
Abstract
Study Design:
Multicenter retrospective study.
Objectives:
To investigate the risk of symptomatic recurrent laryngeal nerve palsy (RLNP) following cervical spine surgery, to examine risk factors for its development, and to report its treatment and outcomes.
Methods:
A multicenter study from 21 high-volume surgical centers from the AOSpine North America Clinical Research Network was performed. Each center screened for rare complications following cervical spine surgery, including RLNP. Patients were included if they underwent cervical spine surgery (levels from C2 to C7) between January 1, 2005 and December 31, 2011. Data were analyzed with regard to complication treatment and outcome. Cases were compared to a control group from the AOSpine CSM and CSM-I studies.
Results:
Three centers reported 19 cases of RLNP from a cohort of 1345 patients. The reported incidence of RLNP ranged from 0.6% to 2.9% between these 3 centers. Fifteen patients (79%) in the RLNP group were approached from the left side. Ten patients (52.6%) required treatment for RLNP—6 required medical therapy (steroids), 1 interventional treatment (injection laryngoplasty), and 3 conservative therapy (speech therapy). When examining outcomes, 73.7% (14/19) of cases resolved completely, 15.8% (3/19) resolved with residual effects, and in 10.5% (2/19) of cases this could not be determined.
Conclusions:
In this multicenter study examining rare complications following cervical spine surgery, the risk of RLNP after cervical spine surgery ranged from 0.6% to 2.9% between centers. Though rare, it was found that 16% of patients may experience partial resolution with residual effects, and 74% resolve completely.
Keywords
Introduction
Recurrent laryngeal nerve palsy (RLNP) is a known complication of cervical spine surgery. 1,2 Given the proximity of both recurrent laryngeal nerves to the esophagus and trachea, these nerves may be damaged most often during anterior approaches to the neck, in which surgical trauma may occur. Unilateral or bilateral RLNP may manifest as dysphonia, aspiration, and/or dysphagia; in other cases it may be entirely asymptomatic. 3,4
The estimated incidence of RLNP with vocal cord paralysis after anterior cervical spine surgery is between 0.2% and 24.2%. 1 Risk factors include right-sided approaches and revision procedures. 1 However, most studies examining this complication are single-institution case series, which may be at risk of diagnostic, operative, and management bias. 1
The purpose of this multicenter study was to investigate the risk of symptomatic RLNP following cervical spine surgery, to examine risk factors for its development, and to report its treatment and outcomes.
Methods
Study Design and Population
This study received institutional review board approval at all participating institutions. This was a retrospective multicenter case-series study involving 21 high-volume surgical centers from the AOSpine North America Clinical Research Network, selected for their excellence in spine care and clinical research infrastructure and experience. Medical records for 17 625 patients who received cervical spine surgery (levels from C2 to C7) between January 1, 2005 and December 31, 2011, inclusive, were reviewed to identify occurrence of 21 predefined treatment complications. The complications included reintubation requiring evacuation, esophageal perforation, epidural hematoma, C5 palsy, RLNP, superior laryngeal nerve palsy, hypoglossal or glossopharyngeal nerve palsy, dural tear, brachial plexopathy, blindness, graft extrusion, misplaced screws requiring re-op, anterior cervical infection, carotid artery injury or cerebrovascular accident, vertebral artery injuries, Horner’s syndrome, thoracic duct injury, tetraplegia, intraoperative death, revision of arthroplasty and, pseudomeningocele. The comparative (control) group consisted of subjects enrolled in the AOSpine CSM and CSM-I studies.
Data Collection
Trained research staff at each site abstracted the data from medical records, surgical charts, radiology imaging, narratives, and other source documents for the patients who experienced one or more of the complications from the list. Data were transcribed into study-specific paper Case Report Forms (CRF). Copies of CRF forms were transferred to the AOSpine North America Clinical Research Network Methodological Core for processing, cleaning and data entry.
Data Analysis
Descriptive statistics were provided for baseline patient characteristics. Paired t test was used to analyze changes in clinical outcomes at follow-up compared with preoperative status.
Results
The 21 participating centers reported outcomes of 17 625 patients. Three centers reported 19 cases of RLNP from a screened cohort of 1345 patients; the incidence of RLNP ranged from 0.6% to 2.9% between these 3 centers. All patients presented with hoarseness and were diagnosed with a combination of flexible nasolaryngoscopy and/or flexible fiber-optic laryngoscopy. Three patients (15.8%) with RLNP had a history of previous cervical spine surgery.
General Patient Demographics and Operative Variables
Characteristics of patients in the RLNP and control groups are summarized in Table 1. Patient age and gender were not significantly different between groups, but 27.5% of patients in the control group reported smoking compared with only 5.3% in the RLNP cohort (P = .031). Patients in the control group had more severe myelopathy compared with patients in the RLNP group, as evidenced by worse modified Japanese Orthopaedic Association (13 vs 17.4) and Nurick (3.0 vs 1.3) scores (P < .001).
Demographics of Patients Who Experienced Recurrent Laryngeal Nerve Palsy (RLNP) Compared With the Control Group.
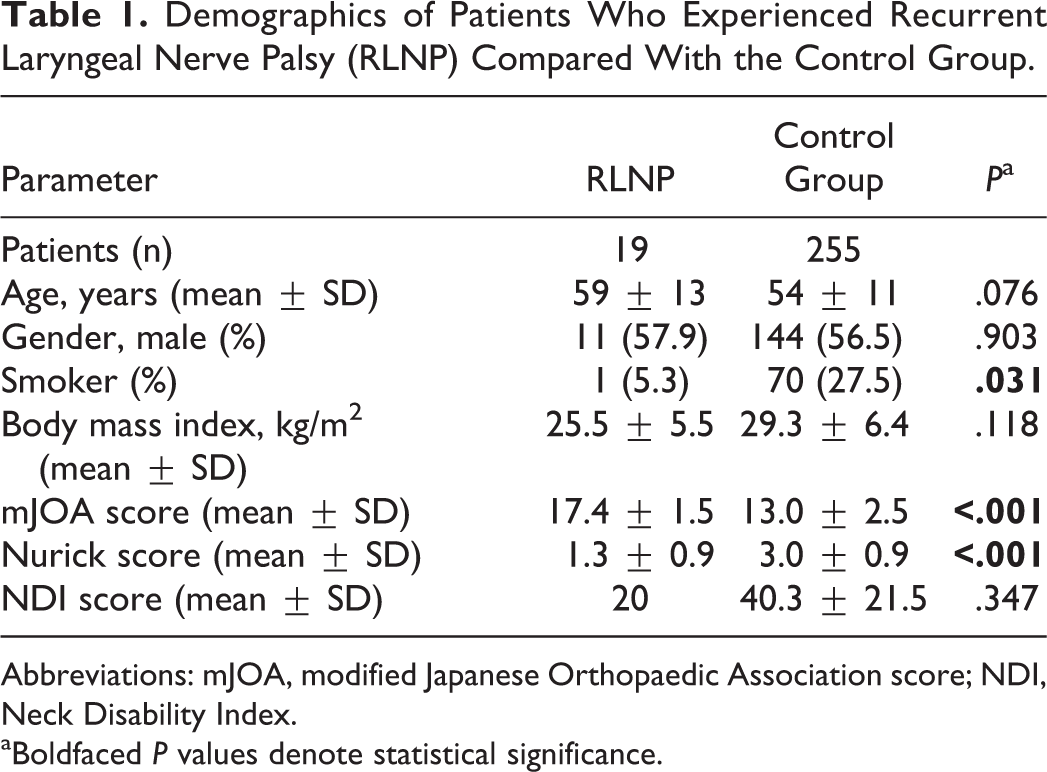
Abbreviations: mJOA, modified Japanese Orthopaedic Association score; NDI, Neck Disability Index.
aBoldfaced P values denote statistical significance.
The operative approach was also significantly different between groups, with circumferential operations being more common in the control group versus the RLNP group (7.1% vs 0%), and posterior approaches being more common in the RLNP group versus the control group (5.3% vs 0%) (Table 2). The C5 vertebra was involved in 93.7% of cases in the control group compared with 73.7% in the RLNP group (P = .009). Fifteen patients (79%) in the RLNP were approached from the left side.
Surgical Variables of Patients Who Experienced Recurrent Laryngeal Nerve Palsy (RLNP) Compared With the Control Group.
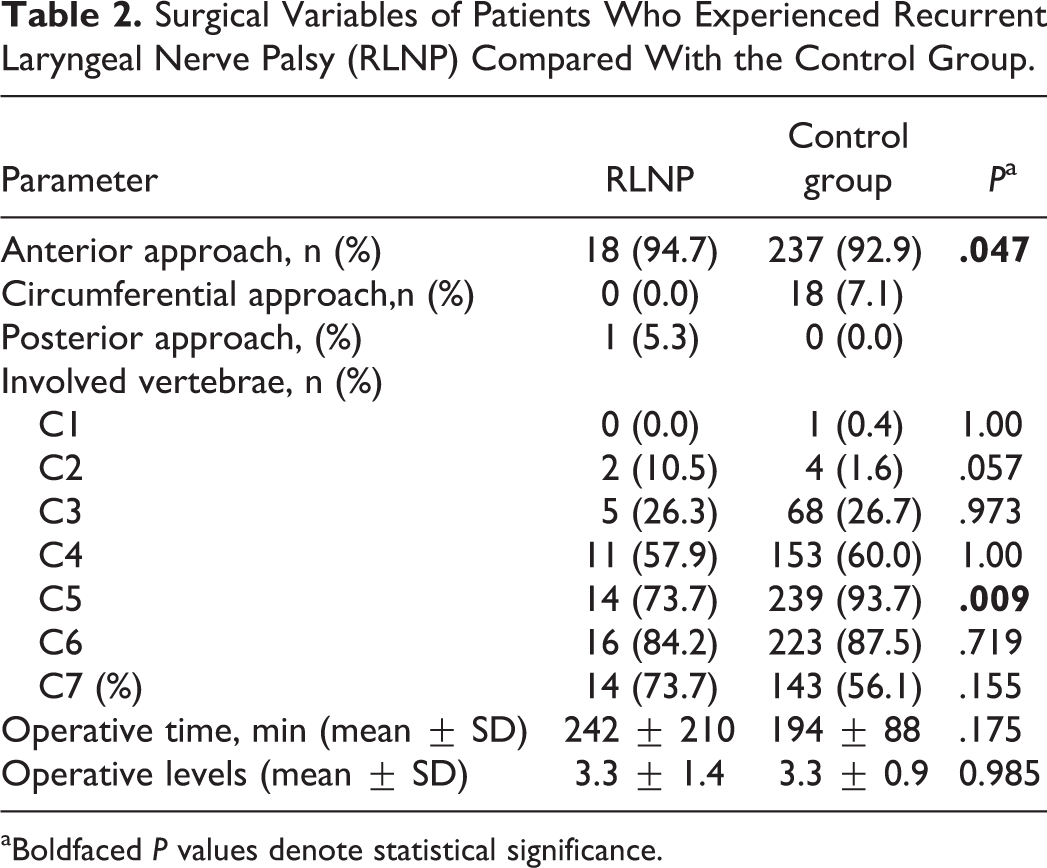
aBoldfaced P values denote statistical significance.
Outcomes
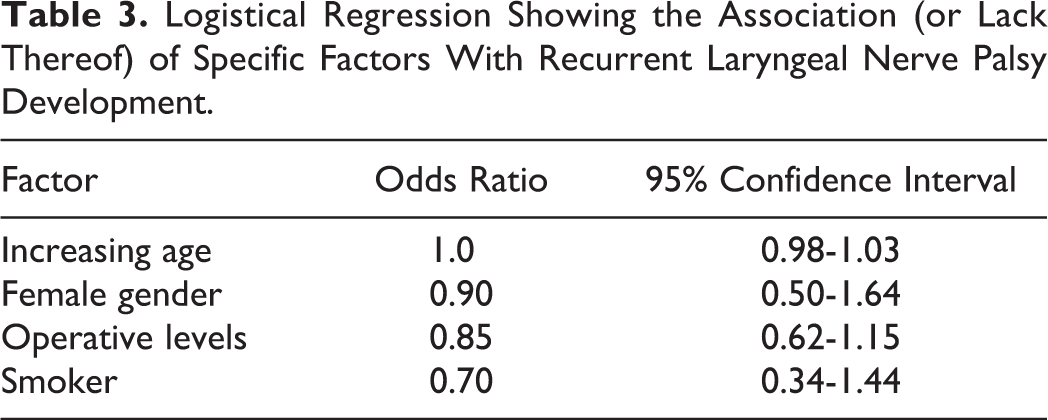
Ten patients (52.6%) required treatment for RLNP—6 required medical therapy (steroids), 1 interventional treatment (injection laryngoplasty), and 3 conservative therapy (speech therapy). Patients who received steroids had vocal cord dysfunction and hoarseness; they all recovered completely. When examining outcomes, 73.7% (14/19) of cases resolved completely, 15.8% (3/19) resolved with residual effects, and in 10.5% (2/19) of cases this could not be determined. A logistical regression was performed to identify potential factors associated with RLNP (Table 3).
Logistical Regression Showing the Association (or Lack Thereof) of Specific Factors With Recurrent Laryngeal Nerve Palsy Development.
Discussion
RLNP is a known complication of anterior exposures to the neck, more commonly utilized in cervical spine surgery and thyroid surgery. While head and neck surgeons are accustomed to exposing the RLN during thyroid surgery, 5,6 spine surgeons do not regularly do so. 3 RLNP may occur secondary to direct injury to the nerve during exposure, traction injury, 7 or nerve entrapment between the inflated cuff of the endotracheal tube and retractor blades. 8,9 The latter mechanism is thought to account for up to 11.2% of cases, 10 suggesting that this injury is not always due to surgical manipulation.
In this multicenter study, we sought to examine the occurrence of symptomatic RLNP after cervical spine surgery, finding an overall incidence of 0.6% to 2.9% across centers. Notably, 94.7% of these cases occurred during anterior-only approaches, and only 1 occurred during a posterior approach. The reported incidence in the literature is highly variable, ranging from 0% to 15.4% in prospective studies and from 0.2% to 7.9% in retrospective studies. 1 However, the largest multicenter study to date utilized the Cervical Spine Research Society database to identify complications in cervical spine surgery from 1989 to 1993, finding a 0.2% rate of RLNP after screening 4,589 patients. 11
Risk Factors
Identified risk factors for postoperative RLNP from both prospective and retrospective studies include: revision procedures, right-sided surgery, level of intervention, multilevel procedures, duration of surgery, type of surgery, and outpatient surgery. 1 Nonetheless, the evidence quality supporting these risk factors is low, and there is only “good” evidence suggesting revision procedures carry an increased risk of RLNP; all other risk factors stem from studies categorized as “moderate” or “poor” evidence studies. 1
As mentioned previously, endotracheal tube intubation may cause direct pressure on the RLN and cause vocal cord paralysis. From an anatomical perspective, it is relevant to know that the anterior branch of the RLN innervates the thyroarytenoid and lateral cricoarytenoid muscles, and that the endotracheal tube may cause nerve ischemia by inducing pressure onto the nerve and submucosal surface. 12 In the present study, 1 case of RLNP developed after a posterior approach, which was most likely due to intubation. In a prospective observational study with the objective of identifying ways to reduce the rate of RLNP, the authors found that reduction of cuff pressure below 20 mm Hg reduced the rate of symptomatic palsy from 2.2% to 0.7% in patients with left-sided approaches. 3
In our study, only a small fraction of patients (15%) were undergoing a revision procedure, and the majority of patients were approached from the left side (79%).
Prevention and Management
Although RLNP may be entirely asymptomatic, in some cases it may lead to microaspiration, coughing, dyspnea, and transient or even permanent hoarseness. 13,14 Apart from reduced cuff pressure as a means to decrease the risk of RLNP, other studies have investigated the role of electromyographic monitoring. Dimopoulos et al 15 utilized laryngeal intraoperative myography in an attempt to predict the development of RLNP after anterior cervical discectomy and fusion in 298 patients. The authors found significant laryngeal activity in 14.4% of patients, of whom 2.3% developed RLNP. The sensitivity of monitoring was calculated at 100%, the specificity at 87%, the positive predictive value at 16%, and the negative predictive value at 97%. Thus, the authors concluded that “laryngeal intraoperative electromyography is a high-sensitivity modality that can provide real-time information and can potentially minimize the risk of operative RLN injury.” 15
Another preventive strategy that has been explored is the use of methylprednisolone, albeit in only one prospective trial. 16 Pedram et al 16 compared the development of vocal cord paralysis in 78 patiens receiving 1 mg/kg of intravenous methylprednisolone immediately after anterior cervical surgery and at 12 and 24 hours versus 236 control patients (no steroids). The authors found a risk of vocal cord paralysis of 2.6% in the steroid group, compared to 3.8% in the control (not statistically significant). 16
Treatment for RLNP includes neurotrophic medications, glucocorticoids, vasodilators, ultrashort wave therapy, voice training, vocal cord injection, reinervation methods, and others. 14 In this study, only 56% of patients required some form of treatment. Six patients required medical therapy (steroids), one interventional treatment (injection laryngoplasty), and three conservative therapy (speech therapy). The rest of the cases only involved mild RNLP and resolved on their own.
Outcomes
As mentioned earlier, most symptoms of RLNP are transient, but in a subset of patients permanent or residual hoarseness may occur. In the present series, 73.7% (14/19) of cases resolved completely, 15.8% (3/19) resolved with residual effects, and in 10.5% (2/19) of cases this could not be determined.
Limitations
The most important limitation of this study is that it relied on a retrospective chart review, rather than a prospective evaluation. Information was collected by research assistants from clinical and operative notes, which carries the risk of information bias. Given that the control group stemmed from the CSM/CSM-I studies, specific variables that were included in the present study such as approach (right vs left) were not recorded in the control group, and were thus not available for analysis. Nevertheless, this is one of the largest studies to date investigating the incidence of rare complications after cervical spine surgery, particularly RLNP.
Conclusion
In this multicenter study examining rare complications following cervical spine surgery, the risk of RLNP was estimated to be between 0.6% and 2.9%. Though rare, it was found that 16% of patients may experience partial resolution with residual effects, and 74% resolve completely.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ziya L. Gokaslan reports grants from AOSpine North America, personal fees from AO Foundation, grants from AOSpine, outside the submitted work; Zachary A. Smith reports grants from AOSpine North America during the conduct of the study; Wellington K. Hsu reports grants from AOSpine North America during the conduct of the study, personal fees from Medtronic, personal fees from Stryker, personal fees from Bacterin, personal fees from Graftys, personal fees from Ceramtec, personal fees from Relievant, personal fees from Bioventus, personal fees from Globus, personal fees from SpineSmith, outside the submitted work; Sheeraz A. Qureshi reports grants from AOSpine North America during the conduct of the study, and is a consultant and receive royalties from Stryker Spine, Biomet Spine, and RTI; Thomas E. Mroz reports other from AOSpine, during the conduct of the study, personal fees from Stryker, personal fees from Ceramtec, other from Pearl Diver, outside the submitted work; Michael Fehlings reports grants from AOSpine North America during the conduct of the study; and K. Daniel Riew reports personal fees from AOSpine International, other from Global Spine Journal, other from Spine Journal, other from Neurosurgery, personal fees from Multiple Entities for defense, plantiff, grants from AOSpine, grants from Cerapedics, grants from Medtronic, personal fees from AOSpine, personal fees from NASS, personal fees from Biomet, personal fees from Medtronic, nonfinancial support from Broadwater, outside the submitted work; Mohamad Bydon reports grants from AOSpine North America during the conduct of the study; Rafael De la Garza-Ramos reports grants from AOSpine North America during the conduct of the study; Samuel K. Cho Dr. Cho reports grants from AOSpine North America during the conduct of the study; grants from OREF, personal fees from Stryker, personal fees from Medtronic, personal fees from DePuy Synthes, outside the submitted work; Evan O. Baird reports grants from AOSpine North America during the conduct of the study; Paul M. Arnold Paul M. Arnold reports grants from AOSpine North America, during the conduct of the study; other from Z-Plasty, other from Medtronic Sofamore Danek, other from Stryker Spine, other from FzioMed, other from AOSpine North America, other from Life Spine, other from Integra Life, other from Spine Wave, other from MIEMS, other from Cerapedics, other from AOSpine North America, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by AOSpine North America Inc., a 501(c) 3 non-profit corporation.