
Abstract
Study Design
Retrospective study.
Objectives
In our recent study, we observed some cases of symptomatic normal vocal cord motility instead of asymptomatic vocal cord palsy (VCP) in preoperative laryngoscopy of a revision anterior cervical spine surgery (ACSS) cohort. We assumed the intrinsic muscle atrophy caused by recurrent laryngeal nerve injury could cause vocal cord-related symptoms. Thus, radiological examinations were reviewed in relation to the posterior cricoarytenoid (PCA) muscle, one of the intrinsic muscles.
Methods
We retrospectively analyzed 64 patients who underwent a revision ACSS. Patients with vocal cord-related symptoms were classified as symptomatic group (group S, n = 11), and those without symptoms as asymptomatic group (group AS, n = 53). The bilateral size and signal intensity of the PCA muscles in these patients were measured in the axial view with preoperative computed tomography (CT) and magnetic resonance imaging (MRI) evaluations. Since the size and signal intensity values were different on each image, the ratios of the contralateral and ipsilateral muscle values were analyzed for each modality.
Results
There was no VCP on laryngoscopy study. However, the mean ratio of the PCA muscle size on CT was 1.40 ± .37 in group S and 1.02 ± .12 in group AS (P = .007). These values on the MRI were 1.49 ± .45 in group S and 1.02 ± .14 in group AS, which was also a significant difference (P = .008).
Conclusions
Evaluating the size of the PCA muscle before revision ACSS may predict a previous recurrent laryngeal nerve injury. Careful planning for the appropriate approach should be undertaken if vocal cord-related symptoms and atrophy of PCA muscle are evident.
Keywords
Introduction
Vocal cord palsy (VCP) is the most notable complication of anterior cervical spine surgery (ACSS) and occurs when recurrent laryngeal nerve or superior laryngeal nerve is injured.1-3 It has been reported in previous studies that revision ACSS may cause a 4.5 times higher rate of nerve injury compared to primary surgery.3-5 Other studies have also reported that asymptomatic VCP arises in 8%–10% of patients who have received a preoperative laryngoscopic screening before revision ACSS.6,7 Therefore, Panello et al 6 recommended that preoperative laryngoscopic examination should be routinely performed to confirm the presence of unilateral VCP before revision ACSS ro reduce the risk of bilateral VCP.
We observed however in our recent study in a preoperative laryngoscopic screening that vocal cord motility was normal in all cases but that 17.2% of these patients had vocal cord-related symptoms. 8 Although the motor function in these patients was found to have recovered during the follow-up period after surgery, we postulated that there might be other causes of their residual symptoms. We speculated therefore that an intrinsic muscle including posterior cricoarytenoid muscle (PCA) atrophy caused by a recurrent laryngeal nerve injury was the underlying cause of these vocal cord-related symptoms. We here retrospectively investigated PCA muscle on preoperative radiologic examinations in an ACSS cohort. The PCA muscle is innervated by recurrent laryngeal nerve and is relatively well-defined on computed tomography (CT) and magnetic resonance imaging (MRI). 9 The purpose of our present investigation was to evaluate the relationship between vocal cord-related symptoms and intrinsic muscle atrophy, and thereby determine the presence of previous recurrent laryngeal nerve injury that may occur during primary operation.
Material and Methods
We retrospectively reviewed the charts of 114 patients who required a revision cervical surgery due to a cervical pathology after the primary procedure, performed by the same cervical spine surgeon (DHL), between March 2009 and June 2019. This study was approved by Asan Medical Center Institutional Review Board, which waived the requirement for patient informed consent because of the retrospective nature of the data analysis (approval No. 20201255). Operative indications were as follows (1) cervical pathology (ASD, pseudoarthrosis, graft failure, etc) after the primary procedure (2) cervical myelopathy patients who progress (3) cervical radiculopathy patients who are not effect even with conservative treatment. The exculsion criteria were as follows: (1) posterior surgery was performed instead of revision anterior cervical surgery (n = 38) (2) follow-up < 1 year (n = 8) (3) If there is no axial cut that can identify the muscle on CT or MRI before revision anterior cervical surgery (n = 4) (4) trauma (n = 3) (5) infection (n = 1).
Data on patients’ demographics (age, sex, and body mass index), initial diagnosis, revision diagnosis, initial procedure, approach direction during the initial and revision operations, time interval between the initial and revision operations, number of previous operations, and initial operation levels were collected and analyzed. A preoperative laryngoscopic screening had been performed in each subject by an ENT specialist using a rigid 70-degree laryngoscopy, and vocal cord motility was found to be normal in all cases in our study population.
The current study patients could be stratified into a preoperative asymptomatic group (group AS) and a group with vocal cord-related symptoms (group S). Vocal cord-related symptoms were defined as voice change or foreign body sensation or intermittent aspiration, all of which were confirmed through the patients’ medical records.
10
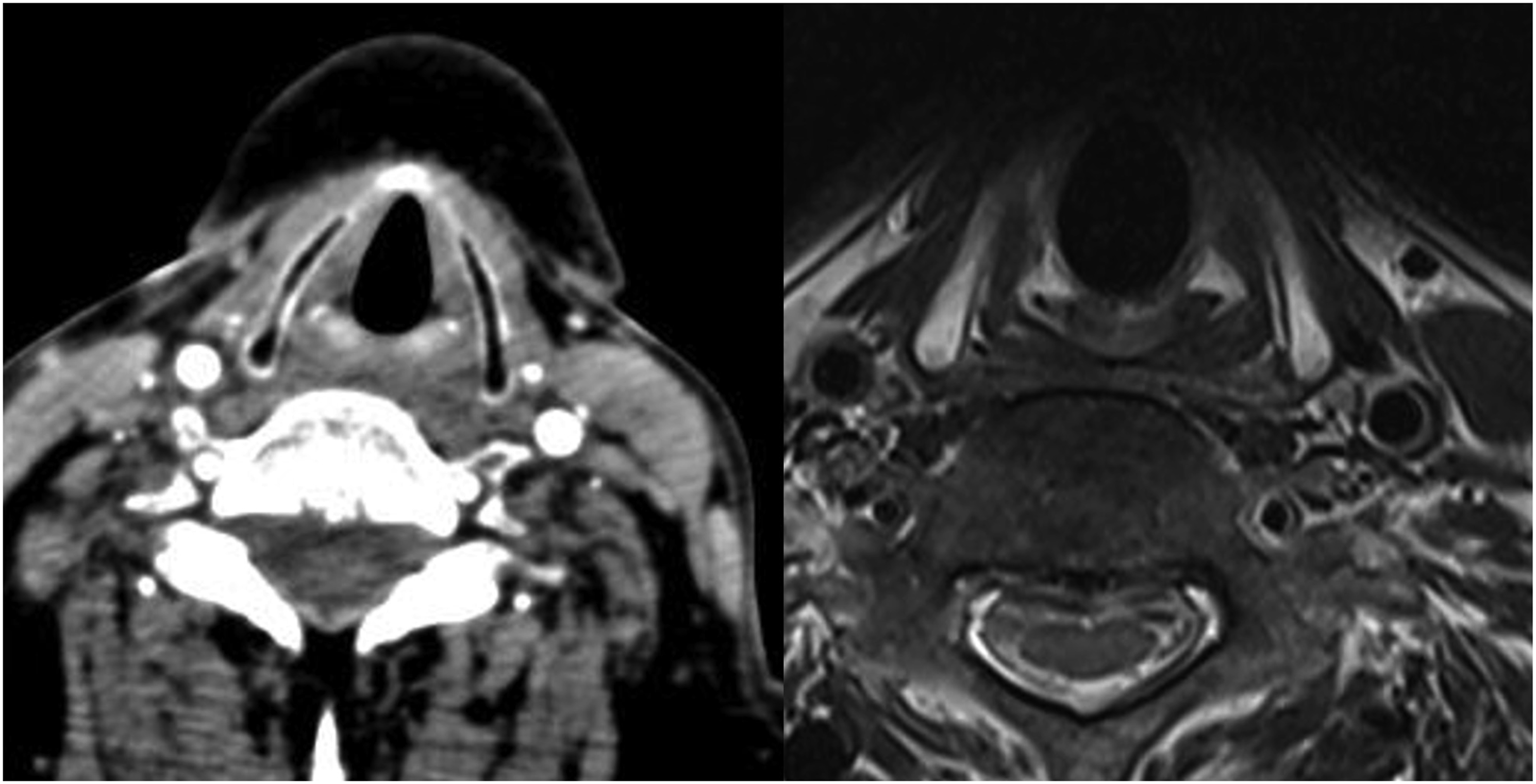
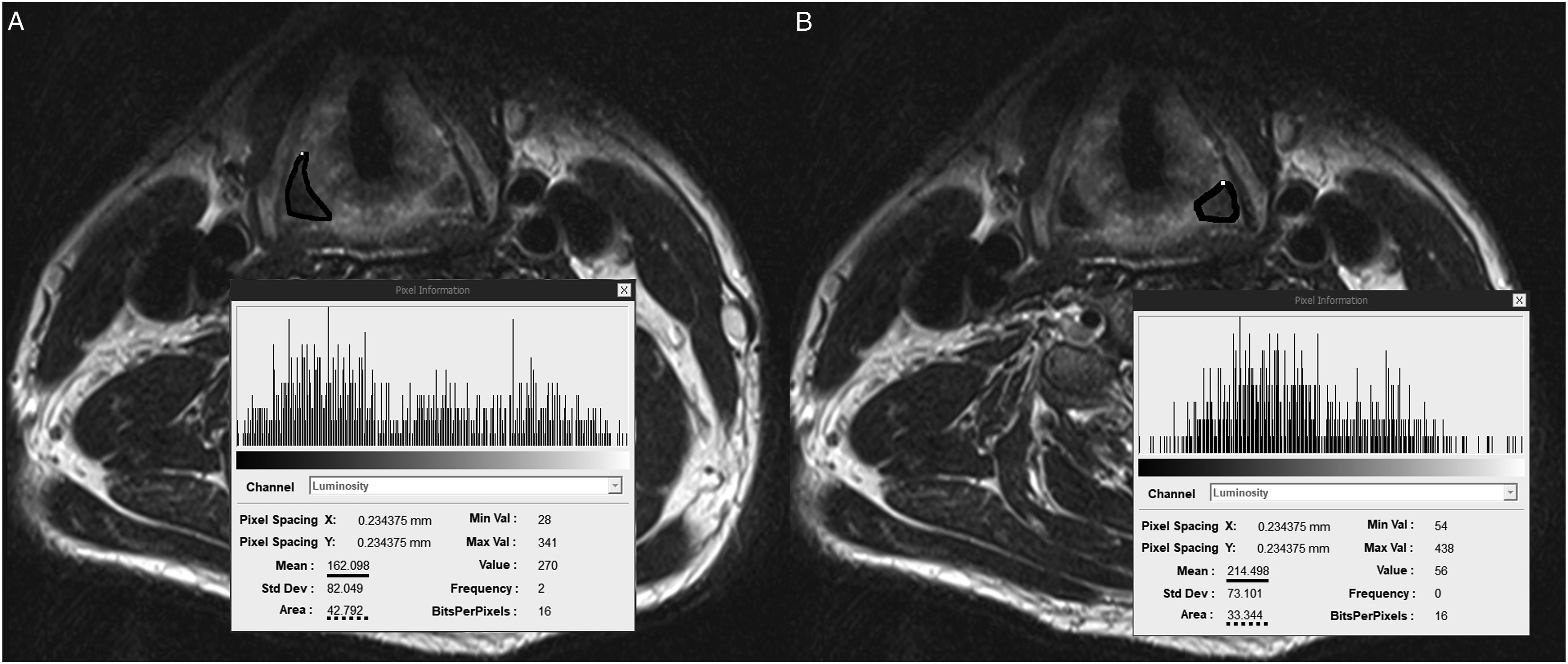
The PCA muscle was evaluated using prior routine 3D vertebral angiography CT and MRI imagery that had been conducted in each patient prior to the revision ACSS (Figures 1, 2). The size and signal intensity of the bilateral PCA muscles detected in the posterior of the thyroid cartilage on CT and MRI axial views were measured using Picture Archiving and Communication System (PACS) (Figure 3). In general, the PCA muscle is well identified at the C5-6 level, and the largest area was measured after finding the PCA muscle in tha axial cut of the corresponding area. All measurements were taken three times and the average values were derived by one person (SYS). Since each value measured on CT and MRI may differ depending on the nature of these imaging modalities, the ratios of the ipsilateral muscle to the contralateral muscle were measured and analyzed in contrast to the previous approach direction in primary operation. Axial illustration of the structure around PCA muscle. Axial CT and MRI scans of the structure around PCA muscle. Representative images of a male patient in group S who underwent a left side approach index anterior cervical spine surgery (he has a voice change symptom without vocal cord palsy) (A) Measuring muscle signal intensity and size of the PCA muscle at the right side. (B) Measuring muscle signal intensity and size of the PCA muscle at the left side. * The solid line means signal intensity and the dotted line means size of the PCA muscle.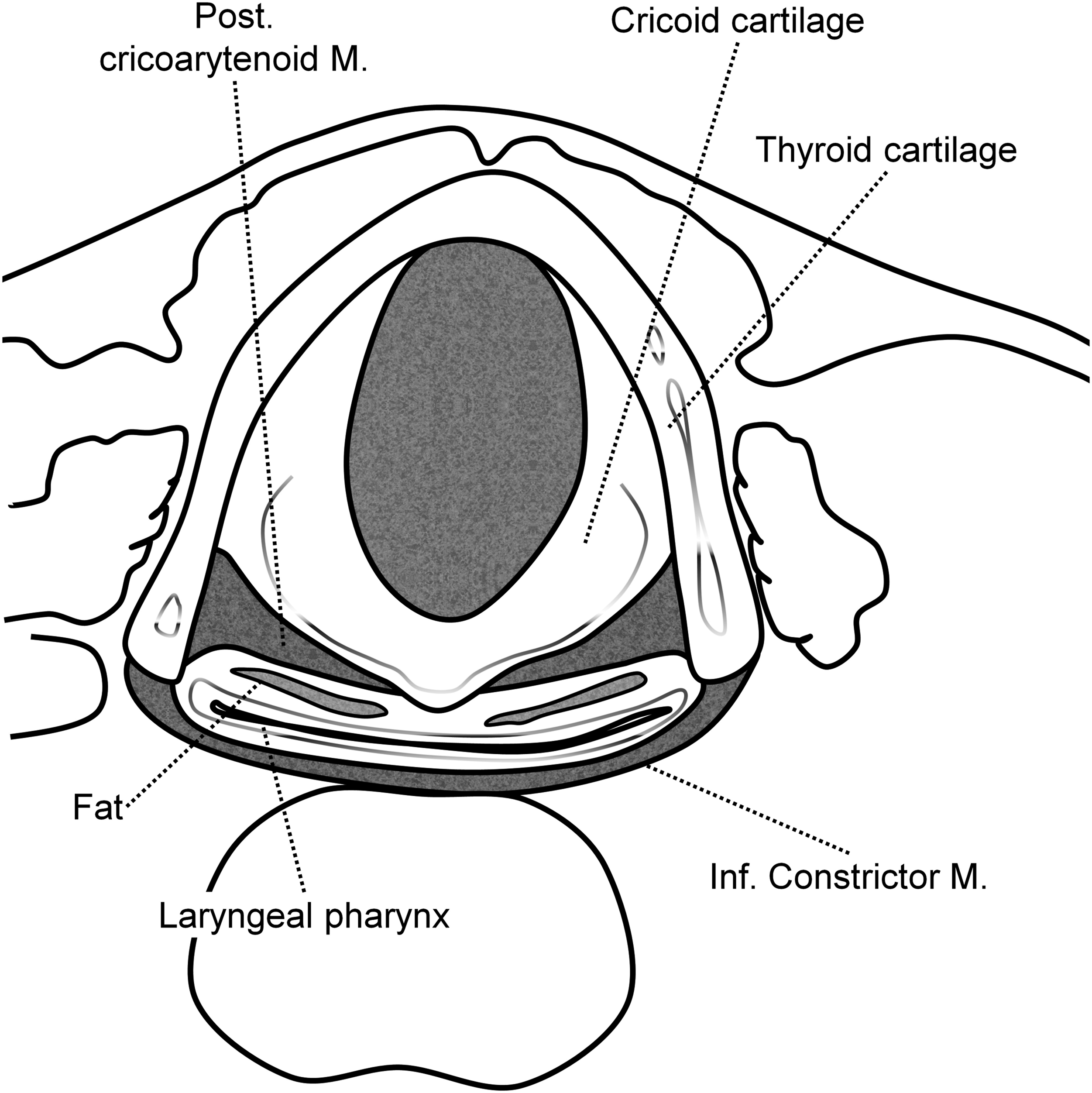
The student t test and Chi-square test were used to compare the differences in each parameter between the study group. All statistical analyses were performed using SPSS Statistics 21.0 (IBM, Armonk, NY, USA). P values <.05 were considered significant.
Results
Demographic and Operative Data for the Study Patients.
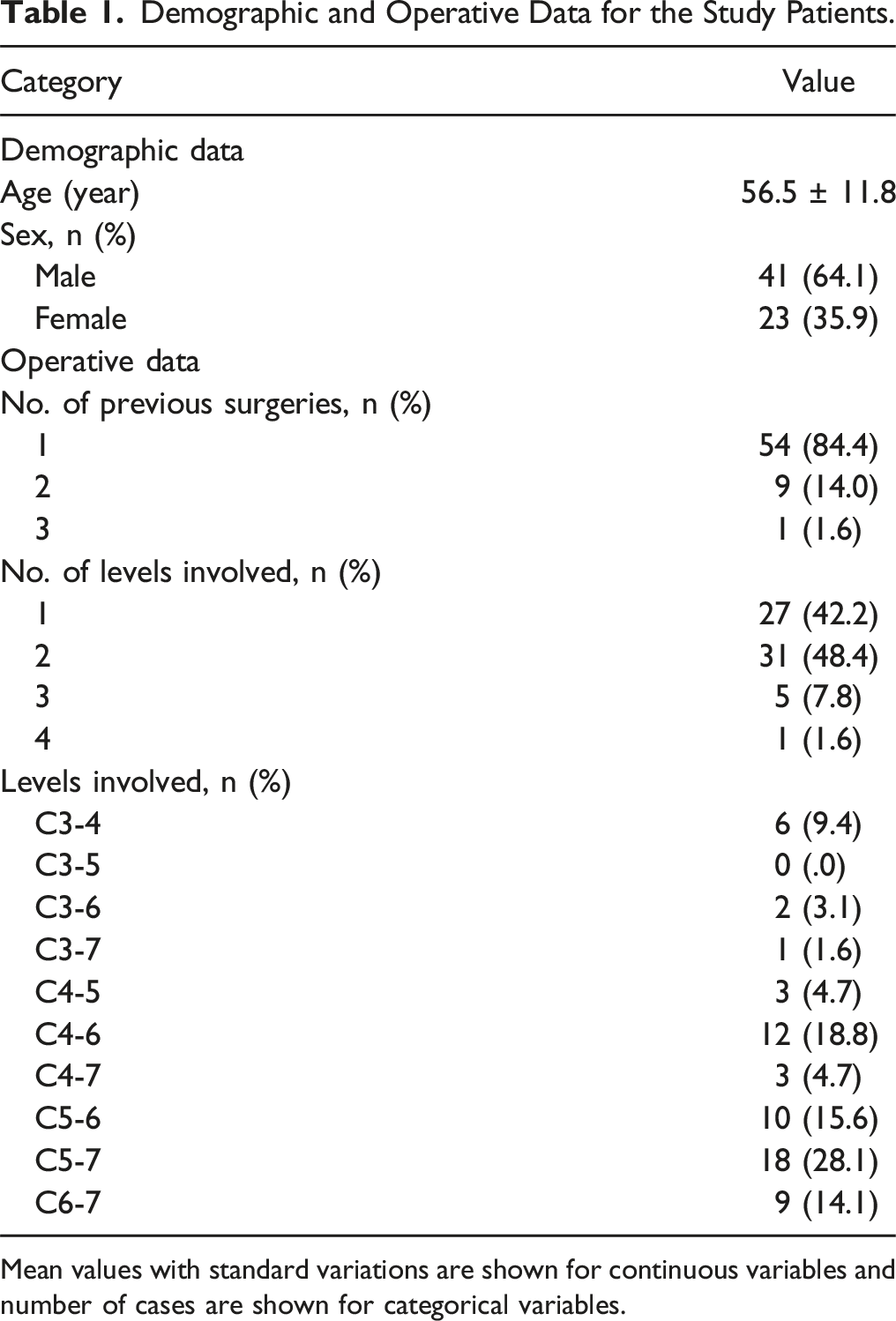
Mean values with standard variations are shown for continuous variables and number of cases are shown for categorical variables.
Comparison of the Demographic and Operative Factors Between the Study Groups.
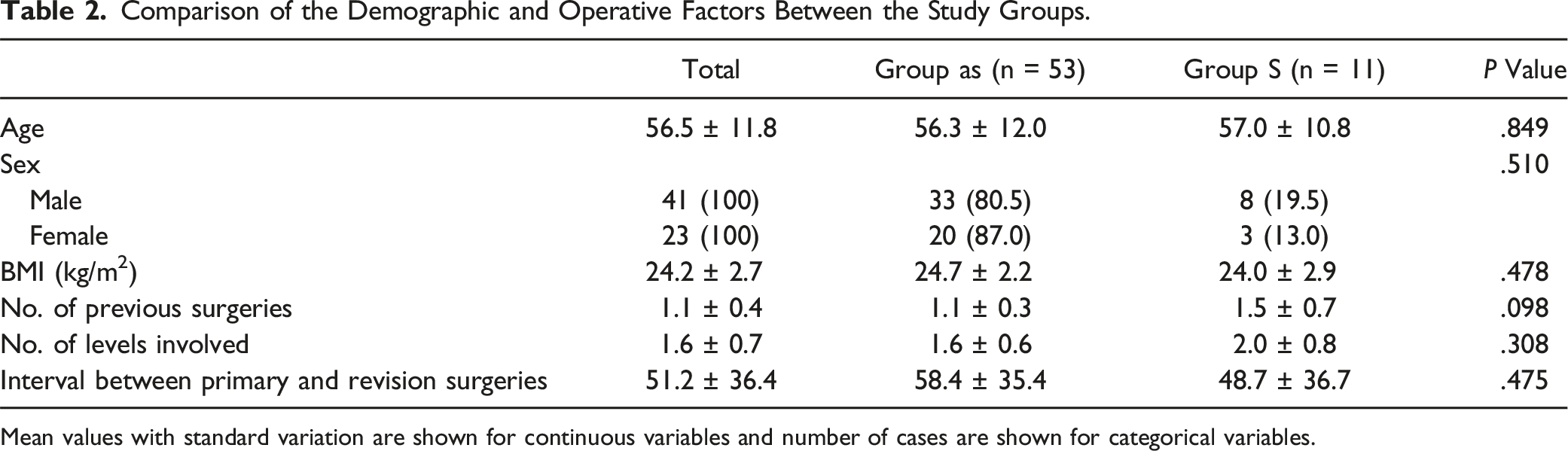
Mean values with standard variation are shown for continuous variables and number of cases are shown for categorical variables.
Comparison of the Radiologic Results Between the Study Groups.
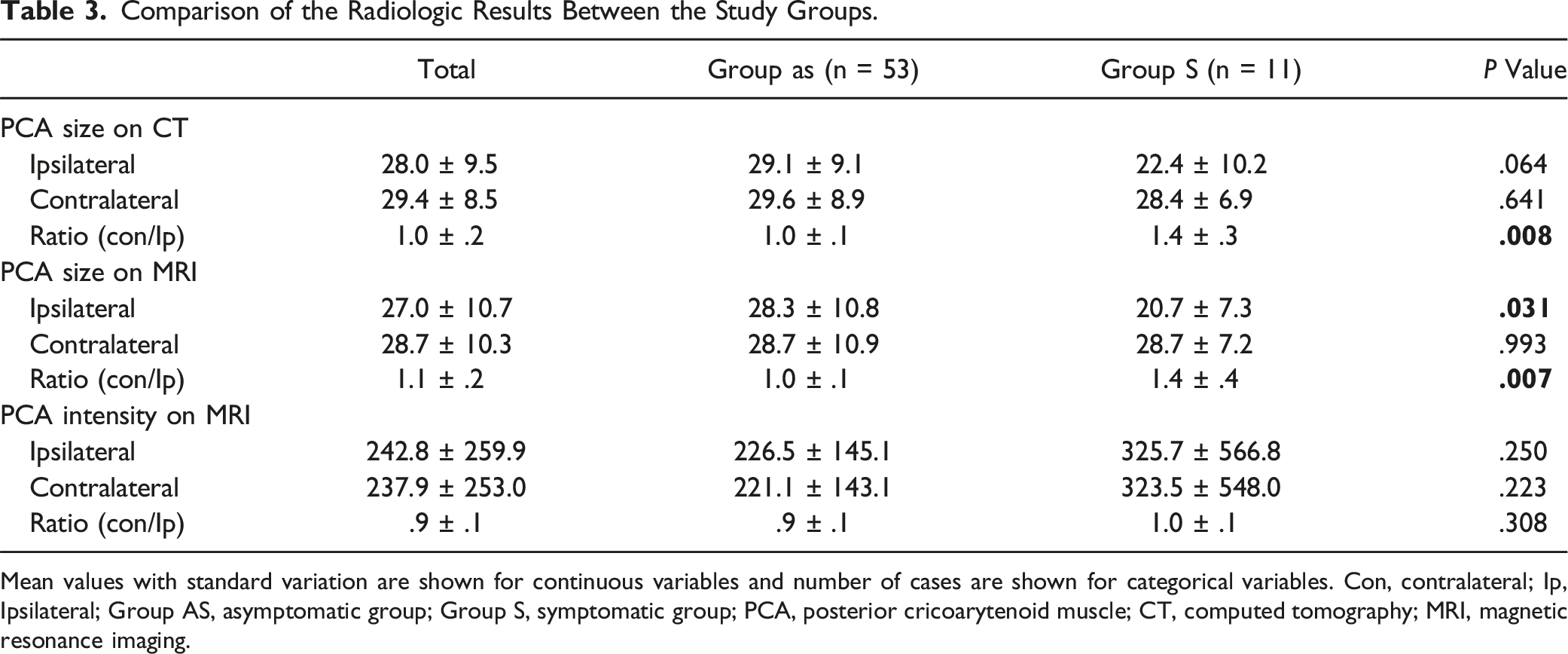
Mean values with standard variation are shown for continuous variables and number of cases are shown for categorical variables. Con, contralateral; Ip, Ipsilateral; Group AS, asymptomatic group; Group S, symptomatic group; PCA, posterior cricoarytenoid muscle; CT, computed tomography; MRI, magnetic resonance imaging.
Discussion
VCP due to a recurrent laryngeal nerve injury is a major complication of ACSS. 1 Previous studies have reported a much higher incidence of VCP following a revision ACSS.3-5 Moreover, the asymptomatic VCP rate had been reported to be 8%–10% in preoperative laryngoscopic screening prior to a revision ACSS.6,7 Manski et al 11 reported that some patients require a permanent tracheostomy for a bilateral VCP after undergoing revision surgery on the opposite side of the unilateral VCP. Panello et al 6 recommended a routine preoperative laryngoscopic examination to confirm the presence of unilateral VCP before revision surgery to reduce the risk of bilateral VCP. Another prior study reported however that there was no decrease in vocal cord motility following the laryngoscopic screening exaination of 64 cases by one of the authors prior to a revision ACSS. 8 Vibratory phase asymmetry was also not observed in that study but some of the enrolled patients who had undergone a primary operation were still having postoperative vocal cord-related symptoms. With regard to that observation, the authors declared that even if vocal cord motility is normal, muscle weakness may remain owing to denervation of the recurrent laryngeal nerve that innervates the vocal cord.
The recurrent laryngeal nerve innervates the intrinsic muscles in the larynx. Among the muscles, the PCA muscle is clinically important because it enables intra-operative monitoring through the placement of electrodes in the post-cricoid region. Dahle et al 12 reported a decrease in EMG amplitude following neuromonitoring of the intra-operative intrinsic muscle upon traction injury of the recurrent laryngeal nerve. Liddy et al 13 described a reliable EMG waveform when monitoring the PCA muscle in accordance with laryngeal nerve stimulation during thyroid surgery.
There have been several reports of nerve recovery by reinnervation after recurrent laryngeal nerve injury. Kupfer et al 14 described a successful innervation of the superior laryngeal nerve after chronic recurrent laryngeal nerve injury in a rat study. Paniello et al 15 reported that the recurrent laryngeal nerve acts on the adductor muscle of the vocal cord, making glottic closure difficult. In addition, the recovery of the adductor muscle strength in that study was found to be related to the severity of the recurrent laryngeal nerve injury.
There have been many reports of muscle atrophy. Wang et al 16 reported that atrophy of the internal laryngeal nerve occurred when the recurrent laryngeal nerve was injured in a rat model. Romo et al 9 concluded that the PCA is an intrinsic muscle innervated by the recurrent laryngeal nerve. They performed CT and MRI analysis in 20 patients with VCP caused by recurrent laryngeal nerve injury, and revealed that 65% of the patients showed different findings on both sides and that this was a significant difference. Our present comparative analysis of symptomatic and asymptomatic cases revealed a significant difference in the PCA muscle size.
MRI evaluations of fatty degeneration caused by muscle atrophy in shoulder lesions have been shown to be important. Goutallier et al17,18 initially proposed a 5-point grading system for evaluating fatty degeneration in disrupted rotator cuff muscles through CT and MRI scanning in two separate studies. Similarly, we thought that it would be helpful to evaluate the signal intensity of muscle in comparison to the normal side at the cervical level on MRI scan. However, the signal intensities did not show any significant difference in this analysis.
A notable limitation of this study is that the number of patients we included was small. Revision ACSS is quite uncommon however and there would not be many cases available from a single institution. Therefore, we conducted the power analysis for our study. We set alpha = .05 and power = .80 as minimum. As a result, the sample size calculation estimated that six patients per group (total 12 patients) would provide 80% power with alpha equal to .05. Additionally, since this study was a retrospective study, three-dimensional studies on muscle size could not be conducted. However, as in Romo’s study, the largest area of the PCA muscle was measured on the axial scan, and an effort was made to reduce the bias as much as possible by using the ratio of both sides. 7 Since this subject has not been well-studied to date, we believe that this study’s findings will be meaningful. It will be helpful to confirm our results in future multi-center prospective investigations.
Conclusion
Although this may be limited information due to small sample size study, surgeons who are aiming to minimize complications, and select the most appropriate approach, when planning a revision ACSS need to be cautious of any differences in the PCA muscle between the two sides evident on a preoperative CT or MRI scan in patients with a vocal cord related-symptom. This evidence might indicate a previous recurrent laryngeal nerve injury.
Footnotes
Acknowledgments
This paper was supported by Eulji University in 2023.
Author’s Note
This study was presented in the International Congress of Korean Society of Spine Surgery (Seoul, May, 2022), 50th Annual Meeting of the Cervical Spine Research Society (San Diego, November, 2022), Spineweek 2023 (Melbourne, May, 2023).
Author Contributions
S.Y.S. Data curation formal analysis, writing-original draft preparation. D.-H.L. Conceptualization writing-reviewing and editing. H.R.L. Data curation. J.H.C. Visualization. C.J.H. Supervision. S.P. Writing-reviewing and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.