
Abstract
Environmental sensitivity is a personality trait reflecting individual differences in response to environmental influences. Although the link between common personality traits and psychopathology is well established, trait sensitivity is often overlooked despite its association with mental health. In this study, we systematically reviewed literature on sensitivity and mental-health outcomes and conducted a meta-analysis to quantify the relationship of sensitivity with depression and anxiety. The review included 33 studies (N = 12,697; 62.51% female; age: M = 25.35 years) and revealed positive correlations between sensitivity and depression, anxiety, psychosomatic symptoms, obsessive compulsive disorder, posttraumatic stress disorder, agoraphobia, and social phobia; correlations ranged from r = .05 to r = .65. The overall effect size was substantial for depression (r = .36, 95% confidence interval [CI] = [.30, .42], p < .001) and anxiety (r = .39, 95% CI = [.34, .44], p < .001). Findings confirm a robust association with mental health, and we explore its potential to inform treatment and prevention.
Keywords
The relationship between the Big Five personality traits and psychopathology is well established, showing consistently that higher levels of neuroticism are associated with poorer mental-health outcomes, including greater depression, anxiety, and psychological distress (Albuquerque et al., 2012; Khan et al., 2005). In addition, the relevance of these personality traits regarding diagnoses, conceptualization, treatment, and treatment outcomes of clients in clinical-therapeutic settings has been discussed and empirically supported, showing, for example, that lower levels of neuroticism and higher levels of extraversion, agreeableness, conscientiousness, and openness are associated with better treatment outcomes (Bucher et al., 2019). A somewhat related but lesser known common personality trait that appears to also be associated with an increased risk of mental-health problems is the trait of sensitivity. Trait sensitivity, often referred to as “sensory-processing sensitivity” (SPS; E. N. Aron & Aron, 1997; E. N. Aron et al., 2012), is characterized by a heightened degree of sensitivity to physical, emotional, and social stimuli, such as bright lights, subtle changes in the environment, and other people’s moods, combined with deeper cognitive processing of such sensory stimulation. Sensitivity is associated with established personality traits, such as neuroticism, introversion, and openness to experiences, but is relatively distinct from them (Lionetti et al., 2019; Pluess et al., 2023). However, despite a growing body of research since the early 2000s showing a positive association between sensitivity and mental health, this relationship is not yet well understood. Therefore, the aim of this study was to systematically review the existing literature on sensitivity and common mental-health outcomes and conduct a meta-analysis to establish the overall effect size for the relationship with depression and anxiety. This not only addresses a gap in the current literature but could also help to determine whether sensitivity is an individual trait that should be considered in clinical science and practice. In other words, if individuals’ level of sensitivity puts them at heightened risk for the development of mental-health problems, it seems crucial to explore the impact of sensitivity in more depth. Better knowledge on the role of individual differences in sensitivity for mental health may not only inform theory (e.g., etiology, conceptualization) but could also have practical implications (e.g., treatment, effectiveness of interventions, treatment outcomes, relapse prevention). We begin by describing the trait of sensitivity, followed by a brief overview of the existing research on sensitivity and mental health, before introducing the current study.
Trait Sensitivity
The conceptualization of sensitivity as a trait, first described by well-known Swiss psychiatrist and psychoanalyst C. G. Jung in 1913 as “innate sensitiveness” (E. N. Aron, 2004; Jung, 1976), has become the focus of empirical research since the mid-1990s. It has been shown that individual differences in registering, processing, and responding to environmental stimuli exist in many species, including humans (Belsky & Pluess, 2009; Ellis et al., 2011). These differences are associated with genetic and prenatal and postnatal environmental factors and are driven by a more sensitive central nervous system (E. N. Aron, 2010; Greven et al., 2019; Wolf et al., 2008).
At least three different theoretical frameworks have since been developed to describe individual differences in sensitivity: differential susceptibility (Belsky, 1997; Belsky & Pluess, 2009), biological sensitivity to context (Boyce & Ellis, 2005), and SPS (E. N. Aron & Aron, 1997). Despite some differences between these frameworks, they all share the notion that individual differences in sensitivity exist for evolutionary reasons and that sensitive individuals are both more vulnerable to the negative effects of adversity and benefit more from positive, supportive experiences. In an attempt to integrate these different sensitivity concepts into a single overarching metaframework, Pluess (2015) introduced the umbrella term “environmental sensitivity” (ES), which has been adopted increasingly in recent years to describe sensitivity as a concept and as a trait. Throughout this article, we refer to “sensitivity” as a more general term rather than an individual conceptualization, such as SPS. Sensitivity has been shown to be the function of a common and normally distributed trait; people generally fall into three distinct groups along a sensitivity continuum: low sensitive (29%), medium sensitive (40%), and high sensitive (31%; Lionetti et al., 2018). To date, one twin study (Assary et al., 2020) and several functional-MRI studies (e.g., Acevedo et al., 2018; A. Aron et al., 2010; Jagiellowicz et al., 2011) support the biological basis of the trait, showing that sensitivity is moderately heritable and marked by higher activation in brain regions that are involved in empathy, social processing, and reflective thinking.
According to E. N. Aron (2010), sensitivity is indicated by heightened sensory sensitivity, being prone to overarousal, emotional reactivity, and depth of processing and can be measured in adults with the original 27-item Highly Sensitive Person Scale (HSPS; E. N. Aron & Aron, 1997) or the more recent 12-item version (Pluess et al., 2023). For children and adolescents, a 12-item Highly Sensitive Child Scale (HSCS) has been developed (Pluess et al., 2018). The HSPS has been translated into multiple languages, validated in many contexts, and is the most common instrument to measure sensitivity in adults (Ponce-Valencia et al., 2022). Initially, E. N. Aron and Aron (1997) proposed that the HSPS was unidimensional, but subsequent studies have found the scale to be multidimensional. For instance, Smolewska et al. (2006) identified a three-factor structure of the scale: (a) Ease of Excitation (EOE), which refers to being easily overwhelmed by internal or external stimuli (e.g., “Are you more than others affected by moods of other people?”); (b) Low Sensory Threshold (LST), which refers to unpleasant sensory arousal from external stimuli (e.g., “Do you become unpleasantly aroused when a lot is going on around you?”); and (c) Aesthetic Sensitivity (AES), which refers to being susceptible to beauty and the arts (e.g., “Are you deeply moved by the arts or music?”). In recent years, a bifactor structure has been confirmed consisting of a general, overarching SPS factor and the three subscales that captures the multidimensionality of the HSPS and the HSCS (Greven et al., 2019; Pluess et al., 2023).
Sensitivity and Mental Health
Over the last 25 years, a growing number of studies and one systematic review (Costa-López et al., 2021) have investigated the relationship between sensitivity measured with the HSPS and mental health in adolescents and adults. These studies provide evidence of a consistent association between high levels of sensitivity and a wide range of symptoms of psychopathology and psychological issues. This includes anxiety and depression (Bakker & Moulding, 2012; Liss et al., 2005, 2008), difficulties in emotional regulation (Brindle et al., 2015), lower levels of subjective happiness (Sobocko & Zelenski, 2015), lower levels of life satisfaction (Booth et al., 2015 ), increased levels of stress (Bakker & Moulding, 2012), physical symptoms of ill health (Benham, 2006), burnout (Golonka & Gulla, 2021), greater dissatisfaction at work, and a greater need for recovery (Andresen et al., 2017; Evers et al., 2008).
Several explanations have been offered regarding the underlying mechanisms hypothesized to drive the detected association between sensitivity and mental-health problems. Benham (2006) and Brindle et al. (2015) suggested that individuals with high levels of sensitivity suffer from poorer mental health than individuals low in sensitivity because of their tendency to feel more easily overstimulated by internal and external stimuli. More specifically, feeling often and quickly overwhelmed in everyday life because of perceiving more stressors could promote a recurring sense of learned helplessness in the individual—a mental state that contributes to depression and anxiety (Yano et al., 2019). Others have proposed that the association between sensitivity and mental-health issues is driven by depth of processing, which refers to deeper cognitive processing of stimuli. For example, Lionetti et al. (2022) identified rumination as an important cognitive risk factor for the development of depressive symptoms in highly sensitive children and suggested that it is exactly this depth of processing that could facilitate rumination and the internalization of problems. Another possible explanation for the association between sensitivity and negative affect, specifically, depression, was proposed by Brindle et al. (2015) and focuses on emotional reactivity—the tendency of highly sensitive individuals to react strongly with “positive” and “negative” feelings. Brindle et al. hypothesized that individuals high in sensitivity are more aware of their negative emotional states while also showing lower self-efficacy regarding how they might change their negative emotional states. In other words, an increased awareness of negative emotional states in someone who lacks the emotional-regulation skills to overcome these could cause recurring feelings of helplessness and negative affect in the individual.
Theories of sensitivity postulate that highly sensitive individuals are not only more affected by adversity but also benefit disproportionately from supportive experiences and environments (Pluess & Belsky, 2013). For example, it has been shown that individuals with high levels of sensitivity benefit more from psychological interventions, such as school-based programs for children with behavioral problems (de Villiers et al., 2018; Greven et al., 2019). To add to this, it has been shown that high levels of sensitivity correlate with positive outcomes, such as an increase in positive affect following positive mood induction and more positive responses to antibullying and depression-prevention programs in children and adolescents (Lionetti et al., 2018; Nocentini et al., 2018; Pluess & Boniwell, 2015).
The Current Study
Given growing evidence that sensitivity plays an important role in mental health, in this preregistered study, we aimed to systematically review all existing studies to date and conduct the first meta-analysis on sensitivity to establish the overall effect size with common mental-health problems (i.e., depression and anxiety). Given that the age of onset of most mental disorders is between the mid-teens and the mid-20s (Kessler et al., 2007), in the current study, we focus specifically on adolescents and adults. Based on previous research, we expected that sensitivity, measured with the HSPS or the HSCS, would show a moderate and positive association with various mental-health disorders, specifically, with depression and anxiety.
Transparency and Openness
The systematic review was preregistered in Prospero in September 2021 before any search or analysis was carried out. The preregistered protocol in Prospero was updated in light of an additional systematic search in 2024. It can be found at https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=273011&VersionID=2289747. All the relevant materials are provided in the Supplemental Material available online. The data-analysis code and any other materials can be obtained on request from the corresponding author.
Method
This systematic review follows the PRISMA reporting guidelines (Page et al., 2021). It was preregistered in PROSPERO (CRD42021273011). Because the review mainly includes cross-sectional studies, the Appraisal Tool for Cross-Sectional Studies (AXIS) for quality assessment was employed (Downes et al., 2016). For the quality assessment of all included studies, see Table S1 in the Supplemental Material.
Data sources
A Boolean literature search using the connecting words OR and AND to combine identified search terms was conducted in the following seven databases: PsycArticles, PsycInfo, Medline, Web of Science, CINAHL Plus, Scopus, and PubMed. Additional articles were identified through citation searching and approaching authors directly if the full-text articles were not available (for the finalized database search strategy, see Table S2 in the Supplemental Material).
Search strategy
The review team (T. Falkenstein, L. Sartori, and M. Pluess) developed and piloted a search strategy based on relevant keywords and index terms relating to “sensitivity” (e.g., “Highly Sensitive Person,” “Sensory Processing Sensitivity”) and “mental health” (e.g., “Depression,” “Anxiety,” “Emotion* Regulation”). Keywords and index terms had to appear in the title or the abstract of the studies. Inclusion criteria (e.g., studies had to be peer reviewed and published in academic journals; mean age of participants must be 12 years and above) and exclusion criteria (e.g., studies published before 1997, studies that explored the relationship between sensitivity and subclinical outcomes, e.g., resilience, self-efficacy, stress) were identified (for the complete list of inclusion and exclusion criteria, see Table S3 in the Supplemental Material). To be as specific as possible regarding the definition of trait sensitivity, we decided to focus on only the most researched trait-sensitivity construct, which is SPS, measured with the HSPS (E. N. Aron & Aron, 1997) or any of its variations (e.g., short/long versions, HSCS for children, HSPS for adults) given that the different versions of the HSPS all share the same bifactor structure with three subscales (LST, EOE, AES) and measure the same sensitivity construct (SPS). Other sensitivity measures (e.g., Adult Temperament Questionnaire by Rothbart et al., 2000; Sensory Processing Sensitivity Questionnaire by De Gucht et al., 2022) were not included. To define “common” mental-health problems and to focus on clinical diagnoses that are most common in the general population, according to the World Health Organization (WHO), the search was limited to broader “diagnostic categories” in the International Statistical Classification of Diseases and Related Health Problems (ICD-10; WHO, 1994), such as depressive disorders, anxiety disorders, bipolar disorder, posttraumatic stress disorder (PTSD), schizophrenia, and personality disorders. Hence, we considered only mental-health disorders listed in ICD-10 or the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013) rather than subclinical outcomes, such as burnout or stress. Measurement tools or subscales of included mental-health measures that focused on nonmental-health-specific symptoms (e.g., subjective happiness, stress) rather than mental health were therefore also excluded. Given that most published studies on sensitivity and mental health are based on samples from a general population and not a clinical population (and do not include clinical assessment), we focused on self-report mental-health measures that are often used in clinical practice (e.g., Beck Depression Inventory [BDI], Beck Anxiety Inventory [BAI], Depression, Anxiety and Stress Scale [DASS-21]). After the piloting stage, an initial Boolean literature search was conducted in December 2021 and updated in late February 2024, resulting in the combined numbers presented in Figure 1 (including results from additional citation searches based on the citations of extracted studies).
PRISMA flow diagram of study selection process.
Selection of articles and quality control
Once the review team had decided on the final string of search terms, preliminary searches were conducted to pilot the study-selection process. Following successful piloting, the first reviewer (T. Falkenstein) conducted a Boolean literature search. The second reviewer (L. Sartori) duplicated the search criteria to validate result numbers. Any discrepancies were discussed between the two reviewers, which continued until results matched. If results could not be matched, a third reviewer (M. Pluess) examined the respective reviewer’s Boolean search. After the review team reached an agreement, their respective searches were extracted to EndNote, and duplicates were automatically removed.
In the second stage of the reviewing process, results were extracted to Rayyan software for coding in which the two reviewers (T. Falkenstein and L. Sartori) independently assessed title and abstracts to decide whether articles met the inclusion criteria. Each of the reviewers’ decisions were blinded, and any disagreements—at this stage or at any stage of the process—were resolved through discussion and/or the involvement of the third collaborator (M. Pluess).
In the third stage of the reviewing process, the full text of all articles that were not excluded during the second stage were screened by both reviewers independently, and data were extracted. Once it was finalized which articles to include, AXIS was applied independently by the two reviewers (T. Falkenstein and L. Sartori) for quality assessment. This process involved rating 20 characteristics of the included studies as “yes,” “no,” “maybe,” or “N/A.” It indicates the risk of bias for the studies included in the systematic review and meta-analysis (see Table S3 in the Supplemental Material).
Extracted data and synthesis of results
Data extraction was conducted by the two reviewers (T. Falkenstein and L. Sartori). The extracted information consisted of authors, year of publication (print or online), country (area of data collection), sample size, gender breakdown, age (mean, standard deviation), study design, SPS measurement tool, mental-health-measurement tool, and the correlation coefficient r between sensitivity and mental-health outcome. Key characteristics of the included studies are presented in Table 1. Main results of the included studies (e.g., effect size between sensitivity and mental health based on Cohen’s d) are presented in Table 2. In preparation for the meta-analysis, studies were categorized into three different mental-health-outcome groups: (a) depression, (b) anxiety, and (c) other (e.g., PTSD, psychosomatic symptoms, personality disorder).
Main Characteristics of Included Studies
Note: F = female; M = male.
Sample size at Time 1; sample size at Time 2 (1-month follow-up) = 54; sample size at Time 3 (4-month follow-up) = 55.
Sample size seasonal-affective-disorder group; sample size healthy-control-subjects group = 30; total sample size = 61.
Sample size at Time 1.
Sample size at Time 3 (measurement for only sensory-processing sensitivity and depression); sample size at Time 1 = 209; sample size at Time2 = 95.
Gender distribution at Time 3; gender distribution at Time 1, F = 53.11%; gender distribution at Time 2, F = 49.47%.
Age at Time 3; age at Time 1: M = 12.8 years (SD = 0.5); age at Time 2, M = 13.7 years (SD = 0.6).
Sample size at Time 1.
Main Results of the Included Studies
Note: SPS = sensory-processing sensitivity; HSPS = Highly Sensitive Person Scale; HSCS = Highly Sensitive Child Scale; HSPS-J19 = 19-item, Japanese version of the HSPS; J-HSCS = Japanese version of the HSCS; GDS = Goldberg Depression Scale; DASS-21 = Depression, Anxiety and Stress Scale; PHQ-9 = Patient Health Questionnaire-9; BDI-II = Beck Depression Inventory-II; MDI = Major Depression Inventory; DSRSC = Depression Self-Rating Scale for Children; DSRS-C = Birleson Depression Self-Rating Scale for Children; BDI = Beck Depression Inventory; SDS = Self-Rating Depression Scale; CES-D = Center for Epidemiologic Studies Depression Scale; BAI = Beck Anxiety Inventory; HAQ = Hierarchical Anxiety Questionnaire; SHAI = Short Health Anxiety Inventory; STAI = State-Trait Anxiety Scale; SPAI = Social Phobia and Anxiety Inventory; GAD-7 = Generalized Anxiety Disorder Scale; OCI-R = Obsessive-Compulsive Inventory–Revised; Y-BOCS = Yale–Brown Obsessive Compulsive Scale; DOCS = Dimensional Obsessive-Compulsive Scale; OCD = obsessive compulsive disorder; PCL-5 = PTSD Checklist for DSM-5; PTSD = posttraumatic stress disorder; PTSD-RI = PTSD Reaction Index; APD = avoidant personality disorder based on criteria from the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1994); HSCL = Hopkins Symptom Checklist, Japanese version; EOE = Ease of Excitation; AES = Aesthetic Sensitivity; LST = Low Sensory Threshold.
Correlation coefficient r was calculated based on reported regression coefficient β = 0.60 (p = .024) with the help of PlotDigitizer software and R Version 4.2.3. software programs.
Time 1 (preintervension) was only measurement for SPS and depression.
Time 3 was only measurement for SPS and depression.
Time 1 (n = 70).
Time 2 (1-month follow-up; n = 54).
Time 3 (4-month follow-up; n = 55).
Information provided by the authors.
Meta-analysis
A meta-analysis was conducted on a selected number of studies for the two most common mental-health-outcome categories among reviewed studies: depression and anxiety. The mental-health outcomes in the third category (e.g., PTSD, psychosomatic symptoms, personality disorder) were too varied and studies too few for inclusion in a meta-analysis. The previously identified inclusion criteria (e.g., studies must assess the trait of sensitivity using the HSPS [E. N. Aron & Aron, 1997] or any of its translations and variations) and exclusion criteria (e.g., studies that explore the relationship between sensitivity and subclinical outcomes) for the systematic review helped to increase the homogeneity of the included studies and therefore strengthened the results of the meta-analyses.
Outcomes included in each analysis were selected to ensure that the independence assumption is upheld, excluding correlation coefficients of any of the three subscales (EOE, LST, AES) from the same studies. In other words, only those outcomes that featured the total score of the HSPS and not its subscales were considered in each meta-analysis. When a study provided both, a total score and the subscales (AES, LST, EOE), only the total HSPS-score outcome was included, not the subscale outcomes. This was done to avoid having the same sample included multiple times in the same meta-analysis. Longitudinal studies with repeated measurements were included only once, using either the first measurement or the time point when sensitivity and mental health were measured at the same time. If a study considered several outcomes (e.g., social phobia, agoraphobia) from the same diagnostic category (e.g., anxiety), the study was included only once with the mental-health outcome that is more common (e.g., social phobia was included; agoraphobia was not). In the case of mental-health measures with different subscales, such as the DASS-21 (Lovibond & Lovibond, 1995), we included only the relevant subscale (e.g. anxiety or depression were included; stress was not) in the respective meta-analysis (anxiety or depression).
Data from the included studies was extracted to an Excel sheet from which it was uploaded into IBM SPSS (Version 29) software for analysis. Results were transformed into Fisher’s z scores to facilitate meta-analysis and back-transformed to a correlation coefficient when appropriate for interpretation. Using precalculated effect sizes, we performed separate random-effects meta-analyses for depression and anxiety. Results are presented in the form of two forest plots (see Figs. 2 and 3). Restricted maximum likelihood was applied to estimate the heterogeneity variance (Langan et al., 2019). Heterogeneity statistics (including τ2 and I2) are presented to help understand between-studies variation in effect size.
Forest plot for the correlation between sensitivity and depression. Random-effects model. Heterogeneity: τ2 = 0.02, H2 = 8.22, I2 = 0.88. Significance level: p < .001.
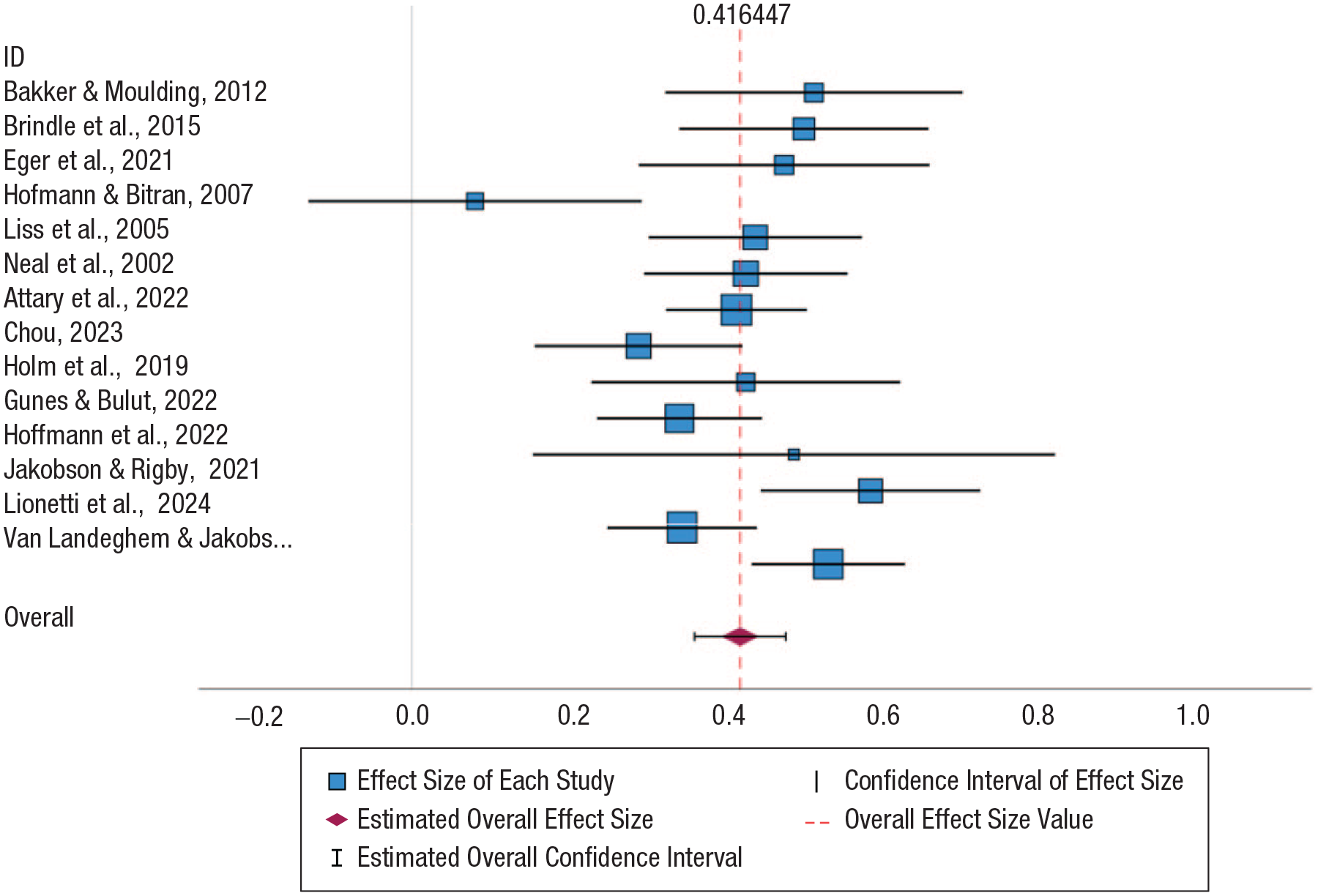
Forest plot for the correlation between sensitivity and anxiety. Random-effects model. Heterogeneity: τ2 = 0.01, H2 = 2.43, I2 = 0.59. Significance level: p < .001.
Both 95% confidence intervals (CIs) and prediction interval (PIs) are provided for the effect-size estimates of the two meta-analyses. Although the 95% CI accounts primarily for sampling variability, it does not consider between-studies heterogeneity. In contrast, the reported PI represents the range within which the true effect size of a new study, selected at random from the same population, is expected to fall. In other words, whereas the CI provides a range for the average effect size, the PI provides a more realistic expectation of the variation in effect sizes that might be observed in future studies on ES and mental-health outcomes. Therefore, both intervals are provided.
Results
In the database search, we identified 829 studies in total. After the removal of duplicates (n = 198), titles and abstracts of 631 studies were screened, of which, 563 studies were removed. Full-text screening was conducted for the remaining 68 studies. During this process, a further 39 studies were excluded, which reduced the final number to 29 studies. The data extraction was then conducted. In addition, 10 further studies were identified through other methods (citation searching and contacting authors directly if full-text articles were not available), of which, six were subsequently included. This resulted in a total of 33 studies included in this review (for a flow diagram, see Fig. 1).
Description of included studies
All 33 included studies used a correlational study design; there were 27 cross-sectional studies, five longitudinal studies, and one case-control study. Most of the included studies were conducted in Japan (six), followed by four studies that were conducted internationally (online) and four studies that were conducted in the United States. Three studies were conducted in Canada. Two studies were conducted in Iran, China, and Lebanon, and one study was conducted in Ireland, South Korea, Serbia, Turkey, Germany, Israel, Denmark, Austria, Norway, and the UK. The dates of first publication (print or online) ranged from 2000 to 2024. The sample size of the studies ranged from 38 to 2,412; total sample size across all included studies was 12,697, of which, 62.51% were female (Table 1). The mean age of the participants was 25.35 years. Only two studies included clinical samples drawn from hospital patients—either in treatment for obsessive compulsive disorder (OCD) or showing clinically elevated PTSD symptoms after an accident. The rest of the studies used samples from the general population, mostly students.
Description of sensitivity measures
Twenty-seven of the 33 included studies used the HSPS (E. N. Aron & Aron, 1997)—mostly the long rather than the short version—and six studies used the HSCS (Pluess et al., 2018).
Three of the 33 studies investigated the three subscales of the HSPS in relation to mental-health outcomes instead of considering the total HSPS score (Khosravani et al., 2021; Liss et al., 2008; Takahashi et al., 2020). Four studies explored both the total HSPS score and its three subscales in relation to mental-health outcomes (Jakobson & Rigby, 2021; Lionetti et al., 2024; Van Landeghem & Jakobson, 2024; Wu et al., 2021). The majority of 26 studies considered only the total HSPS score rather than the three subscales (Table 2).
Description of the mental-health measures
Mental-health measures included in the studies were grouped into three broad diagnostic categories: (a) depression, (b) anxiety, and (c) other. The mental-health measures most used in the depression category were different translations of the DASS-21 (Lovibond & Lovibond, 1995), which was used seven times, followed by different versions and translations of the BDI (Beck & Beamesderfer, 1974; Beck et al. 1996; Beck & Steer, 1987), which was used in six studies. The Patient Health Questionnaire (Spitzer et al., 1999) was used in four studies. The mental-health measures included in the anxiety category were used to identify different forms of anxiety, such as social phobia, agoraphobia, general levels of anxiety, and OCD symptoms and severity. The measure most often employed in the studies was the DASS-21 (Lovibond & Lovibond, 1995), in different translations, which was used in seven studies. This was followed by different versions and translations of the BAI (Beck et al., 1988; Beck & Steer, 1990), which was used in three studies, and the State Trait Anxiety Inventory (Spielberger et al.,1970), which was also used in three studies. The Social Phobia and Anxiety Inventory (Beidel et al., 1989) was used in two studies. The mental-health measures used in the “other” category focused on psychosomatic symptoms, PTSD, and avoidant personality disorder. The measure most often employed was the Posttraumatic Stress Disorder Reaction Index (Steinberg et al., 2004), which was used twice (Table 2).
Relationship between sensitivity and mental health
All the studies included in the systematic review that used the total score of the HSPS found positive correlations between sensitivity and mental-health outcomes. The summary of the included studies shows that sensitivity is positively correlated with a variety of mental-health outcomes, such as depression, anxiety, social phobia, agoraphobia, psychosomatic symptoms, OCD, PTSD, and avoidant personality disorder. The strength of these correlations ranges from weak (r = .05) to strong (r = .65, p < .01), mostly centering around a moderate effect size.
The three studies (Khosravani et al., 2021; Liss et al., 2008; Takahashi et al., 2020) that explored the relationship between mental-health outcomes and the three HSPS subscales—EOE, LST, and AES—found that the subscales vary in their correlations with mental-health outcomes; AES had the weakest correlation. For example, in Liss et al. (2008), only EOE and LST were significantly correlated with depression, whereas AES was not. In the same study, AES showed the weakest correlation with anxiety (r = .24, p < .001) out of the three subscales. In the study by Khosravani et al. (2021), AES was not associated with OCD severity, whereas LST correlated with OCD severity. In the same study, all three subscales showed correlations with general level of anxiety, but AES was correlated with only one OCD symptom (“unacceptable thoughts”), whereas the other two subscales showed positive correlations with multiple OCD symptoms. Khosravani et al. (2021) further showed that that all three subscales significantly correlated with depression—EOE showed the strongest correlation (r = .43, p < .001). Again, it was AES that showed the lowest correlation (r = .15, p < .05) out of the three subscales.
Meta-analysis
Based on the studies included in the mental-health-outcome categories depression and anxiety, we conducted two separate meta-analyses to establish the overall effect size.
Characteristics of included studies
All mental-health outcomes from the two categories depression and anxiety were included in the meta-analysis, except for three studies (Khosravani et al., 2021; Liss et al., 2008; Takahashi et al, 2020), which focused exclusively on the relationship between mental health and the three HSPS subscales instead of the total HSPS score. Another reason for exclusion was if the correlation between HSPS and depression and anxiety was not reported separately (Cadogan et al., 2023). In addition, all other studies from the “other” category were also excluded from the meta-analysis (Grinapol et al., 2022; Karam et al., 2019, 2024; Meyer & Carver, 2000). Therefore, eight studies from the 33 studies had to be excluded from the meta-analysis, resulting in a total of 25 studies. The meta-analysis for depression featured 22 study outcomes, and the meta-analysis for anxiety featured 14 study outcomes. The total number of participants of all 25 studies included was 8,428.
Effect size for sensitivity and mental-health outcomes
Figures 2 and 3 show the forest plots for depression and anxiety. Each plot displays the effect size of each study included and its CI and the estimated global effect size and its CI.
Figure 2 illustrates meta-analysis results derived from effect sizes relating to the correlation between sensitivity and depression and includes 22 study outcomes. The pooled z score among these studies is 0.38 (95% CI = [0.31, 0.45]). Translated to the original correlation-coefficient scale, this corresponds to a medium, highly significant correlation coefficient of r = .36 (95% CI = [.30, .42], p < .001). Figure 2 also highlights that all studies individually produced statistically significant positive correlations. Dong et al. (2022) came closest to not producing a significant result, with the most conservative correlation of r = .05 (95% CI = [.01, .09]). The influence of studies on the pooled effect size had little variation. Hjordt and Stenbæk (2019) had the smallest weight (2.12%) and the smallest sample size (N = 30) of the studies included. Dong et al. (2022) had the largest sample size (N = 2,133) and therefore the largest weight (5.57%). The relatively small variation in weightings despite large differences in sample size can be attributed to the considerable heterogeneity present in the meta-analysis (τ2 = .02, I2 = 88%, p < .001). The presence of heterogeneity means that although there is strong evidence of a positive moderate correlation overall, it is possible for individual studies to produce smaller z scores/correlations. This is apparent given that the 95% PI associated with the pooled effect is 0.06 to 0.69 on the z-score scale and .06 to .60 expressed as correlation coefficient.
Figure 3 illustrates the equivalent meta-analysis containing effect sizes relating to the correlation between sensitivity and anxiety and includes 14 study outcomes in total. The pooled z score of this meta-analysis is 0.42 (95% CI = [0.36, 0.47]). The pooled correlation coefficient is r = .39 (95% CI = [.34, .44], p < .001) when transformed from this z score and therefore is similar in strength and statistical significance to the depression-outcome meta-analysis. However, one individual study (Hofmann & Bitran, 2007) did not produce significant results. The study with the largest sample size (N = 484) and weight (8.84%) for the pooled results is the study by Attary et al. (2022). The study with the smallest sample size (N = 38) and weight (2.81%) is the study by Hoffmann et al. (2022). There is a slightly larger difference in weights compared with the depression analysis despite a smaller range of sample sizes. This is due to a lower level of heterogeneity estimated from the random-effects model (τ2 = .01, I2 = 59%, p < .001). The 95% PI for the pooled z score was 0.23 to 0.61, and translated to the r correlation-coefficient scale, it was .22 to .54.
In both meta-analyses, the estimated PI is wider than the CI because it incorporates both sampling variability and the heterogeneity across included studies.
Discussion
The aim of this study was to systematically review the existing literature on the relationship between trait sensitivity, often referred to as “sensory-processing sensitivity” or described with the umbrella term “environmental sensitivity,” and common mental-health problems in adolescents and adults, followed by a meta-analysis to establish the overall strength of this association. Our hypothesis was that sensitivity, measured with the HSPS or the HSCS, would be positively and moderately associated with various mental-health disorders, including depression and anxiety.
The systematic review, which included 33 studies in total, revealed positive and moderate correlations between sensitivity and various mental-health outcomes, such as depression, anxiety, psychosomatic symptoms, OCD, PTSD, agoraphobia, social phobia, and avoidant personality disorder.
A random-effect meta-analysis was then employed to establish the overall effect size of the relationship between sensitivity and the two most common mental-health outcomes: depression and anxiety. Our findings show a moderate and significant association for both depression and anxiety. This supports our hypothesis and confirms that sensitivity is significantly correlated with common mental-health outcomes.
Our observation that sensitivity correlates with many different common mental-health problems beyond depression or anxiety raises the question of whether a transdiagnostic perspective of mental health (Clark, 2009; Dalgleish et al., 2020) could be particularly useful when it comes to further understanding the role of the trait in mental health and its clinical application. Based on our findings, the sensitivity framework seems to be in line with a broad approach to etiology, conceptualization, and treatment that is less confined by diagnostic categories and diagnostic-specific interventions. This is because sensitivity correlates with many different mental-health problems. For example, it seems feasible that individuals, irrelevant of their diagnosis, who score high on the HSPS subscales EOE and LST may especially benefit from treatment plans focusing on strengthening emotional-regulation skills, applied relaxation, mindfulness, and so on. In turn, individuals with high levels of AES might respond particularly well to the positive effects of arts, music, and nature. Considering the comorbidity of diagnoses and the heterogeneity of clinical presentations in clinical contexts, sensitivity appears to represent a promising transdiagnostic risk factor.
The strength of the overall effect size was similar for anxiety and depression, but the association between sensitivity and anxiety shows a greater homogeneity. One possible explanation for this could be that core aspects of sensitivity, such as depth of processing or the tendency to respond with overstimulation, are more similar to or overlap with symptoms of anxiety rather than symptoms of depression regardless of environmental influences. For example, feeling physically and emotionally aroused because of overstimulation is likely experienced as feeling anxious or could lead to feelings of anxiety and subsequent avoidance of certain situations. Depth of processing might reflect a tendency to worry about future outcomes or could lead to imagining possible future scenarios in a given situation that could account for some anxiety. Depression, on the other hand, might be more dependent on the environmental factors and the quality thereof. For example, some studies have shown lower levels of depression in highly sensitive individuals who have grown up in supportive and positive environments but higher levels of depression in highly sensitive individuals who have grown up in adverse, emotionally unsupportive environments (E. N. Aron et al., 2005; Slagt et al., 2018). Hence, the likely variability in environmental quality between individuals and samples might account for greater heterogeneity in the association between sensitivity and depression.
When considering the three subscales of the HSPS in more detail, it is notable in our findings that AES showed a consistently weaker or no correlation at all with mental-health outcomes. This suggests that different facets of the HSPS relate differently to mental-health problems. This is in line with previous studies (Benham, 2006; Brindle et al., 2015; Lionetti et al., 2022), mentioned in the introduction of our study, which offer possible explanations for the underlying mechanisms that could drive the association between sensitivity and depression and anxiety. All the suggestions for the reasons why sensitivity correlates with mental-health outcomes focus not on the global trait as such but on specific aspects of the trait, such as depth of processing, emotional reactivity, and overstimulation. It seems that the more challenging aspects of sensitivity are captured in the HSPS subscales EOE and LST and less so in the subscale AES. This could explain its weaker correlation with mental-health outcomes found in our study.
Looking beyond the correlation with depression and anxiety, it is noticeable that we found moderate and positive correlations with agoraphobia and avoidant personality disorder in three studies (Hofmann & Bitran, 2007; Meyer & Carver, 2000; Neal et al., 2002). These correlations in addition to the moderate correlation with social introversion found in a previous study (E. N. Aron & Aron, 1997) invite the question of whether agoraphobic withdrawal and avoidance could be interpreted as maladaptive coping strategies—in response to overstimulation and emotional reactivity—that are particularly common in individuals with high levels of sensitivity.
Strengths and limitations
To our knowledge, this is the most extensive systematic review on sensitivity and mental health in adolescents and adults and the first meta-analysis on the topic to estimate the global effect size of this relationship.
However, there are several limitations that need to be addressed. First, most of the studies included used convenience samples, usually students, that predominantly consisted of young, highly educated women. This overrepresentation of women and the homogeneous sampling make it difficult to predict whether the observed correlations might also apply to a more diverse population. Second, most studies included were not preregistered. Third, only two studies (Grinapol et al., 2022; Holm et al., 2019) featured clinical samples. Fourth, all included studies employed a correlational design (one study also employed an experimental design), and of these, only five were longitudinal. This makes it difficult to draw causal inferences as to whether sensitivity precedes mental health. It could also be the case that heightened sensitivity is a consequence of mental-health problems. Thus, longitudinal and experimental designs are required to further investigate the relationship between sensitivity and mental health. Finally, all included studies relied on self-report measures, which are subject to social-desirability bias and the participant’s subjectivity and are influenced by the participant’s specific level of introspection.
Future research
Despite these limitations, the current findings are informative for future research in several ways. Most important, our findings support the notion that the personality trait of sensitivity should be considered as an important factor in clinical research and practice.
The effect size for the correlation between sensitivity and depression is similar in strength to the much researched relationship between neuroticism and depression (Chow & Roberts, 2014; Jourdy & Petot, 2017; Kotov et al., 2010). Because sensitivity is also moderately correlated with neuroticism, based on findings from a meta-analysis on sensitivity and the Big 5 personality traits by Lionetti et al. (2019), which was further supported by Pluess et al. (2023), it remains unclear to what degree the identified association between sensitivity and mental health is mediated or explained by neuroticism. Future research on sensitivity and mental health should address this question by exploring the role of neuroticism in relation to sensitivity and mental health.
The use of clinical samples in future research could help to explore whether the established relationship between sensitivity and common mental-health problems is similar in strength in a clinical context. This will also provide further insights into whether and how sensitivity shapes the effectiveness of therapeutic interventions or treatment outcomes in clinical-therapeutic settings. More specifically, future research should employ randomized controlled trials to explore the efficacy of specific therapeutic interventions (e.g., cognitive restructuring, mindfulness, emotion-focused interventions) for clients differing in their sensitivity levels (e.g., high, medium, and low). Apart from more varied research designs (e.g., longitudinal studies) and sampling methods (e.g., control group), future research should also ensure that samples are more gender-balanced and varied in age and investigate whether gender and age moderate the relationship between sensitivity and mental-health outcomes. For example, in a study by Ueno et al. (2019) that focused on the relationship between sensitivity and age, it was found that the two HSPS subfactors, LST and EOE, decreased linearly with age, whereas the third subfactor, AES, increased. Future research should further explore this in relation to mental-health outcomes.
Given their different associations with mental health, with AES being less associated with mental health in contrast to EOE and LST, the HSPS subscales should be explored in more depth in future research. Focusing on both, the total HSPS score and its subscales may provide clinicians with the possibility of creating a “sensitivity profile” (e.g., low in AES, high in EOE) of a person in treatment with implications for treatment plans. Future research could address how different sensitivity profiles might relate to disorder-specific symptoms and clinical presentations (e.g., negative cognitive styles, maladaptive schemas), treatment, and relapse prevention.
In addition, the use of alternative sensitivity measures for adults and adolescents that are not limited to self-reports, such as structured interviews similar to the newly developed Highly Sensitive Child Interview (Kähkönen et al., 2024), will be crucial to advance knowledge on sensitivity and mental health.
Clinical implications
The findings of this study suggest that sensitivity should be considered more in clinical practice. Considering that about 31% of the general population can be considered highly sensitive (Lionetti et al., 2018) and that sensitive individuals seem to respond better to some psychological interventions than less sensitive individuals (Lionetti et al., 2018; Nocentini et al., 2018; Pluess & Boniwell, 2015), sensitivity may be relevant not only for the etiology of psychological disorders but also for psychoeducation, treatment, and relapse prevention. To begin with, it seems crucial that awareness of sensitivity is improved among mental-health-care professionals so that clinicians and practitioners can recognize the trait in their patients early on in their treatment. Sensitivity could be a useful component in a patient’s formulation in addition to other relevant aspects (e.g., individual characteristics, biographical experiences, adaptive/maladaptive behaviors, core beliefs, negative automatic thoughts, maladaptive schemas). Apart from therapeutic work with adult patients, Assary et al. (2023) further suggested that the sensitivity framework may also inform therapeutic work with children and adolescents in particular. This is because it provides the opportunity to reframe emotionally reactive responses in some adolescents as a sign of their sensitive disposition instead of or at least in addition to a potentially more stigmatizing diagnostic label. In addition, educating young patients and their carers about the trait of sensitivity might help to improve resilience because the concept introduces the idea that highly sensitive adolescents are more responsive to treatment, not less responsive. This could be an important and valuable message early on in treatment of vulnerable adolescents.
However, further research is required for a better understanding of whether and how an individual’s level of sensitivity shapes treatment response and experiences and needs in therapy. For example, an early study on sensitivity and psychological interventions by Soons et al. (2010) found that highly sensitive clients benefited disproportionately from a mindfulness-based stress-reduction program aimed at reducing their levels of social anxiety and stress while increasing their levels of self-acceptance. Given that Soons et al. did not use the HSPS but the Dutch version of the abbreviated Adult Temperament Questionnaire (Rothbart et al., 2000), it was not included in our systematic review and meta-analysis. However, findings highlight that better knowledge of sensitivity might help clinicians and practitioners to tailor and individualize psychological support and interventions in accordance to the individual level of sensitivity of the patient. This could help to make treatment and relapse prevention more effective.
Given that highly sensitive individuals are more likely to experience more frequent and intense emotional responses to environmental stimuli in combination with strong cognitive reactivity, improving emotional-regulation skills may represent an essential part of treatment and relapse prevention for highly sensitive individuals. Wyller et al. (2017), for instance, in accord with Lionetti et al. (2022), theorized that the relationship between sensitivity and mental health is due to the key characteristics of sensitivity—depth of processing or cognitive reactivity—which contributes to maladaptive thought content and processes. Hence, Wyller et al. suggested that future research and therapeutic interventions should focus on this particular key aspect of sensitivity. They proposed that mindfulness-based cognitive therapy might be particularly beneficial for highly sensitive individuals in treatment given that it targets cognitive reactivity. The aforementioned findings by Soons et al. (2010) seem to support their theory that mindfulness-based therapies may be especially helpful for highly sensitive individuals in treatment. Furthermore, the findings by Brindle et al. (2015) and Bakker and Moulding (2012)—both included in our study—also point toward the relevance of mindfulness-based interventions. Brindle et al. found that the association between sensitivity and depression was partially mediated by acceptance of negative affective states, whereas Bakker and Moulding concluded that mindfulness and acceptance mediated the association between sensitivity and anxiety. However, other emotion-regulation skills that are not necessarily mindfulness-based (e.g., improving distress tolerance, increasing interpersonal effectiveness, developing emotional or behavioral strategies to self-soothe, formulating alternative thoughts and more adaptive behaviors, improving problem-solving skills) but instead draw from cognitive-behavioral therapy, emotion-focused therapy, or dialectical-behavioral therapy could be of clinical relevance for highly sensitive individuals in treatment, too. This requires further exploration in clinical science and practice.
Conclusion
In this systematic review and meta-analysis, we identified a positive and significant relationship between sensitivity and common mental-health problems, such as depression and anxiety. Results could have implications for future research and clinical practice and justify further exploration of the relationship between sensitivity and mental health. More research is needed, in particular to investigate the role of sensitivity in clinical populations and test whether and how sensitivity influences the effectiveness of therapeutic interventions.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026251348428 – Supplemental material for The Relationship Between Environmental Sensitivity and Common Mental-Health Problems in Adolescents and Adults: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cpx-10.1177_21677026251348428 for The Relationship Between Environmental Sensitivity and Common Mental-Health Problems in Adolescents and Adults: A Systematic Review and Meta-Analysis by Tom Falkenstein, Luke Sartori, Margherita Malanchini, Kristin Hadfield and Michael Pluess in Clinical Psychological Science
Footnotes
Acknowledgements
We especially acknowledge the invaluable contribution to Dean Langan from University College London for overlooking the preparation and conduction of the meta-analysis.
Transparency
Action Editor: Jennifer L. Tackett
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.