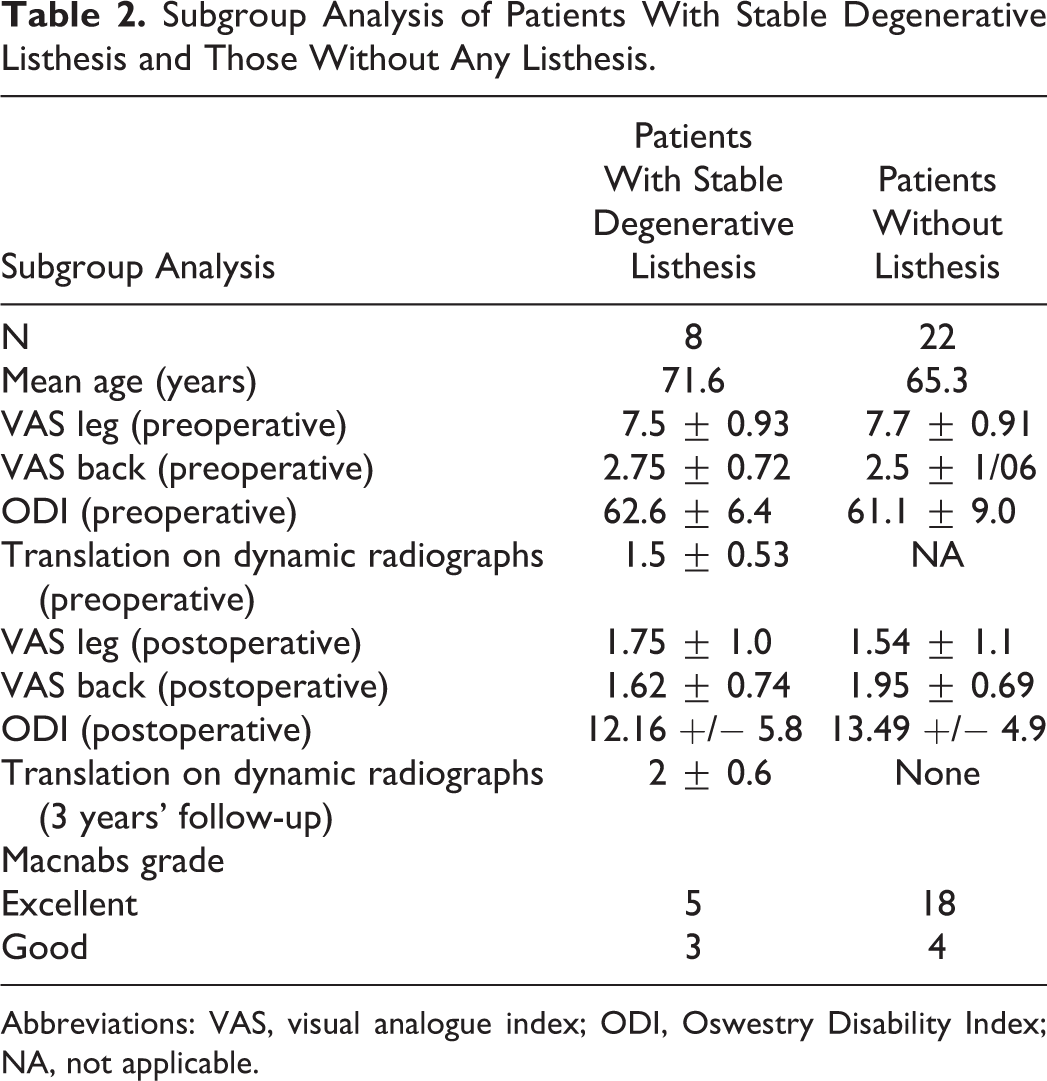
Abbreviations: VAS, visual analogue index; ODI, Oswestry Disability Index; NA, not applicable.
Discussion
Association With Instability
LISCs were first described by Baker 13 in 1885. They were described as a cause of nerve root compression in 195 0 14 and later confirmed by Kao et al 15,16 LISCs are typically situated posterolateral to the thecal sac, causing lateral recess stenosis and radiculopathy. These are most frequently seen at L4-L5, which is the single most mobile segment of the vertebral column. 5,6,17 In this study 23 of the 30 patients suffering from symptomatic LISCs presented at the L4- L5 level, supporting the hypermobility theory.
Various studies have highlighted spinal segmental instability as the cause of LISCs, 18,19 while others have implicated repetitive microtrauma. 11,18,20 Our observations question the etiology of instability as a cause of LISCs. Overt dynamic instability, defined as more than 11° of angulation and 3.5 mm of translation (values cited by Panjabi and White 12 for instability) was seen preoperatively in only 3 of the 36 patients and were managed with a fusion procedure (excluded from the final study group), while the remaining patients had acceptable segmental translation and angulation on flexion-extension erect radiographs. Standing dynamic radiographs in the subgroup of patients with stable degenerative spondylolisthesis revealed a mean postoperative translation of 2 mm as compared with the preoperative translation of 1.5 mm. However, all these patients continued to remain asymptomatic with no increase in back pain and with mid-term results comparable to the group without associated spondylolisthesis. There was no statistically significant difference seen in the outcomes of the two groups. Studies also cite a positive correlation between degenerative spondylolisthesis and sagittal lumbar facet-joint orientation. 21,22 Interestingly, in this series the orientation of the facet joints was mostly coronal (42.6 ± 6.1; <50), thus providing adequate segmental stability.
Some degree of lumbar spine disc degeneration with LISCs is reported in most clinical series. Metellus et al 20 observed that 89% of patients presented had disc degeneration. Lyons et al 11 reported 46% of patients with LISCs had degenerative disc disease. Disc degeneration, an indicator of spinal segment degeneration was present in all the cases. Since degeneration shares a high association with LISCs, it is reasonable to expect the degenerative cascade as described by Yong-Hing and Kirkaldy-Willis 23 to provide insight into the formation of synovial cysts. The cysts typically form as a part of complex local changes that occur within the facet joints to provide segmental stability in response to the first stage of the degenerative cascade, that is, disc degeneration and the consequent loss of disc height. After the loss of disc height, this cascade witnesses a stage of segmental instability resulting in a sequence of local adaptive changes, as an attempt is made to return stability to the affected segment (third stage). The progressive grading of intervertebral disc degeneration (modified Pfirrmann’s Grading System) coincides with the progressive stages of the degenerative cascade. If segmental instability shares an association with LISC formation, a higher distribution of LISCs at the higher grades of degenerative disc can be expected, that is, during the phase of segmental instability. However, in this study, we found the LISCs were present in patients with the involved level disc being evenly spread across all the stages of the degenerative cascade. Also, the presence of cysts in the earlier grades of degeneration disputes the “segmental instability factor” as the trigger for synovial cyst formation. In one of the patients, the synovial cyst was noticed at a stable L3-4 level, which was associated with mild disc degeneration while there was degenerative spondylolisthesis at the adjacent L4-5 level with no accompanying cyst formation (Figure 3a–c). As the L3-4 level was stable, only a cystectomy was done for this patient. The coronal inclination of the facet joints, absence of radiological instability, and poor correlation with stages of disc degeneration discourages an association between synovial cysts and instability. A hypermobile level (L4-5 most commonly involved) with constraints to mobility from coronally inclined facets may generate stress and micromotion encouraging cyst formation.
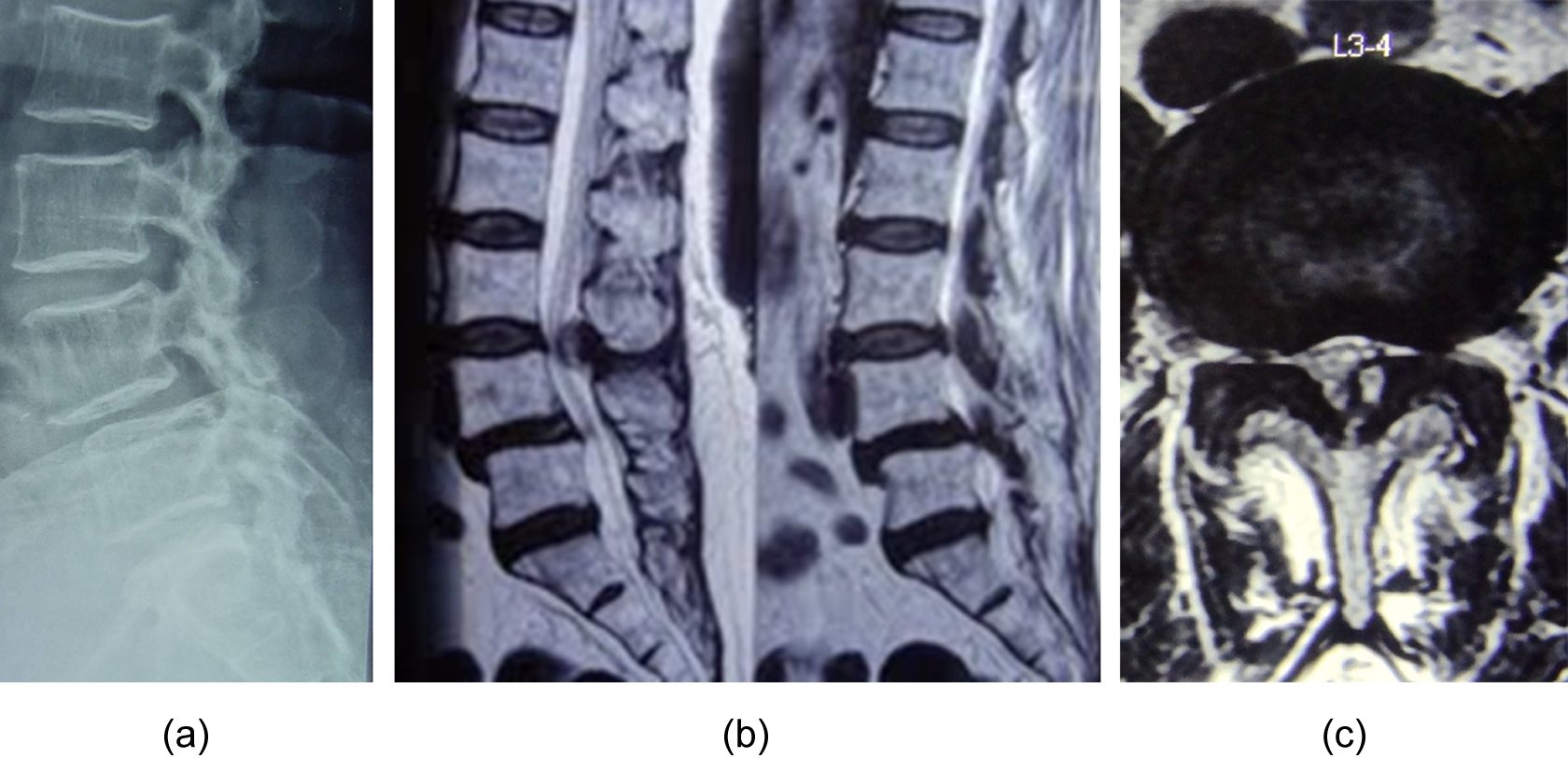
(a-c) L4/5 degenerative spondylolisthesis with facet cyst at stable L3/4.
Microsurgical Decompression
Many management options for symptomatic LISCs have been well studied. These range from image guided percutaneous procedures under local anesthesia to cyst excision and segmental fusion. Casselman 24 reported the first percutaneous facet joint steroid injection under radiological guidance. In 2009, Martha et al 25 reported the outcomes of the largest case series of LISCs managed by percutaneous, computed tomography–guided steroid injection and cyst rupture in 101 patients with long-term follow up. Cyst rupture was successfully carried out in 81% of the cases; however, 54% of patients subsequently underwent surgery due to inadequate relief of symptoms. While it is a safe, percutaneous procedure which is done under local anesthesia, it is also associated with high recurrence rates and often subsequent surgical procedures. The definitive treatment for symptomatic, unresolving synovial cysts not responding to conservative management is surgical. 7,11,19 The type of decompressive procedure and the need for fusion is debatable. A complete laminectomy and medial facetectomy was recommended, but some authors found this unacceptable as it could cause segmental instability. 4 –6 Similar incidence of postoperative instability following a microdecompression procedure for synovial cyst excision 11,19 is reported in literature as that of decompression for spinal stenosis without instability. 26,27 This finding reaffirms that no such underlying “micro”-instability exists in LISCs.
Xu et al 3 found that patients receiving laminectomy alone have an increased incidence of recurrent back pain and recurrent cyst relapse compared with those who underwent fusion. Khan et al 2 similarly observed those who underwent fusion had better outcomes than those who underwent laminectomy alone. Bydon et al 7 in a systematic literature review (1970-2009) of 82 published studies totaling 966 patients found 1.8% of the decompression-alone group developed same level recurrence while none of the fusion patients had cyst recurrence. In the same article, they discussed the spinal hypermobility theory of cyst pathogenesis and also proposed the possibility of concomitant fusion and cyst excision to prevent recurrence. The authors came to these conclusions as, within an average of 25.4 months postoperative, 6.2% of the only decompression group required revision surgery for mechanical back pain/instability. In the current study, with a minimal follow-up duration of 36 months and using the midline sparing microdecompression technique, no patients developed a same level recurrence of cyst or mechanical back pain. Hence the authors are of the opinion that concomitant fusion is not always needed to completely avoid recurrence. The authors believe that unless there is a demonstrable segmental instability assessed by clinical evaluation, dynamic radiographs, all LISCs can be treated successfully by decompression alone. Concern for decompression resulting in iatrogenic instability has led to use of microsurgical techniques in cyst excision involving minimal damage to the bony structures as was described by Deinsberger et al. 28 They recommended this approach, claiming it reduces the chances of instability and also the need for fusion. The authors also support this opinion.
Postoperative MRI scan done in 5 randomly selected patients, showed adequate decompression of the cysts without excess bony excision (preserved facets and midline structures) to compromise the stability of the segment (Figure 4a and b). This reflected well in the clinical outcomes as measured by VAS and ODI scores. The patient with an incidental durotomy was managed by squirting fibrin glue over the defect and no primary closure of the tear was attempted. Layered, watertight closure was done. The patient was mobilized out of bed the next day morning. No adverse sequelae were noted. All patients were asymptomatic at the last follow-up and this may reflect that there was no recurrence of the cyst. However, it is hard to conclude the same in the absence of MRI. No other complications were observed. All patients had relief of their leg symptoms which maintained at the last follow-up.
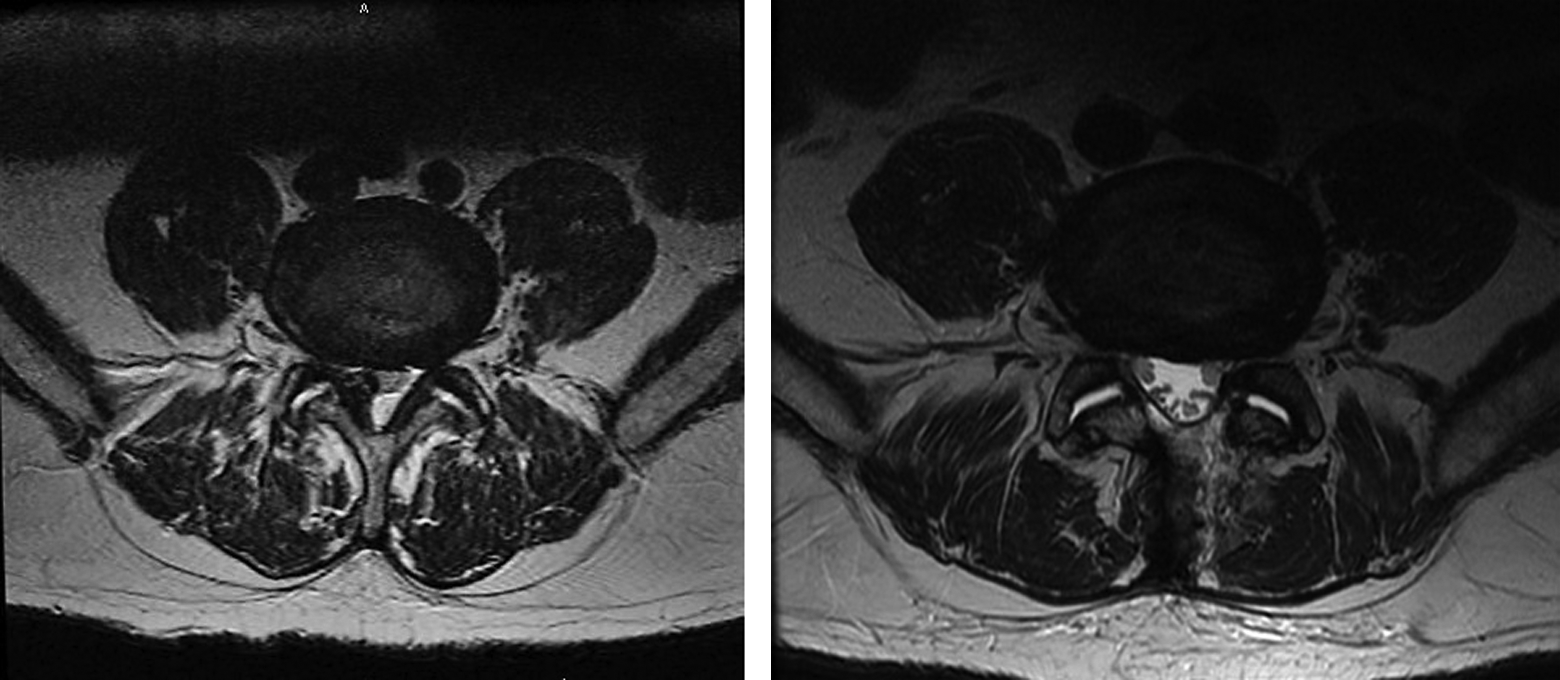
Microsurgical resection of the cyst showing adequate decompression without facet joint violation.
Limitations of the Study
This was a retrospective study with all cases operated by a single surgeon (corresponding author) and hence the results need to be corroborated by larger multicentric trials. The radiographic outcomes assessment was non-independent and evaluation did not include a MRI scan at 3 years’ follow-up. The deduction that there was no recurrence of the cyst is indirect, as none of the patients developed any clinical features suggestive of cyst recurrence (radiculopathy or back pain).
Conclusion
The coronal inclination of the facet joints, absence of radiological instability, and poor correlation with stages of disc degeneration suggests the presence of adequate residual stability. In this study, stand-alone decompression for LISCs without instability had well sustained good/excellent outcomes. Fusion is recommended for LISCs with associated instability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.