
Abstract
Interpretation biases (IBs) play a central role in cognitive models of anxiety disorders and are considered a transdiagnostic feature across anxiety disorders and severity levels. However, the magnitude of this bias in anxiety and modulating factors are largely unknown. In this three-level meta-analysis, we investigated the associations between IBs and symptoms of anxiety. Database searches (PsycINFO, PubMed, ProQuest Dissertations) led to 295 samples with 1,450 contrasts. An overall medium effect size (g = 0.48, 95% confidence interval = [0.43, 0.52]) was found. Equivalent effect sizes were found for youths and adults and different disorder categories and clinical statuses. Effect sizes were larger for studies using direct measures, verbal stimuli, disorder-specific stimuli, and negative (as opposed to positive) stimuli. Overall, results are consistent with the view that anxiety is associated with IBs across different disorders and severity levels. These findings have implications for cognitive theories of anxiety and clinical interventions.
Keywords
Anxiety disorders present a major mental-health burden, with global prevalence estimates ranging from 5% to 10% (Baxter et al., 2013). Contemporary research into the etiology of anxiety disorders has been guided by cognitive-science approaches that implicate higher-order cognitive processes in both symptom development and maintenance (e.g., Clark, 1986; Hirsch & Mathews, 2012; Hofmann, 2007). One higher-order cognitive process that has received much empirical and theoretical support in anxiety disorders is the tendency to consistently interpret ambiguous information in a negative manner—a negative interpretation bias (IB; Hirsch et al., 2016). For example, a person not greeting you example, a person not greeting you back could be interpreted as a sign that the person is angry instead of simply not hearing you. A central assumption of transdiagnostic cognitive models of many anxiety disorders is that IBs have a causal effect on symptoms (e.g., Clark, 1986; Hirsch & Mathews, 2012; Hofmann, 2007). Based on this, treatments have been developed to alter negative IBs in a more benign or positive direction and, in turn, alleviate symptoms of anxiety disorders (e.g., Beck, 1976; Fodor et al., 2020; Woud & Hofmann, 2023).
Theoretical Models of IB in Anxiety Disorders
Cognitive models have been instrumental in explaining the development and maintenance of anxiety, particularly through biases in information processing. Although these models offer a robust framework, they exist alongside other pathways, including, for example, biological, neuronal, or environmental approaches, which can also contribute to understanding the multifactorial nature of anxiety disorders (e.g., Martin et al., 2009; Steimer, 2002). However, because the present meta-analysis is specifically about interpretational processing biases in anxiety, our focus remains on cognitive models of anxiety. In the following section, we describe a basic model of anxiety and a selection of specific models that propose particular mechanisms and conditions through which IBs may lead to symptoms of anxiety (for information on other models of anxiety, see e.g., Mathews & MacLeod, 2005).
The basic cognitive model of anxiety disorders (Beck & Clark, 1997) proposes that a potential threat-relevant stimulus automatically captures a person’s attention. If an initial, relatively automatic interpretation of the stimulus then leads to its perception as threat-relevant, threat-related cognitions are automatically triggered, narrowing one’s focus to one’s negative interpretation of the stimulus. The final processing step comprises a more elaborative (re)evaluation of the stimulus and of whether the person can cope with the anxiety-provoking situation. This, in turn, leads to an exacerbation or reduction of anxiety, depending on whether the situation was evaluated as manageable. The basic cognitive model conceptualizes this information-processing pattern as a normative and nonpathological process that gradually becomes pathological because of, for example, an overgeneralization and overestimation of danger or an exacerbated susceptibility to potentially threatening stimuli.
In addition to this general model, several cognitive models have elaborated on how IBs may contribute to symptom development and maintenance in specific anxiety disorders, emphasizing the role of disorder-specific stimuli in triggering IBs (cf. Beck et al., 1987). To illustrate, the cognitive model of panic disorder (PD; Clark, 1986; Ehlers & Margraf, 1989) postulates that ambiguous bodily responses, such as an increased heartbeat, are interpreted in a catastrophic manner, for example, as a sign of an impending heart attack rather than a harmless bodily reaction. Such biased processing is then hypothesized to increase levels of anxiety, which, in turn, may lead to additional bodily responses, further reinforcing IBs. Consequently, a vicious cycle of anxiety, misinterpretations, and bodily response can be triggered, ultimately resulting in a panic attack and dysfunctional safety behaviors to avoid future attacks. Comparable with Beck and Clark (1997), Ehlers and Margraf (1989) differentiated between a fast and a slow feedback loop, including fast and automatic interpretations that exacerbate anxiety and slower, more reflective interpretations that are hypothesized to down-regulate anxious-mood states.
The cognitive model of social anxiety is another well-established model that focuses on negative interpretations of ambiguous social information (Hofmann, 2007; e.g., a smiling face can be interpreted as a welcoming or smirking facial expression). According to this model, individuals with (high levels of) social anxiety tend to focus excessively on themselves during social situations, monitoring their own behavior and internal states rather than external social cues. In addition, they hold negative self-perceptions and expect others to evaluate them critically, assuming they appear, for example, anxious or incompetent. Consequently, ambiguous social situations are interpreted negatively, reinforcing fears of embarrassment or rejection. To cope, individuals engage in avoidance or safety behaviors, such as avoiding eye contact, which, in turn, maintain their anxiety rather than reducing it. In addition, postevent rumination leads to a distorted recall of social interactions, further strengthening IBs and increasing future anxiety.
Another relevant example is the model of pathological worry, highlighting the role of IBs in the context of generalized anxiety disorder (GAD; Hirsch & Mathews, 2012). According to this model, individuals with (high levels of) pathological worry tend to interpret ambiguous situations in a threatening manner (e.g., potential upcoming financial problems), which reinforces negative expectations about potential future events. As a result, IBs contribute to a cycle of persistent worry in which individuals remain in a hypervigilant cognitive state in which threats are continually perceived and processed as such. Consequently, IBs are strengthened and automatized through learning experiences and unfold throughout a person’s lifetime. Furthermore, the model differentiates between pathological and nonpsychopathological worry by emphasizing the role of cognitive resources, such as attentional control. Specifically, the model proposes that in nonpathological worry, cognitive resources, such as attentional control or positive interpretational processing, help counteract IBs. However, in pathological worry, these resources are overwhelmed by negative information, impairing effective coping strategies.
To conclude, in this overview, we show that cognitive models of anxiety share the assumption that IBs trigger and maintain symptoms of anxiety. However, the conditions under which IBs are activated vary substantially, and among other factors, measurement and sample features may play a crucial role in this context. Accordingly, the present meta-analysis is structured around two central questions examining these features. From a methodological perspective, the theoretical conditions under which IBs are thought to be associated with anxiety (e.g., a competing negative and positive IB is associated with the exacerbation or down-regulation of worry) has led to the development of several measures of IBs aiming to operationalize these conditions (Schoth & Liossi, 2017). This richness in methodological variation has the potential to produce heterogeneity in the estimation of the effect of IBs in anxiety, leading to the first central question of the present work: Under what assessment conditions are IBs observed in anxiety? Next to methodological variation, research on IBs in anxiety shows large variation in the samples that have been investigated to validate cognitive models (e.g., regarding age or the samples’ diagnostic status). Although cognitive models do not specify the particular samples to which they apply, much of the research in this area assumes that IBs are universally relevant and that measures assessing them are broadly applicable. This raises the question of whether the predicted association between IBs and anxiety holds across samples with varying characteristics, such as differences in age or clinical-anxiety status. The second central question of the present work is thus the following: Who shows IBs in the context of anxiety?
Under What Assessment Conditions Are IBs Observed in Anxiety?
Direct versus indirect assessment
IB measures are typically designed based on how IBs are operationalized, for instance, through direct or indirect measures (cf. Everaert et al., 2017). Direct measures ask directly for an individual’s interpretation, for example, by providing potential interpretations of an ambiguous situation that participants rate for their plausibility (e.g., McNally & Foa, 1987) or instructing participants to create sentences by sorting scrambled word sets (Wenzlaff & Bates, 1998). Indirect measures, in contrast, rely on behavioral reactions. In priming paradigms, for example, participants are primed with disorder-related words (e.g., in the context of panic: “palpitation”) and are then instructed to, for example, categorize disorder-related or unrelated target words (e.g., “heart attack” or “flower”) or nonwords (e.g., “krsmp”) as actual words or nonwords (e.g., Feng et al., 2019; Hermans et al., 2010; Zahler et al., 2020). Faster reaction times to disorder-related targets compared with unrelated targets are supposed to be indicative of stronger associative connections between negative information (cf. Fischler, 1977) and in the context of IB research, reflect a stronger negative bias. Although direct measures provide high face validity by explicitly asking participants about their interpretations or to rate predefined interpretations, this strength is accompanied by a significant risk of response biases and demand effects. That is, anxious individuals may choose negative interpretations not only because of a negative IB but also because they believe the researcher expects negative responses and wish to align with that expectation (Everaert et al., 2017). Furthermore, direct measures often rely on hypothetical scenarios in which participants are asked to indicate how they believe they would interpret a given situation. This raises important questions about the accuracy of self-reported introspection because individuals may not always be able to reliably predict their actual interpretations in similar real-life contexts. Indirect measures have been developed to mitigate these limitations; however, their psychometric properties, particularly their validity in assessing IBs and their internal consistency, remain subjects of ongoing debate (Würtz & Sanchez-Lopez, 2023). Nevertheless, both direct and indirect measures contribute unique insights into the role of IBs in anxiety. Consequently, a central moderator investigated in the present meta-analysis is whether IBs were assessed with either an indirect- or direct-assessment method. This would help identify which tasks are potentially better in capturing IBs linked to anxiety, 1 thereby informing evaluations of the potential biases introduced by the choice of measurement method.
Matched versus unmatched stimuli
Although cognitive models of anxiety disorders share the assumption that IBs are central to the development and maintenance of symptoms, they often emphasize the role of disorder-specific stimuli as the primary trigger for IBs. This assumption has been summarized as the “content-specificity hypothesis” (cf. Beck et al., 1987; Klein et al., 2019). For instance, catastrophic misinterpretations of bodily responses are the key trigger in PD (e.g., Clark, 1986), negative interpretations of ambiguous social situations are central in the context of social anxiety (e.g., Hofmann, 2007), and catastrophizing interpretations of a topic of current concern are highlighted in generalized anxiety (e.g., Hirsch & Mathews, 2012). The examination of content specificity is typically operationalized by assessing the relationship between symptoms of a specific disorder and IBs measured using disorder-specific stimuli and then comparing this relationship with biases measured with disorder-unspecific stimuli (cf. Stuijfzand et al., 2018; Subar et al., 2022). The primary distinction between different anxiety disorders lies in the specific object or situation that triggers anxiety, making content specificity a key factor in differential diagnosis. For example, if someone becomes anxious and panicky when entering a crowded bar, the classification depends on what type of cognition triggered the anxiety. If the central concern is being judged by others, the anxiety would be classified as social anxiety, whereas the concern of not being able to leave the room in case of a panic attack would be indicative of agoraphobia. Given the importance of content specificity in the differential diagnosis of anxiety disorders, using stimuli that either aligned or did not align with the primary concern of a specific anxiety disorder was tested as a moderator. Examining this moderator may offer insights into the validity of content specificity as a core factor in anxiety.
Verbal versus nonverbal stimuli
IBs can be operationalized using verbal stimuli, for instance, written descriptions of ambiguous scenarios that participants are asked to interpret (McNally & Foa, 1987). Although these measures have made invaluable contributions to the understanding of IBs in anxiety, their external validity might be limited. For example, participants only read about feared situations and have to rely on their imagination to place them and predict their reactions. Furthermore, as highlighted in the section comparing direct assessments versus indirect assessments, individual differences in accuracy of self-reported introspection may be a limiting factor. To overcome these limitations and facilitate engagement in the presented (ambiguous) situation, pictorial or video-based stimuli have been used, for example, by showing participants ambiguous, anxiety-related situations (In-Albon et al., 2008) or ambiguous facial expressions (Maoz et al., 2016). However, although such stimuli offer greater ecological validity, their drawback is their increased complexity (cf. Chen et al., 2020). To illustrate, although verbal stimuli can deliver information in a relatively standardized manner, an ambiguous face, for example, has several additional features likely influencing interpretational processes, that is, features that are difficult to control (e.g., attractiveness, symmetry). Because both types of stimuli offer advantages in either internal or external validity, testing whether stimulus type moderates effect sizes could help determine whether IBs are detectable only when using highly controlled stimuli or also emerge when using stimuli that more closely resemble real-life experiences.
Absolute Versus Relative Assessment
Although cognitive models of anxiety disorders typically focus on negatively biased interpretations (e.g., Clark, 1986), some models suggest that positive versus negative interpretations may serve distinct functions. For instance, in the context of GAD, Hirsch and Mathews (2012) proposed that positive and negative interpretations compete for cognitive resources. As a result, the balance between these interpretations plays a crucial role in determining whether an individual becomes engaged in a cycle of worry (for similar considerations in the context of panic, see Ehlers & Margraf, 1989). Furthermore, there is emerging evidence that positive and negative IBs play partially independent roles in the development and maintenance of symptoms, and each contribute uniquely to the variance in anxiety-disorder symptoms (Huppert et al., 2003; Steinman et al., 2020). Such theoretical considerations and empirical findings also affect how IBs are assessed and indexed. On the one hand, IBs can be assessed in a relative way, in which the tendency to engage in positive interpretations is measured against the tendency to engage in negative interpretations, yielding a combined score. For example, a measure requiring participants to evaluate the plausibility of both positive and negative interpretations of an ambiguous scenario would be considered a relative assessment. This approach allows for comparisons of whether a participant finds negative interpretations more plausible than positive ones or vice versa. On the other hand, IBs can be assessed in an absolute way, in which the tendency to engage in positive versus negative interpretations would be assessed independently, generating separate positivity and negativity scores without directly comparing them with each other. In the present meta-analysis, these different conceptualizations motivated the question of whether the relative assessment or absolute assessment of IBs shows stronger associations with symptoms. Thus, the conceptualization of IBs, whether assessed as relative, absolute positive, or absolute negative, was examined as a moderator of the relationship between IBs and anxiety.
Categorical Versus Dimensional Studies
To allow a comprehensive investigation of IBs in anxiety, studies with different designs need to be included. The most notable design difference is the choice of either a categorical investigation of anxiety and IBs (i.e., difference between different levels of anxiety, e.g., clinical or nonclinical) or a dimensional investigation in which the association (e.g., correlation) between continuous measures of anxiety and IBs is assessed. To evaluate the validity of aggregating findings across different study designs, the study design, that is, categorical or dimensional, was considered as a moderator, following standard practices in meta-analytical research (e.g., Chen et al., 2020; Everaert et al., 2017).
Who Shows IBs in the Context of Anxiety?
Adults versus youths
Many anxiety disorders have their onset several years before adulthood (Solmi et al., 2022). There is growing evidence that children and adolescents show an association between IBs and symptoms of anxiety (Stuijfzand et al., 2018) and that the strength of this association is comparable with the associative strength observed in adult populations (Chen et al., 2020). Although cognitive models of anxiety postulate that negative IBs develop in early childhood (e.g., Beck & Clark, 1997), research on IBs has predominantly focused on adult samples (cf. Songco et al., 2020), questioning the generalizability of these results in younger samples. Results of the meta-analysis by Stuijfzand et al. (2018) provide critical insight into this issue. Their results indicate that even within a relatively narrow age range (i.e., a maximum age of 21 years and a mean age below 18 years), age was a significant predictor of the IB-anxiety association. Specifically, as age increased, the association between negative IBs and anxiety levels in children and adolescents also strengthened. If such an effect is evident in a relatively homogeneous sample, it raises the question of how much stronger this relationship is in a sample spanning childhood, adolescence, and adulthood. Therefore, participants’ age group, that is, youths versus adults, was included as a moderator in examining the relationship between IBs and anxiety.
Disorder categories
Given the central role of IBs in various anxiety disorders, the first-line recommendation in terms of treatment is cognitive-behavioral therapy (CBT). CBT aims to identify patients’ negative interpretations and catastrophizing assumptions and challenge them through behavioral experiments. However, the emphasis on identifying and addressing negative IBs varies significantly across treatments for different disorders. For example, although challenging IBs is a core element in the treatment of social anxiety, it plays a more secondary role in the treatment of specific phobias (e.g., Bandelow et al., 2022; Wolitzky-Taylor et al., 2008). The varying emphasis on IBs across treatments for different anxiety disorders raises the question of whether this is reflected in the strength of the association between IBs and symptoms across disorders. To explore this, effect sizes of IBs in anxiety were compared across different anxiety-disorder categories.
Clinical status
From a diagnostic perspective, categorizing individuals as either “clinical” or “nonclinical” is essential for determining whether treatment is warranted (cf. Bandelow et al., 2022). However, research suggests that this strict distinction may not fully capture the complexity of psychopathology because mechanisms such as IBs exist along a continuum of symptom severity. Instead, it has been suggested that mental disorders should be viewed dimensionally such that subclinical symptoms differ from clinical symptoms in intensity and the level of distress they cause rather than in their underlying mechanisms (Haslam et al., 2012, 2020; Ruscio, 2010). This perspective is supported by cognitive models of anxiety that describe anxious interpretations and their relationship with symptoms as a normal process (e.g., Beck & Clark, 1997). This relationship is considered pathological only when it leads to significant impairment or distress for the individual. Although this perspective implies that the strength of the association between IBs and anxiety symptoms may be similar across clinical and subclinical samples, some research has questioned whether cognitive mechanisms truly function the same way in clinical and subclinical anxiety (e.g., Loscalzo et al., 2018). Investigating whether IBs exhibit similar associations with symptoms of anxiety in both subclinical and clinical anxiety could provide insight into the generalizability of findings from subclinical populations and their relevance as a model for clinical research. Consequently, the sample status, that is, whether the sample was diagnosed with an anxiety disorder or subclinical symptoms of anxiety were investigated, was used as a moderator. 2
Control-group status
IBs are transdiagnostic (risk) factors and thus characterize multiple mental disorders, for instance, depression (Everaert et al., 2017); disorders from the obsessive-compulsive spectrum, such as health anxiety (Du et al., 2023); or eating disorders (e.g., Korn et al., 2020). Several studies investigating the presence of (anxiety disorder specific) IBs compared anxious samples with nonanxious clinical samples in addition to healthy control subjects (e.g., Hermans et al., 2010). Because of the relevance of IBs in other mental disorders, however, the inclusion of effect sizes from these comparisons might underestimate the strength of the associations between IBs and anxiety. Consequently, the status of the control group (healthy/low-anxiety control group vs. nonanxious clinical control group) was tested as a moderator.
Comorbid depression
There is substantial evidence with large effect sizes supporting the association between IBs and (levels of) depression (Everaert et al., 2017). In addition, anxiety disorders and depression frequently co-occur, and there are high rates of comorbidity between the two (e.g., Johansson et al., 2013). Accordingly, it is important to examine whether the observed association between IBs and anxiety symptoms is partially or fully attributable to comorbid depressive symptoms or symptoms of anxiety are uniquely associated with IBs. Accordingly, in this meta-analysis, we compared studies that excluded participants with comorbid depressive symptoms with those that included individuals with clinical or above-threshold depressive symptoms and studies that did not assess depressive symptoms. This, in turn, could guide future research on IBs in anxiety by determining whether excluding participants with comorbid depressive symptoms is necessary to enhance the validity of the findings.
Comorbid anxiety disorders
Specific anxiety disorders are thought to be associated with content-specific negative IBs (cf. Beck et al., 1987). Consequently, each specific anxiety disorder should be linked to negative IBs for a distinct set of stimuli while showing weaker associations with more general negative IBs. In contrast, the presence of multiple comorbid anxiety disorders may extend a negative IB toward multiple sets of stimuli, thereby strengthening the association between the IB and symptoms. Because comorbidity between different anxiety disorders is common (e.g., Goldstein-Piekarski et al., 2016), the presence of at least one comorbid anxiety disorder was examined as a moderator to determine whether multiple anxiety disorders have an additive effect on the association between IBs and symptoms. This analysis could guide future research on the relationship between IBs and symptoms of specific anxiety disorders and help to determine whether comorbid anxiety disorders should be excluded to obtain a more precise estimation of effect sizes.
Aims of the present meta-analysis
Several meta-analyses have examined the relationship between disorder-specific IBs and anxiety symptoms (e.g., Chen et al., 2020; Ohst & Tuschen-Caffier, 2018). For example, Chen et al. (2020) found a strong association between social anxiety and IBs across 44 studies in which effect sizes remained consistent across clinical and subclinical samples. Significant moderators were, for example, the use of reaction-time-based measures and stimulus type. The meta-analysis by Ohst and Tuschen-Caffier (2018) included seven studies and quantified how strongly patients diagnosed with PD misinterpreted bodily sensations or panic-unrelated, external events as catastrophic compared with healthy control participants and patients with other anxiety disorders. Analyses revealed medium to large effects for the catastrophic misinterpretation of bodily sensations both between patients with PD and healthy control participants and between patients with PD and patients with other anxiety disorders. In contrast, for the catastrophic misinterpretation of external events, the effects were medium to large when comparing patients with PD with healthy control participants but showed a small negative effect when comparing them with patients with other anxiety disorders. Taking a broader perspective, Stuijfzand et al. (2018) analyzed 77 studies on IBs in childhood anxiety and found a moderate effect size, which increased with age. Note that effect sizes were larger when disorder-specific stimuli were used. This result was partly replicated by Subar et al. (2022), who summarized the results of 19 studies. Their analyses revealed a small correlation between symptoms of anxiety and measures of IBs when stimuli were matched to the anxiety disorder. However, the effect size was nonsignificant when stimuli were not matched
Although prior meta-analyses have clearly advanced understanding of IBs in anxiety, they have primarily focused on specific disorders, samples, or limited sets of moderators. If key moderators, such as stimulus matching or measurement type, are crucial, their moderating role should be observable across different anxiety disorders. To address these open questions, in the present meta-analysis, we take a significant step forward and provide a comprehensive estimate of the IB-anxiety association across different disorders using a very broad set of moderators. By systematically and directly comparing methodological and sample-related moderators, in the present meta-analysis, we aim to determine whether IBs are a universal feature of anxiety. Accordingly, the findings will enhance understanding of the theoretical mechanisms underlying IBs in anxiety, offering deeper insights into whether IBs are a transdiagnostic feature of anxiety disorders and identifying potential boundary conditions.
Method
Transparency and openness
The present meta-analysis was conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines (Rethlefsen et al., 2021) and preregistered on PROSPERO (CRD42021287986) before the start of the literature search (for the PRISMA checklist, see Table S1 in the Supplemental Material available online). However, during the literature-search process, an amendment to the protocol was submitted that excluded the planned literature search on PsyArXiv. This was done because of a missing filter for studies that were already published elsewhere by the time of the search, which made it difficult to identify and exclude duplicates. Other deviations from the preregistration are noted (in notes) in the relevant sections of the article. All materials, including the coding scheme, the analysis script, and the extracted data, are openly available on OSF (https://osf.io/cmg5x/).
Literature search and study selection
Relevant literature was initially searched in November 2021, and then an updated search was run on February 29, 2024, both times using the databases APA PsycINFO accessed through EBSCOhost, PubMed, and ProQuest Dissertations. In a first step, the following search string was used: (anxi* OR GAD OR worr* OR agoraphob* OR panic OR specific phob* OR social anxie* OR phobi* OR mutism OR fear) AND ((interpret* OR apprais* OR schema* OR process* OR cognitive OR affective) AND bias*). In a second step, commonly used measures of IBs were entered into the search string, and an additional search was conducted using the resulting string: (scrambled sentence* task OR homophone task OR homograph task OR ambiguous face identification task OR recognition test OR lexical decision task OR interpretation bias questionnaire* OR word-sentence association* OR ambiguous story and sentence completion tasks OR grammar decision task OR reading time task OR semantic priming task) AND (anxi* OR GAD OR worr* OR agoraphob* OR panic OR specific phob* OR social anxie* OR phobi* OR mutism OR fear) AND ((interpret* OR apprais* OR schema* OR process* OR cognitive OR affective) AND bias*). In addition, an email was sent via mailing lists of the German Psychological Society (Deutsche Gesellschaft für Psychologie) to identify unpublished data. In a final step, lists of included studies of relevant other meta-analyses were scanned for potentially eligible studies (Chen et al., 2020; Gonsalves et al., 2019; Ohst & Tuschen-Caffier, 2018; Stuijfzand et al., 2018; Subar et al., 2022; Würtz et al., 2022). 3
For resulting articles, in the initial search, titles and abstracts were independently scanned for eligibility by two authors (F. Würtz and M. Kunna), followed by a full-text scan of articles identified as potentially eligible in the first stage, conducted by the same two authors. All data were extracted independently by two authors: F. Würtz extracted all data, and M. Kunna and C. Lindgraf independently extracted data from half of the full texts. In the updated search, the data screening and data extraction were completed independently by E. Abado and Y. Amanvermez. Overall, agreement between authors was substantial, with κ = .73 for titles and abstracts and κ = .80 for full-text eligibility. After data extraction, authors of studies who provided insufficient data for inclusion in the meta-analysis were contacted twice via email, initially with a 1-month deadline, followed by a second request with a 2-week deadline. If the required data were not provided within the second deadline, the article was excluded. For an overview of the study-selection process, see the PRISMA flow diagram in Figure 1.
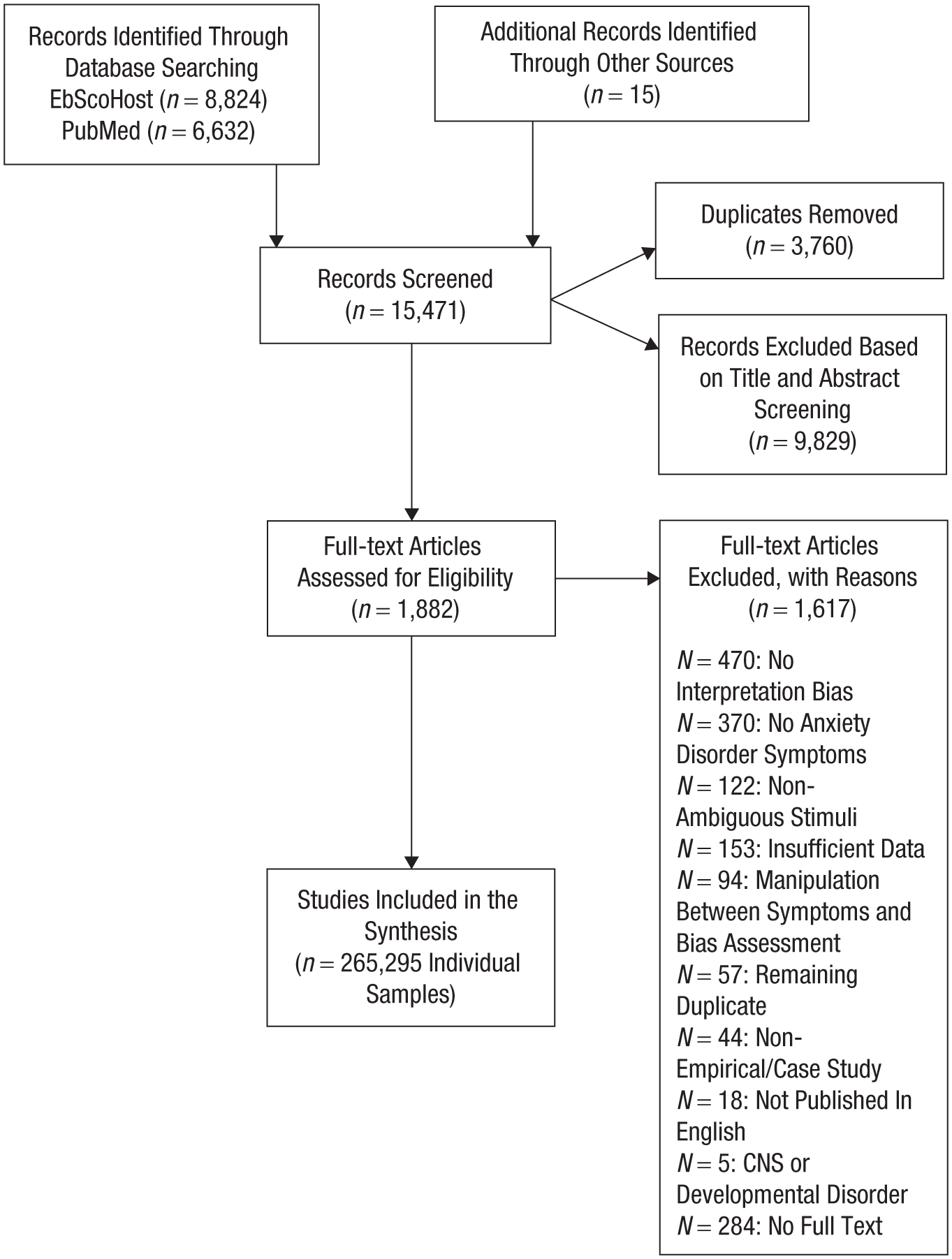
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram.
Study eligibility
The following inclusion criteria were applied: (a) The study assessed symptoms of an anxiety disorder listed in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), or included at least one sample of diagnosed patients, or included an at-risk sample for the development of an anxiety disorder (e.g., children of parents with an anxiety disorder), or assessed unspecific symptoms of anxiety (e.g., assessed via the anxiety subscale of the Depression, Anxiety, and Stress Scale [DASS]; Lovibond & Lovibond, 1995). (b) The study assessed IBs and symptoms of anxiety cross-sectionally (i.e., within the same survey or the same laboratory experiment).
The following exclusion criteria were applied: (a) Studies were excluded if a diagnosed sample was tested but the sample’s primary diagnosis was not an anxiety disorder. Samples with comorbid depressive disorders were excluded only if the focus of the study was on depression and not on the association between IBs and anxiety. (b) The primary symptom assessment was not part of the DSM-5 anxiety disorders (e.g., a study included anxiety-relevant questionnaires but was investigating IBs in relation to eating disorders). If no disorder of primary interest was specified, the study was included (e.g., only nonspecific symptoms of anxiety were assessed, yet the study still focused on anxiety). (c) Studies with samples consisting of participants with central nervous system disorders or diseases (e.g., Parkinson’s disease), learning disorders, or developmental disorders were excluded. (d) Studies applying a manipulation (e.g., stress induction, experimental manipulation of interpretational processing, or treatment) before or between the assessment of the relationship between IBs and anxiety were excluded. However, in case a study applied a baseline assessment testing the associations before the manipulation, the data of this assessment time point were included. (e) Studies using the State-Trait Anxiety Inventory (STAI-T; Spielberger et al., 1983) as a sole indicator of participants’ anxiety were excluded because of recent findings suggesting that the STAI-T primarily measures negative affectivity and is more strongly associated with depression than with anxiety (Knowles & Olatunji, 2020). 4 (g) Studies not published in English, case studies and case series, and nonempirical and nonquantitative studies were excluded.
Data coding
The independent raters extracted data from individual studies based on a structured coding scheme. 5 The following study characteristics were extracted: authors, publication year, journal, publication status (peer reviewed vs. not peer reviewed), sample size, gender distribution (% female), mean age, age group (< 18 years [youths] vs. ≥ 18 years [adults]), anxiety-group status (clinical, analog [unselected samples], remitted, at risk), control-group status (nonanxious clinical, low anxiety, healthy control group), study design (categorical vs. dimensional), and exclusion of participants with a (comorbid) depressive disorder (yes vs. no). Regarding the IBs, the following characteristics were extracted: IB conceptualization (absolute vs. relative), IB valence (positive vs. negative), IB operationalization (direct vs. indirect), disorder-specific stimulus matching (matched vs. unmatched stimuli), and stimulus type (verbal vs. pictorial). For the anxiety measures, the following information was extracted: specified anxiety disorder (social anxiety, separation anxiety, generalized anxiety, PD [including anxiety sensitivity], specific phobias, multiple anxiety disorders [e.g., total score of questionnaires assessing multiple symptom categories], unspecific symptoms [e.g., DASS-anxiety]), presence of comorbid anxiety disorder[s] [yes vs. no], anxiety-disorder assessment [clinical interview, self-report, chart diagnosis]). For aggregated information summarizing the extracted data, see Table S2 in the Supplemental Material.
Statistical approach
Before aggregation, all effect sizes were converted to Hedges’s g, providing an unbiased population estimate of the standardized mean difference (Hedges, 1981). Effect sizes for positive IB scores (the higher the score, the more positive the interpretation) were inverted to allow aggregation with negative IB scores. Consequently, effect sizes describe the association between a stronger negative IB and symptoms of anxiety. Effect sizes for individual categorical studies (comparing an anxious sample with a nonanxious sample) were primarily calculated using the extracted means and standard deviations using the escalc function of the metafor package (Viechtbauer, 2010), that is, by dividing the mean difference of the two groups by the pooled standard deviation. If means and standard deviations were not available, effect sizes were calculated based on other available information, such as t statistics and degrees of freedom, one-way F statistics, means and standard errors, or the reported Cohen’s d effect sizes. Correlation coefficients extracted from dimensional studies were converted to Hedge’s g using the conv_delta function of the metafor package (Viechtbauer, 2010).
Meta-analytical aggregation was done using three-level random-effect models calculated via the rma.mv function of the metafor package with restricted maximum likelihood estimation. The three-level structure allows for the inclusion of multiple effect sizes of individual studies while accounting for the resulting nested variance structure (Van Den Noortgate et al., 2015). Specifically, the resulting heterogeneity in effect sizes can be then attributed to three sources, that is, between-study variance (Level 3), within-study variance (Level 2), and random sampling (Level 1). Log-likelihood tests were applied to test whether individual variance components made significant contributions to the model fit by comparing the full model including all variance components with individual models excluding either the Level 2 or Level 3 variance component. Confidence intervals and p values with cluster-robust standard errors for effect sizes were calculated using the clubSandwich package (Pustejovsky, 2023) to account for the dependency between effect sizes extracted from the same studies. In addition to the 95% confidence interval (CI), which presents the boundaries that contain the true population effect size with a probability of 95%, 95% prediction intervals (PIs) were calculated, containing the effect size that would be found in a specific future study with a probability of 95%. After fitting the first random-effects model, the data were scanned for potential outliers with standardized residuals >|3|, which were then excluded in a next step to avoid biases in effect-size estimates through single influential studies. Remaining heterogeneity in effect sizes was investigated through preregistered moderation analyses (for deviations regarding the selection of moderators, see Note 5). Because testing multiple moderators can increase the probability of Type I errors, we applied the Benjamini-Hochberg (BH) procedure to control the false-discovery rate and adjust significance levels in this meta-analysis (Benjamini & Hochberg, 1995).
Risk of bias
The risk of bias for individual studies was assessed using the adapted checklist by Downs and Black (1998) as outlined by Everaert et al. (2022). The applied scale consisted of 21 items assessing the risk of bias introduced via potential flaws in reporting, lack of external and internal validity, and study power. Each of the 21 criteria was rated on a 2-point scale (1 = no potential threat to validity, 0 = potential threat to validity, 0 = unable to determine) except for one item assessing the reporting of potential confounding variables, which was rated on a 3-point scale (1 = potential confounders reported, 0.5 = partial reporting of potential confounders, 0 = no reporting of potential confounders, 0 = unable to determine). For a similar scoring procedure, see Everaert et al. For the mean ratings per category across all studies, see Table S3 in the Supplemental Material; for individual ratings, see Table S4 in the Supplemental Material.
Risk of bias across studies was investigated in several ways. First, a funnel plot was generated and tested for asymmetry using Egger’s test to investigate whether results were potentially subject to small-sample bias (Egger et al., 1997). A funnel plot presents the effect sizes of studies in relation to their respective standard error, that is, the precision of their estimate, and thus, studies with smaller samples are attributed lower precision compared with studies with larger samples. Next, sensitivity analyses according to Mathur and VanderWeele (2020) were conducted (Braginsky et al., 2023). 6 Specifically, a “worst-case meta-analysis” was conducted including only nonaffirmative studies (i.e., studies with a nonsignificant relationship between IB and anxiety or with a significant relationship in the opposite direction than expected) to test whether the overall effect size would remain significant given the maximal plausible publication bias. Next, the necessary severity of publication bias, that is, the ratio of unpublished nonaffirmative studies compared with published affirmative studies to reduce the real effect size of IBs in anxiety to zero, was calculated; higher numbers indicate a stronger necessary publication bias and thus a greater robustness of results. Finally, effect sizes were compared between peer-reviewed and non-peer-reviewed articles (e.g., articles in scientific journals vs. master’s theses) via moderation analyses.
Software and packages
All analyses were run in R (Version 4.3.1; R Core Team, 2022) using RStudio (Version 2023.6.1.524; Posit Team, 2023) and R Markdown (Xie et al., 2019) for the preparation of the initial results section. All meta-analytical procedures were conducted using the metafor package (Viechtbauer, 2010), and analyses of publication bias were ran using the package PublicationBias (Braginsky et al., 2023). Cluster-robust CIs for effect sizes and accompanying p values were calculated using the clubSandwich package (Pustejovsky, 2023).
Results
Study characteristics
A total of 295 independent samples comprising a total of 50,296 participants with 1,450 calculated contrasts were included in the meta-analysis. The included studies were conducted between 1987 and 2024; most of them included adult samples (k = 177, n = 29,476) and used a dimensional study design (k = 204, n = 41,829). The overall percentage of female participants was 63.09% and ranged between 0% and 100%. With 72 (24%) of studies, the largest proportion of studies were conducted in the United States. For a comprehensive summary of the extracted study characteristics, see Table 1; for the full list of studies and an overview of the included IB measures and their categorization, see Table S2 in the Supplemental Material.
Overall Study Characteristics
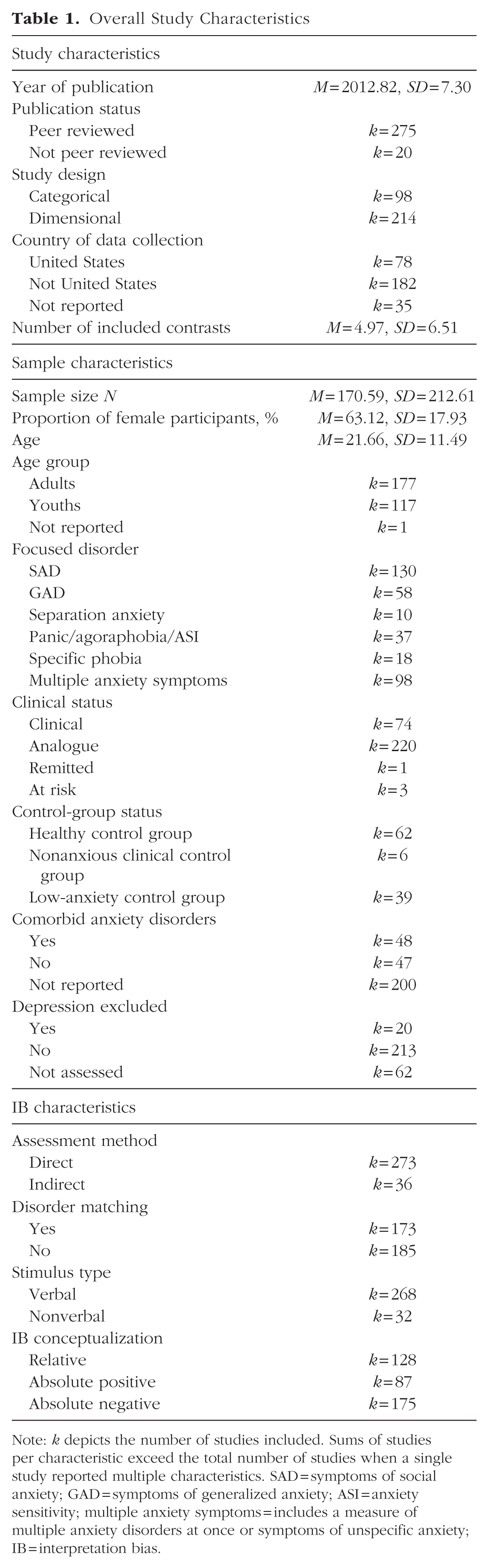
Note: k depicts the number of studies included. Sums of studies per characteristic exceed the total number of studies when a single study reported multiple characteristics. SAD = symptoms of social anxiety; GAD = symptoms of generalized anxiety; ASI = anxiety sensitivity; multiple anxiety symptoms = includes a measure of multiple anxiety disorders at once or symptoms of unspecific anxiety; IB = interpretation bias.
Overall effect-size association between IBs and anxiety
The overall effect size for the association between IBs and anxiety was g = 0.48, 95% CI = [0.43, 0.52], 95% PI = [−0.43,1.38], p < .001. Based on outlier analyses (standardized |residuals| > 3), 19 contrasts were identified as potential outliers that were excluded in all further analyses to improve accuracy of effect-size estimates. Repeating the main analysis excluding these outliers, we found that the effect size was g = 0.48, 95% CI = [0.44, 0.52], 95% PI = [−0.34, 1.30], p < .001. Nevertheless, a significant amount of heterogeneity remained even after excluding these outliers, Q(1,430) = 11,225.46, p < .001. Specifically, there was a significant amount of within-study (Level 2) variance, σ² = .09, χ²(1) = 2,582.3, p < .001, and between-study (Level 3) variance, σ² = .08, χ²(1) = 295.78, p < .001. The percentages of variance contributed at the different levels were the following: variance contributed by random sampling = 10.19%, within-study (Level 2) variance = 47.89%, and between-study (Level 3) variance = 41.92% (for the caterpillar plot depicting the effect sizes with accompanying 95% CIs and the overall effect size, see Fig. 2).
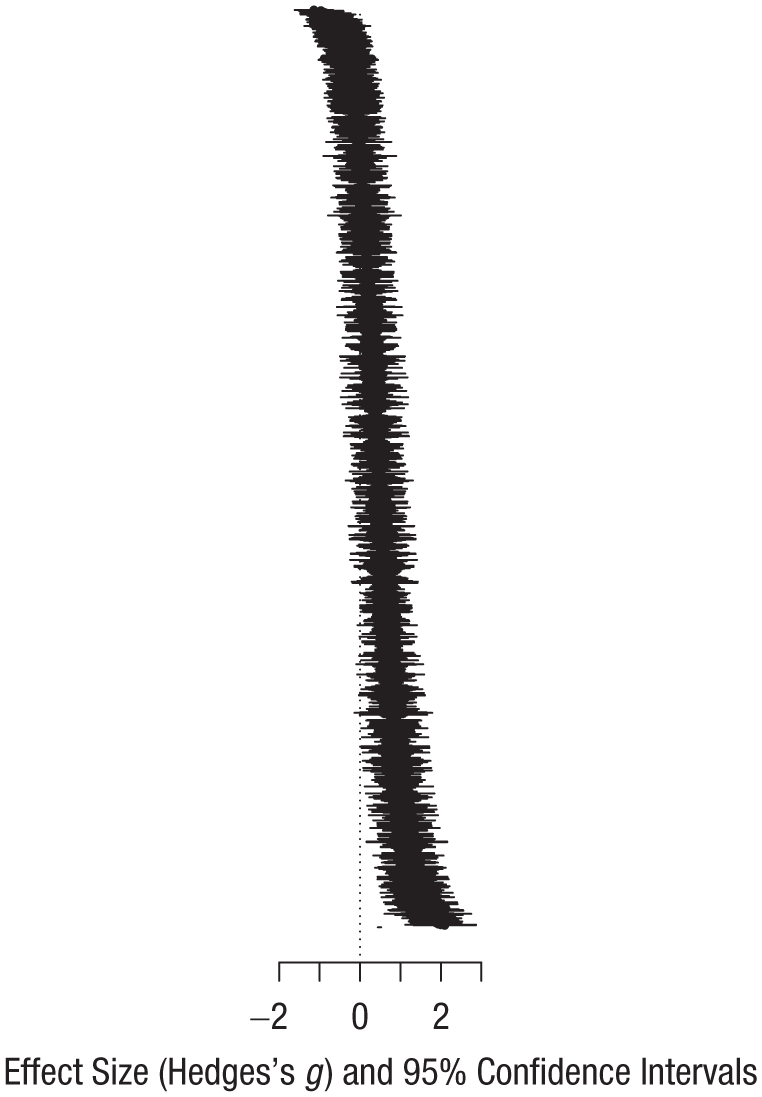
Forest plot of included studies.
Moderation analyses
To shed light on potential sources of heterogeneity, planned moderation analyses were carried out (for an overview, see Table 2).
Summary of Moderation Analyses
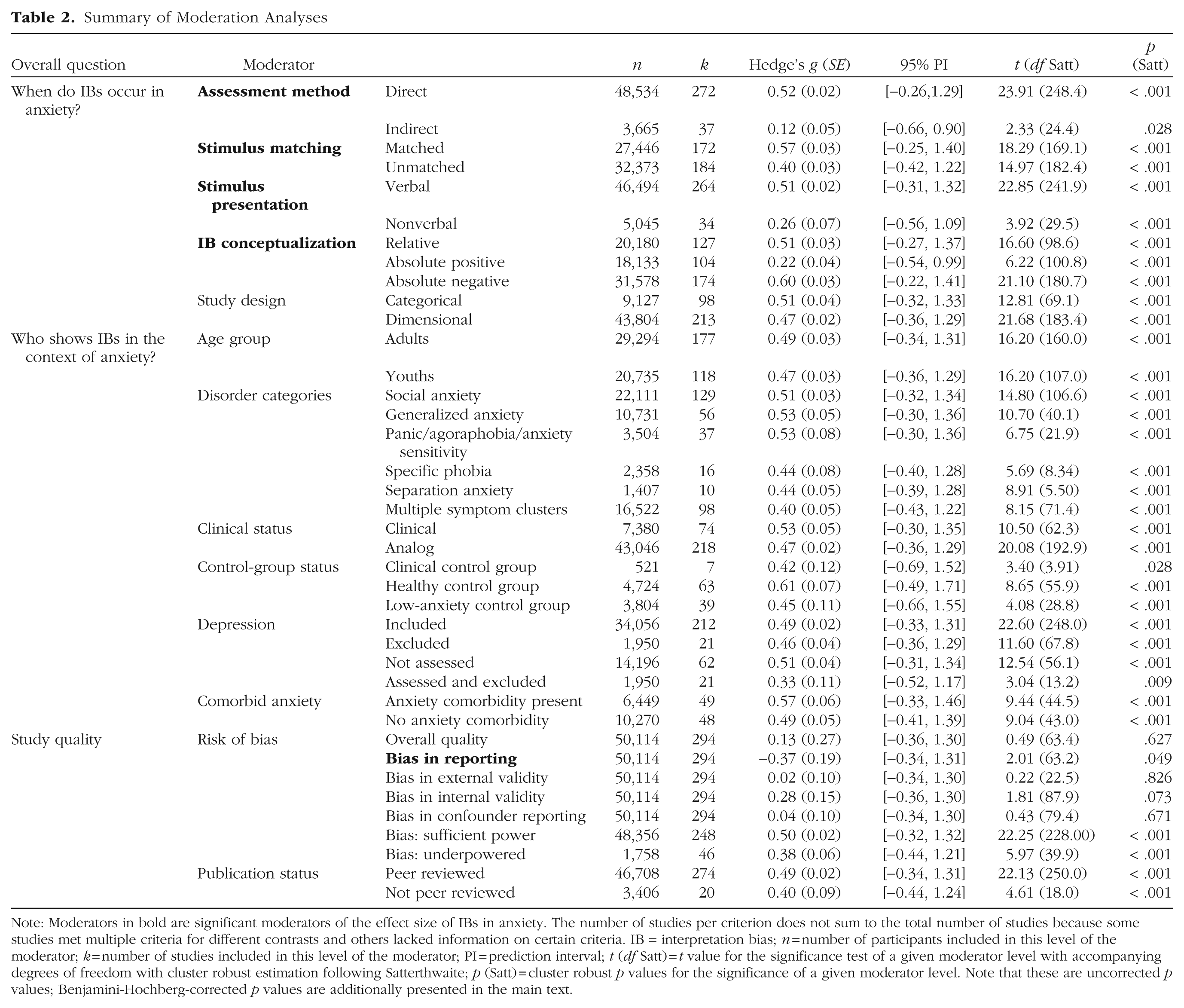
Note: Moderators in bold are significant moderators of the effect size of IBs in anxiety. The number of studies per criterion does not sum to the total number of studies because some studies met multiple criteria for different contrasts and others lacked information on certain criteria. IB = interpretation bias; n = number of participants included in this level of the moderator; k = number of studies included in this level of the moderator; PI = prediction interval; t (df Satt) = t value for the significance test of a given moderator level with accompanying degrees of freedom with cluster robust estimation following Satterthwaite; p (Satt) = cluster robust p values for the significance of a given moderator level. Note that these are uncorrected p values; Benjamini-Hochberg-corrected p values are additionally presented in the main text.
Under what assessment conditions do IBs occur in anxiety?
The assessment method was a significant moderator such that direct measures compared with indirect measures produced larger effect sizes for the association between IBs and anxiety, F(1, 1429) = 78.20, p < .001, BH-adjusted p = .005, with an estimated difference in effect sizes of g = 0.40, 95% CI = [0.28, 0.52]. Furthermore, the application of disorder-specific, matched stimuli was a significant moderator, indicating that IB measures including stimuli matched to the disorder-specific cognition of a given anxiety disorder produced larger effect sizes compared with nonmatched stimuli, F(1, 1429) = 38.63, p < .001, BH-adjusted p = .005, with an estimated difference in effect sizes of g = 0.17, 95% CI = [0.10, 0.25]. Stimulus type was also a significant moderator, that is, verbal stimuli produced significantly larger effect sizes compared with nonverbal stimuli (e.g., video or pictorial), F(1, 1429) = 13.82, p = .001, BH-adjusted p = .005, with an estimated difference in effect sizes of g = 0.24, 95% CI = [0.10, 0.39]. Furthermore, whether contrasts relied on an absolute or relative conceptualization of IBs was a significant moderator such that absolute positive conceptualizations were associated with smaller effect sizes compared with relative conceptualizations and absolute negative conceptualizations, F(1, 1429) = 134.50, p < .001, BH-adjusted p = .005, with an estimated difference in effect sizes of g = −0.32, 95% CI = [−0.39, −0.24]. Contrasts relying on absolute negative conceptualizations produced larger effect sizes compared with relative conceptualizations and absolute positive conceptualizations, F(1, 1429) = 66.19, p < .001, BH-adjusted p = .005, with an estimated difference in effect sizes of g = 0.20, 95% CI = [0.13, 0.27]. In general, contrasts relying on a relative IB conceptualization produced slightly larger effect sizes compared with all contrasts relying on absolute conceptualizations, F(1, 1429) = 9.83, p = .009, BH-adjusted p = .035, g = 0.113, 95% CI = [0.03, 0.20]. Finally, it did not differ whether studies applied a categorical or dimensional study design, F(1, 1429) = 1.19, p = .318, BH-adjusted p = .486, supporting the validity of aggregating data from both study types.
Who shows IBs in the context of anxiety?
Regarding sample-related moderators, there were no significant differences in effect sizes. To illustrate, testing the age group in which IBs were assessed showed no significant difference in the effect size between youths and adults, F(1, 1427) = 0.17, p = .664, BH-adjusted p = .702. Furthermore, testing each anxiety-disorder category and studies that included an aggregate score of multiple anxiety disorders against the remaining categories showed that there was no symptom category that specifically differed from the remaining categories, F(1, 1429) < 2.09, p = .282, BH-adjusted p = .486. In addition, effect sizes did not differ between studies that included clinical samples compared with studies including fully analog samples, F(1, 1429) = 1.76, p = .264, BH-adjusted p = .486. Comparing contrasts using different control groups revealed no differences between studies that included a nonanxious clinical control group, a healthy control group, or a low-anxiety control group, F(1, 628) < 2.37, p = .414, BH-adjusted p = .529. Effect sizes for the association between IBs and anxiety did not differ significantly based on whether studies explicitly excluded participants with a diagnosis of depression or above-threshold symptoms of depressive symptoms, F(1, 1429) = 4.93, p = .156, BH-adjusted p = .359. The comparison was also nonsignificant when studies were compared based on whether depressive symptoms were assessed, F(1, 1429) = 0.73, p = .359, BH-adjusted p = .486, or whether studies explicitly included participants with depressive symptoms compared with studies that excluded or did not assess these symptoms, F(1, 1429) = 0.30, p = .597, BH-adjusted p = .702. Following up this pattern of results by comparing inclusive and exclusive studies only when depressive symptoms were assessed, we also found no significant difference between inclusive and exclusive studies, F(1, 1145) = 4.11, p = .187, BH-adjusted p = .391. Finally, the presence of multiple anxiety disorders compared with a single anxiety disorder was not associated with a difference in effect sizes, F(1, 578) = 0.85, p = .356, BH-adjusted p = .486.
Risk of bias
Our risk-of-bias assessment using the adapted version of Downs and Black (1998) indicated that some methodological limitations were present across studies. In particular, the reporting of exact p values was limited: Only 41% of studies met this criterion. Furthermore, only a small proportion of studies (6.78%) involved samples that could be considered representative of the target population. Several internal-validity criteria were also either not reached at a sufficient level or not reported in some studies. For instance, only 40.68% of studies employed IB measures that were deemed valid and reliable, and just 28.81% accounted for potential confounding variables.
Testing the funnel-plot asymmetry as an indicator of possible small-sample bias using Egger’s test indicated no significant asymmetry via a nonsignificant intercept, β0 = −0.07, t(117.80) = 0.18, p = .859, and thus no small-sample effects (for the funnel plot, see Fig. 3). Calculating a “worst-case meta-analysis” including only nonaffirmative studies revealed an effect size that was close to zero yet still statistically significant, g = 0.05, 95% CI = [0.02, 0.09], p = .001, 95% PI = [−0.30, 0.41]. Furthermore, the publication bias calculated to be necessary to render the effect size nonsignificant indicated that no severity of publication bias could attenuate the overall effect size to zero, indicating a relative robustness of the results in relation to a publication bias (Mathur & VanderWeele, 2020). As a final test for the potential impact of publication bias, effect sizes were compared between peer-reviewed and non-peer-reviewed studies. The effect sizes, however, did not differ significantly, F(1, 1429) = 1.08, p = .333, BH-adjusted p = .486.
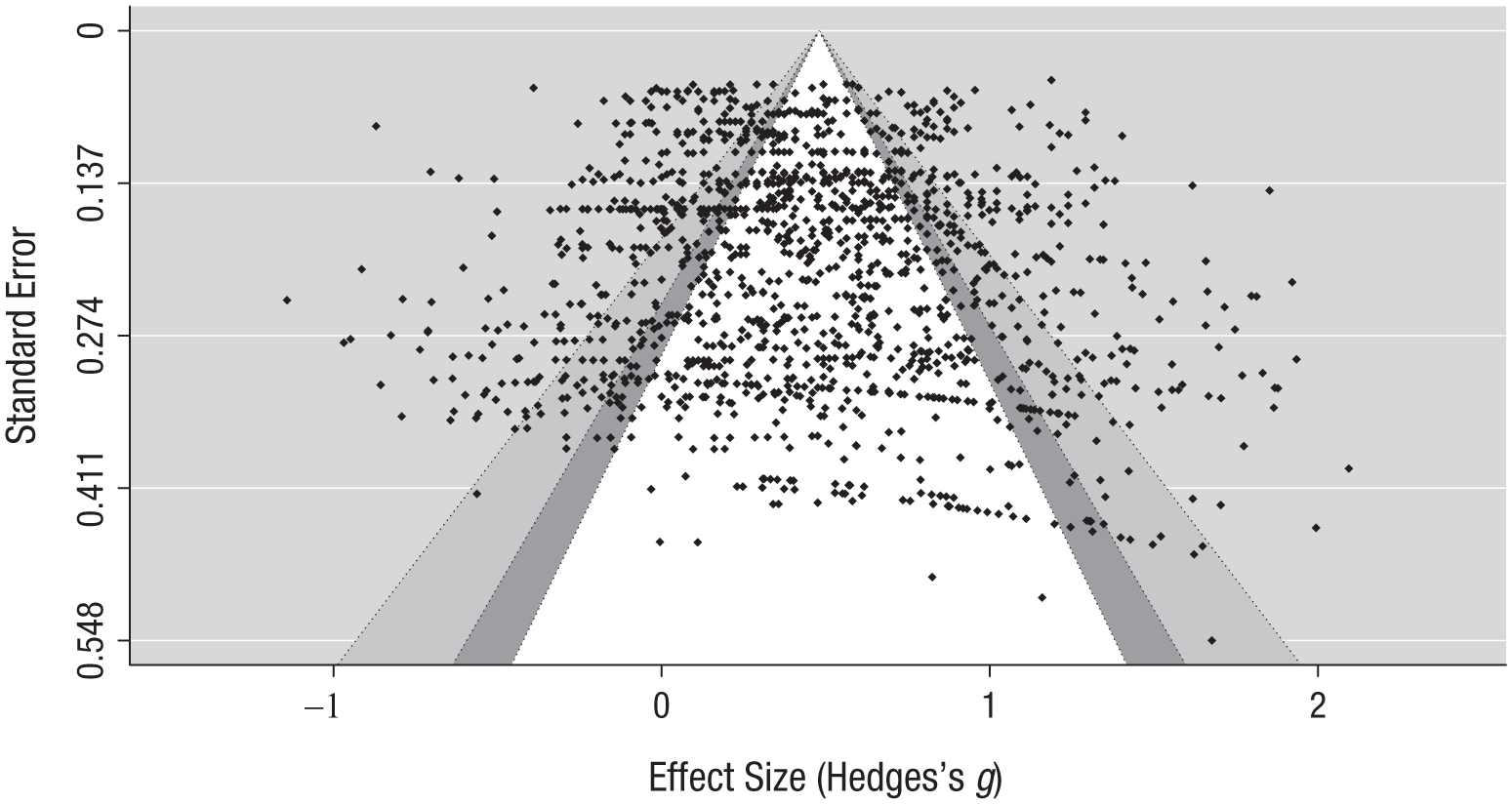
Funnel plot of included studies.
Testing the individual study quality as a potential moderator of effect sizes showed that the overall quality score of the study was not associated with the effect size, F(1, 1334) = 0.29, p = .627, BH-adjusted p = .702. Better reporting was associated with a lower effect size, F(1, 1414) = 3.69, p = .049, albeit BH-adjusted p = .161, g = −0.37, 95% CI = [−0.74, 0.00], 95% PI = [−0.34, 1.31]. However, neither threats to the internal validity, F(1, 1337) = 3.37, p = .073, BH-adjusted p = .210, nor threats to the external validity, F(1, 1429) = 0.05, p = .826, BH-adjusted p = .826, nor potential confounders, F(1, 1429) = 0.19, p = .671, BH-adjusted p = .702, were associated with differences in effect sizes. Finally, effect sizes from studies that had sufficient power did not differ from underpowered studies, F(1, 1429) = 3.53, p = .099, BH-adjusted p = .253.
Full model and explained heterogeneity
Rerunning the main model with all significant moderators included still resulted in a high level of unexplained heterogeneity, Q(1,425) = 8,624.44, p < .001. Specifically, a significant proportion of within-study (Level 2) variance, σ² = .07, χ²(1) = 1,694.76, p < .001, and between-study (Level 3) variance, σ² = .06, χ² (1) = 235.46, p < .001, remained. The percentage of contributed variance at the different levels were the following: variance contributed by random sampling = 12.92%, within-study (Level 2) variance = 48.16%, and between-study (Level 3) variance = 38.93%, which corresponds to an increase of within-study (Level 2) variance of 0.27% and a reduction of between-study (Level 3) variance of 2.99%.
Discussion
The aim of this meta-analysis was to quantify the strength of the association between IBs and anxiety across different anxiety disorders and sample types and to identify moderators of this association. Across all contrasts, the effect size for the association between IBs and anxiety was medium sized and positive, indicating that a stronger negative IB was associated with stronger symptoms of anxiety. In line with cognitive models of anxiety, our results suggest that IBs have transdiagnostic relevance across varying levels of anxiety and different anxiety disorders. This extends previous meta-analytic evidence by demonstrating their generalizability and supporting a unified model of anxiety symptoms. To further explore the high levels of heterogeneity, planned moderation analyses were conducted, which revealed that several methodological factors were associated with variations in effect sizes. Specifically, direct measures produced larger effect sizes compared with indirect measures, verbal stimuli produced larger effect sizes compared with nonverbal stimuli, stimuli that were matched to the disorder-specific cognition of a specific anxiety disorder were associated with larger effects, and relative IB conceptualizations were associated with larger effect sizes compared with absolute IB conceptualizations. Note that absolute positive conceptualizations produced the smallest effect size compared with absolute negative conceptualizations or relative conceptualizations, suggesting that a positive IB was less strongly associated with symptoms of anxiety than a negative IB.
Sample characteristics did not appear to be associated with differences in effect sizes, that is, no sample-related moderator, such as age, clinical status, or comorbidities, was associated with differences in effect sizes. Furthermore, neither the individual study quality nor small-sample or publication biases were found to pose significant threats to the validity of the present results; an association between better reporting and smaller effect sizes did not survive p-value correction. However, the high level of unaccounted heterogeneity, even after including all significant moderators, continues to limit the interpretability of the results.
Under what assessment conditions are IBs observed in anxiety?
Consistent with earlier meta-analyses on the role of IBs in psychopathology (Chen et al., 2020; Du et al., 2023; Everaert et al., 2017), we found that direct measures were associated with considerably larger effect sizes compared with indirect measures (e.g., relying on reaction times), although the effect size for indirect measures was still statistically significant. There are several explanations that may account for the significantly larger effect sizes for direct measures compared with indirect measures. A first explanation, also brought forward in earlier meta-analyses (cf. Everaert et al., 2017), is that the association between IBs and anxiety might be inflated because of response biases that direct measures are susceptible to. Second, direct measures rely on the same self-report methodology as anxiety measures, increasing shared-method variance and thus strengthening the association between the two. Third, the tasks’ psychometric properties are an important concern. For example, although results from measures of IBs are typically reported without estimates of the tasks’ reliability (cf. Gonsalves et al., 2019; Würtz et al., 2022), this is a particular issue with indirect measures of IBs (cf. Everaert et al., 2017). As a result, it remains unclear whether the observed differences in effect sizes are due to the absence of any effect identified through indirect measures or another important consideration in this context, limited power resulting from low reliability (Parsons et al., 2019). Hence, further theoretical and empirical work is warranted to improve and optimize indirect-assessment tools, comparable to work on other reaction-time-based measures in the context of experimental psychopathology (e.g., Kahveci et al., 2023). For instance, empirical and simulation-based studies could help guide the design (e.g., trial length and number) of indirect reaction-time measures to obtain adequate reliability.
Our results regarding the matching between stimuli and disorder-specific cognitions eliciting an IB are also in line with previous meta-analytic work (Stuijfzand et al., 2018) and support cognitive models of anxiety that emphasize content specificity (e.g., Clark, 1986; Hofmann, 2007). That is, although we found that anxiety is associated with an overall bias to interpret ambiguity negatively, such an IB was particularly prominent when disorder-specific stimuli were the to-be-interpreted target, for example, bodily responses in PD or social situations in social anxiety disorder. However, our meta-analysis extends findings from previous meta-analytic work (e.g., Stuijfzand et al., 2018, who showed this result in samples of children) by showing that the pattern is present across all participant populations, that is, independent of participants’ age. Put differently, content-specific IBs seem present in anxiety across the life span. Furthermore, the investigation of content specificity by Stuijfzand et al. (2018) was primarily based on studies on social anxiety. Although the present meta-analysis predominantly includes studies on social anxiety, it also included a great number of contrasts, thus allowing the investigation of content specificity in other anxiety contexts, such as (subclinical) panic, GAD, and specific phobias. Accordingly, our meta-analysis clearly extends earlier findings by showing that content-specific IBs are present in each specific disorder. These findings contribute to the validation of the diagnostic emphasis on core cognitions in specific anxiety disorders. For example, if a patient reports a fear of crowded places but primarily expresses concern about being subjected to negative judgments or comments from others, it may be advisable to assess for a potential (comorbid) diagnosis of social anxiety.
Another significant moderator was the application of verbal stimuli versus nonverbal stimuli in which results showed that verbal stimuli were associated with larger effect sizes. In aiming to explain this finding, we note that the researchers’ degrees of freedom in selecting stimuli and stimulus complexity may play a central role: Although verbal stimuli, for instance, the description of an ambiguous social situation, offer some room for heterogeneity, such as sentence length or language complexity (Schoth & Liossi, 2017), the use of images requires a much larger number of decisions. For example, when researchers aim to assess IB using pictorial stimuli in the context of social anxiety, it is essential to use ambiguous images that are socially relevant. This requires determining whether to use, for example, social scenarios or individual features, such as facial expressions, and this initial decision already introduces a potential source of heterogeneity. Should the decision be made to use faces, there is currently no consensus on the most effective way to operationalize ambiguity in facial expressions, specifically, whether surprised, neutral, or morphed facial expressions provide the most accurate representation (cf. In-Albon et al., 2008; Leung et al., 2022; Maoz et al., 2016). Taken together, even within a single anxiety-disorder category, pictorial stimuli offer large room for variability, which, in turn, constrains the size and precision of the measured effects. Next to the variability introduced by different types of images, pictorial stimuli are likely to be significantly more complex than verbal stimuli. Although sentences offer a relatively standardized transfer of information, images allow participants the possibility to shift their attention to different parts of the image (for a meta-analysis on the role of attention in anxiety, see Bar-Haim et al., 2007) and leave room for personal preferences, such as the perceived attractiveness of a face or the people depicted in the scene. Because all these factors contribute to heterogeneity in bias assessment with pictorial stimuli, it is crucial to first determine which types of stimuli are most suitable for specific research questions and subsequently standardize the assessment process. Furthermore, stimulus standardization through the sharing of validated stimuli should be promoted (for a discussion of standardization in IB research, see Würtz et al., 2022). Although this is relatively easy for verbal stimuli, copyright restrictions for image databases or protection of personal information for facial stimuli can limit their shareability. Given that pictorial stimuli offer certain advantages over verbal stimuli, such as potentially greater personal relevance and ecological validity, it is worthwhile to invest in their development. However, this will require extensive piloting of the selected stimuli, particularly with respect to their ambiguity, relevance, and complexity, before using them in confirmatory studies.
Finally, a methodological moderator of the effect sizes of IBs in anxiety was the conceptualization of IBs, that is, that an absolute positive IB was associated with smaller effects compared with an absolute negative or relative IB. Specifically, although our results suggest that anxiety is associated with both the presence of a negative IB and the absence of a positive IB, the latter association was considerably weaker. This finding supports the suggestion that positive and negative IBs should be seen as two different dimensions of the IB construct instead as two endpoints of the same dimension (cf. Huppert et al., 2003; Steinman et al., 2020). One potential reason for this finding might be that negative IBs are directly and relatively specifically associated with anxiety, whereas the absence of a positive IB might be, rather, associated with more general symptoms, such as trait-anxiety or negative affect (for similar reasoning, see Huppert et al., 2003). Given the varying strength of the association between IBs and anxiety depending on whether IBs were measured categorically or dimensionally, it is important to make an informed decision about which conceptualization best aligns with the specific research question. Although relative conceptualizations integrate information on positive and negative biases and thus produce larger effect sizes (cf. Everaert et al., 2017), it is impossible to distinguish whether, for example, the presence of a negative bias or the absence of a positive bias produces the outcome. However, studies on, for example, causal effects of IBs aim to induce a particular direction of IB, positively or negatively, and should therefore apply measures that index those dimensions separately. This is of particular importance given the common finding from experimental work that positive but not negative inductions of IBs are more successful (for different disorders, see Dietel et al., 2018; Joormann et al., 2015; Möbius et al., 2015; for anxiety, see Würtz et al., 2023), raising the question whether and why the two valence dimensions differ in terms of their modifiability.
Who shows IBs in the context of anxiety?
Across all studies, there were no sample-related moderators that explained significant differences in effect sizes of IBs in anxiety, suggesting that IBs occur irrespective of participants’ age, the specific type of anxiety disorder, the sample’s clinical status, or comorbidities. Our findings converge with earlier meta-analytical research on attentional or memory biases in psychopathology that revealed no difference between youths and adults in the association between biases and symptoms (Bar-Haim et al., 2007; Everaert et al., 2022), possibly suggesting that cognitive mechanisms of childhood psychopathology do not differ from those relevant in adults. Furthermore, the lack of significant effects for specific disorders as moderators underlines the assumption of a general model of pathological anxiety (Beck & Clark, 1997), supporting the notion that IBs play a central role in anxiety irrespective of the specific disorder.
The assumption that anxiety disorders should be considered as a continuum in research (cf. Chen et al., 2020) is supported by our data: Effect sizes did not vary based on participants’ (clinical) group status, that is, whether they belonged to analog samples with subclinical anxiety symptoms or had a diagnosed clinical anxiety disorder. Together with findings from other meta-analytic research in interpretation, memory, and attention biases (Bar-Haim et al., 2007; Everaert et al., 2017, 2022), our results suggest that although mental disorders may differ in symptom severity, they likely share common underlying mechanisms given that the association between IB and symptoms did not vary with participants’ clinical status. This, in turn, further highlights the value of data derived from analog samples as meaningful models for clinical anxiety.
Excluding or including participants with comorbid depression did not affect the strength of the association between IBs and anxiety. This is partly surprising and suggests that using a “pure” sample of participants without comorbid depression is not necessary to obtain a realistic estimate of the effect. In fact, excluding participants with depression might even decrease the quality of the estimations. To illustrate, because comorbidity between anxiety and depression is rather common, with about 50% of people suffering from anxiety also experiencing depressive symptoms (e.g., Johansson et al., 2013), excluding participants with depression might create a rather nonrepresentative and selective sample without a significant advantage in terms of internal validity.
Further methodological implications
One additional result of the present meta-analysis is the finding that research on IBs in anxiety is subject to extensive heterogeneity, limiting the interpretability of the present results. An important aim of future research should therefore be to identify potential methodological sources of this heterogeneity. One approach would be to address the significant variability in methods used to assess IBs (Schoth & Liossi, 2017), as demonstrated in our moderation analyses comparing different operationalizations of IB. However, some variability in methods is necessary for cross-validation of findings across different measures of IBs. Moreover, although there is emerging evidence suggesting promising psychometric properties of IB measures, such as the Scrambled Sentences Task (SST), which is mainly used in the context of depression (e.g., Würtz et al., 2022), many studies in our meta-analysis lacked clear reporting of (good) psychometric characteristics. To improve future research in this field, we recommend that researchers provide detailed information on the reliability and validity of their IB assessments and ensure appropriate control for potential confounders and representative sampling methods. Therefore, it is currently unclear which IB measures are ideal to assess IBs in terms of internal validity, reliability, or general operational features (e.g., automatic or elaborative aspects; see Hirsch et al., 2016) and which measures are susceptible to produce noise that then increases the variability in effect sizes. Although in this meta-analysis, we aimed to investigate methodological heterogeneity, this was limited to our operationalization of moderators (e.g., the choice of categorization: verbal vs. nonverbal or matched vs. unmatched). However, there may be more subtle differences between measures, for instance, the amount of time participants had to generate an interpretation or the numbers of trials, and such variations and differences could also contribute to the unaccounted heterogeneity. A central methodological recommendation would therefore be to standardize IB assessments, that is, reevaluate all available IB measures via systematic validation studies and theoretical work. This, in turn, could guide researchers’ choice of a suitable assessment tool for a specific IB-related research question (for further reading on measurement practices and theoretical underpinnings, see Flake & Fried, 2020; Scheel, 2022). A final suggestion for follow-up studies concerns the potential moderating role of stress or mood manipulations in the relationship between IBs and anxiety. Specifically, the strength of the association between IBs and anxiety may vary under conditions of stress or heightened negative affect. Although in the present meta-analysis, we focused on the direct association between IBs and anxiety, future research should examine how such contextual factors may influence or amplify this relationship.
Clinical implications
Results of our meta-analysis show that IBs are associated with anxiety irrespective of whether an individual suffers from subclinical symptoms or are diagnosed with a clinical anxiety disorder. However, because of the cross-sectional nature of our analyses, the direct clinical implications are somewhat limited. Nevertheless, it seems reasonable to consider interventions aimed at reducing negative IBs, in fact, a common approach in clinical practice, particularly in evidence-based treatments, such as cognitive restructuring in CBT (e.g., Woud & Hofmann, 2023). The primary goal of cognitive restructuring is to shift patients’ focus and help them reevaluate their biased thinking patterns. This process encourages the development of more adaptive cognitions, which, in turn, should reduce negative or anxious responses to specific situations. Our findings, which suggest a stronger association between negative IBs and anxiety symptoms compared with the absence of a positive IB, are thus consistent with the focus on addressing negative IBs in treatment. However, it is also important to consider interventions that are easily disseminated and scalable (cf. Koster et al., 2009), and in this context, potential clinical implications can be drawn from clinical-experimental research. To illustrate and as pointed out by previous meta-analyses on the role of IBs in psychopathology and their experimental modification (e.g., Everaert et al., 2017; Fodor et al., 2020), there is large room for improvement when thinking of, for example, cognitive-training interventions aiming to reduce negative IB. Specifically and in line with our findings, it seems important to design IB trainings for anxiety focusing on the reduction of negative IBs into more neutral or benign interpretations rather than the induction of positive IBs. This would also be in line with recent discussions that positive interpretations presented in training can sometimes be too positive to be credible for people with a strong negative IB in the first place (e.g., clinical samples) and thus may lead to reactance (cf. Woud et al., 2021).
Limitations
The results of the present meta-analysis need to be interpreted in light of several limitations. First, studies were included only if they were published in English language, potentially introducing cultural biases. Furthermore, the investigation of IBs was limited to interindividual comparisons, which allowed us to address the question whether IBs differentiate between anxious and nonanxious samples but not the question whether different groups of participants show a specific pattern of biases. Another limitation in interpreting the results is the high degree of heterogeneity that could not be explained by the moderation analyses. Although it was the aim of the present analysis to follow a comprehensive approach aggregating highly heterogeneous data, the broad conceptualization of how IBs should be conceptualized and assessed (Schoth & Liossi, 2017) and the heterogeneity in individual assessment tools (Flake & Fried, 2020; Würtz et al., 2022) put a limit on the precision of the obtained effect-size estimates. Although we acknowledge that factors such as ethnicity and socioeconomic status are important moderators, they were not included in our meta-analysis because of the limited availability of relevant data, as confirmed during the extraction and aggregation process. In addition, the classification of ethnicity varies across countries, and the relevance of different ethnic groups depends on the regional context, further complicating cross-study comparisons. Nevertheless, these remain important moderating factors that should be considered when examining IBs in anxiety. Another important direction for future research is to examine the included moderators separately for youth samples versus adult samples to gain a more nuanced understanding of how these moderators may interact differently across the life span. That is, this approach would enhance understanding of how developmental factors and age-related differences shape the relationship between IBs and anxiety symptoms in conjunction with the included moderators. A final limitation is that all studies included in this meta-analysis are cross-sectional, which constrains our ability to infer causality. For a broader perspective, readers may refer to literature examining IBs in the context of anxiety or the wider spectrum of emotional psychopathology using longitudinal and experimental designs (e.g., Hirsch et al., 2016; Jones & Sharpe, 2017; Martinelli et al., 2022; Vos et al., 2025; Woud, 2023).
Conclusion
Anxiety is associated with the tendency to consistently interpret ambiguous information in a negative manner. This association is found for both the direct measurement and indirect measurement of IBs; however, direct measures produced larger effects than indirect measures. Furthermore, assessment through verbal stimuli leads to significantly larger effects compared with using nonverbal stimuli. Although anxiety is associated with a negative general IB, there is evidence for content specificity. That is, the association between IBs and levels of anxiety was considerably stronger in case disorder-specific cognitions were used to infer IBs. Finally, the lack of a positive IB was less strongly associated with symptoms of anxiety compared with an absolute negative or relative IB. Regarding sample-related variables, neither participants’ age, nor the clinical status of the anxious or control groups, nor comorbidities modulated the strength of the effect sizes. These findings suggest that IBs are universally relevant in anxiety, which validates the assumptions of various cognitive models in the context of anxiety, that is, disorder-specific models of anxiety versus general models of anxiety. This, in turn, has important implication for clinical work, supporting the need for techniques that specifically reduce IBs. However, the assessed strengths of IB depended on the type of measure, indicating that systematic research is needed to further elucidate the operational features, underlying mechanisms, and boundary conditions of IBs in the context of anxiety.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026251392855 – Supplemental material for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis
Supplemental material, sj-docx-1-cpx-10.1177_21677026251392855 for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis by Felix Würtz, Marius Kunna, Simon E. Blackwell, Chiara Lindgraf, Elinor Abado, Yagmur Amanvermez, Jürgen Margraf, Jonas Everaert and Marcella L. Woud in Clinical Psychological Science
Supplemental Material
sj-docx-2-cpx-10.1177_21677026251392855 – Supplemental material for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis
Supplemental material, sj-docx-2-cpx-10.1177_21677026251392855 for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis by Felix Würtz, Marius Kunna, Simon E. Blackwell, Chiara Lindgraf, Elinor Abado, Yagmur Amanvermez, Jürgen Margraf, Jonas Everaert and Marcella L. Woud in Clinical Psychological Science
Supplemental Material
sj-docx-3-cpx-10.1177_21677026251392855 – Supplemental material for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis
Supplemental material, sj-docx-3-cpx-10.1177_21677026251392855 for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis by Felix Würtz, Marius Kunna, Simon E. Blackwell, Chiara Lindgraf, Elinor Abado, Yagmur Amanvermez, Jürgen Margraf, Jonas Everaert and Marcella L. Woud in Clinical Psychological Science
Supplemental Material
sj-docx-4-cpx-10.1177_21677026251392855 – Supplemental material for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis
Supplemental material, sj-docx-4-cpx-10.1177_21677026251392855 for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis by Felix Würtz, Marius Kunna, Simon E. Blackwell, Chiara Lindgraf, Elinor Abado, Yagmur Amanvermez, Jürgen Margraf, Jonas Everaert and Marcella L. Woud in Clinical Psychological Science
Supplemental Material
sj-docx-5-cpx-10.1177_21677026251392855 – Supplemental material for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis
Supplemental material, sj-docx-5-cpx-10.1177_21677026251392855 for Interpretation Biases in Anxiety: A Three-Level Meta-Analysis by Felix Würtz, Marius Kunna, Simon E. Blackwell, Chiara Lindgraf, Elinor Abado, Yagmur Amanvermez, Jürgen Margraf, Jonas Everaert and Marcella L. Woud in Clinical Psychological Science
Footnotes
Acknowledgements
We thank all authors who have contributed unpublished data to this meta-analysis. We further thank Julia Grönwald and Laura Borris for their assistance in collecting the full texts of included articles. The funders had no role in the study design, collection, analysis, or interpretation of data; writing the manuscript; or the decision to submit the article for publication. All materials, including the coding scheme and instructions, extracted data, and analysis script, are openly available on OSF: ![]() .
.
Transparency
Action Editor: Kelsie T. Forbush
Editor: Jennifer L. Tackett
Author Contributions
The senior authors, M. L. Woud and J. Everaert, contributed equally to this work.
ORCID iDs
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.