
Abstract
Comparisons with social, expectation-based, counterfactual, and temporal standards may play a significant role in the maintenance of social anxiety disorder (SAD). The general comparative-processing model outlines the comparison process, encompassing comparison frequency, discrepancy, and affective/behavioral impact. For instance, an individual may frequently compare their performance to their colleagues’, perceive themselves as less competent, and consequently experience negative emotions that lead to avoidance. Two studies examined these processes across different time frames. In a 10-day ecological momentary assessment with 133 individuals with probable SAD, daily stressors and all comparison components (frequency, discrepancy, impact) were positively linked to social anxiety both between and within individuals. Additionally, comparison affective and behavioral impact were significant within-person mediators. In Study 2, which had 376 participants and included four assessments over 1 year, stable between-person effects and less consistent within-person effects were found. These findings advance our understanding of comparative thinking in SAD and may inform related therapeutic interventions.
Keywords
Social anxiety disorder (SAD) is characterized by excessive fear of negative evaluation by others, resulting in heightened anxiety before, during, and after social interactions, increased avoidance behavior, and substantial impairment in daily functioning (Stein & Stein, 2008). The cognitive model of SAD (Clark & Wells, 1995) posits that this condition arises from comparisons between an individual’s perceived social image and social or personal standards. Comparative thinking may thus play a crucial role in the development and maintenance of SAD (Goodman et al., 2021) such that fear of negative evaluation and negative self-evaluations are nourished by a perceived discrepancy to unfavorable reference frames. For instance, excessive negative self-evaluations (e.g., “I’m awkward and out of place”) and fear of negative evaluation (e.g., “Everybody must think that I’m awkward and out of place”) can be nourished by upward social comparison (e.g., “Others at work seem far more socially skilled than I am”) or upward counterfactual comparison (e.g., “If only my hands didn’t shake so easily, I’d have great conversations”). Despite valuable contributions (Aderka et al., 2013; Goodman et al., 2021), previous research on social comparison and SAD has several limitations. It has not examined multiple types of comparison standards in concert, has assessed comparisons in an undifferentiated manner, has rarely adopted a process-oriented approach, and has not examined comparison processes across different temporal frames.
In two studies, we aimed to address these gaps by examining the engagement of socially anxious individuals in social, counterfactual, expectation-based, and temporal comparison standards, as well as the within- and between-person effects of these comparisons on SAD symptoms. Drawing on previous theoretical work on social comparison (Wood, 1996), we examined comparative thinking from a process-based perspective (Morina, 2021) that has been largely neglected in research on social anxiety. This process-based perspective distinguishes between comparison frequency (i.e., frequency of engagement in comparisons), comparison discrepancy (i.e., perceived discrepancy to the standard on the comparison dimension), and comparison affective and behavioral impact (i.e., potential affective and behavioral change following comparison). Each of these facets may contribute to the maintenance or exacerbation of SAD symptoms. Specifically, frequent comparisons may heighten self-consciousness and increase monitoring of one’s social performance, whereas large comparison discrepancies may undermine self-esteem and reinforce negative self-beliefs. In turn, the affective and behavior responses (e.g., feeling distressed, avoiding social interactions, engaging in safety behaviors) may contribute to the maintenance or exacerbation of SAD symptoms over time (Gerber et al., 2018; McCarthy & Morina, 2020; Schlechter, Hoppen, & Morina, 2024).
We therefore conducted an ecological momentary assessment (EMA) study (Study 1) to examine the relationship between everyday comparative thinking, daily stress, and SAD symptoms. On a broader timescale, we ran a four-wave longitudinal study (Study 2) over a time course of 1 year to identify longer term patterns (e.g., how habitual comparative thinking predicts changes in social anxiety over time). Although affective disorders are often characterized by short-term fluctuations, we aimed to contrast the potential short-term fluctuations observed in Study 1 with the broader patterns of symptom progression and longer term stability or change in the context of comparative thinking captured in Study 2. Accordingly, we aimed to contrast short-term fluctuations, ranging from diurnal to intraweekly time frames (Study 1), with long-term patterns spanning several weeks to months (Study 2), providing valuable insights into the mechanisms of comparative thinking and SAD.
The Comparison Process
Comparative thinking is a fundamental aspect of human cognition (Festinger, 1954). The general comparative-processing model (gComp; Morina, 2021) outlines central elements of the comparison process. Broadly, comparisons can be made to upward (i.e., better-off), downward (i.e., worse-off), or lateral (i.e., similar) standards (Festinger, 1954; Wood, 1996). Engagement in comparisons serves different motives of self-enhancement, self-verification, self-assessment, and self-improvement (Helgeson & Mickelson, 1995). The comparison process begins with the selection of a standard within a given comparison domain, which can be initiated by either external or internal stimuli and can occur either spontaneously or deliberately (Wood, 1996). According to the selective accessibility model (Mussweiler, 2020), this involves forming an initial similarity or dissimilarity hypothesis that then guides a selective search for confirming information. This selective activation of information shapes the final comparison judgment and often results in assimilation or contrast effects. The basic comparison process involves three variables: the comparer’s prior mental representation of the target dimension, the mental representation of the standard, and the integration of the first and second components, which yields the comparison outcome, representing the posterior target construal of the comparer (Morina, 2021). Drawing on appraisal models (Ellsworth, 2013), gComp proposes that the evaluation of the comparison outcome depends on its relevance to the individual’s motives, values, and perceived coping capacity, leading to its appraisal as appetitive, neutral, or aversive. Comparisons deemed motivationally relevant are likely to elicit significant reactions.
In the context of SAD, important comparison domains include both social impressions (i.e., how individuals think they come across in social interactions) and overall subjective well-being. Overall well-being represents a relevant comparison domain in SAD because it directly relates to individuals’ perceptions of their life satisfaction, emotional state, and overall functioning, areas often evaluated negatively by those with SAD (Stein & Stein, 2008). For instance, an individual might compare themselves with a colleague regarding how socially confident they appear during work interactions. The dimension here is social impression, the target is the individual’s own social impression, and the standard is their colleague. In this process, the individual examines the (dis)similarities between their own perceived confidence (i.e., the target of the comparison) and that of the colleague (i.e., the standard), yielding a comparison outcome that captures the perceived discrepancy between the target and the standard. In this example, the individual believes they appear less socially confident than their colleague. Thus, the direction represents an upward comparison. As a result, the individual may experience negative affect and heightened self-consciousness, followed by social anxiety. These cognitive and emotional responses can also influence subsequent behavior and emotional states associated with SAD, such as avoidance (Cuming et al., 2009). Similarly, the individual may compare their current well-being to other standards, such as their past well-being (e.g., “I used to feel better than I do now”) or their expected well-being (e.g., “At this stage of my life, I should be doing much better than I am”), all of which may further aggravate SAD symptoms.
Comparison Types
According to self-awareness theory (Duval & Wicklund, 1972), heightened self-focus in social situations increases sensitivity to discrepancies between the self and relevant standards, driving comparative processes that shape emotional and behavioral responses. In individuals with SAD, an increased self-focus may intensify engagement in comparative thinking. Social comparison is the most studied form of comparative thinking (Festinger, 1954; Gerber et al., 2018). Individuals with SAD may frequently engage in social comparison with others who they perceive as more socially competent, driven by heightened self-awareness in social situations, a fear of negative evaluation by others, and the endorsement of unrealistic social standards (Aderka et al., 2013; Antony et al., 2005; Clark & Wells, 1995). Unfavorable social comparisons may reinforce perceptions of social inadequacy, validate social anxieties, and contribute to anticipatory anxiety about potential negative outcomes in social interactions (Aderka et al., 2013; Morrison & Heimberg, 2013). Additionally, individuals with SAD may engage in expectation-based comparison (Higgins, 1996; Lewin, 1951), for example, by often concluding that they came across worse than they should have in social interactions (Aderka et al., 2013; Clark & Wells, 1995). Individuals with SAD may also use counterfactual comparisons (Kahneman & Miller, 1986) by contemplating how past social events could have unfolded more favorably and how their current life would differ if these counterfactual scenarios were true. This can lead to negative social emotions such as shame or embarrassment. Last, temporal comparisons (Albert, 1977) may also play an important role in SAD. For example, a past temporal comparison assessing one’s current well-being against that of “two years ago,” when they may have been less socially anxious, can evoke a sense of loss or hopelessness, potentially worsening SAD symptoms. Likewise, a prospective temporal comparison with anticipated selves (e.g., “I will be doing worse in the future than I am now”) may reflect anticipatory anxiety, catastrophic thinking, and negative self-fulfilling prophecies.
According to gComp (Morina, 2021), comparisons can be categorized as appetitive, neutral, or aversive depending on how the comparison outcome (downward, lateral, upward) aligns with the comparer’s underlying motivation. Drawing on Dweck (2017), gComp defines motives broadly, encompassing basic needs, values, and goals. Comparison outcomes are perceived as appetitive when they align with the comparer’s motives, neutral when perceived as irrelevant, and aversive when perceived as a threat. Thus, although an individual may engage in a comparison for self-evaluative purposes, the comparison outcome (e.g., “Others are doing better than I am”) can still be experienced as aversive if the resulting information negatively impacts self-relevant needs, values, or goals. Upward comparisons are typically perceived as aversive and downward comparisons as appetitive. However, downward prospective temporal comparison is an exception to this rule because anticipating future decline is usually perceived as aversive rather than appetitive. Overall, upward social, past temporal, counterfactual, and expectation-based comparisons, as well as downward prospective temporal comparisons, represent aversive comparisons (Morina & Schlechter, 2023; Morina et al., 2023). Although individual reactions may vary depending on context and interpretation, these comparison types are generally more likely to challenge self-relevant needs, values, or goals and elicit negative affect. Because aversive comparisons (rather than appetitive comparisons) have been linked more strongly to negative mental-health outcomes in prior work (Morina et al., 2023) and given the current research focus on the interrelations between comparisons and SAD, this work solely focused on aversive comparison types.
Prior Research
Existing studies on the relationship between comparative thinking and SAD have primarily focused on social comparison or social rank (Aderka et al., 2013; Gilbert, 2000; Weisman et al., 2011). The available studies indicate that individuals with social anxiety report higher comparison tendency or frequency and lower social ranking (i.e., between-person differences). One study investigated counterfactual thinking and found that individuals with social anxiety reported more upward counterfactual thoughts than individuals without social anxiety (Monforton et al., 2012). Despite valuable contributions, most prior studies have been limited by their reliance on retrospective assessments and cross-sectional research designs (Aderka et al., 2013; Gilbert, 2000; Weisman et al., 2011). These limitations may have introduced memory biases in the reports of comparative thinking, and they also preclude insights on within-person effects (e.g., Jiang & Ngien, 2020). “Within-person effects” refers to fluctuations within an individual on a given assessment and can be directly related to engendered emotional responses. For instance, comparing more frequently than one’s own usual baseline may lead to a noticeable increase in the comparer’s SAD symptom levels.
EMA is an ideal methodological approach for investigating how comparison processes unfold in naturalistic settings and affect SAD symptoms (Arigo et al., 2020). In EMA, participants report their thoughts, feelings, and behaviors multiple times per day in response to pre-established prompts, offering a nuanced understanding of between- and within-person effects. We are aware of two studies that used diary approaches or EMA in the context of social comparison or social ranking and SAD. In a 2-week diary study, Antony et al. (2005) found that individuals with SAD engaged in more upward social comparison than individuals without SAD. Goodman et al. (2021) conducted a 3-week daily diary study with undergraduates and a 2-week EMA study involving adults diagnosed with SAD and a nonclinical control group and assessed social ranking (e.g., indicating whether one feels inferior/superior or incompetent/competent relative to other people). In this study, social anxiety was associated with less favorable and more fluctuations of social ranking. The association between social ranking and momentary affect/social anxiety was stronger in individuals with elevated trait social anxiety compared with less socially anxious participants.
Given that Goodman et al. (2021) found considerable fluctuations in social ranking, it is important to investigate how within-person fluctuations are linked to daily stressors. In particular, when facing daily stressors, individuals may engage in more unfavorable thought patterns. Research indicates that individuals with SAD tend to display greater stress sensitivity (Farmer & Kashdan, 2015) and more anxiety when facing social stress (Klumbies et al., 2014). This stress-induced sensitivity may contribute to an increase in aversive comparisons and a more negative affective impact via several potential pathways. Overall, individuals are more likely to engage in comparisons when confronted with uncertainty or negative emotions, driven, for example, by motives of self-assessment or self-enhancement. For individuals with social anxiety, exposure to challenging social situations may heighten comparison engagement during pre-, peri-, and postevent processing.
In these postulated dynamics, it is relevant to examine whether individual difference variables such as avoidance or safety behavior (Cuming et al., 2009), attitudes toward social comparison (Schlechter, Meyer, & Morina, 2024), or perfectionism (Newby et al., 2017) influence within-person fluctuations of comparative thinking and SAD symptoms. Safety behaviors maintain anxiety by preventing disconfirmation of negative beliefs, potentially strengthening the impact of comparative thinking on SAD symptoms (Cuming et al., 2009). Attitudes toward social comparison reflect individuals’ motivational orientation toward comparison, which may intensify emotional and cognitive responses to social comparisons (Schlechter, Meyer, & Morina, 2024). Perfectionism, characterized by excessively high standards and self-critical evaluations, can amplify vulnerability to negative self-relevant information obtained through comparison, thereby exacerbating social anxiety (Shafran & Mansell, 2001). On the basis of these considerations, we hypothesized that these variables would moderate the relationships between comparative thinking and SAD symptoms, intensifying the associations among individuals exhibiting higher levels of these individual difference variables.
Aims of Current Research
This project sought to advance this line of research in at least five ways. First, building on prior work that broadly examined social comparison without focusing on specific dimensions, we focused on two comparison domains particularly implicated in SAD: social impressions (i.e., how people think they come across) and well-being. Second, whereas prior work has been limited to social comparison, we took a more comprehensive approach to studying comparative thinking by incorporating assessments of expectation-based, counterfactual, and temporal comparisons beyond social comparison. Third, we examined various components of the comparison process in SAD, namely comparison frequency, discrepancy, and affective and behavior impact (Morina, 2021). Our main model posits that comparison frequency leads to increased perceived discrepancy, which then influences affective and behavioral outcomes related to social anxiety symptoms. Specifically, frequent engagement in comparisons heightens sensitivity to information that emphasizes discrepancies, thereby making self-other differences more salient. This process is supported by prior research demonstrating a strong correlation between comparison frequency and perceived discrepancy (rs > .50; Schlechter, Hoppen, & Morina, 2024). Theoretically, we assume that discrepancy represents an appraisal that is contingent on the occurrence of comparisons, in line with appraisal models (Moors et al., 2013; Morina, 2021). Moreover, we assume comparison frequency to be shaped by motivational factors (e.g., Gregg et al., 2011; Sharot & Sunstein, 2020), whereas discrepancy emerges as a downstream outcome in the comparison process. Accordingly, greater perceived discrepancy is likely to elicit negative affective responses, potentially contributing to fluctuations in SAD symptoms. Fourth, we incorporated prior findings on daily stressors by examining their role in comparative thinking and SAD symptoms. Fifth, we combined a daily-level EMA study with a 1-year-long longitudinal study, allowing a more comprehensive investigation of comparative thinking, daily stress, and SAD symptoms across different time scales.
Overview of the Current Studies
Study 1 was a preregistered 10-day EMA study comprising three daily assessments. For individuals with elevated SAD symptoms, these assessments were complemented by a baseline, post-EMA, and 3-month follow-up assessment. We applied a validated clinical cutoff to select participants with elevated SAD symptoms (Peters et al., 2012), focusing on individuals most relevant to the study’s aims. This allowed us to focus on a sample more representative of individuals likely experiencing meaningful social anxiety. Specifically, we investigated how aversive social, expectation-based, and counterfactual social impression comparison frequency, perceived discrepancy, and affective impact are related to daily stressors, SAD symptoms, and mood (our secondary outcome variable). Hypotheses were preregistered.
Study 2 was conducted over the course of 1 year, with data collected at four measurement points. Here, we investigated the longitudinal relationship of aversive well-being comparison frequency, discrepancy, and affective impact and SAD symptoms in the general population. The study protocol was preregistered.
Our main hypotheses were based on the gComp framework (Morina, 2021). Primary hypotheses for both studies posited that higher comparison frequency, discrepancy, and negative affective impact would be positively associated with SAD symptoms at the between-person level. At the within-person level, we expected that daily assessment (Study 1) or measurement points (Study 2) with higher-than-usual comparison frequency, discrepancy, and negative affective impact would be positively associated with SAD symptoms. We further hypothesized that the relationship between comparison frequency and SAD symptoms would be mediated by within-person discrepancy and negative affective impact. In addition, in Study 1, we expected that individuals experiencing more daily stressors relative to their own baseline would report more SAD symptoms than usual and that this relationship would be mediated by a higher comparison frequency. We further examined whether individual differences in safety behaviors, negative attitudes toward social comparison, and perfectionism would moderate the outlined relationships between the variables. As an additional exploratory research question, we examined whether the behavioral impact of comparison (i.e., perceived self-reported changes in behavior because of comparisons) would be associated with SAD on a between- and within-person level and whether behavior changes would mediate the within-person relationships between comparison frequency and SAD symptoms as well as comparison affective impact and SAD symptoms.
Transparency and Openness
Preregistration
Study 1 was fully preregistered, including study details and our hypotheses (https://osf.io/a4ukc/?view_only=6ce423f4354248d2a4cd02cfc580a5c1). Results pertaining to the main hypotheses (cf. supra) are presented here, whereas additional preregistered analyses can be found in the Supplemental Material available online. Study 2 was also preregistered (https://osf.io/6mgv2/?view_only=210f65b330da490e82289db5be996878) and is part of a broader research project focusing on SAD symptoms among various other constructs. Our specific hypotheses for Study 2 were not preregistered. We report the data pertaining to the hypotheses of Study 2 here.
Data, materials, code, and online resources
All data and code for reproducing this study are available on OSF (https://osf.io/jqpf2/?view_only=c5f3ec961fd944289e369c38ffd70689).
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Ethical approval
Both studies were approved by the University of Münster Faculty of Psychology and Sports Science Ethics Committee and were carried out in accordance with the provisions of the Declaration of Helsinki.
Method
Study 1
Participant recruitment
English-speaking participants were recruited online via Prolific (Palan & Schitter, 2018). This platform allowed us to reach a broad range of participants, and research suggests that the data quality obtained from Prolific is generally high (Douglas et al., 2023). Prolific’s participant pool consists of people from most of the 38 Organisation for Economic Cooperation and Development countries. To qualify for screening in this study, participants were required to reside in the Central European time zone (± 1 hr) to allow an efficient dissemination of study reminders. In addition, they had to be at least 18 years old and speak fluent English. Participants who reported being on vacation during the data collection period were not eligible because we did not expect reliable participation of these participants. Data were collected using the online survey software formR (Arslan et al., 2020). Of the 551 participants who started the screening, 501 provided their informed consent to participate in the study. Several quality and plausibility checks were done: One participant was excluded because of missing data, two for failing attention checks, 19 for completing the survey too quickly (under 2.5 min), and one for providing implausible responses (i.e., having no variance in their data).
Initial screening
For the main EMA study, only participants who met the screening criteria for probable SAD were invited to participate. The cutoff values for eligibility were a score of 7 or higher on the six-item Social Interaction Anxiety Scale (SIAS-6) and a score of 2 or higher on the six-item Social Phobia Scale (SPS-6; Peters et al., 2012). As a result, 293 participants were invited to participate.
Sample size considerations and participant flow
The preregistered target sample size for the main EMA study was at least 100 participants. We conducted an a priori power analysis for intensive longitudinal data accounting for temporal dependencies (Lafit et al., 2021). Expected effects and estimates (e.g., variance of random intercept) were derived from our previous EMA work (Schlechter et al., 2025) as well as from Goodman et al. (2021) both for the between- as well as the within-person level. This analysis indicated sufficient power to detect such effects with 100 participants while also considering the length of the study (10 days) as well as financial restrictions. Thirty measurement points (i.e., 10 days with three assessments each) were chosen to balance minimal burden on participants while maintaining sufficient statistical power on the within-person level. Study spots were allocated on a first-come, first-served basis among eligible candidates. One hundred forty-one participants provided their informed consent and completed the baseline survey. One participant later requested to be excluded. Two participants were excluded for failing at least two of three attention checks, and one participant was excluded for completing the survey unrealistically quickly and displaying an unusual response pattern (as detected with the careless package in R; Ward & Meade, 2023; Yentes & Wilhelm, 2021). Four participants did not participate in the EMA phase and were removed from the analysis. The final sample thus consisted of 133 participants. Figure S1 in the Supplemental Material visually illustrates the successive exclusions of participants.
Compensation
Participants were compensated at least £8 per hour for their participation. There was a tiered compensation system (only screening, baseline, and postsurvey: £10; screening, baseline, and follow-up survey + 20% of EMA measurements: £15; screening, baseline, and postsurvey and ≥ 50% completion of the EMA phase: £20; screening, baseline, and postsurvey and ≥ 80% completion of the EMA phase: £25; participation in all components: £30; additional participation in the follow-up survey 3 months later: £5).
Procedure
The study consisted of five parts: a screening prestudy to determine eligibility criteria (5–7 min), a baseline survey (approximately 25 min), the EMA phase with 30 measurements over a 10-day period with three measurements per day (morning, noon, and evening; 2–3 min per measurement), a postsurvey on the day after the EMA phase (approximately 25 min), and a follow-up survey 3 months later. Data collection for the screening occurred from April 24 to April 25, 2024, whereas the EMA phase took place from May 4 to May 26, 2024. At the start of the baseline survey, participants received detailed information about the study. After reviewing this information, they provided informed consent and then answered the baseline survey questions. By providing their Prolific ID, they were eligible to receive invitations for the subsequent survey measurements at scheduled times (9 a.m., 2 p.m., and 7 p.m.; note that these times deviated 1 hr from our preregistration because they were deemed more feasible in the different time zones) via the Prolific chat for the following 10 days. If participants did not respond within 2 hr of receiving an invitation, the corresponding assessment was omitted. The fixed sampling schedule, inviting participants to complete the survey three times daily at consistent times with a 2-hr response window, facilitated integration into their daily routines (for recommendations on EMA studies, see Fritz et al., 2024).
Participants
Participants’ age ranged from 18 to 60 years old (M = 28.32 years, SD = 7.35). Overall, 54% identified as male. Participants were from 18 different countries and held 23 different nationalities, with one participant reporting a dual nationality. Additional demographic information can be found in Table S1.
Measures
The complete list of assessed variables is available in the preregistration. For clarity, only the measures analyzed in the current work are reported here. In this examination, we mainly focused on the results from the baseline survey (e.g., individual difference variables) and the EMA phase (e.g., daily comparative thinking, daily stressors, and SAD symptoms). Data from the follow-up assessments were not used in this study. A full list of all items used in the current contribution can be found in the Supplemental Material.
Screening
The SIAS-6 (Peters et al., 2012) was used to assess the fear or discomfort individuals experience in social interactions. The SIAS-6 consists of six items (e.g., “I find it difficult mixing comfortably with the people I work with”), and response options range from 0 (not at all characteristic or true of me) to 4 (extremely characteristic or true of me). A cutoff value of ≥ 7 is indicative of probable SAD (Peters et al., 2012). For the SIAS-6, the internal consistency (α) in the current study was .88.
The SPS-6 (Peters et al., 2012) was applied to assess subjective experience of anxiety in social situations. The SPS-6 comprises six items, and respondents rate their agreement with statements concerning various aspects of SAD symptoms (e.g., “I worry I might do something to attract the attention of other people”). The response format is the same as for the SIAS-6. A cutoff value of ≥ 2 is indicative of probable SAD (Peters et al., 2012). For the SPS-6, internal consistency (α) in the current study was .91.
Baseline assessment
To assess individual differences in safety behaviors, negative attitudes toward social comparison, and perfectionism, we used the Subtle Avoidance Frequency Examination (Cuming et al., 2009), Attitudes Toward Social Comparison Inventory (Schlechter, Meyer, & Morina, 2024), and the Short Form of the Revised Almost Perfect Scale (Rice et al., 2014), respectively. We describe the measures in detail in Supplemental Material 1.
EMA phase
To maintain our focus on the most clinically relevant comparison types and to minimize participant burden, we limited assessments to upward social, expectation-based, and counterfactual comparisons in Study 1. Note that temporal comparisons were assessed only in Study 2 because they were considered more integral to the domain of well-being comparisons as examined in Study 2. We assessed upward social, expectation-based, and counterfactual comparisons with one item, each of which was based on the Comparison Standards Scale for Appearance (Morina et al., 2023). The comparison dimension was adjusted to reflect how participants perceived their own impression in social interactions. Regarding comparison frequency, participants were asked to indicate how often they had engaged in such comparisons since the last measurement on a scale from 0 (not at all) to 5 (very often). Items were preceded by a questions such as, for example, “If you reflected on how you come across to others and the impressions you have made since the last assessment, how often have you compared yourself with others who you think made better impressions on others than you?” The precise formulations varied across assessment points to specify the time frame (i.e., morning assessment: “since yesterday evening”; midday: “since this morning”; evening: “since this afternoon”). If participants scored an item ≥ 1 (i.e., indicating at least some engagement in the respective comparison type), they were subsequently asked three questions. First, participants were asked to indicate on a scale from 0 (not at all) to 5 (much better) how much better they thought they came across than others. Second, for the perceived comparison affective impact on participants’ emotional state, we asked participants to indicate on a scale from −3 (much worse) to +3 (much better) how the comparison had made them feel since a specific time frame (e.g., the previous night, the last assessment). Third, for the perceived self-reported impact of the comparison on participants’ behavior (i.e., perceived behavioral influence), we asked participants to indicate on a scale from 0 (not at all) to 5 (very much) to what extent the comparison had influenced their behavior since a specific time frame (e.g., the previous night, the last assessment). Given their conceptual overlap and shared patterns in prior work, social, expectation-based, and counterfactual comparisons were treated as one construct of upward comparisons (Morina & Schlechter, 2023; Morina et al., 2023). Across all observations, Cronbach’s alphas were .86 for comparison frequency (between-person ω = .86, within-person ω = .70); .84 for comparison discrepancy (between-person ω = .85, within-person ω = .66); .79 for perceived comparison affective impact (between-person ω = .80, within-person ω = .69); and .88 for perceived comparison behavior (between-person ω = .89, within-person ω = .76).
Daily stress was assessed with the Daily Inventory of Stressful Events (Almeida et al., 2002). This scale captures different potential daily stressors with seven items on a dichotomous yes/no scale (e.g., “Since last night did you have an argument or disagreement with anyone?”). Cronbach’s alpha across all observations was .56 (between-person ω = .64, within-person ω = .46).
Daily social anxiety was assessed with three items adapted from validated social anxiety scales previously utilized in EMA studies (Goodman et al., 2021; Kashdan & Steger, 2006). We used this scale to assess the core aspect of social anxiety with three items on a scale from 0 (not at all) to 7 (very much). An example item reads “Since the last assessment, I worried about what other people thought of me.” Cronbach’s alpha across all observations was .91 (between-person ω = .91, within-person ω = .85).
Negative mood was assessed with the short version of the Positive and Negative Affect Schedule (PANAS; Thompson, 2007) comprising five negative mood items. Participants rated items on a scale from 1 (not at all) to 5 (extremely) on the basis of their feelings since the last assessment. Alongside the five PANAS emotions, we added the adjective “stressed” to assess the stress level of the participants. Notably, although comparison affective impact was assessed by asking participants about change in affect as a result of the respective comparison, the PANAS assessed overall negative affect between measurements. To avoid misunderstanding, we use the term “mood” to refer to negative affect measured with the PANAS. Cronbach’s alpha across all observations was .86 (between-person ω = .90, within-person ω = .81).
Analysis procedure
Analyses were conducted in R (Version 4.5.1; R Core Team, 2025) using the lme4 package for fitting mixed-effects models (Bates et al., 2009). We used multilevel models to account for the hierarchical data structure, with measurements (Level 1) nested within individuals (Level 2). Specifically, these models examined how comparison frequency, discrepancy, and affective impact predict social anxiety disorder symptoms (primary outcome) and negative mood (secondary outcome). Throughout our main models, the comparison variables (frequency, discrepancy, or affective impact) served as a time-varying predictor with two components: a trait variable (representing between-person differences) and a state variable (representing within-person deviations). The trait variables were obtained by centering the variable to the sample mean, whereas the state variables were derived by centering to the individual means. We initially fitted an unconditional means model to obtain information about the extent of total variance present in the outcome variable, partitioning it into within-person variance and between-person variance. By computing the intraclass correlation (ICC) as the ratio of the random intercept variance (between-person) to the total variance, we assessed the proportion of variance attributable to between-person variation. When there was sufficient within-person variance, we proceeded with fitting the multilevel models. Random-intercept and random-slope models were then calculated using the restricted maximum likelihood (Bates et al., 2009) and incorporating both state and trait components as predictors. These models were used to test our first set of hypotheses. To examine temporal associations between momentary predictors and social anxiety, we extended our multilevel models by including lagged state-level predictors. Specifically, for each model, the within-person predictor was lagged by one measurement occasion within each participant. This allowed us to test whether momentary experiences at Time t − 1 predicted social anxiety at Time t. We also included lagged social anxiety as a covariate to account for autocorrelation and better model change in social anxiety over time.
To test our hypothesized within-person mediation effects, we used multilevel structural equation modeling. Specifically, we examined whether the within-person relationship between state comparison frequency and the outcomes was mediated by within-person differences in comparison discrepancy or comparison affective impact and whether the within-person relationship between daily stressors and social anxiety was mediated by comparison frequency. To estimate 99% confidence intervals (CIs) for the indirect effects, we used bootstrapping resampling with 10,000 iterations. We also exploratorily tested whether interindividual difference variables (i.e., safety behaviors, attitudes toward social comparison, and perfectionism) assessed at baseline moderated the outlined relationships between the variables (for results, see Supplemental Material 2). We set α at .01 as preregistered.
Study 2
Procedure
We conducted a four-wave longitudinal study over 1 year, with assessments every 3 months. We opted for four assessments across 1 year to balance the ability to capture longer term symptom trajectories with a minimization of participant burden and potential attrition, as recommended for clinical longitudinal research (Gustavson et al., 2012). Before starting our survey, all participants provided informed consent and received detailed information concerning data protection and general information about participating. At each time point, participants completed a battery of questionnaires, including measures of aversive well-being comparison and mental-health outcomes. The questionnaires were implemented in the survey platform Unipark. Participants were recruited through Prolific (Palan & Schitter, 2018). Prolific requires a minimum hourly reward of £6, which participants received at each wave. For demographic information, we assessed age, gender, country of origin, country of residence, marital status, education, monthly income, and subjective socioeconomic status. The first survey wave began on January 25, 2024, followed by the second on April 18, 2024, the third on July 15, 2024, and the fourth on October 14, 2024. The average survey duration was 20.70 min (SD = 8.95) for Time 1 (T1), 17.19 min (SD = 8.04) for Time 2 (T2), 16.44 min (SD = 7.86) for Time 3 (T3), and 16.38 min (SD = 7.80) for Time 4 (T4).
Sample size considerations
Sample size considerations were based on three factors: recruitment challenges, financial constraints, and heuristic considerations (Lakens, 2022). Determining a sample size a priori was challenging given the complexity of the models to be tested and practical constraints (i.e., financial resources for participant compensation). Therefore, at each time point, we aimed to recruit 400 participants, accounting for dropouts across subsequent waves to ensure a sufficient number of participants at each stage to produce stable parameter estimates (Schönbrodt & Perugini, 2013; Wolf et al., 2013).
Exclusion
Initially, NT1 = 452, NT2 = 384, NT3 = 371, and NT4 = 338 individuals provided informed consent. As preregistered, we examined our data for careless/inconsistent responding to our online survey (Curran, 2016; Ward & Meade, 2023) using the careless package in R (Yentes & Wilhelm, 2021). In addition, we excluded participants who needed less than 2 s to respond to an item because this is indicative of careless responding (Bowling et al., 2023). Moreover, participants were excluded if their completion time exceeded the mean by 2.50 SDs because this may indicate interruptions during survey participation. Participants were also excluded if they failed at least two of three attention checks. Participants were excluded because of missing demographic data and/or only participating at one time point. Figure S2 shows a flowchart of participant exclusion.
Participants
Table S2 summarizes demographic data across four time points with sample sizes decreasing from T1 (N = 376) to T4 (N = 306). Mean age (from 33.29 to 34.74 years) and gender distribution (approximately 61% male, 39% female) were consistent over time. Most participants held a bachelor’s degree (approximately 45%) or higher (approximately 16% to 18% postgraduate), whereas lower education levels were rare. Marital status remained stable, with most participants being single/never married (approximately 55% to 57%) or married/in a domestic partnership (approximately 40% to 42%). Around 8% to 10% were in psychological treatment across the time points. Dropout analysis revealed that participants who only took part at T1 did not differ in any demographic variables or social anxiety levels compared with participants who took part at two time points or more. There was only a trend that males were more likely to drop out (p < .02).
Materials
The full list of the assessed variables can be found in the preregistration. Here, we report only the measures analyzed in the current work. The SIAS-6 and SPS-6 (Peters et al., 2012) were again applied to assess symptoms of social anxiety. We used one sum score of both scales as a proxy of social anxiety. Internal consistency (α) ranged from .93 to .94.
The Comparison Standards Scale for well-being (CSS-W; Morina & Schlechter, 2023) was used to assess aversive well-being comparisons (for all items, see the supplemental material). The CSS-W comprises three parts: 14 obligatory items that assessed the frequency of well-being comparisons in the past 3 weeks on a scale from 0 (not at all) to 5 (very often), 14 optional subitems that assessed the discrepancy compared with the standard on a scale from 0 (not at all) to 5 (much better/worse), and 14 optional subitems that tapped into the affective impact on a bipolar scale from −3 (much worse) to +3 (much better). Optional items were presented only when the frequency question was answered with a score of 1 or higher. In the validation study (Morina & Schlechter, 2023), the structure of the CSS-W revealed two correlated latent factors: aversive comparisons (defined as potentially threatening the comparer’s motives) and appetitive comparisons (defined as potentially aligning with the comparer’s motives). Upward social, past temporal, counterfactual, and expectation-based comparisons, as well as downward prospective temporal comparisons, constitute the aversive comparison factor because these standards threaten the comparers’ motives. In the current study and in line with our research aims, we assessed only the aversive well-being comparison subscale (i.e., seven items in total and up to 21 items per person if the frequency items are answered with a score above 0). That is, we had three aversive well-being comparison subscales (i.e., comparison frequency, discrepancy, and affective impact). Internal consistency (α) was .80 to .84 for aversive comparison frequency, .79 to .87 for aversive comparison discrepancy, and .78 to .80 for aversive comparison affective impact.
Analysis procedure
Data analysis was conducted in R (R Core Team, 2025). Pathway analyses were examined using the R package lavaan (Rosseel, 2012). Missing data were accounted for by using the full information maximum likelihood method (Lee & Shi, 2021). Parameter estimates and significance tests were performed for all models using 10,000 bootstrapping iterations (Hayes, 2015). We set α at .01 as preregistered.
First, the relationship between comparison frequency and SAD symptoms was modeled in a random-intercept cross-lagged panel model (RI-CLPM; Hamaker et al., 2015), which considered both autoregressive and cross-lagged paths (for a visual presentation, see Fig. 1). Both comparison frequency and SAD symptom severity served as predictors (for the next measurement time point) and criteria (for the previous time point). This allowed both constructs to predict themselves and each other at the following time point. Following Hamaker et al. (2015), random intercepts with fixed factor loadings of 1 were specified for the two key constructs: comparison frequency and SAD symptoms. Importantly, the values of the autoregressive and cross-lagged paths were interpreted at the within-person level, which is a key advantage of this modeling approach (Hamaker et al., 2015).
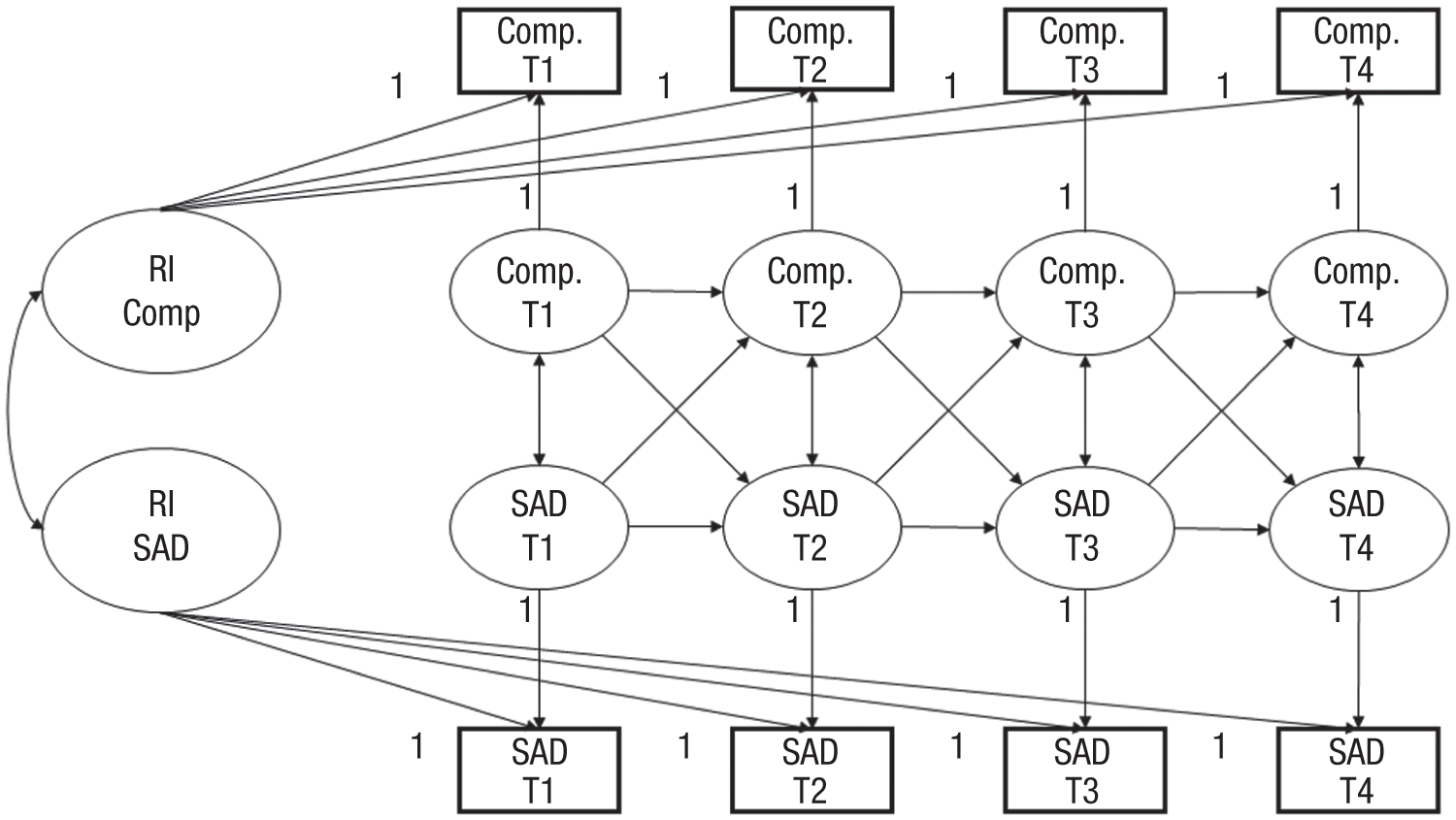
Visual representation of RI-CLPM in Study 2. RI-CLPM = random-intercept cross-lagged panel model; RI = random intercept; SAD = social anxiety disorder symptoms; Comp = comparison frequency.
Additionally, we ran pathway models to test serial mediation effects (for a visual representation, see Fig. 2). In each of these models, aversive comparison frequency at T1 served as the predictor, whereas SAD symptom severity at T2 was the criterion in different models. Again, SAD symptoms at the preceding time point were included as a predictor to model autoregression in all models. These autoregressive paths captured the effects of the current level of a construct on its own future level, representing construct stability. The predictive relationship between comparison frequency and prospective SAD symptoms was modeled through serial mediation analysis to capture the comparison process as outlined in gComp (Morina, 2021). In these models, the discrepancy at T1 served as the first mediator, and the affective impact of aversive well-being comparisons at T1 served as the second mediator variable. The same models were run with comparison frequency, discrepancy, and affective impact at T2 and T3 as predictor variables for SAD symptoms at T3 and T4, respectively.
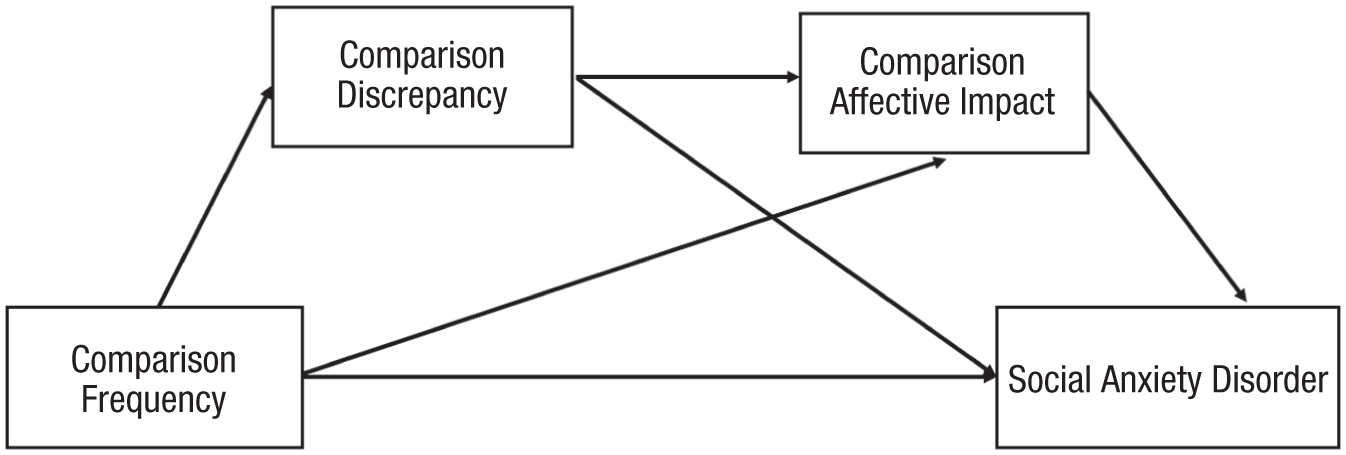
Visual representation of the serial multiple mediation models of the association between aversive comparison frequency and SAD symptoms and at the next wave. The comparison discrepancy serves as the first mediator, and comparison affective impact serves as the second mediator. SAD = social anxiety disorder.
Study 1 Results
Descriptive statistics
Over the course of the 10 assessment days, the 133 participants in the final sample completed a total of 2,962 EMA assessments (M = 22.27, SD = 8.53). Fifty-seven participants (43%) completed 80% to 99% of the EMA questionnaires, whereas 26 participants (20%) completed all 30 questionnaires. The number of completed EMA assessments remained fairly consistent over time. However, slightly fewer questionnaires were completed in the mornings compared with other times of the day.
Table S3 presents the means, standard deviations, and correlations for all variables at the between-person level. Social anxiety was significantly positively correlated with negative mood, comparison frequency, comparison discrepancy, daily stressors, attitudes toward social comparison, safety behavior, and perfectionism. Social anxiety was also significantly negatively correlated with perceived comparison affective impact. Negative mood as assessed with the PANAS was positively correlated with comparison frequency, comparison discrepancy, daily stressors, attitudes, safety behavior, and perfectionism. Negative mood was also negatively correlated with perceived comparison affective impact. Comparison frequency was strongly positively correlated with comparison discrepancy and moderately correlated with attitudes toward social comparison, safety behavior, and perfectionism. Comparison frequency was negatively correlated with comparison affective impact. Comparison discrepancy yielded correlations with attitudes and safety behavior. It also showed a significant negative correlation with perceived comparison affective impact. Perceived comparison affective impact was negatively correlated with all variables. Daily stressors were positively correlated with attitudes, safety behavior, and perfectionism. Attitudes were significantly positively correlated with safety behavior and perfectionism. Last, safety behavior showed a significant positive correlation with perfectionism.
Multilevel models
The ICC of the null model indicated that 50% of the variance in social anxiety was attributable to differences between individuals, and 50% was attributable to differences within individuals, which confirmed the assumed nested data structure. For negative mood (secondary outcome), 53% of the variance was attributable to between-person differences, and 47% was attributable to within-person differences.
Between-person differences (trait variables)
The random-slope and random-intercept models (see Tables S4–S7) revealed significant differences between individuals in how trait variables affected social anxiety (see Fig. 3). Specifically, for comparison frequency (Table S4), we found a strong positive relationship with social anxiety, suggesting that individuals who compare more frequently tend to experience higher levels of social anxiety. Similarly, comparison discrepancy (Table S5) was positively related to social anxiety, indicating that people who perceive a greater difference between themselves and the standard tend to report more social anxiety. Perceived affective impact (Table S6) showed a significant negative relationship with social anxiety, suggesting that individuals who experience greater negative affect following comparisons are more likely to report higher social anxiety. Daily stressors (Table S7) were also positively related to social anxiety, supporting the idea that individuals with higher average stress levels than other individuals experience more social anxiety. As shown in Tables S8 to S11, similar patterns were observed for our secondary outcome, negative mood, supporting our hypotheses tested for between-person effects.
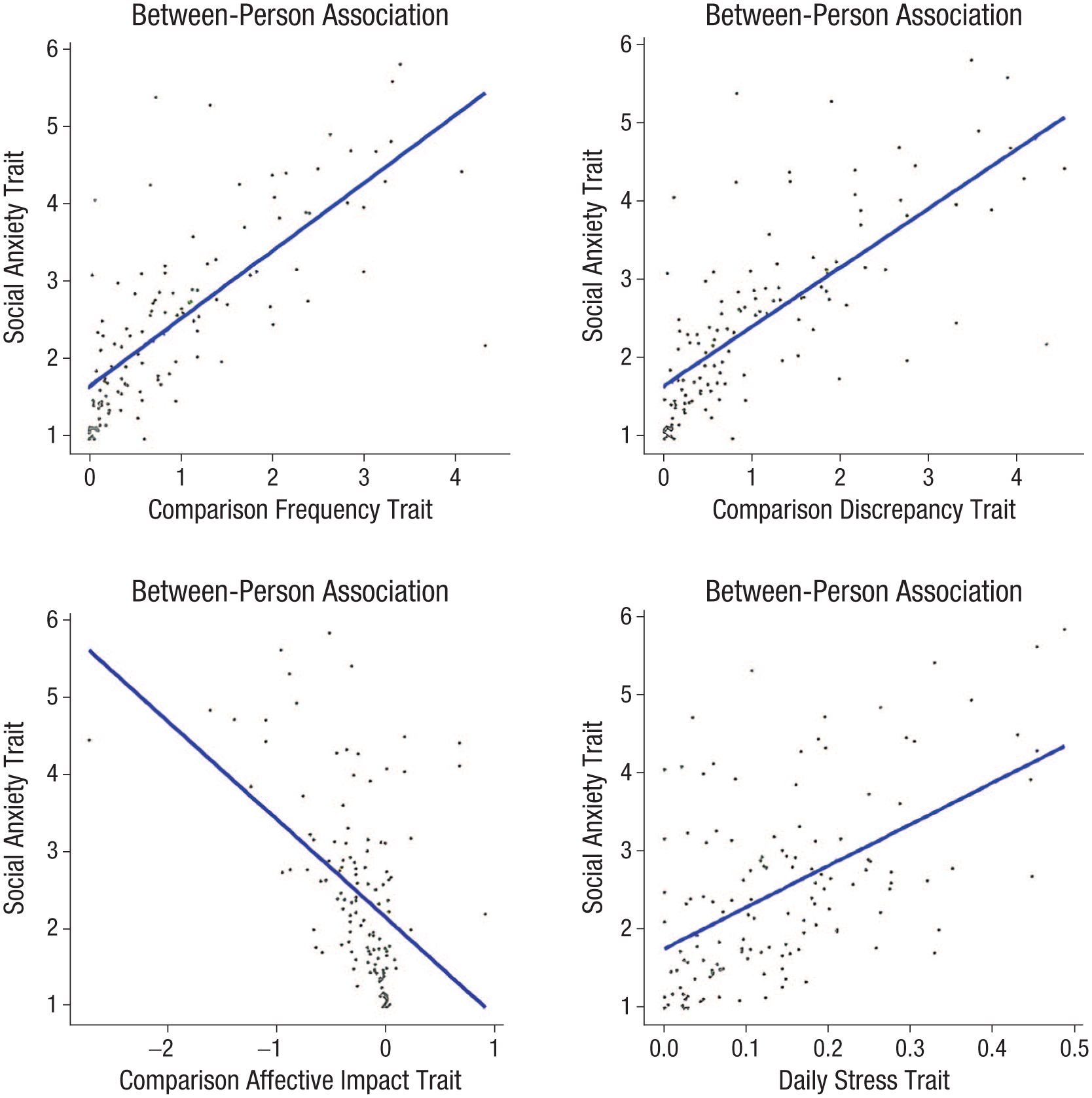
Visual illustration of between-person effects on social anxiety for comparison frequency (top left), comparison discrepancy (top right), comparison affective impact (bottom left), and daily stressors (bottom right).
Within-person differences (state variables)
At the within-person level, state variables were significantly associated with social anxiety (see Fig. 4 and Supplemental Tables 4–7); however, lagged effects including autoregressive effects were nonsignificant in all models. Concurrently, comparison frequency (Table S4) was positively associated with social anxiety, suggesting that individuals experienced more social anxiety during assessments with higher comparison frequency. Comparison discrepancy (Table S5) was similarly positively related to social anxiety, indicating that greater comparison discrepancy during a given assessment was linked to higher levels of social anxiety. Perceived affective impact (Table S6) showed a negative association with social anxiety, suggesting that higher-than-usual negative affective impact was associated with greater-than-usual social anxiety at that assessment. Daily stressors (Table S7) were positively related to social anxiety, supporting the hypothesis that momentary stressors contribute to increased social anxiety during a given assessment. As shown in Tables S8 to S11, these same patterns were observed for our secondary outcome, negative mood, confirming the hypotheses tested for within-person effects.
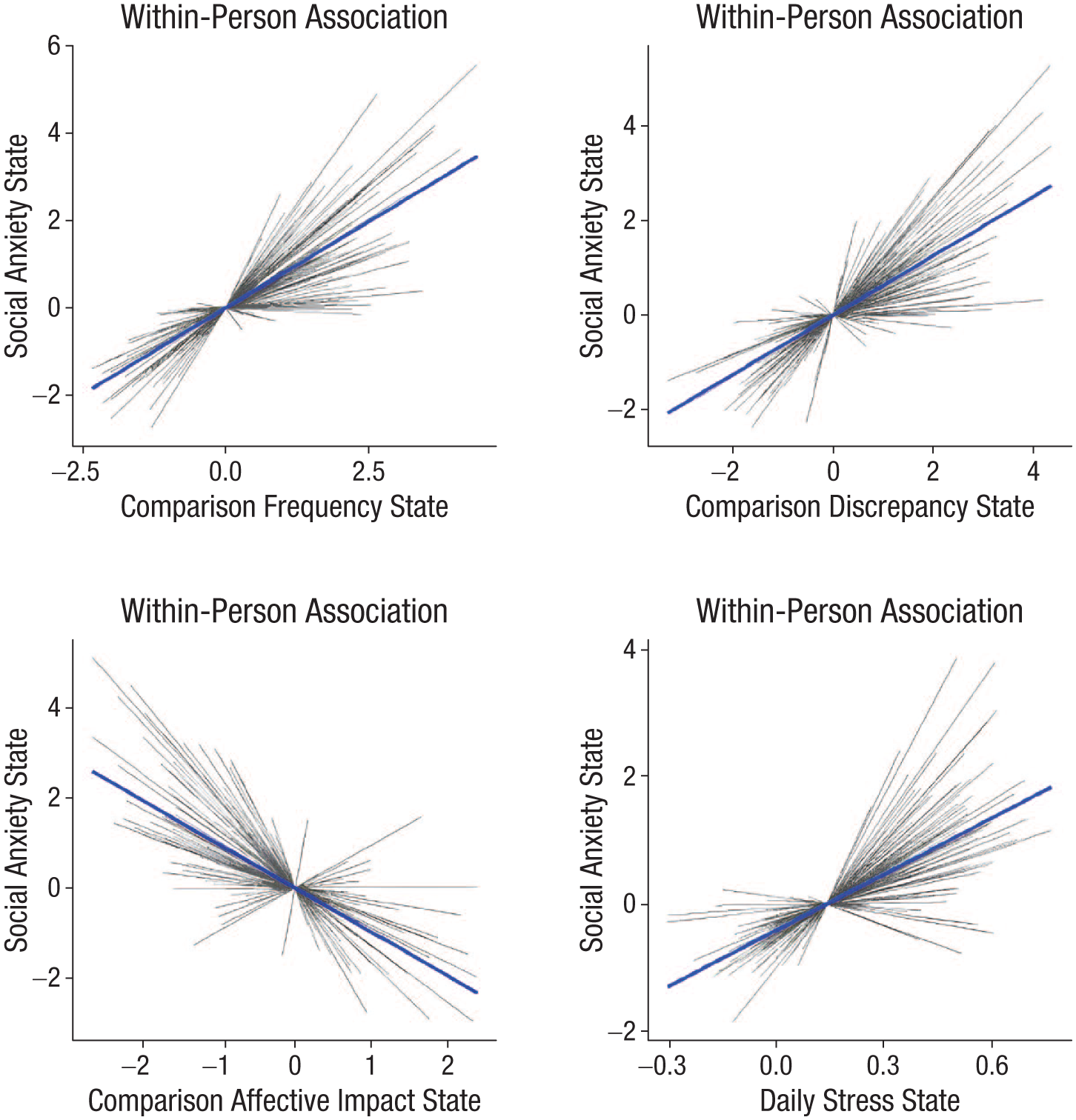
Visual illustration of within-person effects on social anxiety for comparison frequency (top left), comparison discrepancy (top right), comparison affective impact (bottom left), and daily stressors (bottom right).
Mediation effects
The within-person as well as the between-person relationships between comparison frequency and social anxiety were not mediated by comparison discrepancy—within-person indirect effect = 0.05, 99% CI = [−0.09, 0.20], p = .12; between-person indirect effect = −0.03, 99% CI = [−0.35, 0.29], p = 0.85. When comparison frequency and discrepancy were included in the same model, comparison discrepancy was no longer significant (p = .48 and p = .82, respectively), leading to the rejection of the mediation hypothesis.
However, the within-person relationship between higher-than-usual comparison frequency and increased SAD symptoms was partly mediated by a higher comparison negative affective impact—within-person indirect effect = 0.14, 99% CI = [0.08, 0.19], p < .001)—whereas the between-person association was not significant—between-person indirect effect = 0.12, 99% CI = [–0.02, 0.22], p = .020. Thus, our mediation hypothesis regarding the comparison affective impact was partly confirmed.
Additionally, the within-person relationship between daily stressors and social anxiety was partly mediated by comparison frequency—within-person indirect effect = 1.11, 99% CI = [0.80, 1.42], p < .001—yet not on a between-person level—between-person indirect effect = 0.96, 99% CI = [–0.01, 1.77], p = .022. Experiencing more-than-usual daily stressors led to increased social anxiety symptoms, partially mediated by higher comparison frequency, confirming our hypothesis.
Exploratory research questions
The perceived impact of comparison behavior impact was associated with SAD symptoms at both the between-person (estimate = 0.91, SE = 0.09, p < .001) and within-person (estimate = 0.87, SE = 0.06, p < .001) levels. Moreover, comparison behavior impact emerged as a significant mediator for the effects of comparison frequency and SAD symptoms—indirect effect = 0.22, 99% CI = [0.12, 0.31], p < .001—and between comparison affective impact and SAD symptoms—indirect effect = −0.44, 99% CI = [−0.57, −0.31], p < .001.
Study 2 Results
Descriptive statistics
Table S12 presents the descriptive statistics for the main variables. Comparisons across the four measurement time points revealed no significant differences in scores over time, with the exception that comparison discrepancy decreased from T1 to T2. Table S13 also displays the correlations between all variables at all time points. As expected, all variables showed significant associations in the anticipated directions, both cross-sectionally and longitudinally.
RI-CLPM
The RI-CLPM demonstrated excellent model fit—χ² = 7.28, p = .608, comparative fit index = 1.00, Tucker-Lewis index = 1.00, root-mean-square error of approximation = .01, standardized root-mean-square residual = .02, N = 376, df = 9. Table S14 contains all coefficients of the RI-CLPM. At the between-person level, there was a significant positive covariance (standardized estimate = 0.50, p < .001) between the random intercepts for comparison frequency and social anxiety, indicating that individuals who engaged in more frequent comparisons tended to report more social anxiety. At the within-person level, a significant covariance between comparison frequency and social anxiety was found only at T4 (standardized estimate = 0.31, p < .001), suggesting that individuals who reported higher-than-usual within-person comparison frequency at T4 also reported higher-than-usual social anxiety. No significant covariances were observed at the other three time points (all ps > .070). Furthermore, with the exception of the T3 and T4 autoregressive effects, no other effects were significant in the RI-CLPM.
Serial pathway models
Figure 2 depicts the serial pathway models for the proposed mediation pathways (for all coefficients, see Table S15). In these models, comparison frequency predicted social anxiety, comparison discrepancy at T1 served as the first mediator, and the affective impact of well-being comparisons at T1 was the second mediator. The same models were tested with comparison frequency, discrepancy, and affective impact at T2 and T3 as predictors of social anxiety at T3 and T4, respectively.
When autoregressive effects were included, none of the comparison variables significantly predicted social anxiety at the subsequent time point (apart from SAD symptoms themselves; all ps < .001). In models excluding autoregressive effects, most significant associations observed in single-variable models disappeared when the three comparison variables were considered together. Additionally, no clear mediation effects were found.
However, for the T2 and T3 models, higher comparison frequency predicted greater negative affective impact, which in turn predicted higher social anxiety. Still, the indirect effect was not significant—indirect effect = 0.04, 99% CI = [−0.00, 0.08], p = .059.
Discussion
We conducted two studies to examine how aversive comparisons and SAD symptoms interrelate. Comparative thinking was analyzed as a process in which frequent comparison may increase perceived discrepancies, trigger negative affect, and subsequently contribute to SAD symptoms. Study 1 used an EMA design to examine the role of comparative thinking in the domain of social impressions, stress, and SAD in individuals with clinical SAD symptoms over diurnal to intraweekly timeframes. Study 2 was a year-long, four-wave longitudinal study to identify how well-being comparisons relate to changes in social anxiety over time.
Short-term fluctuations and long-term patterns
Study 1 aligns with and extends the diary approach by Antony et al. (2005) and the EMA approach by Goodman et al. (2021). In these studies, social anxiety was associated with less favorable social comparisons and more fluctuations in its occurrence. Our findings extend this research by also examining expectation-based, counterfactual, and temporal comparisons in addition to social comparison. In line with our preregistered hypotheses, our study revealed that both between-person and within-person variations in comparative thinking were significantly associated with SAD symptoms and negative mood. Individuals who frequently engaged in comparisons perceived larger comparison discrepancies, experienced more negative emotions as a result, and reported greater behavior change, all of which were associated with higher SAD symptoms. These between-person effects reflect stable, long-term differences among individuals (e.g., Individual A engages in more comparisons than Individual B, and Individual A has higher overall SAD symptoms than Individual B). On a momentary level, higher-than-usual comparison frequency, greater comparison discrepancy, more negative affective impact, and increased behavior changes were associated with higher social anxiety during assessments (e.g., at a given assessment, an individual compared themselves more than usual and experienced heightened social anxiety). However, this accounted only for concurrent associations because lagged effects were nonsignificant, which may be attributed to the time lags being too long to capture enduring effects of comparisons.
In contrast, Study 2 revealed more complex long-term patterns, with most hypotheses not being confirmed. Although habitual comparison frequency was positively associated with SAD symptoms at the between-person level, within-person analyses revealed limited evidence of cross-sectional or temporal relationships between comparison variables and SAD. Specifically, comparison frequency and SAD symptoms exhibited significant within-person covariation at just one time point (T4). Critically, in Study 1, within-person fluctuations were assessed much more frequently and closer in time than in Study 2, which may explain the difference in findings. In particular, well-being comparisons were measured retrospectively for the previous 3 weeks, with assessments occurring 3 months apart. This broad time frame may have diluted the detection of short-lived fluctuations in comparison behaviors and their immediate impact on SAD symptoms. In addition, individuals may find it difficult to recall specific instances of comparison over a 3-week period. Comparisons are dynamic and context dependent (Morina, 2021), potentially influencing SAD symptoms in the short term but stabilizing by the next assessment. For example, heightened comparison frequencies and their affective impact after a stressful event might temporarily increase SAD symptoms but subside before the next evaluation 3 months later, underrepresenting these within-person effects. Nonetheless, we found stable between-person differences over a period of 1 year, which may present cumulative effects over time. This may highlight the importance of habitual comparison tendencies as a potentially relevant factor for SAD.
The comparison domains
The difference in comparison domains may also have contributed to differential findings between Studies 1 and 2. Participants’ perceptions of how they came across in social interactions, as assessed in Study 1, are inherently linked to interpersonal evaluations and are likely more directly tied to SAD symptoms. They may thus present a potent and proximal trigger for social anxiety. In contrast, well-being comparisons may reflect a broader, more stable tendency to evaluate oneself negatively in relation to different comparison standards (Diener et al., 2017; Keyes et al., 2010). Consequently, they may evoke less immediate emotional responses and thus exert different long-term effects. This tendency may extend beyond specific situations and perpetuate a chronic sense of lower well-being, leading to stable between-person differences in SAD symptoms. Although the immediate emotional impact of well-being comparisons may be less intense than social impression comparisons, their cumulative effects could shape well-being evaluations over time. This may explain why well-being comparisons, even when measured across broader timeframes, still showed stable associations with SAD symptoms at the between-person level.
Daily stress
In Study 1, daily stressors were positively related to SAD symptoms both on a within- and between person level. In line with our preregistered hypotheses, within-person comparison frequency explained part of the variance in this relationship. This dual pathway suggests that stress may be a critical antecedent of engaging in aversive comparative thinking, which, in turn, is associated with social anxiety. Stressful experiences often lead to increased self-focused attention, which is central in SAD maintenance (Clark & Wells, 1995). When faced with daily stressors—whether social, occupational, or individual—individuals may be more likely to engage in aversive comparisons to evaluate their social impression relative to various comparison standards (Gerber et al., 2018). This increased comparison frequency may function as an automatic stress response and reflect the need for self-assessment, self-improvement, or self-enhancement, especially in social contexts (Gregg et al., 2011; Schlechter, Meyer, & Morina, 2024; Sedikides & Strube, 1997). For individuals prone to SAD, this strategy may reinforce their fear of being negatively evaluated, potentially exacerbating their anxiety. Rather than providing relief or insight, frequent comparisons can amplify stress by creating or even reinforcing perceptions of discrepancy between oneself and different comparison standards. Stressors also diminish cognitive resources, such as self-regulation and perspective taking, and individuals with SAD display greater stress sensitivity (Farmer & Kashdan, 2015) and higher anxiety levels when facing social stress induction (Klumbies et al., 2014). As stress accumulates, individuals may rely on habitual cognitive patterns, such as dysfunctional comparative thinking, that align with their preexisting vulnerabilities. This, in turn, may intensify aversive comparisons and amplify their detrimental impact on well-being.
Further mediation effects
On a momentary level, perceived comparison affective and perceived behavior impact (but not comparison discrepancy) emerged as mediators of the link between comparison frequency and social anxiety symptoms. This aligns with cross-sectional examinations and two-wave longitudinal findings on the relationship between well-being comparisons and depression, anxiety, psychological well-being, and posttraumatic stress disorder symptoms (Morina & Schlechter, 2023; Schlechter, Hellmann, & Morina, 2024; Schlechter, Hoppen, & Morina, 2024). Frequent comparisons may trigger negative affective reactions, such as shame or anxiety, which in turn may amplify feelings of social discomfort, fear of negative evaluation or rejection, and sense of social competence. Perceived affective impact may create a feedback loop in which increased comparison frequency leads to stronger affective responses, which in turn may intensify social anxiety symptoms. Furthermore, perceived comparison behavior impact emerged as a significant mediator, partly accounting for the relationship between comparison frequency and SAD symptoms. This finding suggests that frequent comparisons may increase social anxiety by prompting maladaptive behaviors, such as avoidance or excessive self-monitoring, that reinforce anxiety over time (Cuming et al., 2009). Similarly, perceived comparison behavior impact mediated the relationship between comparison affective impact and SAD symptoms, suggesting that comparison affect directly influences behaviors that perpetuate social anxiety (e.g., avoidance behavior). The mediation analyses in Study 2 did not identify robust indirect pathways linking comparison frequency, discrepancy, and affective impact to future SAD symptoms, although all comparison variables were significantly related to SAD symptoms across time in bivariate associations. One exception was the T2 to T3 pathway, in which comparison frequency predicted negative affective impact, which in turn was associated with SAD symptoms. Thus, this mediation model points in the same direction as the mediation effect in Study 1. However, the indirect effect was rather weak and not consistently observed across time points, and no mediation effect occurred when autoregressive pathways were accounted for.
Exploratory research questions
Interindividual differences in safety behaviors (Cuming et al., 2009), attitudes toward social comparison (Schlechter, Meyer, & Morina, 2024), and perfectionism (Newby et al., 2017) did not moderate the relationship between comparisons and SAD symptoms, contrary to expectations, although they were independently associated with SAD symptoms (for a discussion, see Supplemental Material 3).
Theoretical contribution of the current work
The current work contributes to the theoretical understanding of SAD by integrating cognitive, emotional, and behavioral components of comparison. Our findings align with gComp (Morina, 2021). Importantly, we identified perceived comparison behavioral influence as a critical element in this process, in which comparisons not only were associated with negative emotions but also with maladaptive behaviors, such as avoidance or heightened self-monitoring, that may reinforce SAD symptoms. For instance, an individual prone to comparing their social performance with colleagues at work may perceive large discrepancies (e.g., being less confident or assertive). The resulting affective changes may, in turn, influence behavior, potentially leading to social avoidance, which perpetuates the cycle of social anxiety. This aligns with the cognitive-behavioral model of SAD (Clark & Wells, 1995), which emphasizes the interplay of maladaptive appraisals, emotional responses, and behaviors in maintaining social anxiety. Our between-person findings suggest that long-term habitual comparative thinking may represent a relevant factor for SAD. Combined with our insights on daily stress, this resonates with diathesis-stress models, in which external stressors exacerbate this vulnerability by heightening comparison frequency and its behavioral impact.
Clinical implications
Our findings have potential implications for research on the treatment of SAD. Frequent comparisons and the affective and behavioral reactions they evoke may play a central role in the experience of SAD. This suggests that therapeutic interventions aimed at targeting frequent upward comparisons could be particularly effective in mitigating emotional distress in individuals with SAD. Cognitive-behavior therapy may be particularly useful in helping individuals reflect on their tendency to engage in aversive comparisons and potentially reframe perceived comparison discrepancies. Additionally, interventions that target an increase in conscious recognition of or adaptive coping with the affective impact of comparisons, such as mindfulness practices or emotion-regulation strategies, could help patients effectively manage the negative affective impact during or after comparisons. Furthermore, addressing external stressors and teaching coping strategies for managing daily stress as well as comparison-related emotions could reduce the likelihood of initiating comparative thinking. However, experimental and intervention studies are required before these theoretical considerations can be effectively translated into clinical practice.
Strengths and limitations
Our study extends prior research on comparisons and SAD by focusing on social impressions and well-being as relevant comparison domains in this field. We expanded the scope of prior work beyond social comparison by including expectation-based, counterfactual, and temporal comparisons. Moreover, we examined comparison as a process consisting of comparison frequency, discrepancy, and perceived affective and perceived behavioral influence. Additionally, we scrutinized how daily stress influences social comparisons and anxiety. Last, we combined daily-level EMA with longitudinal data over the course of 1 year to provide a more comprehensive understanding of how short-term fluctuations and long-term patterns in comparative thinking impact SAD symptoms.
The following limitations merit mention. First, our longitudinal study designs do not permit causal conclusions. Experimental studies manipulating comparative behavior are needed to address this. Second, both studies relied on self-report measures, which may be subject to biases. Clinical interviews to establish a SAD diagnosis and behavior observations of comparative behavior in real-life settings are potential next steps in this regard. Third, our studies focused primarily on comparisons within specific domains (e.g., social impressions or well-being), which does not fully capture the breadth of comparison processes across different contexts. Future research could expand on these findings by exploring other domains of comparison. Fourth, the samples were relatively homogeneous in terms of demographic characteristics, which may limit the generalizability of the findings to more diverse populations. Further research with more diverse samples could help determine whether the observed patterns hold across different cultures or demographic groups. Fifth, although our comparison items were adapted from established measures, assessing comparative thinking in real time introduces several interpretative complexities. Participants were asked to report how often they engaged in comparisons, the perceived discrepancy, and the perceived affective and behavioral impact of those comparisons since the last assessment. However, it remains unclear whether participants averaged their responses across multiple comparisons or focused on the most salient or recent instance. This ambiguity complicates the interpretation of the intensity and specificity of reported comparison effects. Moreover, participants may have varied in their interpretation and application of the concept of “comparison,” particularly across different comparison types (e.g., social vs. counterfactual). Future research should apply emerging guidelines such as the ESM-Q framework a priori to evaluate and ensure the quality of EMA items (Eisele et al., 2025). Sixth, reliability coefficients for daily stress were rather low, which may have introduced measurement error and potentially attenuated observed associations. Seventh, we exclusively focused on aversive comparisons, which mostly contained upward comparison. Although this focus is grounded in prior research indicating that aversive comparisons are especially threatening and closely linked to negative mental-health outcomes (McCarthy & Morina, 2020; Morina & Schlechter, 2023), the exclusion of lateral and downward comparisons limits the scope of our findings. Including these additional comparison directions may provide a more comprehensive understanding of the role of comparison in SAD. Future research should examine whether upward comparisons are uniquely associated with social anxiety, or whether more complex, interactive patterns also emerge in response to lateral or downward comparisons. Eighth, the use of a cutoff to exclude participants with lower levels of social anxiety in Study 1 limits the generalizability of our findings to individuals with subclinical or minimal symptoms. Ninth, our causal comparison model represents a theory-driven simplification that focuses on one of the most plausible pathways (Morina, 2021) while not claiming exclusivity.
Conclusion
Our findings revealed significant effects of comparative thinking on SAD both on the within-person (short-term fluctuations) and between-person (long-term stable patterns) levels. On the within-person level, frequent comparisons and their affective and behavior impact were linked to momentary increases in SAD symptoms. On the between-person level, habitual patterns of comparative thinking showed stable associations with SAD even over the course of 1 year, suggesting that these tendencies represent enduring significant factors. The findings underscore the central role of comparative thinking in SAD, advancing our theoretical understanding of this condition.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026261424180 – Supplemental material for Comparative Thinking and Clinical Social Anxiety: Within- and Between-Person Effects in a Daily Ecological Momentary Assessment Study and a Four-Wave Longitudinal Study
Supplemental material, sj-docx-1-cpx-10.1177_21677026261424180 for Comparative Thinking and Clinical Social Anxiety: Within- and Between-Person Effects in a Daily Ecological Momentary Assessment Study and a Four-Wave Longitudinal Study by Pascal Schlechter, Thomas Meyer, Lianna E. Kerneck, Pia Schulze Mengering, Thole H. Hoppen, Meret König and Nexhmedin Morina in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Jennifer Lau
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.