
Abstract
The feeling of being of little worth can trigger suicidal thoughts and behaviors (STBs). In this meta-analysis, we examined the association between self-esteem and STBs based on 114 studies and tested potential moderators of this association. We found moderate to strong negative associations between self-esteem and STBs (ideation: r = −.435, d = −0.805; behavior: r = −.258, d = −0.828; combination of thoughts and behaviors: r = −.405, d = −1.610). In this meta-analysis, we identified evidence gaps, including the need for more studies on the association between suicidal behavior and self-esteem, more research on the second half of life, and more longitudinal studies. Overall, this meta-analysis provides a more nuanced understanding of the relationship between self-esteem and STBs and contributes to the existing literature on suicide prevention.
Keywords
Suicide is a pressing global issue; more than 700,000 deaths by suicide occur annually (World Health Organization, 2021). In the United States alone, suicide was one of the leading causes of death in 2020, claiming 45,979 lives (Centers for Disease Control and Prevention, 2023). The impact of suicide extends beyond the individual, negatively affecting an average of 135 people per suicide, including loved ones and clinical staff (Cerel et al., 2019). Given the far-reaching impacts and societal costs of suicidal thoughts and behaviors (STBs), researchers have dedicated significant efforts to understanding the associated risk and protective factors (e.g., Favril et al., 2022; Franklin et al., 2017). One factor that—theoretically (e.g., Bryan et al., 2020; Joiner, 2005) and empirically (e.g., Eades et al., 2019; Wild et al., 2004)—has been consistently and across various age groups linked to high levels of STBs is low self-esteem. In the present systematic review and meta-analysis, we examined the relationship between self-esteem and STBs across different developmental periods.
Definitions
Contemporary research typically distinguishes between suicidal ideation and suicidal behavior (Crosby et al., 2011; Goodfellow et al., 2020). Suicidal ideation (also called suicidal thoughts) refers to thinking about or considering suicide (Klonsky et al., 2016). Suicidal behavior includes (aborted and interrupted) suicide attempts and suicides (Van Orden et al., 2010). Both types of suicidal behavior, nonfatal and fatal, include self-initiated, potentially injurious actions that are accompanied by a (nonzero) intent to die (Posner et al., 2014). Although suicidal ideation is a strong predictor of suicide, most individuals who experience suicidal thoughts do not engage in suicidal behavior (Bryan, 2021; Franklin et al., 2017; McHugh et al., 2019). Moreover, STBs can be considered as transdiagnostic symptoms that can occur across diagnostic boundaries and in individuals with different mental disorders (Schechter & Goldblatt, 2020). However, especially suicidal thoughts are not restricted to clinical samples but may occur in the general population (e.g., DeVylder et al., 2015).
Self-esteem refers to an individuals’ subjective evaluation of their worth as a person (Leary & Baumeister, 2000). It is conceptualized as the “feeling that one is ‘good enough’” (Rosenberg, 1965b, p. 31), which includes aspects of self-acceptance, self-satisfaction, and self-respect. Very low self-esteem, in turn, is characterized by dysfunctional and destructive self-evaluation, often associated with self-criticism and self-hate (Turnell et al., 2019). According to sociometer theory (Leary & Baumeister, 2000), self-esteem acts as a gauge of an individual’s social relationships (i.e., the “sociometer”), and self-esteem is likely to suffer when relationships are threatened or undermined (e.g., because of social rejection).
Despite the established association between low self-esteem and a plethora of psychopathological symptoms, including depression and anxiety (Orth & Robins, 2022), several dimensions of the relationship between self-esteem and STBs remain poorly understood. First, the potential moderating factors in the relationship between self-esteem and STBs are insufficiently clear. Second, the role of self-esteem in the course of STBs—whether it plays a different role in the ideation and execution of suicidal behaviors—remains poorly defined. Finally, the varying operational definitions and measurements of STBs and (to a lesser extent) of self-esteem used across studies complicate direct comparison and consensus building in this research area. In the present meta-analysis, we use rigorous criteria for including studies, and homogeneous definitions help reconcile these discrepancies and strengthen the nuanced understanding of the relationship between self-esteem and STBs.
Theoretical Perspectives on the Interplay of STBs and Self-Esteem
Interpersonal theory of suicide
A key element of the interpersonal theory of suicide—one of the most prominent ideation-to-action theories of suicide (cf. Klonsky & May, 2015; O’Connor & Kirtley, 2018)—is to posit pathways by which suicidal ideation and both nonfatal and fatal suicidal behavior develop (Joiner, 2005; Van Orden et al., 2010). Two core constructs are most relevant for suicidal ideation according to the interpersonal theory of suicide: thwarted belongingness and perceived burdensomeness. “Thwarted belongingness” refers to the feeling of not being accepted or included in a social group or community. “Perceived burdensomeness” also captures a facet of social disconnection by referring to the perception that one is a burden on others and that one’s presence is detrimental to the well-being of individuals around them. According to the interpersonal theory of suicide, near-lethal or lethal suicidal behavior occurs only when suicidal ideation and the capability for suicide coincide, which includes heightened pain tolerance and fearlessness about death and dying (Chu et al., 2017; Joiner, 2005).
Both thwarted belongingness and perceived burdensomeness show conceptual proximity and empirical relations to low self-esteem (Eades et al., 2019; Van Orden et al., 2010, 2012). People with low self-esteem may feel like they do not fit in with a social group or community. This can result in a sense of thwarted belongingness. At the same time, people with low self-esteem may also feel like they are a burden on others and that their presence is not beneficial to the people around them, which can lead to feelings of perceived burdensomeness. In the context of the interpersonal theory of suicide, low self-esteem can thus be understood as an antecedent for perceived burdensomeness and thwarted belongingness. More specifically, the association between low self-esteem and suicidal ideation should be mediated by perceived burdensomeness and thwarted belongingness (cf. Teismann et al., 2024).
In sum, based on the interpersonal theory of suicide, negative associations between STBs and self-esteem can be expected. This negative association should be stronger between low self-esteem and suicidal ideation than between low self-esteem and suicide attempts simply because the theory sees factors (fearlessness of death and dying, pain tolerance) responsible for the development of suicidal behavior that are likely to develop independently of self-esteem, whereas factors responsible for suicidal ideation (e.g., perceived burdensomeness, thwarted belongingness) are more closely related to low self-esteem.
Fluid-vulnerability theory
Fluid-vulnerability theory (Rudd, 2006)—a generic theory of suicide—hypothesizes that suicidal crises arise in the context of an intricate, multicomponential, self-reinforcing dynamic system in which individually functional constellations of risk factors escalate and shift abruptly rather than gradually (Butner et al., 2021; Kaurin et al., 2022). Put differently, the theory postulates a “suicidal mode” that can be activated (i.e., the patient is suicidal) by specific triggers, such as stressful and uncertain life events. However, the suicidal mode can also effectively be deactivated (i.e., the patient is at low risk). The concept of the suicidal mode includes many risk factors and protective factors for suicidal behavior. One core risk factor mentioned in the fluid-vulnerability theory is the cognitive suicidal belief system, which includes themes such as unlovability and perceived burdensomeness (Rudd, 2006). According to this perspective, people with overly negative beliefs and assumptions about themselves (and others)—that is, people with low self-esteem—are more likely to experience intense emotions in response to stressful events or experiences. These emotions can, in turn, lead to STBs (Bryan et al., 2013, 2019). Items that are designed to assess these dysfunctional, suicidogenic beliefs show high conceptual proximity to cognitions characterizing low self-esteem (e.g., “I am completely unworthy of love” or “There is nothing redeeming about me” from the Suicide Cognitions Scale revised; Bryan et al., 2022). Consequently, the conceptual closeness between the cognitions characteristic of STBs and low self-esteem suggests a significant negative association between STBs and self-esteem such that low self-esteem leads to suicidal ideation and behavior. However, unlike the interpersonal theory of suicide, the fluid-vulnerability theory does not specify whether certain types of negative cognitions (e.g., perceived burdensomeness, thwarted belongingness) are more critical for developing suicidal thoughts than other types (e.g., self-devaluation, entrapment). In addition, the fluid-vulnerability theory does not emphasize factors that are particularly relevant for the transition from suicidal thoughts to suicidal behavior. The fluid-vulnerability theory puts more emphasis on viewing suicide risk as an intricate, multicomponential, self-reinforcing, dynamic system (Kaurin et al., 2022; Rudd et al., 2006), which is further evidenced by subjective reports of people who have attempted suicide (e.g., Wyder & De Leo, 2007). Because of this heterogeneity in both indicators of risk factors and their links to suicidal thoughts and behaviors, the theory does not provide differential hypotheses regarding the relationship between low self-esteem and suicidal thoughts and behavior but, rather, puts emphasis on viewing suicide risk as an idiosyncratic phenomenon.
Previous Empirical Findings on the Interplay of STBs and Self-Esteem
Given the theoretical significance of self-esteem for the emergence of STBs, it is not surprising that many empirical studies also confirm a moderate to strong relationship between the constructs (based on guidelines proposed by Funder & Ozer, 2019) across different age groups, such as adolescents and older adults (e.g., Brausch & Gutierrez, 2010; Eades et al., 2019; Wild et al., 2004). Self-esteem is also emphasized in research on resilience against STBs. In this context, high self-esteem is considered a protective factor against STBs (Johnson et al., 2011; Teismann & Brailovskaia, 2020).
Only one previous meta-analysis on this association exists—explicitly focused on youths. This meta-analysis suggests that youths with lower self-esteem are at high risk for future suicide attempts (d = 0.58, 95% confidence interval [CI] = [0.44, 0.74]; Soto-Sanz et al., 2019). This meta-analysis included only nine studies, focused solely on suicidal behavior, and examined individuals ages 12 to 26 years, which limits the generalizability of the findings. In the present meta-analysis, we take a broader approach by examining both suicidal ideation and suicidal behavior. Moreover, we considered studies from childhood to old age and were thus able to include considerably more studies. Studying the relationship between self-esteem and STBs in different age groups may allow for the identification of age-specific correlates of STBs, acknowledging that enhancing self-esteem may work for one age group in reducing STBs but may not be as effective for another age group. Consequently, we provide a more comprehensive perspective on the link between self-esteem and STBs.
Potential Moderating Effects on the Association Between STBs and Self-Esteem
In addition to examining the general strength of the STB–self-esteem link, in the present meta-analysis, we aimed at providing a more detailed understanding of their association by examining possible moderators, such as clinical versus nonclinical samples, the average depression score of the sample, age, and gender.
Clinical versus nonclinical samples
Associations between self-esteem and STBs might differ between clinical and nonclinical samples for at least two reasons.
First, the range of variation in the investigated variables is important for correlational analyses. In clinical samples, especially those reporting clinically relevant experiences of distress, the ranges of variation in suicidal ideation and self-esteem are likely restricted, affecting the estimates of the sampling variance in the correlation coefficient (Millsap, 1989). This restriction may lead to lower estimates of the meta-analytic correlation.
Second, theoretically, low self-esteem might have different implications in clinical versus nonclinical contexts. In clinical samples, low self-esteem may often be a symptom of underlying mental disorders, such as depression or anxiety, which are directly associated with suicidal ideation and behaviors (e.g., Sareen et al., 2005). In contrast, in nonclinical samples, low self-esteem may be viewed as a risk factor or correlate that contributes to vulnerability but does not necessarily indicate a clinical condition. Thus, the functional equivalence of low self-esteem might differ between these groups, potentially leading to variations in the strength and nature of its association with STBs. To explore these theoretical and conceptual differences, we included the sample type (clinical sample vs. general population) as a moderator in our analyses.
Depression scores of the sample
Depression is characterized by pervasive negative affect and maladaptive cognitive patterns, such as rumination and negative thinking (e.g., Fried et al., 2016), all of which can amplify the negative impact of low self-esteem. Individuals with higher levels of depression may experience more intense feelings of worthlessness and hopelessness, making the relationship between low self-esteem and suicidal thoughts and behaviors more pronounced. Furthermore, depression often leads to social withdrawal and isolation, reducing the availability of social support and intensifying feelings of loneliness (Cacioppo et al., 2006). In such contexts, low self-esteem can more directly contribute to suicidal ideation and behavior. Given these considerations, the level of depression could significantly moderate the relationship between self-esteem and STBs, highlighting the importance of including the average depression score as a moderator in our meta-analysis. This moderator analysis was not preregistered.
Age
Age might also moderate the relationship between STBs and self-esteem. STBs manifest throughout the life span (Nock et al., 2014), escalating from adolescence (around age 12) to young adulthood (approximately age 21; Lawson et al., 2022). In addition, various longitudinal studies assessing the trajectory of self-esteem observed an upswing from adolescence to middle adulthood (peaking around ages 50–60) and a subsequent declining trend accelerating into late adulthood (Orth et al., 2018; Orth & Robins, 2014). These patterns suggest “normative” developmental trajectories for STBs and self-esteem, indicating that individuals, on average, may be more susceptible to STBs and low self-esteem during specific life stages. Yet these trajectories do not conclusively determine whether low self-esteem is a more pronounced risk factor for STBs during certain life stages or if it remains an age-independent risk factor. Developmental periods, such as adolescence, young adulthood, midlife, and old age, each come with distinct psychosocial challenges that can affect the relationship between self-esteem and STBs. For instance, during childhood and adolescence, individuals are navigating rapid physical, emotional, and social changes; self-esteem issues at this critical period may have profound effects on their mental health and vulnerability to STBs. Conversely, in older adults, factors such as life transitions, loss of loved ones, and changes in health status may be more important than self-esteem in predicting STBs, and thus, the association between self-esteem and STBs could be weaker in older samples compared with younger samples. By considering these developmental contexts, we aimed to explore whether the strength and nature of the relationship between self-esteem and STBs differs between age groups.
Prior research, including Orth and Robins (2022), advocates that high self-esteem is advantageous across diverse developmental periods. Moreover, a meta-analysis examining the prospective link between self-esteem and depression, spanning from childhood to late adulthood, found no age-related moderating impact (Sowislo & Orth, 2013). Despite these findings, our analysis included the mean age of the sample as a potential moderator, aiming to ascertain the generalizability of these concurrent meta-analytic associations across various age groups and developmental phases.
Gender
Previous meta-analyses found that the effect of low self-esteem on subsequent depression operated independently of gender (Sowislo & Orth, 2013). However, it is unclear whether this finding applies equally to the association between self-esteem and STBs. Therefore, we examined whether the percentage of women in a sample moderated the meta-analytic associations. Several factors might explain why self-esteem could play a different role in STBs for women and men.
Small gender differences in self-esteem are documented; females typically report slightly lower self-esteem than males, especially during adolescence (e.g., Quatman & Watson, 2001). This difference may influence the relationship between self-esteem and STBs. However, regarding the trajectory of self-esteem from age 14 to age 30, no gender differences were found (Erol & Orth, 2011).
Moreover, gender differences exist in the prevalence and methods of STBs and suicide. Women are more likely to experience suicidal ideation and attempt suicide, whereas men are more likely to die by suicide, often using more lethal methods (Schrijvers et al., 2012). Moreover, the availability and utilization of social support and differences in coping mechanisms can influence the relationship between self-esteem and STBs. Women are more likely to seek and receive social support than men (e.g., Flaherty & Richman, 1989), which might help mitigate the impact of low self-esteem on STBs. Conversely, men, who might be less inclined to seek support because of societal norms, could be more vulnerable to the effects of low self-esteem on STBs.
Given these considerations, we explored whether gender, as indicated by the percentage of women in a sample, moderated the association between self-esteem and STBs. With this analysis, we aim to provide insights into whether self-esteem plays a greater role in STBs for one gender compared with the other, thereby offering a more nuanced understanding of this relationship.
Time frame of measures
Both self-esteem and STBs can be examined in a “trait-like” fashion, using measures that employ time frames such as “in general,” and in a “state-like” fashion, using measures with time frames such as “currently” or somewhat broader, “during the past 2 weeks.” Previous research showed that low self-esteem predicts depressive symptoms only when trait time frames for self-esteem were applied but not when state time frames were applied (Braun et al., 2021). In this meta-analysis, we included and coded all time frames to examine whether the link between self-esteem and suicidality differs depending on the time frame used.
Beyond the above-mentioned key moderators, we included further exploratory moderators, such as the ethnicity of the sample, the publication year, and the type of self-esteem scale used. Those exploratory moderators were included to test the generalizability of our findings across different study and sample characteristics.
The Present Study
The primary aim of our study is to provide a comprehensive meta-analytic review of the association between self-esteem and STBs 1 across different developmental periods and sample characteristics. Despite previous research on the relationships between these variables, there has been a lack of synthesis in the literature that examines this relationship across diverse populations and contexts. Moreover, to date, an unresolved question in the literature is whether self-esteem is more strongly related to suicidal ideation or suicidal behavior. In this meta-analysis, we thus separately examined the association between self-esteem and suicidal ideation and the association between self-esteem and suicidal behavior. Because suicidal ideation is a cognitive symptom and self-esteem is associated with cognitive evaluations about oneself, one might expect stronger associations between self-esteem and suicidal ideation than between self-esteem and suicidal behavior. Relatedly, the interpersonal theory constructs of perceived burdensomeness and thwarted belongingness are more directly related to suicidal ideation than behavior (Chu et al., 2017).
As preregistered, we hypothesized a significant, negative association between self-esteem and STBs. Accordingly, we expected that people with STBs report lower self-esteem than people without STBs. We expected large effect sizes for the associations of interest (based on the conventions by Funder & Ozer, 2019). Specifically, we expected the meta-analytic association between self-esteem and suicidal ideation (measured using a metric scale) to be about r = −.40 to r = −.50. For the group comparison between individuals with and without suicidal behavior, we expected effects of comparable size (i.e., Cohen’s ds = −0.70 to −0.80). These hypotheses were based on previous empirical research on this association (e.g., Soto-Sanz et al., 2019) and the theoretical considerations outlined above, which suggest moderate to strong negative associations between self-esteem and STBs.
Method
Transparency and openness
Preregistration
The review protocol was preregistered on the OSF: https://osf.io/fj2s8.
Data, materials, code, and online resources
To complement this preregistration, we also provide the raw data (including all coded information from the included individual studies) and the R code: https://osf.io/uqr78/. Moreover, we provide further online supplementary material (OSM) at OSF: https://osf.io/672ug/.
Literature search
The systematic literature search was performed in March 2022 (Week 2) and updated in April 2023 (Week 4) using PsycINFO through Ovid. This search engine also includes certain types of gray literature, such as dissertations. The following search terms were applied in the abstract and title: ((self-esteem OR “self esteem” OR self-worth OR “self worth” OR self-liking or “self liking” OR self-respect OR “self respect” OR self-view OR “self view” OR self-concept OR “self concept” OR self regard OR “self-regard” OR “self-opinion” OR “self opinion” OR self-perception OR “self perception”) AND (suicid* OR self-injurious OR self-injury OR “self injurious” OR “self injury” OR “self-harm” OR “self harm” OR parasuicid* OR SITB OR NSSI)). Study eligibility was determined in a two-step procedure. In Step 1, all titles and abstracts of the studies found in the systematic literature search were screened for inclusion versus exclusion. Those studies that were included in Step 1 were again consulted in Step 2. In this step, the articles were coded based on the full texts using a standardized coding manual. We prepared this systematic literature review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses standards (Page et al., 2021).
In addition to the search results from the standardized literature search, we also included eligible studies that we identified through a manual search (e.g., forward-backward search, articles included in other systematic reviews) and through a call for unpublished data via mailing distributor lists of academic groups (e.g., German Society of Psychology, International Network of Early Career Researchers in Suicide and Self-Harm) and social media.
Exclusion criteria
We applied the following exclusion criteria: (a) no measure of self-esteem available, (b) no measure of suicidal ideation or suicidal behavior, 2 (c) not an empirical-quantitative study, (d) inconsistent information on effect-size data (e.g., in abstract, text, tables, figures), (e) insufficient information to compute the effect size, (f) duplicate of another already included data set, (g) no full-text access, and (h) no English, German, or Spanish language. In the case of exclusion of duplicates, priority was given to the studies with the larger sample, and these were included. In total, only 10 studies were excluded as duplicates. For more details on the exclusion criteria, see the preregistration (https://osf.io/fj2s8). The flow diagram in Figure 1 visualizes the literature search and eligibility assessment.
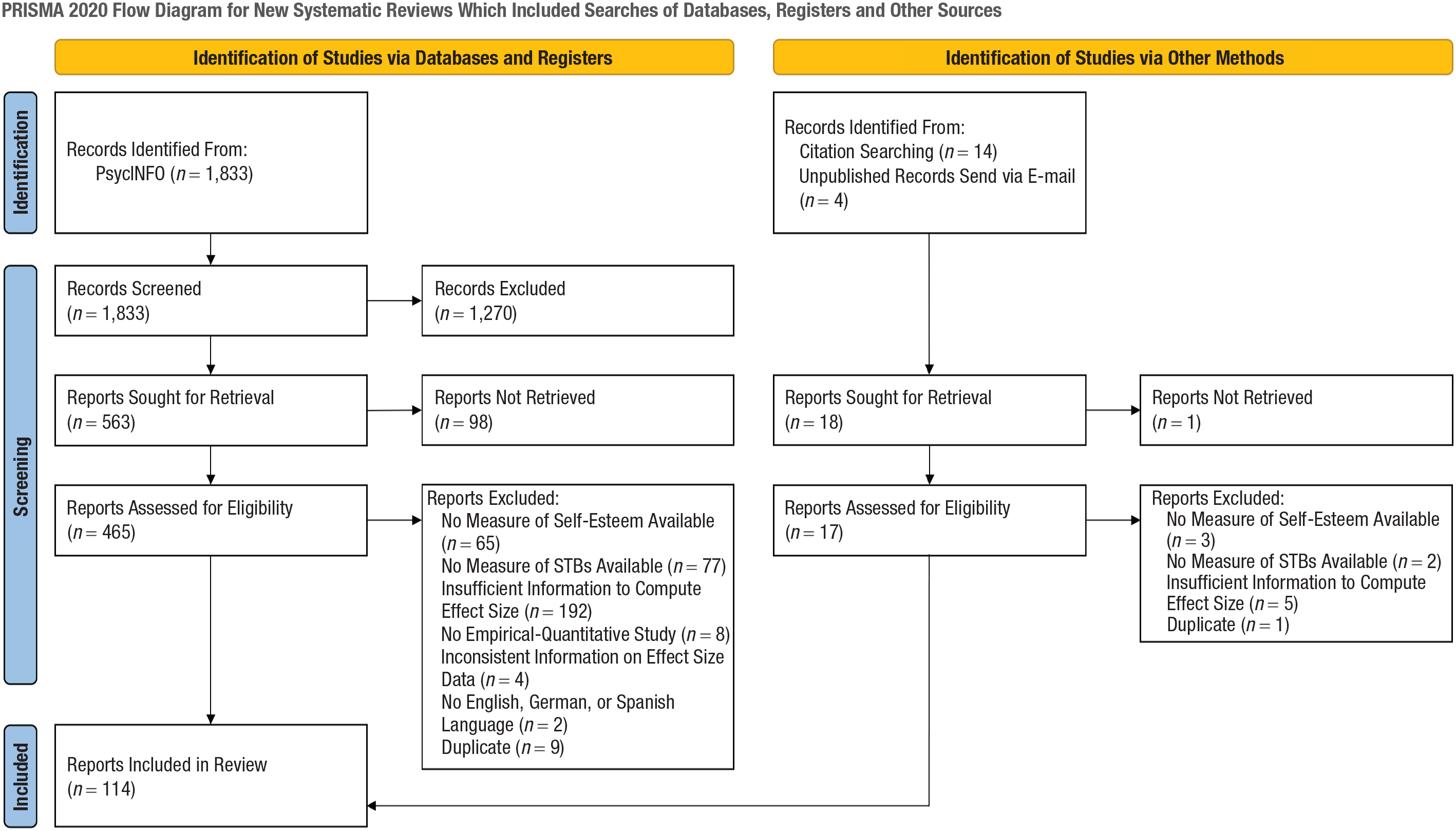
Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 flow diagram. The template of this flow diagram was adapted from Page et al. (2021). For more information, visit http://www.prisma-statement.org/.
Coding of articles
Our systematic literature search resulted in 1,833 search hits. Furthermore, 14 articles were identified by checking the reference list of the meta-analysis on self-esteem and suicidal behavior in youths by Soto-Sanz et al. (2019), and four studies were included as a result of a call for unpublished data. In Step 1, 300 articles were double-coded by three raters (i.e., Rater 1 double-coded 100 studies that were originally coded by Rater 2, Rater 2 double-coded 100 studies that were originally coded by Rater 3, and Rater 3 double-coded 100 studies that were originally coded by Rater 1). All raters had a bachelor’s degree in psychology and were trained in coding for meta-analytic studies. The interrater agreement regarding inclusion versus exclusion was above 90% for all pairs of raters.
In Step 2, in total, 482 articles were coded, and effect sizes from 114 articles were finally included in the meta-analysis. For the references of all included articles, see Table S1 in the OSM at https://osf.io/672ug/. The three coders from Step 1 plus two additional experienced researchers performed the Step 2 coding. Coding was performed using a coding manual that was defined a priori and preregistered (https://osf.io/uqr78/). For an overview of all descriptive characteristics that were coded for each included article, see https://osf.io/uqr78/. In Step 2, 25 studies were double-coded. The interrater agreement regarding the inclusion versus exclusion of articles was 88% in this step. Across all coded sample characteristics, study characteristics, and effect-size information, the average percentage of interrater agreement was 93.7% (range = 73.8%–100%; see Table S2 in the OSM at https://osf.io/672ug/). The rare cases of disagreement between the coders were solved by discussion and joint consultation of the original article.
In cases in which necessary information for the inclusion of a study was missing in the published article (i.e., missing correlations on the relevant outcomes), the corresponding author was contacted via email (if a valid email address could be found). In total, we contacted 164 authors, of which 14 responded with the requested information and another 21 informed us that they could not provide us with the information for various reasons (e.g., they no longer have access to the data).
Quality assessment
The quality of the included individual studies was assessed with respect to the following criteria: (a) Were the inclusion criteria for the sample clearly defined? (b) Were the study participants and setting described in detail? (c) Was the selection process such that the recruited subjects represented the target population? (d) Was self-esteem measured validly and reliably? (e) Were STBs measured validly and reliably? and (f) Was the statistical analysis appropriate and robust (i.e., for correlations, samples of 250 or more were considered robust; Schönbrodt & Perugini, 2013). These criteria were adapted from JBI’s critical appraisal tools to assess the trustworthiness, relevance, and results of published articles (Moola et al., 2020).
Studies were evaluated based on six questions, each of which was answered with “yes” (i.e., 1 point) or “no” (i.e., 0 points). The quality was considered good if at least five criteria were met, fair if four criteria were met, and low when three or fewer criteria were met.
Final database for the meta-analyses
Because of the two different types of studies on STBs and self-esteem (i.e., correlational studies and studies with mean comparisons), we conducted two meta-analyses: one with the correlation coefficient Pearson’s r as the effect size of interest and one with the standardized mean difference (Cohen’s d) as the effect size of interest. The meta-analyses based on r comprised 101 effect sizes and overall 54,184 individuals. The meta-analyses based on d comprised 43 effect sizes and overall 62,772 individuals.
Of all included effect sizes, 102 described the association between suicidal ideation and self-esteem, 18 described the association between suicidal behavior and self-esteem, and 24 effect sizes described the association between a mixture of suicidal ideation and behavior and self-esteem (e.g., some studies use measures that combined the assessment of suicidal ideation and previous suicide attempts).
General meta-analytic procedure
If Pearson’s r was reported in the published article to represent the association between self-esteem and suicidality (both measured using a metric scale), we transformed all correlations using Fisher’s r-to-z transformation (Shadish & Haddock, 2009). To enhance interpretability and to allow comparison with other meta-analyses based on correlations, these z scores were subsequently back-transformed to r for reporting in this article.
If a standardized mean difference was reported (Cohen’s d) to represent the association between self-esteem and STBs (measured dichotomously), this effect size was used. If studies reported means and standard deviations, our preferred effect size was Cohen’s d, which was calculated based on the given descriptive information (for more details on the equations, see our uploaded analysis plan). We computed our meta-analytic estimation separately for studies reporting Pearson’s r and a standardized mean difference (or the information needed to calculate this effect-size measure). However, as a sensitivity analysis, we converted r to d using the following formulas described in Borenstein et al. (2009). More specifically, we converted Pearson’s r to a standardized mean difference d using
We estimated random-effect meta-analytic models using robust variance estimation (RVE) to account for dependency among effect sizes by using the robumeta package (Fisher & Tipton, 2015) in R (R Core Team, 2020). For more details regarding the statistical models (including sample equations for the metaregression models), see the OSM.
We originally planned and preregistered that we aim also to examine longitudinal associations between self-esteem and STBs while controlling for prior levels of these variables if at least 10 studies with at least two measurement points are available. Because our database included only four longitudinal studies, of which only one reported a longitudinal association for a control group of individuals not undergoing a self-esteem-enhancing intervention (King et al., 2021), these analyses had to be dropped.
Moderator tests
We tested several moderators of the cross-sectional association between self-esteem and STBs. We estimated the metaregression models for each moderator separately, in which one potential moderator (e.g., percentage of females in the sample) predicts the effect size (i.e., the association between self-esteem and suicidality). Categorical characteristics (e.g., sample type) are included as dummy-coded predictors. Finally, we estimated a metaregression model in which the effect size is predicted by all moderators that were statistically significant in the previously estimated separate models (thereby controlling for the overlap among different study and sample characteristics).
Outlier and publication-bias analyses
We conducted a sensitivity analysis to check if there were outliers influencing the results. If so, effect sizes were reported with and without studies removal. We used the cooks.distance function and the influence function using the metafor package (Viechtbauer, 2010; Viechtbauer & Cheung, 2010) to evaluate the existence of influencing outliers.
To examine if there is evidence of publication bias, we visually and statistically inspected the funnel-plot asymmetry using contour-enhanced funnel plots (Peters et al., 2008). The funnel plots ignore the multilevel structure of effect sizes nested in articles because no multilevel procedure for funnel plots exists. We additionally used the trim-and-fill method to iteratively adjust the funnel plot for missing (unpublished) studies until the funnel plot is symmetric (Duval & Tweedie, 2000). To statistically test the funnel-plot asymmetry, using the RVE approach, we conducted the funnel-asymmetry test (FAT), precision-effect test (PET), and precision effect estimate with standard error (PEESE) test. The FAT was conducted in the first step. For this purpose, we predicted the effect size by its standard error, which is analogous to the traditionally used Egger’s regression test (Egger et al., 1997). There is an indication of publication bias if the slope coefficient in this metaregression model significantly differs from zero. In the second step, the PET was conducted independently of the FAT results. The PET uses the same metaregression as the FAT but tests whether the intercept significantly differs from zero. If the PET intercept is not statistically significant, the intercept serves as an estimate of the overall effect, correcting for publication bias. If the PET intercept is statistically significant, the PEESE test was conducted in a third step. The corresponding PEESE intercept becomes the best unbiased overall effect estimation (Alinaghi & Reed, 2018; Stanley & Doucouliagos, 2014). For all R scripts, including effect-size calculating formulas and the raw data set used for our analyses, see https://osf.io/uqr78/.
Results
Study characteristics
Across all 114 included studies, the sample sizes ranged from 15 to 9,304 participants, with a median of 262. The mean age of the samples ranged from 7 to 73 years (M = 23.99, SD = 12.63). The proportion of females in the samples ranged from 0% to 100% (M = 58.49%, SD = 19.08%). The samples of the included studies came from 26 different countries (about 34% from North American countries, k = 43; 27% from Europe, k = 35; 12% from China, k = 15). About 39% (k = 49) of the samples predominantly consistent of White/European people, 23% (k = 29) predominantly consisted of Asian people, 5% (k = 6) predominantly consisted of Hispanic/Latin American people, 4% (k = 5) predominantly consisted of Black people, and about 12% (k = 16) reported samples with an ethnical mix (i.e., the sample did not consist of 70% or more people from one specific ethnic group). The other 17% (k = 21) of effect sizes were based on samples that were not closer described in terms of ethnicity. The majority of samples were described as community (convenience) samples (58%; k = 74).
About 18% (k = 23) of studies reported clinical samples (either inpatients or outpatients, mainly with mental-health issues). The clinical samples varied in terms of diagnoses and included, for example, participants with a bipolar spectrum disorder (e.g., Weinstein et al., 2015), schizophrenia spectrum disorder (e.g., Fulginiti & Brekke, 2015), major depressive disorder (e.g., Soylu et al., 2013), borderline personality disorder (e.g., Laporte et al., 2018), but also permanently physically disabled participants (Juriši & Marušic, 2009). Other sample types, such as college/university student samples (15%; k = 19), nationally representative samples (3%; k = 4), or other sample types, including mixed samples (6%; k = 7), were less often reported.
Almost all studies included applied measures of self-esteem and STBs with trait time frames (e.g., “in general,” “in the past 4 years,” “at any time in your life”). Eleven studies employed state time frames to measure STBs (e.g., “in the past week”; Chen et al., 2021), and only one included study employed a state time frame to measure self-esteem (“during the past 2 weeks”; Jones et al., 2014). Because of the low number of studies using a state time frame, we had to drop the moderator analyses examining whether the association between self-esteem and STB differs depending on the time frame used. Most of the included effect sizes were based on self-report measures (92%; k = 117), such as the Rosenberg Self-Esteem Scale (Rosenberg, 1965a) to examine self-esteem and the Beck Scale for Suicide Ideation (Beck, 1991) or the Suicide Behaviors Questionnaire–Revised (Osman et al., 2001) to examine STBs. A further 6% (k = 8) of the effect sizes stem from studies using clinical interviews for either STBs or self-esteem or both, and 2% (k = 2) did not specify the type of measurement.
The majority (93%; k = 118) of included effect sizes stemmed from articles published in peer-reviewed journals. The year of publication (or year of data collection in case of unpublished data) ranged from 2004 to 2023 (Mdn = 2014). When more than one sample was reported in an article, we first determined the mean values for each article to calculate these descriptive characteristics. The overall quality of the included studies was fair to good (48% good quality, 35% fair quality, 14% low quality). For a full overview of the quality-assessment results, see Tables S4 and S5 in the OSM.
Identification of outliers
We identified influential outliers in our meta-analyses of the associations between suicidal ideation and self-esteem, suicidal behavior and self-esteem, and the combination of STBs and self-esteem. Specifically, we excluded three effect sizes based on Pearson’s r but zero effect sizes based on Cohen’s d in the meta-analysis of suicidal ideation and self-esteem. Likewise, we excluded one effect size based on Pearson’s r and zero effect sizes based on Cohen’s d in the meta-analysis of suicidal behavior and self-esteem. In the meta-analysis of the association between the combination of STBs and self-esteem, we removed one effect size based on Cohen’s d and one effect size based on Pearson’s r. The results reported below correspond to the analyses after removing these outliers. For results for the full data set, see Table S6 in the OSM. The overall results were very similar regardless of whether the outliers were removed.
Association between suicidal thoughts and self-esteem
We found large and negative meta-analytic effect sizes for the association between suicidal thoughts and self-esteem in studies using Pearson’s r (i.e., studies measuring suicidal ideation and self-esteem on a metric scale) and studies using Cohen’s d (i.e., studies comparing self-esteem scores between groups high vs. low in suicidal ideation) as effect-size measure. For studies using Pearson’s r, the meta-analytic effect size was r = −.435, 95% CI = [−.469, −.400], with 82 effect sizes. For Cohen’s d, the meta-analytic effect size was d = −0.805, 95% CI = [−1.120, −0.486], with 20 effect sizes. According to Funder and Ozer (2019), these effect sizes can be considered large and clearly indicate that low self-esteem is associated with higher levels of suicidal ideation (or that people with higher levels of suicidal ideation show lower levels of self-esteem). Both meta-analytic effect-size estimates (i.e., r and d) are within the expected range or even slightly larger (preregistration: r = −.40 to r = −.50 and Cohen’s d = −0.70 to d = −0.80)
Association between suicidal behavior and self-esteem
The association between suicidal behavior and self-esteem was examined in considerably fewer studies (studies using Pearson’s r: k = 4; studies using Cohen’s d: k = 14). Consequently, this meta-analytic association can be estimated with less precision. However, we again found a strong, negative association across both effect-size types (r = −.258, 95% CI = [−.414, −.088]; d = −0.828, 95% CI = [−1.010, −0.645]) based on the conventions to interpret effect sizes by Funder and Ozer (2019). These associations indicate that low self-esteem is associated with higher levels of suicidal behavior (or that people showing suicidal behavior report lower self-esteem scores). The meta-analytic r was lower than preregistered (see above), and the meta-analytic d was within the expected range or even slightly larger. However, because of the few studies synthesized in these analyses, the meta-analytic effect sizes must be interpreted cautiously.
Associations between mixtures of STBs and self-esteem
Because some studies used measures that mix suicidal ideation and suicidal behavior (e.g., the Beck Scale for Suicide Ideation, which includes items on suicidal ideation but also items on suicide attempts; Beck, 1991), we estimated meta-analytic effect sizes for this outcome separately. For studies using Pearson’s r, the meta-analytic effect size was r = −.405, 95% CI = [−.496, −.306], with 15 effect sizes. For Cohen’s d, the meta-analytic effect size was d = −1.610, 95% CI = [−3.950, 0.733], with nine effect sizes. Note that the meta-analytic estimate based on Cohen’s d was not statistically significant, as indicated by the 95% CI including zero. Based on the studies reporting Pearson’s r, again, a large, negative meta-analytic effect size was found that fell in the expected range (as preregistered).
Longitudinal associations between self-esteem and STBs
We identified four studies that examined the longitudinal association between self-esteem and STBs (Blomdahl et al., 2022; King et al., 2021; Laporte et al., 2018; Öztürk & Ekinci, 2018). Because of this low number of studies and effect sizes, we could not meta-analyze them reliably. All four studies were treatment studies. These studies reported, for example, that baseline levels of self-esteem were correlated with suicidal ideation 16 months later at r = −.25 (King et al., 2021). The study by Blomdahl et al. (2022) examined whether a manual-based phenomenological art therapy reduces suicidal ideation and enhances self-esteem in patients with depression. However, the relation between self-esteem and suicidal ideation itself has not been examined. Using a pretest-posttest follow-up design, Öztürk and Ekinci (2018) showed that after a structured education program for improving self-esteem, suicidal ideation was significantly lower. However, no control group was used in this study, limiting its interpretability. Moreover, weekly individual- and group-therapy sessions can enhance self-esteem and reduce suicidal attempts in clinical inpatient samples with borderline personality disorder (Laporte et al., 2018). This finding underscores the potential benefits of incorporating self-esteem improvement as a module in the clinical management of borderline patients to mitigate STBs.
Assessing and correcting for publication bias
Figure 2 displays the contour-enhanced funnel plots for the six meta-analyses conducted separately for suicidal ideation, suicidal behavior, and the combination of ideation and behavior using Pearson’s r and Cohen’s d. To assess publication bias, we applied the trim-and-fill procedure (Duval & Tweedie, 2000) to identify studies that need to be added to achieve funnel-plot symmetry. The random-effect trim-and-fill procedure identified only a need for filling in studies in the meta-analysis that examined the association between suicidal ideation and self-esteem using Cohen’s d as the effect size, indicating potential publication bias.
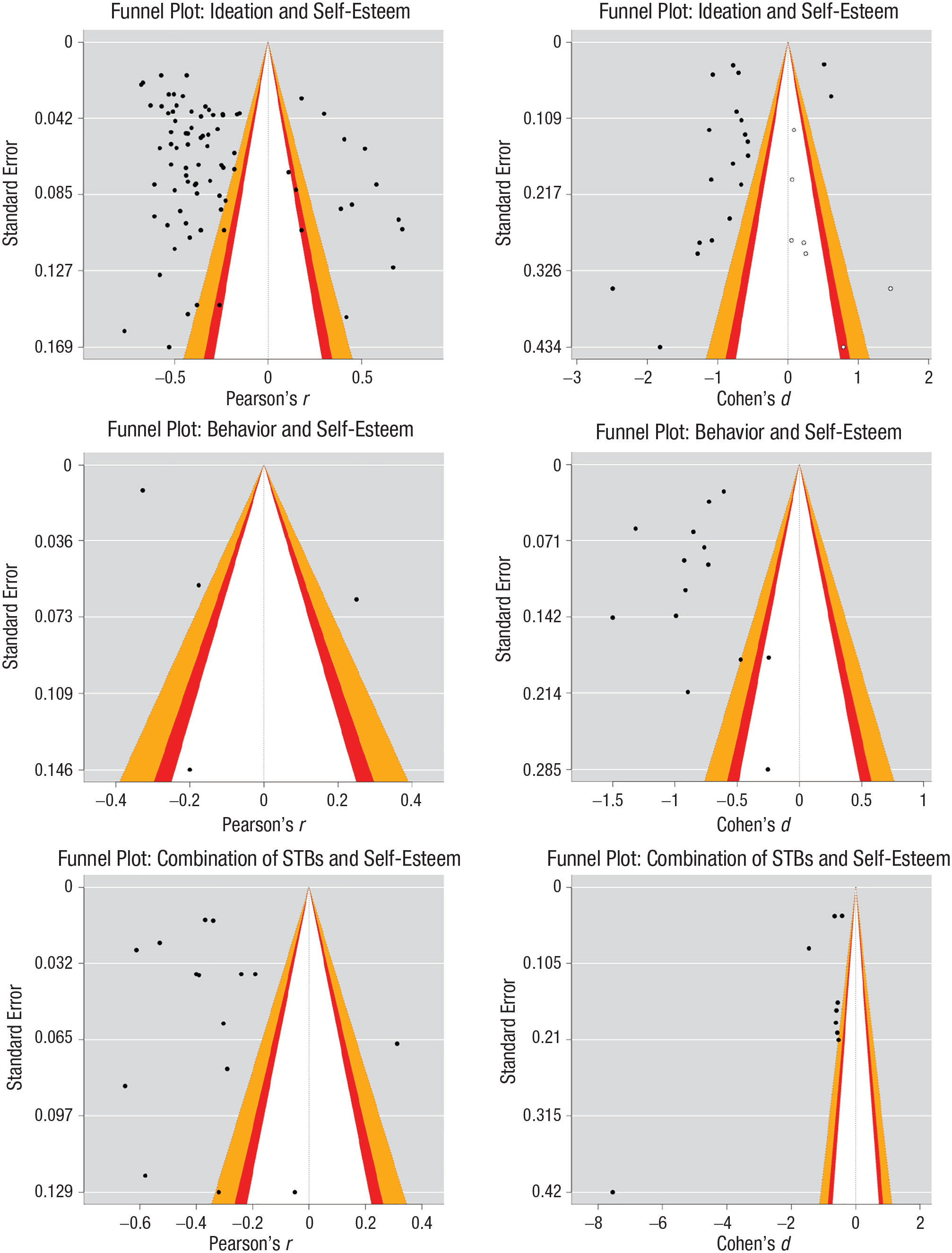
Contour-enhanced funnel plots for the six meta-analyses. Dark-colored points indicate effect sizes included in the respective meta-analysis. White points indicate estimates that must be imputed to achieve symmetry using the trim-and-fill approach (Duval & Tweedie, 2000). Contour lines allow the consideration of the statistical significance of effect-size estimates. White background color indicates p > .10, red background color indicates .05 < p < .10, orange background color indicates .001 < p < .05, and gray background color indicates p < .001.
The PET-PEESE using the RVE approach showed evidence of publication bias in the meta-analysis on the association between suicidal ideation and self-esteem using Cohen’s d, as indicated by the significant PET slope. In all other performed meta-analyses, no indication of publication bias was found. Despite this result, we used the PEESE approach for all meta-analytic models to obtain an unbiased effect-size estimate, adjusted for potential publication bias, which resulted in a more conservative estimate of the association. Table 1 presents the effect sizes adjusted for publication bias using either the PET or the PEESE intercept for each meta-analysis. Especially for the meta-analysis on suicidal ideation and self-esteem using Cohen’s d, the corrected effect size was substantially smaller (d = −0.112) than the uncorrected effect size (d = −0.799).
Comparison of Effect Sizes Uncorrected and Corrected for Publication Bias

Note: r = uncorrected Pearson’s r; r+ = Pearson’s r corrected for publication bias; d = uncorrected Cohen’s d; d+ = Cohen’s d corrected for publication bias; STBs = suicidal thoughts and behaviors.
This coefficient corresponds to the precision-effect-estimate-with-standard-error intercept.
This coefficient corresponds to the precision-effect-test intercept.
p < .05.
Overall, the study presented limited evidence of publication bias across most meta-analyses. However, for the meta-analysis on suicidal ideation and self-esteem using Cohen’s d, both the trim-and-fill and the PET-PEESE approaches indicated publication-bias issues. Therefore, the estimated overall effect in this specific meta-analysis should be interpreted with caution. This issue is also reflected in the smaller estimated effect sizes of the association between suicidal ideation and self-esteem (especially if Cohen’s d is meta-analyzed) corrected for publication bias compared with the uncorrected effect size (cf. Table 1).
Moderation analyses and robustness checks
We did not a priori specify hypotheses regarding the moderation analyses but aimed at exploring whether the associations between STBs and self-esteem are moderated by various study and sample characteristics (i.e., mean age of the sample, percentage of women in the sample, publication year, publication type, country of origin of the sample, ethnicity composition of the sample, sample type, and reliability of self-esteem and suicidality measures). The results of all moderation analyses are presented in Table 2.
Moderator Analyses
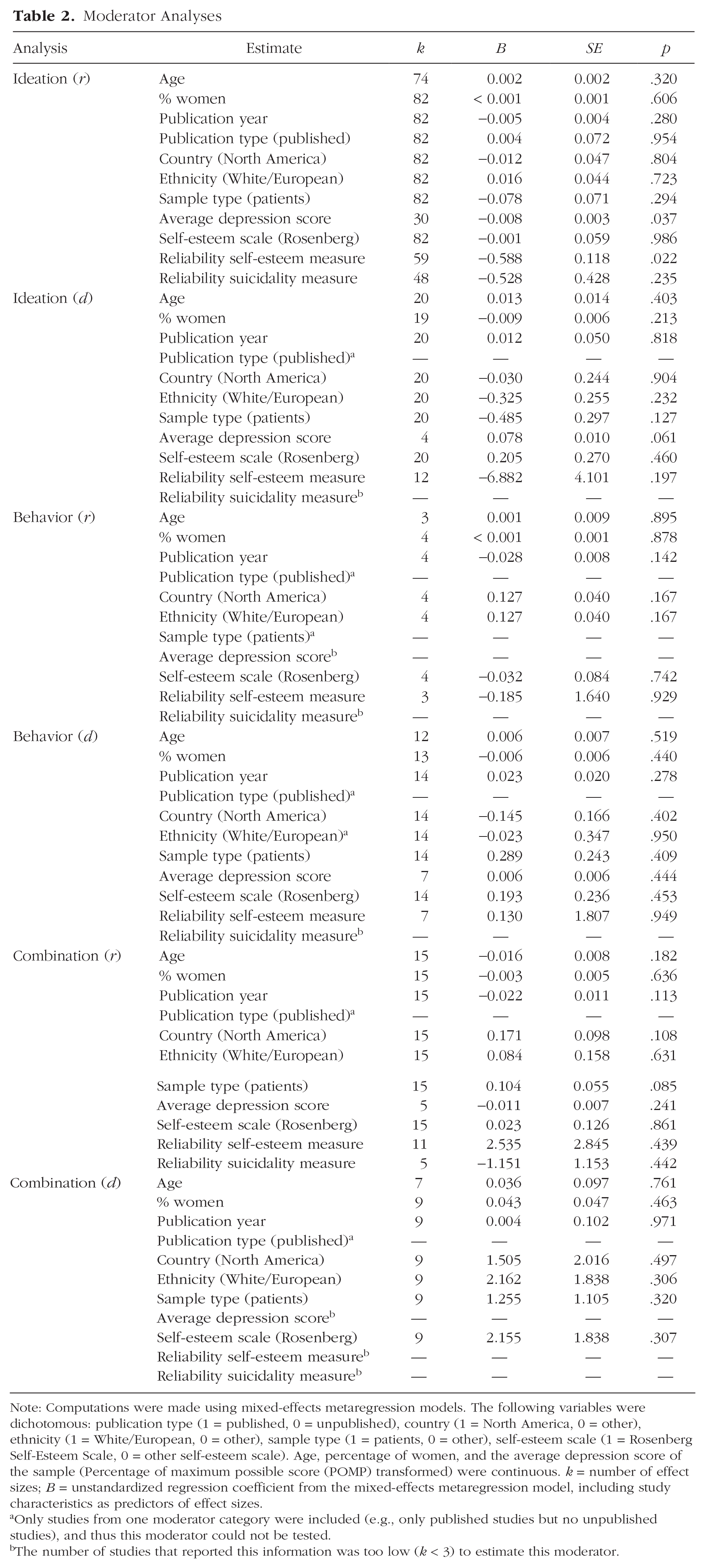
Note: Computations were made using mixed-effects metaregression models. The following variables were dichotomous: publication type (1 = published, 0 = unpublished), country (1 = North America, 0 = other), ethnicity (1 = White/European, 0 = other), sample type (1 = patients, 0 = other), self-esteem scale (1 = Rosenberg Self-Esteem Scale, 0 = other self-esteem scale). Age, percentage of women, and the average depression score of the sample (Percentage of maximum possible score (POMP) transformed) were continuous. k = number of effect sizes; B = unstandardized regression coefficient from the mixed-effects metaregression model, including study characteristics as predictors of effect sizes.
Only studies from one moderator category were included (e.g., only published studies but no unpublished studies), and thus this moderator could not be tested.
The number of studies that reported this information was too low (k < 3) to estimate this moderator.
For most of the analyses conducted, we found no significant moderation effects, indicating that the results are robust and generalizable across various study and sample characteristics. However, for the relationship between suicidal ideation and self-esteem, a significant moderation effect of the average depression score was observed. This finding suggests that higher levels of depression were associated with a more negative relationship between suicidal ideation and self-esteem. Note that this moderation effect was found only in the meta-analysis based on Pearson’s r and not in the one based on Cohen’s d, which raises questions about the generalizability of this moderation effect.
Discussion
In the present meta-analysis, we extended previous research on the association between STBs and self-esteem by (a) differentiating between suicidal ideation and suicidal behavior and (b) examining the associations across different age groups from childhood to late adulthood. In addition, this is the first meta-analysis that conducted moderator analyses to examine several sample characteristics and methodological factors that might affect the association between STBs and self-esteem.
Overall, our results fit very well with existing theories, such as the interpersonal theory of suicide (Joiner, 2005; Van Orden et al., 2010) or the fluid-vulnerability theory (Rudd, 2006): Individuals reporting low self-esteem are at a higher risk for also reporting STBs as indicated by negative associations between self-esteem and STBs. This global conclusion can be drawn for those studies that assessed STBs and self-esteem on metric scales (ideation: r = −.435; behavior: r = −.258; combination: r = −.405) and for those studies that examined mean differences in self-esteem between groups with versus without STBs (ideation: d = −0.805; behavior: d = −0.828; combination: d = −1.610). However, because we included only cross-sectional studies, the causal direction of the effect remains unclear. Generally, the precision of estimation was higher for studies measuring the constructs of interest on a metric scale because more studies could be included that did so compared with studies distinguishing groups with and without STBs.
The effects presented here align with findings from previous meta-analyses on associations between psychopathological symptoms and self-esteem. As mentioned earlier, a previous meta-analysis on the association between suicidal behavior and low self-esteem in youths reported d = 0.58, 95% CI = [0.44, 0.74] (Soto-Sanz et al., 2019). The effect size found in the present meta-analysis (d = −0.828, 95% CI = [−1.010, −0.645] and r = −.258, 95% CI = [−.414, −.088]) is slightly larger but within a similar range when considering the 95% CIs. Moreover, previous meta-analytic findings on the association between self-esteem and depression (Sowislo & Orth, 2013) reported r = −.57, 95% CI = [−.60, −.54], which indicates a slightly stronger association between self-esteem and depression compared with self-esteem and STBs as found in this current meta-analysis. The higher association between self-esteem and depression could be because self-esteem and depression are similar in their conceptual breadth, efficiently summarizing a large amount of cognitive, affective, and behavioral information (Soto & John, 2017). In contrast, STBs are rather narrowly defined constructs, which may result in stronger associations with closely matched criteria than with broader constructs (Ashton et al., 1995; Paunonen & Ashton, 2001).
Robustness and generalizability of findings
In the present meta-analysis, we tested several study and sample characteristics as potential moderators of the associations between STBs and self-esteem. The mainly nonsignificant moderation effects suggest that the results presented in this meta-analysis are robust and generalizable across different study characteristics and sample characteristics. Corresponding to the findings of Orth and Robins (2022), low self-esteem seems to be a rather global associate of STBs regardless of how old persons are or what gender they have. The only statistically significant moderation analysis indicated that average depression scores of the samples moderate the relationship between suicidal ideation and self-esteem. This finding suggests that the more depressed the participants were, the stronger and more negative the association between low self-esteem and suicidal ideation was. This means that individuals with higher levels of depression might experience a more pronounced negative impact of low self-esteem on their suicidal thoughts. Because both low self-esteem and STBs can be symptoms of depression, a co-occurrence of self-esteem and STBs is more likely in individuals reporting more severe depressive symptoms. However, the fact that this moderation effect was observed only in the meta-analysis based on Pearson’s r and not in the one based on Cohen’s d indicates potential variability in how depression moderates this relationship so that this finding should be interpreted with caution. Moreover, not all studies included in this meta-analysis provided information on the average depression score of the sample. Overall, this finding suggests that further research is necessary to confirm and better understand the conditions under which depression moderates the relationship between suicidal ideation and self-esteem.
One limitation of this meta-analysis is that we restricted our search to PsycINFO, which may have excluded relevant studies from other databases, such as PubMed, Medline, or Embase. Although PsycINFO offers extensive coverage of psychological literature and was appropriate for our research focus, expanding the search could have identified additional studies from related fields. To mitigate this, we issued a call for unpublished data, broadening the scope of our analysis beyond what the database search alone could capture. Given the substantial overlap of articles across major databases, we believe most relevant studies were included. Nonetheless, future research should consider a broader database search and explore the metascientific impact of incorporating PubMed, Medline, and Embase alongside PsycINFO in clinical-psychology meta-analyses.
Identified evidence gaps
Identifying evidence gaps, as can be done in meta-analytic reviews, is essential to strengthen the data and stimulate innovative future research. In the present meta-analysis, we identified several gaps in the literature. First, comparably few studies (k = 16) examined the association between suicidal behavior and self-esteem. Suicidal behavior occurs much less frequently than suicidal ideation (Nock et al., 2012; Voss et al., 2019). Accordingly, it is more difficult to conduct studies with individuals with suicide attempts or suicidal behavior in general because they are harder-to-reach populations than populations with suicidal ideation. The results of our meta-analysis highlight that there is a research gap regarding the association between suicidal behavior and self-esteem that should be addressed in the future. Moreover, suicidal behavior is a relatively broad category that groups together different behaviors (e.g., interrupted or aborted suicide attempts and suicides). Because of the overall rather small number of studies that have examined associations between suicidal behavior and self-esteem, it was not possible in this meta-analysis to estimate effects separately for the different forms of suicidal behavior. This finding underscores the call that more research is needed in this area to meta-analyze the different suicidal behaviors separately.
Second, more studies are needed to examine the association between STBs and self-esteem (and other risk factors) in the second half of life. Averaged across all included studies, the mean age of the samples in this meta-analysis was 24.33 years, indicating that most studies used relatively young samples. Moreover, the current evidence on the associations between STBs and self-esteem overly relies on White, educated, industrialized, rich, and democratic (WEIRD) convenience samples. Future research is needed to examine the associations among non-WEIRD samples and more diverse samples. Such studies, particularly in individuals potentially exposed to higher levels of discrimination (e.g., using sexual-minority samples or Black, Indigenous, and people-of-color samples), are crucial because discrimination can negatively affect self-esteem, potentially heightening the risk of STBs (e.g., Plöderl & Fartacek, 2005; Vélez-Grau & Lindsey, 2022). Moreover, because the sources of low self-esteem in marginalized groups might differ from those typically studied in convenience samples (Verkuyten, 2003), such research can contribute to a more comprehensive and nuanced understanding of the relationship between self-esteem and STBs.
Third, future research would benefit from systematically manipulating the time frame of STB assessments to better understand the temporal dynamics and distinguish between trait and state effects. By varying the assessment intervals, researchers can explore how short-term fluctuations versus long-term patterns influence the relationship between self-esteem and STBs. This approach could clarify whether certain risk factors are more predictive of immediate or chronic STB risk, ultimately providing more precise targets for intervention (Hamaker, 2023).
Fourth, we identified a very small number of longitudinal studies that repeatedly measured STBs and self-esteem. Some of these studies were intervention studies that did not report a control group (Laporte et al., 2018; Öztürk & Ekinci, 2018). Consequently, the prospective association between self-esteem and STBs could not be analyzed because the effect may be confounded with the effects of the intervention. As a consequence, the causal direction of the association between self-esteem and STBs estimated in this meta-analysis is unclear. There is preliminary evidence that self-esteem (measured at baseline) prospectively predicts lower suicidal ideation 16 months later (r = −.25; King et al., 2021). However, although bidirectional associations seem plausible, more longitudinal studies are needed to test this hypothesis empirically. Using longitudinal data would also allow one to test the conflicting theoretical perspectives of the vulnerability model and the scar model against each other. The vulnerability model assumes that low self-esteem is a causal risk factor for psychopathology, in which individuals that experience low levels of self-esteem have a higher risk of developing symptoms of psychopathology compared with individuals experiencing high self-esteem (Orth et al., 2016). Relatedly, Baumeister (1990) proposed that suicidal behaviors can be understood as an escape from aversive self-awareness (i.e., an individual perceives oneself as incompetent, dislikable, and inadequate—thus, has low self-esteem). In contrast, the scar model assumes that low self-esteem is a consequence rather than a cause of psychopathology. Suicidal ideation and suicide attempts are assumed to “leave scars” in one’s self-concept that progressively erode self-esteem over time (Frey et al., 2017; Liu, 2019; Wiklander et al., 2003). However, because recent research questioned the vulnerability and scar models for the association between self-esteem and depression (Sorjonen et al., 2022), it remains a task for future research to examine the temporal relationships between self-esteem and STBs with longitudinal data.
Further research directions and clinical implications
In the present meta-analysis, we focused on the between-persons associations between temporally stable SBTs and trait self-esteem. To better understand the processes underlying this association, high-resolution research examining within-persons associations between STBs and self-esteem in daily life would be effective (Santangelo et al., 2020). Such research allows the investigation of whether states of low self-esteem in daily life are risk periods for transitioning from suicidal ideation to suicidal behavior. Moreover, such research may focus on domain-specific self-esteem (e.g., in the domain of peers, family, and body image) in contrast to global self-esteem because such more specific predictors can enhance the nuanced understanding of the association between self-esteem and STBs (Ashton et al., 1995; Paunonen & Ashton, 2001).
Moreover, self-esteem is conceptually and empirically connected to depression (Haehner et al., 2024; Sowislo & Orth, 2013), and depression is often examined as a clinical diagnosis associated with STBs. The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders identifies low self-esteem as a symptom of depression (American Psychiatric Association, 2013), and various depression assessment tools include items closely related to self-esteem. An example is the Beck Depression Inventory, which features the item “I do not feel like a failure,” similar to the item, “All in all, I am inclined to feel that I am a failure” from the Rosenberg Self-Esteem Scale. Despite these connections, there are compelling reasons to consider self-esteem and depression as distinct constructs. Low self-esteem is neither a necessary nor sufficient condition for diagnosing depression (American Psychiatric Association, 2013; Sowislo & Orth, 2013). Moreover, research indicates that self-esteem and depression have different relationships with external factors, such as negative events (Hammen, 2005; Orth et al., 2016). The link between depression and STBs is not as strong as often assumed (e.g., Ribeiro et al., 2018). In addition, theoretical models on STBs do not assign a significant role to depression. According to the interpersonal theory of suicide (Joiner, 2005), depression, like low self-esteem, can lead to perceived burdensomeness and thwarted belongingness, both of which increase the risk for STBs. In the fluid-vulnerability model (Rudd, 2006), depression determines the baseline risk, serving as a background variable in this theoretical framework as well. Given the conceptual proximity between self-esteem and depression, it is crucial for future research—ideally, longitudinal studies—to clearly delineate which of these factors increases suicide risk and at what specific points in time. Understanding the temporal dynamics between self-esteem, depression, and suicidal tendencies will help identify critical periods for intervention and improve preventive strategies.
Clinically, the present results underscore the need to ask for perceptions of low self-esteem and being a burden to others in risk assessments with suicidal patients. In some patients, low self-esteem might be a relevant “suicide driver,” which must be taken into account in case conceptualization and treatment planning. Cognitive-restructuring methods (i.e., evidence gathering, discussion of cognitive distortions) might be used to challenge low self-esteem (Fennell, 2016). Different studies have shown that perceived burdensomeness is malleable through a variety of targeted (web-based) interventions (Buitron et al., 2022; Lieberman et al., 2023; Short et al., 2019). Furthermore, a recent meta-analysis on the effectiveness of self-esteem-related interventions found a small but significant effect of these strategies on reducing suicidal ideation at postintervention and 3-month follow-up (Nguyen et al., 2022). Generally, meta-analytic evidence suggests that cognitive-behavioral therapy (CBT), reminiscence-based interventions, and evaluative conditioning effectively increase self-esteem in adults; the largest effects were found for CBT (Niveau et al., 2021). Consequently, psychotherapists may use these interventions to enhance self-esteem and prevent STBs. In addition, acceptance-and-commitment therapy, which includes enhancing self-compassion and self-kindness and may help improving in psychological flexibility (Yadavaia et al., 2014), can be fruitful in protecting against the negative effects of low self-esteem (Marshall et al., 2015) and shield against STBs (Cleare et al., 2019; Per et al., 2022).
Conclusion
This meta-analysis provides strong evidence for the negative association between STBs and self-esteem across different age groups. The findings highlight the importance of addressing low self-esteem as a potential risk factor for STBs. However, the study also identified several evidence gaps, including the need for more longitudinal studies and research in non-WEIRD samples. Future studies should also investigate the mechanisms linking self-esteem and STBs and examine within-persons associations between STBs and self-esteem in daily life. Overall, the results of this meta-analysis have important clinical implications because enhancing self-esteem may be a promising strategy to prevent STBs.
Supplemental Material
sj-pdf-1-cpx-10.1177_21677026241308163 – Supplemental material for Self-Esteem and Suicidal Thoughts and Behaviors: A Meta-Analytic Review
Supplemental material, sj-pdf-1-cpx-10.1177_21677026241308163 for Self-Esteem and Suicidal Thoughts and Behaviors: A Meta-Analytic Review by Susanne Buecker, Jenny Doll, Sandra Abrantes Diaz, Peter Haehner, Frederic Berg, Aleksandra Kaurin and Tobias Teismann in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Eva Asselmann
Editor: Jennifer L. Tackett
Author Contributions
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.