
Abstract
Study design
A multi-institutional retrospective study.
Objectives
To investigate risk factors of mechanical failure in three-column osteotomy (3COs) in patients with adult spinal deformity (ASD), focusing on the osteotomy level.
Methods
We retrospectively reviewed 111 patients with ASD who underwent 3COs with at least 2 years of follow-up. Radiographic parameters, clinical data on early and late postoperative complications were collected. Surgical outcomes were compared between the low-level osteotomy group and the high-level osteotomy group: osteotomy level of L3 or lower group (LO group, n = 60) and osteotomy of L2 or higher group (HO group, n = 51).
Results
Of the 111 patients, 25 needed revision surgery for mechanical complication (mechanical failure). A lower t-score (odds ratio [OR] .39 P = .002) and being in the HO group (OR 4.54, P = .03) were independently associated with mechanical failure. In the analysis divided by the osteotomy level (LO and HO), no difference in early complications or neurological complications was found between the two groups. The rates of overall mechanical complications, rod failure, and mechanical failure were significantly higher in the HO group than in the LO group. After propensity score matching, mechanical complications and failures were still significantly more observed in the HO group than in the LO group (P = .01 and .029, respectively).
Conclusions
A lower t-score and osteotomy of L2 or higher were associated with increased risks of mechanical failure. Lower osteotomy was associated with better correction of sagittal balance and a lower rate of mechanical complications.
Keywords
Introduction
Adult spinal deformity (ASD) is defined as a deviation of the alignment of the spinal column in adulthood. Recent studies have shown that ASD negatively affects health-related quality of life (HRQOL).1,2 Moreover, operative treatment achieves better HRQOL outcomes than non-operative treatment, especially in patients with severe deformity. 3
Different surgical strategies are suggested for correcting spinal deformity including three-column osteotomy (3CO), multiple corrective interbody fusion, and minimally invasive surgery using lateral lumbar interbody fusion. Despite the growing interest in minimally invasive surgery owing to advances in devices and surgical skills, invasive surgeries are sometimes required for severe and rigid deformities.
3CO uses pedicle subtraction osteotomy (PSO) or vertebral column resection (VCR). PSO and VCR have been described for severe and rigid deformities, mainly through a posterior approach.4-6 3CO for ASD surgery can offer significant deformity correction and lead to marked improvement of the spinal alignment and symptoms. However, 3COs are associated with high rates of mechanical complications and revision surgery.7,8
Studies have reported that an osteotomy at a lower level of the lumbar spine is more physiologically natural and provides a greater angle of correction.9-11 However, only a few studies have examined the influence of the osteotomy level on the risk of postoperative complications and revision surgery in 3CO for patients with ASD. Thus, this multicenter study investigated risk factors of revision surgery caused by mechanical failure in 3COs performed in relatively old Japanese patients, with a focus on the osteotomy level. Our hypothesis is that a lower level of osteotomy would result in better correction and a lower complication rate due to the longer lever arm for the correction (Figure).
Materials and Methods
Inclusion Criteria
This study is a retrospective observational study. Data of all patients with ASD who underwent 3CO between January 1, 2009, and December 31, 2016, at five institutions, which are high-volume spine centers, were retrospectively reviewed. Institutional review board approval was obtained at each site for patient enrollment and data collection protocols. The inclusion criteria were as follows: age ≥21 years at the time of surgery that included posterior instrumentation of ≥4 levels, follow-up period of ≥2 years, and sufficient radiographic data. The etiologies included degenerative kyphosis/kyphoscoliosis, post-vertebral fracture, and post-lumbar surgery. A 3CO was a procedure that involved PSO or VCR.
Data Analysis
Perioperative complications were defined as complications that occurred during and within 1 month after surgery, including neurological disorders, implant failure, deep vein thrombosis (DVT), PE, cerebrovascular diseases, respiratory disorders, cardiovascular disorders, delirium, surgical site infections, and spinal epidural hematoma. Mechanical complications included proximal junctional kyphosis (PJK), distal junctional kyphosis (DJK), pseudarthrosis, rod breakage, and vertebral fracture with or without revision surgery. PJK was defined as kyphosis >10° between the upper-instrumented vertebra and the two-level proximal vertebrae. DJK was defined as radiographically as ≥10° between the superior end plate of the LIV and the inferior end plate of the vertebra below on a standing lateral radiograph. Mechanical failure was defined as mechanical complications requiring revision surgery. 12
Demographic data, including age, sex, body mass index (BMI), medical comorbidities, and bone mineral density (BMD) of the femoral neck, were collected. Medical comorbidities were registered when patients had one of the following: diabetes, renal dysfunctions, cerebrovascular diseases, cardiovascular diseases, or respiratory diseases. Measurements on radiographs included the sagittal vertical axis (SVA), T4–T10 thoracic kyphosis (TK), sacral slope (SS), pelvic incidence (PI), and pelvic tilt (PT). These parameters were evaluated before and at 4 weeks after surgery in the standing position. X-ray images were also evaluated at the final follow-up. The radiographic parameter of −10<PI–LL <10° was defined as ideal alignment according to the SRS-Schwab ASD classification. All patients were distributed into two groups: patients with an osteotomy level higher than L2 as the higher osteotomy (HO) group and those with an osteotomy level lower than L3 as the lower osteotomy (LO) group. We routinely conduct L2-L5 interbody fusion and posterior facet fusion for Th12/L1 and L1/2 except for osteotomy level. In case of sacral fixation, we conduct L5/S1 interbody fusion as well.
Statistics
Statistical analysis was performed using IBM SPSS Statistics for Macintosh version 25.0 (IBM Corp., Armonk, NY, USA). T-tests were used to compare the averages of continuous variables and chi-square tests to compare the proportions of categorical variables between the groups. The F-test was used to confirm whether it is a normal distribution or not. According to the test outcomes, Student’s t-test was used for normal variance data and Welch’s t-test for non-normally distributed data. The risk factor analysis for mechanical failure was performed by multivariate logistic regression with a stepwise forward procedure (P < .1 for entry). A P-value <.05 was considered statistically significant. Missing values were imputed using the last observation carried forward method. Propensity score matching was performed as follows. First, the propensity scores for mechanical failure and non-failure cases were calculated using patient age and sex, preoperative SVA and LL, and sacral fusion. The C-statistics was .6679, which suggested a moderately good fit. Then, HO and LO cases were matched based on the propensity score with caliper <.4.
Results
This study included a total of 111 patients with ASD, who underwent 3CO and had full pre- and postoperative radiographic data and a minimum 2-year follow-up. The mean age at surgery was 72.5 ± 9.1 years, and 92 (82.9%) patients were female. Sixty patients had an osteotomy level of L3 or lower, whereas 51 patients had an osteotomy level of L2 or higher.
Univariate and Multivariate Analysis to Assess Risk Factors for Mechanical Failure.
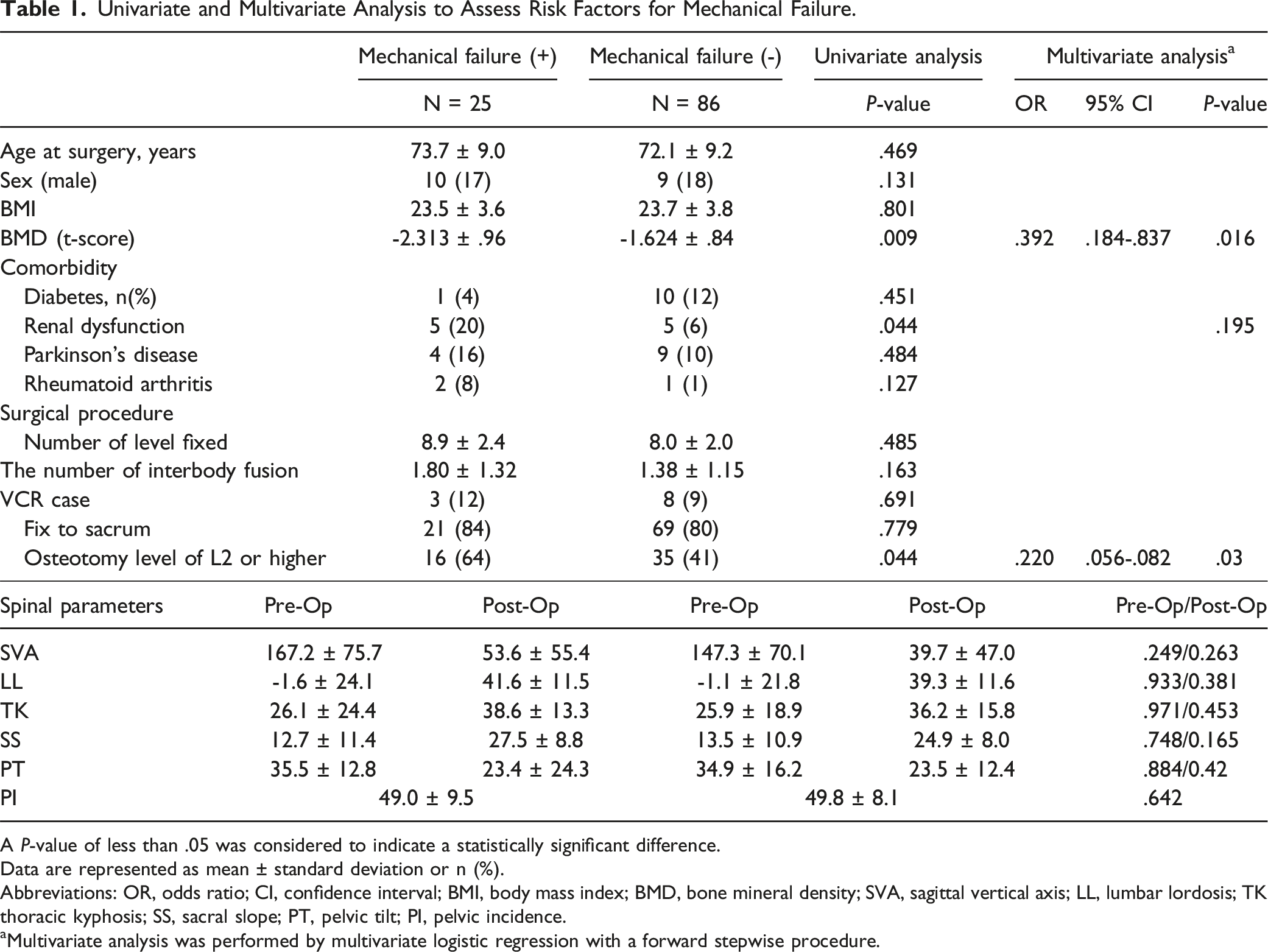
A P-value of less than .05 was considered to indicate a statistically significant difference.
Data are represented as mean ± standard deviation or n (%).
Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; BMD, bone mineral density; SVA, sagittal vertical axis; LL, lumbar lordosis; TK thoracic kyphosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence.
aMultivariate analysis was performed by multivariate logistic regression with a forward stepwise procedure.
Demographic and Operative Characteristics Between the LO Group and HO Group.
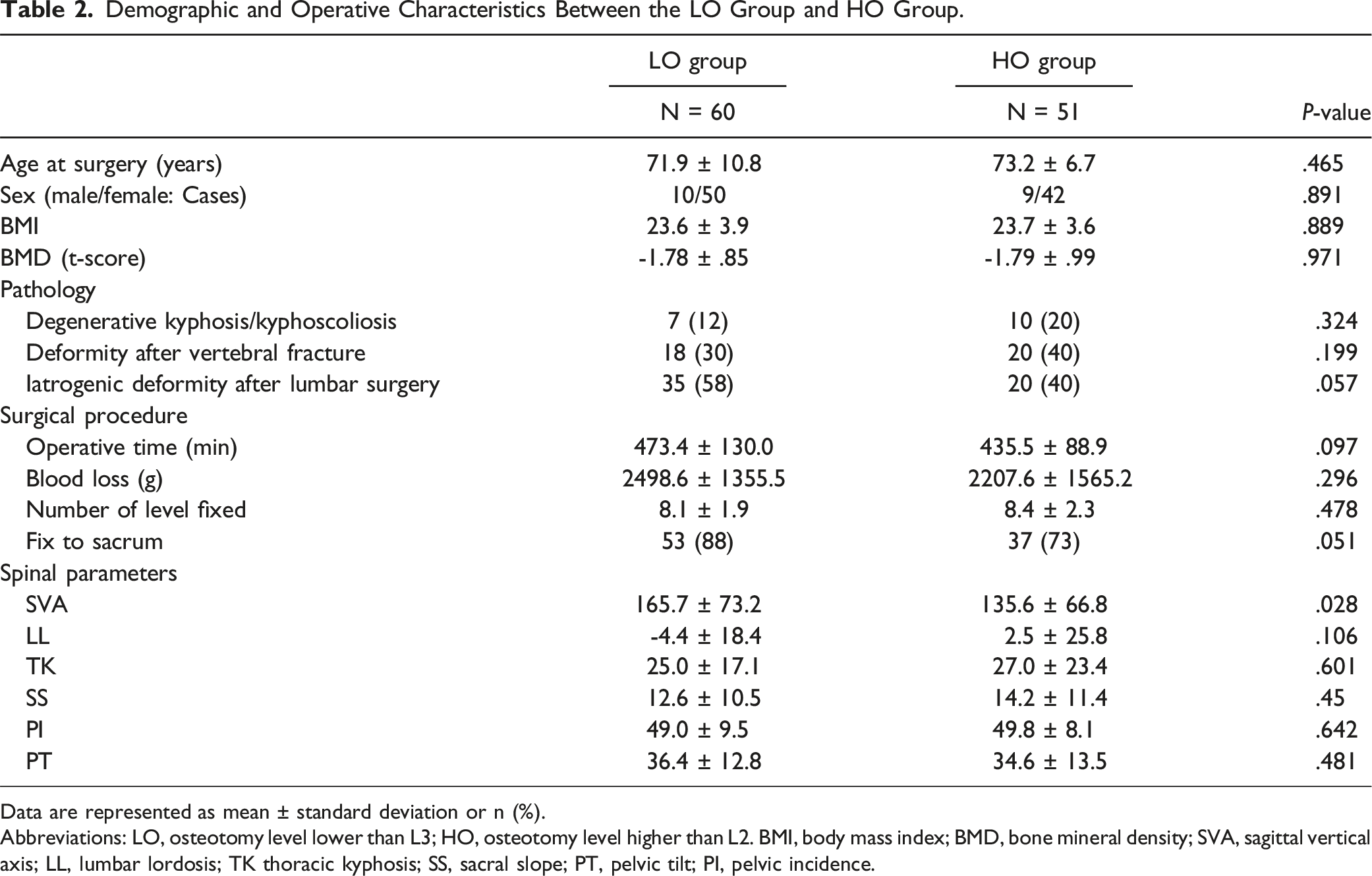
Data are represented as mean ± standard deviation or n (%).
Abbreviations: LO, osteotomy level lower than L3; HO, osteotomy level higher than L2. BMI, body mass index; BMD, bone mineral density; SVA, sagittal vertical axis; LL, lumbar lordosis; TK thoracic kyphosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence.
Postoperative Complications in the LO Group and the HO Group.
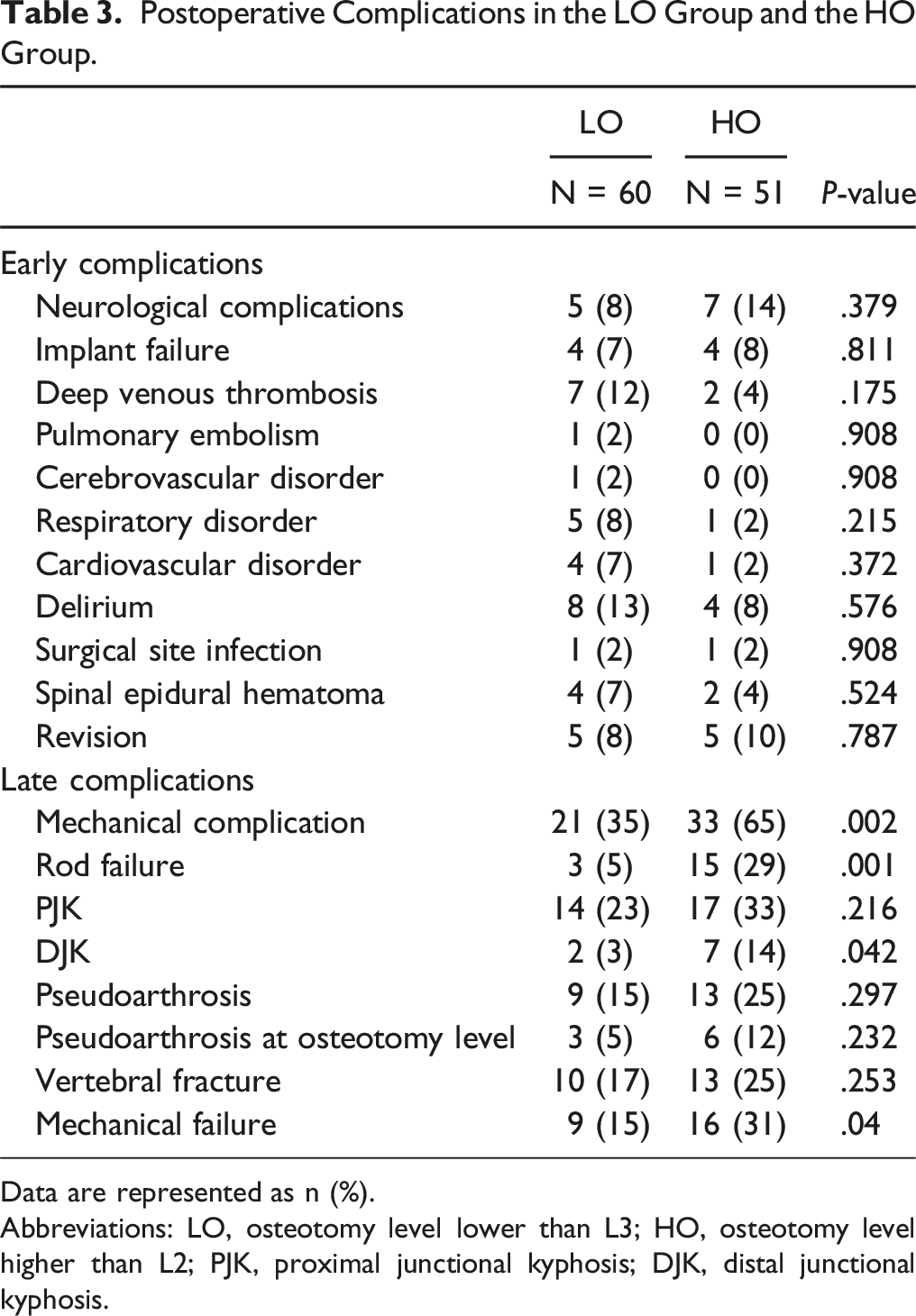
Data are represented as n (%).
Abbreviations: LO, osteotomy level lower than L3; HO, osteotomy level higher than L2; PJK, proximal junctional kyphosis; DJK, distal junctional kyphosis.
Postoperative radiographic Parameters of the LO Group and HO Group.
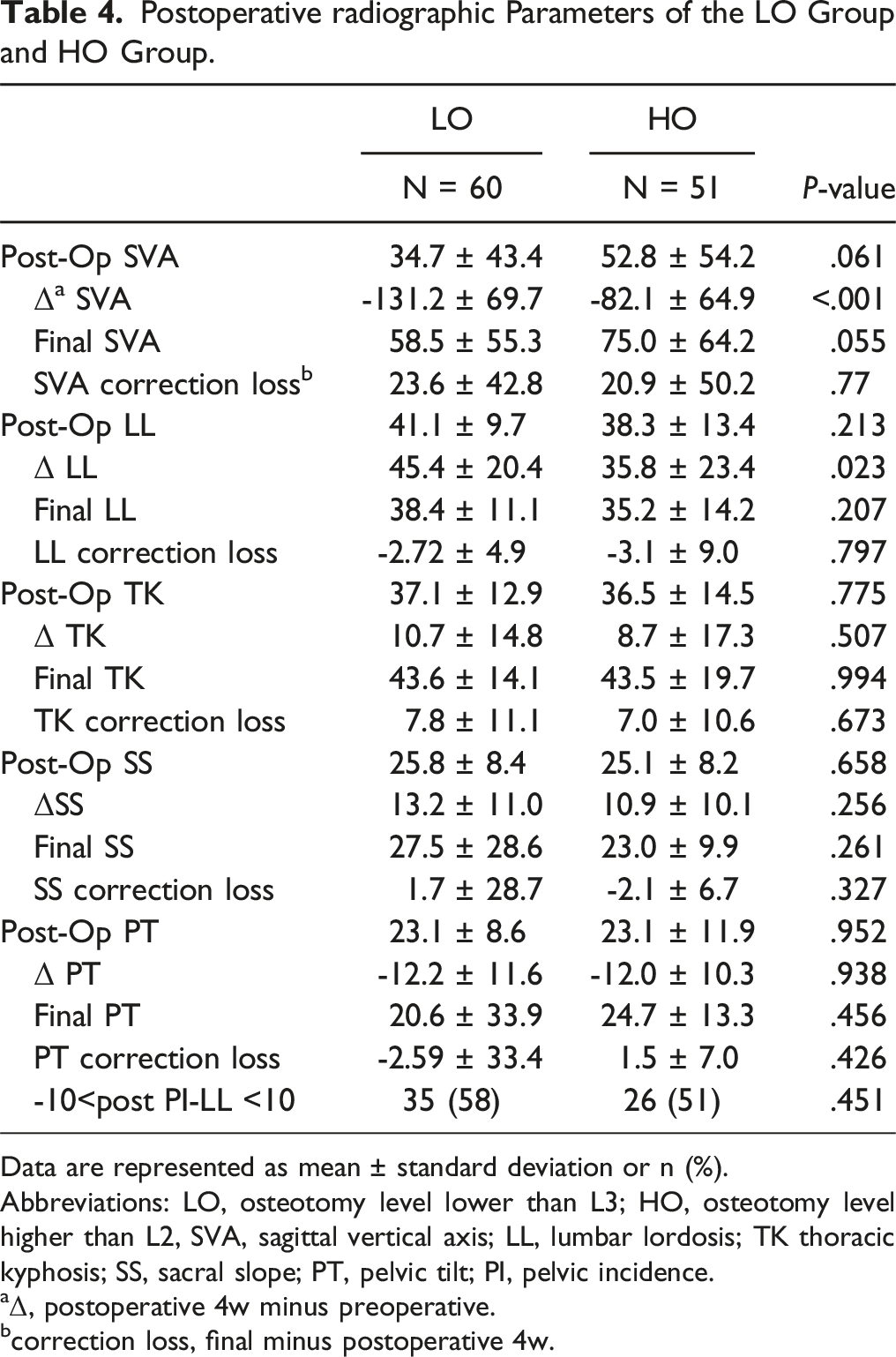
Data are represented as mean ± standard deviation or n (%).
Abbreviations: LO, osteotomy level lower than L3; HO, osteotomy level higher than L2, SVA, sagittal vertical axis; LL, lumbar lordosis; TK thoracic kyphosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence.
Δ, postoperative 4w minus preoperative.
correction loss, final minus postoperative 4w.
Differences Between the LO Group and the HO Group After Propensity Score Matching. a
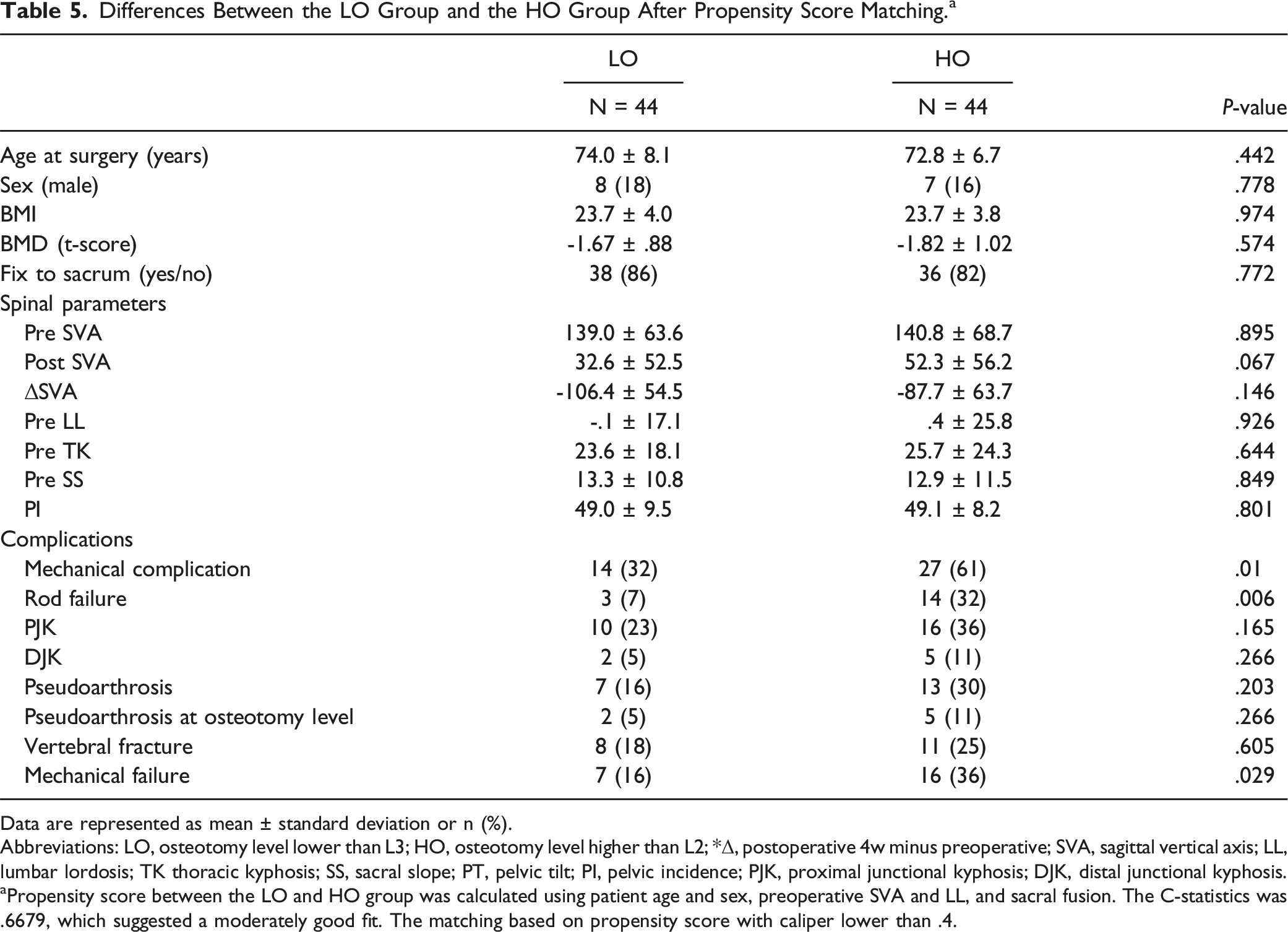
Data are represented as mean ± standard deviation or n (%).
Abbreviations: LO, osteotomy level lower than L3; HO, osteotomy level higher than L2; *Δ, postoperative 4w minus preoperative; SVA, sagittal vertical axis; LL, lumbar lordosis; TK thoracic kyphosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence; PJK, proximal junctional kyphosis; DJK, distal junctional kyphosis.
aPropensity score between the LO and HO group was calculated using patient age and sex, preoperative SVA and LL, and sacral fusion. The C-statistics was .6679, which suggested a moderately good fit. The matching based on propensity score with caliper lower than .4.
Discussion
The spinal osteotomy with the potential to achieve the greatest correction of spinal deformity is the procedure that extends through all three columns of the spine, i.e., 3CO procedures. 13 Although operative techniques such as 3COs, including PSO and VCR, allow significant improvement of severe and rigid spinal malalignment through a posterior-only approach, these procedures were technically demanding and associated with significant complication rates/high revision rates. 14 This study investigated that whether the osteotomy level influenced on deformity correction and complication rates using the propensity score-matched analysis and multiple logistic regression analysis in 111 patients who underwent 3CO. To our best knowledge, this study is the largest sample analysis that discussed whether the osteotomy level affected surgical complications, especially mechanical complications.
A clear consensus regarding the ideal osteotomy level has not yet been established. Surgeons preferred 3CO at L2 or L3 in the era of the first development of PSO/VCR because they regarded that the distal lumbar spine appears to have a greater risk for neurologic complications and fewer fixation points were achievable distally.10,15 Later, a study reported that 3CO at the thoracic level could achieve a robust correction for severe TK or deformity following vertebral fracture. 13 Meanwhile, L3 or L4 has been the common osteotomy level to achieve a good proportion of lumbar lordosis in the last decade. 14 Recently, L5-PSO is becoming more frequently used to obtain a stronger lever arm and a higher power of correcting the sagittal deformity. 4
This study demonstrated that early complications including postoperative neuralgic complications did not differ between the LO and HO groups, whereas late complications were more common in the HO group than in the LO group. 16 Recent development in surgical techniques, devices, or intraoperative neurological monitoring may result in fewer early postoperative complications even in caudal osteotomy. Meanwhile, in this study, the background between the LO and HO groups differed in the rate of sacral fusion, preoperative SVA, and LL. A lower rate of sacral fusion and greater preoperative SVA in the HO group might affect the rate of later complications. Thus, we further matched the preoperative SVA and LL, sacral fusion rate, age, and sex using propensity score-matched analysis. After the matching, there were no significant difference between LO group and HO group in the rate of sacral fixation and other radiographic parameters. The propensity score-matched analysis also showed that the LO group developed lower mechanical complications (31.8% vs 61.4%) and had lower mechanical failure rates (15.9% vs 36.4%) than the HO group, and post SVA tended to be lower in the LO group.
Mechanical complications and failure are relatively common following 3CO surgery.17-19 Penalosa et al 20 reported that the overall rate of instrumentation failure after PSO in ASD surgery within 1 year was 19.5%, and preoperative PI and PT were risk factors of failure. Auerbach et al 7 stated that major complications occurred in 35% of patients who underwent 3CO and that preoperative SVA, age ≥60 years, and presence of ≥3 medical comorbidities are risk factors of major compliactions. Bari et al reported that the mechanical failure rate 2 years postoperatively was 34% and that sacral fusion and preoperative PT >20° were associated with increased risks of revision. 11 Previously, postoperative high global tilt is also reported to be a risk of mechanical complications and revisions. 12 In the current study, the difference between the LO and HO groups was found in Δ SVA and Δ LL, other than mechanical complication/failure. Caudal osteotomy could provide a longer corrective lever arm and achieve greater LL and SVA, which might reduce mechanical complication and failure rates. Pizones et al reported that caudal level of PSO produced lumbar lordosis at the lower level, 11 and Lafage et al 9 showed that deformity correction at the lower level of lumbar spine was associated with lower incidence of mechanical complications. These reports may support our results demonstrating that the lower level of osteotomy reduced mechanical complications and revisions.
Among mechanical complications, rod fracture was more observed in the HO group than in the LO group (29% and 5%, respectively). It is reported that rod fracture was found in 12% of the cases after the ASD procedure, and PSO was a risk factor for rod fracture in the recent meta-analysis. 21 It is practically difficult to completely avoid the rod fracture after long fusion for deformity correction even if we use rigid rod, such as cobalt-chrome rod. However, previous reports suggested that interbody fusions at the adjacent level of the osteotomy and using multiple rods can reduce the risk of rod fracture after the PSO procedure. 22 Therefore, the results of this study suggested that interbody fusion at the adjacent segment of osteotomy and/or multiple rods was highly recommended for procedures with a HO level osteotomy.
Low BMD was found to be related to mechanical failure in the multivariate analysis in this study. We further analyzed the BMD of the LO mechanical failure patients vs LO mechanical non failure cases and the HO mechanical failure cases vs HO mechanical non failure patients. The BMD showed lower values in cases with mechanical failure either in LO or HO group. The mean t-score of LO mechanical failure patients was -2.450 ± .676 and of LO mechanical failure cases was -1.690 ± .835 (P = .092). The mean t-score of HO mechanical failure patients was -2.264 ± 1.065 and of HO mechanical non failure cases was -1.530 ± .866 (P = .046). Low BMD was a cause of subsequent fracture or PJK. Yagi et al 23 reported that BMD was a significant risk factor of PJK in patients who underwent ASD surgery in their propensity score-matched analysis,. Bisphosphonates are first-line agents due to their low cost and high evidences for low BMD patients. However, optimizing bone quality with anabolic agents should be considered in preparation for deformity correction surgeries due to their beneficial and favorable effects on fusion and hardware compared to the antiresorptive drugs. 24 Thus, strong prophylactic treatment, such as Teriparatide or Romosozumab, should be considered when the patient’s t-score was low, regardless of the osteotomy level.
This study has several limitations. First, this study has a selection bias, in which the surgeon could change the surgical procedure and osteotomy level based on the patient’s alignment. Thus, a propensity score matching analysis was performed to reduce the bias. Second, as this is a multicenter study, simple criteria were used to identify mechanical complications using plain-film X-ray imaging. Thus, the diagnosis of mechanical complications by plain-film X-ray imaging may underestimate the rate of pseudoarthrosis. Third, as we focused on radiological mechanical complications after corrective 3CO surgeries for ASD, detailed clinical scores, such as patient-reported outcome measurement, were not included in this study. Prospective studies with large sample sizes and more detailed and longer clinical evaluations are needed to clarify the ideal osteotomy level to obtain the most favorable results. Fourth, we could not elucidate differences in clinical outcomes between PSO and PVCR. We added information of the pathology and the osteotomy technique in Tables 1 and 2 Clinical outcomes might be different between PSO and PVCR considering their surgical invasiveness. However, the osteotomy technique (PSO/PVCR) did not affect mechanical failure or osteotomy level (LO/HO) in the sample size of this study. Despite the limitation, this study addressed the relationship between postoperative complication and osteotomy level in 3CO and indicated that an osteotomy level of L3 or lower had lower mechanical complication/failure rates than that of L2 or higher. The result of this study could help determine the ideal osteotomy level in terms of clinical outcomes in daily clinics or further research.
Conclusions
Mechanical complications and failures were less observed in 3CO at L3 or lower than at L2 or higher, whereas early complications including neurological complications did not differ between the two groups. Low BMD was a risk factor for mechanical failure regardless of the osteotomy level. The surgeon should carefully restore the LL proportion, especially in cases with a high osteotomy level and prophylactic treatment for osteoporosis.
Supplemental Material
Supplemental Material - The lower Osteotomy Level is Associated With Decreased Revision Surgery Due to Mechanical Complications After Three-Column Osteotomy in Patients With Adult Spinal Deformity: A Multi-Institutional Retrospective Study
Supplemental Material for The lower Osteotomy Level is Associated With Decreased Revision Surgery Due to Mechanical Complications After Three-Column Osteotomy in Patients With Adult Spinal Deformity: A Multi-Institutional Retrospective Study by Atsuyuki Kawabata, Kenichiro Sakai, Kentarou Yamada, Kurando Utagawa, Jun Hashimoto, Shingo Morishita, Yu Matsukura, Takuya Oyaizu, Takashi Hirai, Hiroyuki Inose, Masaki Tomori, Ichiro Torigoe, Hiroaki Onuma, Kazuo Kusano, Kazuyuki Otani, Yoshiyasu Arai, Shigeo Shindo, Atsushi Okawa, Toshitaka Yoshii in Global Spine Journal
Footnotes
Author Contributions
AK analysed the data and wrote the original draft. TY, KY conceived of, reviewed, and edited the paper. KS, KU, JH, SM, TO, TH, MY, HI, YM, MT, IT, and KK acquired the data. KO performed the investigation. YA validated the paper. YA, SS, and AO supervised the researched. All authors contributed to the writing of the final manuscript. All authors approved the manuscript to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the ethics committee of all institutions involved. The ethical committee, Tokyo Medical and Dental University; M2017-115. The ethical committee, Saiseikai Kawaguchi General Hospital; 29-2. The ethical committee, Kudanzaka Hospital; 2019-5.
Consent to Participate
Informed consent was waivered by the above ethics committee as the present retrospective cohort study involved already existing data and records at the time of investigation, and did not retain personal identifiers of the gathered information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.