
Abstract
If psychopathology behaves like a complex dynamic system, sudden onset or worsening of symptoms may be preceded by early-warning signals (EWSs). EWSs could thus reflect personalized warning signals for impending psychopathology. We empirically investigated this hypothesis in at-risk youths (N = 122, mean age = 23.6 ± 0.7 years, 57% males) from the clinical cohort of Tracking Adolescents’ Individual Lives Survey (TRAILS-CC), who provided daily emotion assessments for 6 months. We analyzed whether EWSs (rising autocorrelations and standard deviations in emotions) preceded transitions toward psychopathology. Across indicators and a range of analytical options, EWSs had low sensitivity (M = 26%, SD = 11%) and moderate specificity (M = 75%, SD = 14%). Thus, in the present sample, the proposed generic nature and clinical utility of EWSs could not be substantiated. Given this finding, we call for a more nuanced view on the application of complex-dynamic-systems principles to psychopathology and lay out key questions to be addressed in the future.
Keywords
Mental health varies over time: Periods without symptoms of psychopathology may be followed by periods with symptoms and vice versa (Hofmann & Curtiss, 2018). Alternations between such periods can occur suddenly and are difficult to foresee. For instance, relapse of depression or onset of psychosis can occur abruptly, in absence of an obvious trigger (Hayes et al., 2007). This challenges timely detection of emerging psychopathological disorders and hampers prevention and early-intervention efforts.
A complex-systems perspective on psychopathology provides a novel view on the early detection of progressing symptoms. According to this perspective, mental health can be described by alternative states (e.g., mental health vs. mental ill health). When these states are stable, they are resilient to external perturbations (see Fig. S1 in the Supplemental Material available online). This means that stressful situations (perturbations) trigger only brief negative emotions 1 or symptoms of psychopathology. As the instability of mental-health states accumulates, the system’s resilience to perturbations declines (a phenomenon referred to as “critical slowing down”; Scheffer, 2009; Scholz et al., 1987). This means that the negative emotions evoked by perturbations increasingly linger over time. Eventually, the system may reach its tipping point: Negative emotions no longer recede, and a transition toward mental ill health takes place. The critical aspect is that at this point, even small, seemingly innocent perturbations could trigger a transition—and therefore, it may be experienced as sudden and unpredictable. Yet in a wide range of complex systems, such transitions can be anticipated by monitoring the gradual rise of instability in the system (Cramer et al., 2016; Jeronimus, 2019; Olthof et al., 2020; Wichers et al., 2019).
The stability of complex systems can be inferred from certain dynamics in time-series data. Specifically, rising instability coincides with rising autocorrelations, variances, and cross-correlations (Scheffer et al., 2009). These measures are collectively referred to as early-warning signals (EWSs) and have been shown to anticipate a variety of transitions, including sudden crashes of financial markets (Wen et al., 2018), shifts between sleep stages (de Mooij et al., 2020), epileptic seizures (Maturana et al., 2020), the extinction of species (Clements & Ozgul, 2016), the outbreak of a global pandemic (Kaur et al., 2020), and climate changes (Dakos et al., 2008). If psychopathology behaves similarly to these other complex systems, transitions between mental-health states could be anticipated by increasing lingering of emotions (autocorrelation) and rising amplitudes or frequencies of fluctuations (variation) and increasingly strong cross-correlations in emotions. This means that EWSs could have the potential to prospectively indicate individuals’ risk for the onset or worsening of psychopathology.
The suggestion that EWSs may be informative of psychopathology fits well with the finding that individuals who report higher symptom severity also tend to experience higher autocorrelations (Houben et al., 2015; Koval et al., 2012; McGorry et al., 2018; van de Leemput et al., 2014), variances (Houben et al., 2015; Sperry et al., 2020), and cross-correlations in negative emotions (Houben et al., 2015; Nelson et al., 2018). The prospective associations between these respective dynamics and psychopathology are still ambiguous, which might be due to methodological heterogeneity across studies (e.g., the time interval between assessments of emotions and assessments of symptom severity; characteristics of sample and design; Brose et al., 2015; Curtiss et al., 2019; Kuppens et al., 2012; Sperry et al., 2020). Note that the aforementioned studies all investigated between-persons processes (i.e., Do individuals with relatively large symptom transitions also report relatively high levels of EWSs?). Complex-systems principles, in contrast, concern within-persons processes (i.e., Are symptom transitions preceded by rising EWSs in individuals?). To date, the only confirmation of the latter question came from two case studies (Wichers et al., 2016, 2020) and one larger study (N = 31; Curtiss et al., 2019), all involving individuals diagnosed with depression. Thus, although earlier studies were mostly in line with what would be expected according to complex-systems principles, extensive empirical support for EWSs as personalized risk markers for future transitions in psychopathology (beyond depression) is still lacking.
To evaluate complex-systems principles in psychopathology at a within-persons level, mental health should be monitored in real time, as it unfolds in individuals. This is practically challenging because it requires individuals to register their emotions frequently (e.g., daily) during a period in which transitions in mental health are likely to occur (Wichers et al., 2016, 2020). The two previous case studies met this requirement and found that EWSs—indexed by autocorrelations, variances, and cross-correlations in negative emotions—preceded a relapse in depression (Wichers et al., 2016, 2020). These initial findings call for a more systematic investigation into the sensitivity and specificity of EWSs—which will ultimately help to determine the utility of EWSs to clinical practice. In the current study, we therefore investigated whether EWSs anticipate transitions in mental health in a large sample of young adults at increased risk for cross-diagnostic psychopathology. In line with previous studies (Wichers et al., 2016, 2020), we focused on rising autocorrelations and standard deviations as EWSs. Our first aim was to establish the sensitivity and specificity of EWSs. Using daily diary data covering a 6-month period from 122 individuals, we investigated how often transitions in mental health were preceded by EWSs in positive and negative emotions (sensitivity). We also analyzed how often EWSs emerged in individuals who did not undergo transitions in mental health (specificity). Second, we aimed to investigate the probability of a transition in mental health upon detection of EWSs (predictive values 2 ). Given that the detection of EWSs requires many methodological decisions, for instance pertaining to the type of emotions that are monitored and the type of analyses conducted, our third aim was to compare different methods for detecting EWSs. This third aim was not included in our preregistered analyses (see https://www.osf.io/fumrx) but fits well with the exploratory nature of this study and the current status of the field. By providing a comprehensive description of the sensitivity, specificity, and predictive values of EWSs in different methodological settings, we hope to provide a clearer picture of if and when EWSs may have clinical utility.
Method
Procedure
Data were retrieved from the TRacking Adolescents’ Individual Lives Survey (TRAILS) Transitions in Depression 3 (TRANS-ID) study, which was described in detail elsewhere (Schreuder et al., 2020). Briefly, the study included 134 participants from the clinical cohort of TRAILS (Huisman et al., 2008). TRAILS is an ongoing, prospective cohort study with biennial or triennial assessments investigating the development of mental health from preadolescence into adulthood. Participants enrolled in the clinical cohort of TRAILS (TRAILS CC) were referred to a child psychiatric outpatient clinic in the northern Netherlands any time before the age of 11. Because of this history, they are considered at increased risk for psychopathology across the diagnostic spectrum.
TRAILS TRANS-ID was conducted as an add-on study to the regular assessment waves of TRAILS CC. Of the 443 participants who were invited, 134 agreed to participate in TRAILS TRANS-ID. At the time of enrollment in TRAILS TRANS-ID, participants were approximately 23 years old. TRAILS TRANS-ID included a 6-month daily diary study and aimed to investigate the day-to-day fluctuations in emotions in individuals at increased risk for psychopathology. The TRAILS TRANS-ID study was approved by the local Medical Ethical Committee (Reference No. 2017/203). All participants provided written informed consent. All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Diary study
The diary study involved the completion of a questionnaire (diary) every evening for a period of 6 months. Participants received these questionnaires through a link sent in a text message to their mobile phones. Questionnaires assessed thoughts and feelings during the past day (e.g., “To what extent did you feel down today?”) and were rated on a visual analogue scale ranging from 0 (not at all) to 100 (very much). Each questionnaire consisted of 58 items, of which 17 assessed positive emotions (e.g., happy, relaxed, at ease with others), 35 assessed negative emotions (e.g., stressed, tired, irritated), and six concerned event appraisal and drug and alcohol consumption (not included in the present study). Although we consider most of these daily assessments reflective of subthreshold symptoms of psychopathology, we refer to these daily assessments as “positive and negative emotions” in the interest of readability. A more elaborate description of the diary study and a list of all assessed items were reported elsewhere (Schreuder et al., 2020).
Diagnostic interview
Immediately before and after the diary study, the short version of the Schedules for Clinical Assessment in Neuropsychiatry (mini-SCAN) was administered (Nienhuis et al., 2010). The mini-SCAN is a semistructured diagnostic interview that assesses whether individuals meet the criteria for a psychiatric disorder according to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (i.e., mood, anxiety, psychotic, substance use, and attention-deficit/hyperactivity disorder [ADHD]; American Psychiatric Association, 2013). Furthermore, the mini-SCAN includes a screener for autism spectrum disorder. The mini-SCAN was complemented by the aggressive behavior subscale of the Adult Self Report (ASR; Achenbach, 1997), which covers oppositional or antisocial behavior. Both mini-SCAN and the ASR subscale were orally administered by trained interviewers (M. J. Schreuder, R. N. Groen, and a research assistant supervised by M. J. Schreuder and R. N. Groen).
Social functioning
In addition to the diagnostic interview, we assessed social functioning using the Groningen Social Behaviour Questionnaire (in Dutch: Groningse Vragenlijst Sociaal Gedrag [GVSG]; de Jong & van der Lubbe, 2001). The GVSG assesses functioning on nine different domains: parents, partner, younger children, older children, friends, education, occupation, household, and leisure time. In each domain, five questions are rated on a 4-point Likert scale ranging from never to always. Functioning in each of these domains was assessed only if the domain was applicable to the participant (e.g., in case of education, only if the participant was enrolled in education). The domain older children, which reflected participants’ relationship with their children older than 15, was not applicable to any participant and is therefore not described further. On the basis of cutoff scores (de Jong & van der Lubbe, 2001), we categorized scores as reflecting severe impairments, mild impairments, or no impairments in functioning.
Analyses
Analyses consisted of the following steps, which are each described in detail below. First, we defined time series of each individual’s mental health and ill health on the basis of a combination of time series of several positive and negative emotions, respectively. Second, we identified whether and at what moment in time individuals experienced a transition toward psychopathology in these composite time series (see Transitions Toward Psychopathology section). Finally, for each individual and each of the 17 positive and 35 negative emotions separately, we estimated time-varying trends in the autoregressive coefficient (AR) and the standard deviation (see EWSs section). Significant rises in the AR or the standard deviation occurring within 1 or 2 weeks before a transition in mental health were considered to reflect an EWS. The sensitivity, specificity, and predictive values of EWSs were evaluated by examining the relative prevalence of EWSs (a) in individuals who experienced a transition toward psychopathology (sensitivity; positive predictive value) and (b) in individuals who did not experience such a transition (specificity; negative predictive value). All analyses were conducted in R (Version 4.0.2; R Core Team, 2020).
Transitions toward psychopathology
For each individual, we determined whether they experienced a transition toward psychopathology. Such transitions were defined as either a sudden drop in mental health and/or a sudden increase in mental ill health. Both mental health and mental ill health were considered latent constructs. Specifically, we defined mental health as the mean score of four items that reflected positive emotions (i.e., “I felt good,” “I felt happy,” “I could enjoy things,” and “My day was worth living”). These items were selected because they showed the highest loadings in a single-factor model of all 17 positive emotions in a subset of 10 randomly selected individuals (for additional details, see Section 2 in the Supplemental Material available online). Following a similar reasoning, we defined mental ill health as the mean score of the four items that showed the highest loadings in a single-factor model of all 35 negative emotions (i.e., “I felt down,” “I felt stressed,” “I was easily upset,” “I felt restless”; see Section 2 in the Supplemental Material). Thus, we retrieved time series of mental health and ill health for each individual. In both time series, we looked for sudden transitions using change-point analyses.
Change-point analyses iteratively fit left- and right-sided Gaussian Kernel linear regressions (bandwidth 15 observations) for each mental-health estimate in the time series for each individual separately (Muller, 1992). In other words, we estimated mental health at each time point on the basis of (a) all weighted previous observations 4 and (b) all weighted subsequent observations. The difference between the estimates based on previous observations and the estimates based on subsequent observations at a specific point in time is expected to increase if a sudden transition happened at that time point. This procedure was repeated for bootstrapped data. If the findings from empirical data were substantially different from the findings from bootstrapped data (α = .01), the time point with the largest discrepancy was considered a change point or transition point (for a detailed description and illustration, see Smit (2022) and Section 3 in the Supplemental Material). To determine the magnitude of transitions, we computed Cohen’s d using the formula below (Cohen, 1988; Cumming, 2012). Here, the size of transition t of individual i (di,t) is computed by dividing the difference between individual i’s mean mental (ill) health before the transition (mi1) and after the transition (mi2) by the pooled standard deviation. The latter can be derived from individual i’s standard deviation in mental (ill) health before (σi1) and after the transition (σi2):
EWSs
EWSs were operationalized as rising trends in the AR and standard deviation of emotions. For each individual and each emotion, we estimated (a) rises in the AR through generalized additive models (ARGAM; Bringmann et al., 2017), (b) rises in the AR through moving-window analyses (ARMW; Dakos et al., 2012), and (c) rises in the standard deviation through moving-window analyses (SDMW; Dakos et al., 2012). For each of these approaches, which are described in detail below, we varied several settings to evaluate the impact of methodological choices on the detection of EWSs. An overview of these variations is provided in Table 1.
Overview of Settings for Each Method
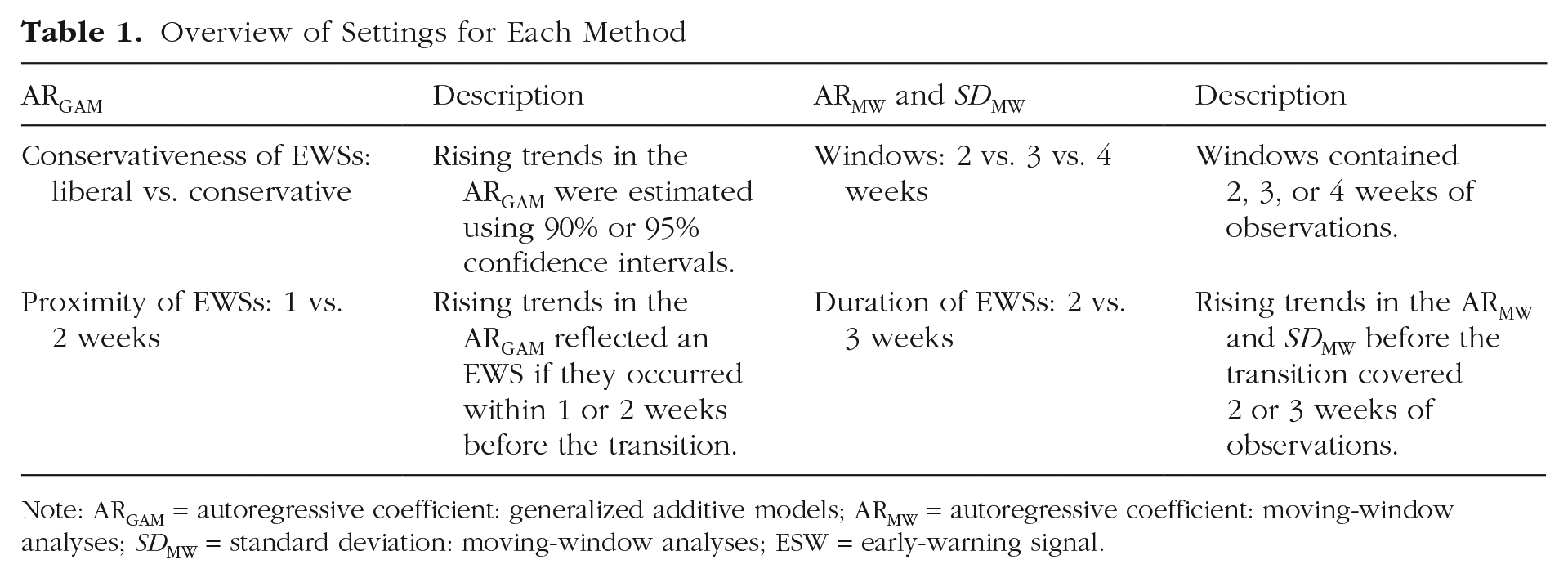
Note: ARGAM = autoregressive coefficient: generalized additive models; ARMW = autoregressive coefficient: moving-window analyses; SDMW = standard deviation: moving-window analyses; ESW = early-warning signal.
Generalized additive models
Generalized additive models can be used to predict an emotion at time t by (a) an intercept and (b) the emotion at t – 1 while allowing for gradual changes in both parameters (cf. a time-varying autoregressive model; Bringmann et al., 2017; Hastie & Tibshirani, 1986; Simpson, 2018; Wood, 2017). These gradual changes in parameters are estimated using nonparametric smooth functions based on thin-plate regression splines. Smoothness is determined by (a) the number of regression splines, which was set to 10 (Bringmann et al., 2017), and (b) a penalization parameter, which was selected by generalized cross-validation. Sudden transitions can be modeled by adding a dummy predictor that encodes the timing of the transition. Generalized additive models assume that the predefined maximum number of regression splines is sufficient to capture the dynamics of the time series. We checked this assumption using the effective degrees of freedom and their associated p values. Furthermore, generalized additive models assume that residuals are mutually independent and normally distributed with constant variance. This was examined using residuals diagnostics plots (Wood, 2017).
It is not yet possible to model rising variances using generalized additive models, and therefore, we could inspect only trends in the autoregressive coefficient (ARGAM). To estimate whether trends in the autoregressive coefficient were significantly increasing or decreasing, we computed the first derivative of the smooth function describing the autoregressive coefficient. This was done using the method of central finite differences described by Simpson (2018). Trends in the autoregressive coefficient were considered significant if the confidence interval around the first derivative did not include zero. If the rising trend occurred within 1 or 2 weeks before the transition, we considered this trend to reflect a warning signal. A similar approach was adopted elsewhere (Burthe et al., 2016; Sommer et al., 2017). In total, we estimated four types of generalized additive models in which we varied (a) the conservativeness of the EWS detection (liberal vs. conservative) and (b) the proximity of EWSs (1 vs. 2 weeks; Table 1). The conservativeness of the EWS detection is given by the confidence interval around the first derivative of the smooth function describing the trend in the autoregressive coefficient. Specifically, for liberal estimations, we computed 90% confidence intervals around the first derivative. If these confidence intervals did not include zero and the first derivative had a positive sign, we concluded that the autoregressive coefficient showed a rising trend. For conservative estimations, we used a confidence interval of 95% around the first derivative. Because this interval is wider, the probability that it does not include zero (and hence, the probability of detecting a rising autoregressive coefficient) is smaller. The second setting we varied concerns the proximity of EWSs. Again, this affects the likelihood that EWSs are detected: Because we allow more time between rising trends in the autoregressive coefficient and the transition, we will more often (falsely) detect EWSs. In sum, different settings of the generalized additive model will yield a different trade-off between the sensitivity and the specificity of EWSs for detecting transitions toward psychopathology.
Moving-window analyses
In moving-window analyses, EWSs are computed within segments (or window) of the time series. These windows slide through the time series by one time step. For instance, the autoregressive coefficient can be computed on the first 2 weeks of observations (X1–X14) and subsequently on X2–X15, X3–X16, and so on. This yields novel time series that depict how parameters computed within the windows, such as the autoregressive coefficient, evolve over time. Within each window, we computed the autoregressive coefficient on the basis of a first-order autoregressive model using detrended data (i.e., ARMW) and the standard deviation (i.e., SDMW). Subsequently, we determined whether there was a rising trend in the autoregressive coefficient and the standard deviation based on Kendall’s τ. To evaluate the impact of methodological decisions on the detection of EWSs, we varied (a) the size of windows (14 vs. 21 vs. 28 observations) and (b) the number of estimates used to compute Kendall’s τ (14 vs. 21 estimates). The size of windows—reflected by the number of observations within each window—determines the smoothness of trends in EWSs. Small windows may yield erratic patterns, whereas larger windows result in smoother trends. Window sizes further affect whether EWSs can be estimated at all: For small window sizes, missing observations within windows may make it impossible to estimate an autoregressive model. For larger window sizes, it may be impossible to fit sufficient windows before the transition for detecting a rising trend in EWSs. Hence, window sizes likely have an impact on the sensitivity and specificity of EWSs. The other setting we varied concerns the number of estimates used for determining rising patterns in the autoregressive coefficient and standard deviation. This introduces a trade-off between the proximity of EWSs—which is higher when a smaller amount of estimates is used—and the reliability of the trend—which is higher when more estimates are used. With three different window sizes and two different settings for computing Kendall’s τ, we estimated six different types of moving-window analyses (Table 1).
Sensitivity, specificity, and predictive values of EWSs
First, we determined the sensitivity of EWSs to detect transitions toward psychopathology by dividing the number of true positives (i.e., how many transitions were preceded by EWSs across individuals) by the total number of transitions for which EWSs could be computed across individuals. A sensitivity of 1, or 100%, indicates that a particular emotion always shows EWSs before a transition, whereas a sensitivity of 0 would mean that EWSs in a particular emotion never signal an upcoming transition. Given that we were primarily interested in anticipating worsening mental health, we inspected EWSs only before transitions toward psychopathology, which we defined as a sudden drop in mental health or a sudden increase in mental ill health. However, we also reported findings for transitions toward well-being (i.e., drops in mental ill health and/or increases in mental health) in Section 7 in the Supplemental Material to inform the interested reader and to rule out the possibility that our findings would be due to a selective focus on transitions toward psychopathology, as opposed to transitions toward well-being.
Second, we addressed the specificity of EWSs by evaluating EWSs in individuals without any transition in mental health. For these individuals, we defined a reference transition point that was equal to the average transition point of individuals who did experience a transition in mental health. If this reference transition would often be preceded by EWSs, the specificity of EWSs would be low. To provide a complete overview of sensitivity and specificity, we computed metrics both (a) for each emotion separately and (b) across emotions. The former reflects the probability of an EWS in a particular emotion given that there was a transition (sensitivity) or the probability of no EWS in a particular emotion given that there was no transition (specificity). The latter was defined as the probability of an EWS in any emotion given that there was a transition (sensitivity) or the probability of no EWS given that there was no transition (specificity). In either case, sensitivity and specificity were computed across individuals—and hence, reflect between-persons estimates.
Finally, we computed the predictive values of EWSs, which indicate the probability of a transition given that EWSs are detected (positive predictive value) and the probability that no transition will occur given that EWSs are not detected (negative predictive value). Predictive values take into account the overall probability of transitions (i.e., the proportion of people that experienced a transition). Together, sensitivity, specificity, and predictive values may inform the utility of EWSs for clinical practice. Formulas for computing sensitivity, specificity, and predictive values and a more detailed explanation of these measures are provided in Section 4 in the Supplemental Material.
Results
Participant characteristics
Of the 134 individuals who enrolled in TRAILS TRANS-ID, 122 (91.0%) completed the diary study. They completed on average 88.45% of diary assessments (SD = 9.87%), which is comparable with the compliance in less-intensive studies (Vachon et al., 2019; Table 2). All participants were of Dutch ethnicity, and most were enrolled in education (N = 72) and/or had a job (N = 65). Participants’ socioeconomic status, as assessed at enrollment in TRAILS-CC, matched the socioeconomic status of the general population in the Netherlands. Before the diary period (i.e., at baseline), 37 (30.33%) individuals met the criteria for at least one psychiatric disorder. After the diary period, 34 (27.87%) met diagnostic criteria. Most of these individuals (N = 23) were also diagnosed at baseline, whereas others (N = 11) experienced the onset of a disorder during the diary period. Mood disorders (N = 25 at baseline and N = 23 after the diary period), anxiety disorders (Ns = 20 and 11), and ADHD (Ns = 7 and 8) were most common. Approximately half of the participants (N = 62 at baseline and N = 68 at post) had severe impairments in at least one domain of social functioning. Impairments in functioning most often concerned problems in enjoying leisure time (e.g., feeling bored), problems in occupation (e.g., not performing well at work), and problems in engaging with friends (at baseline) or with a romantic partner (after the diary period; Table 2).
Sample Characteristics
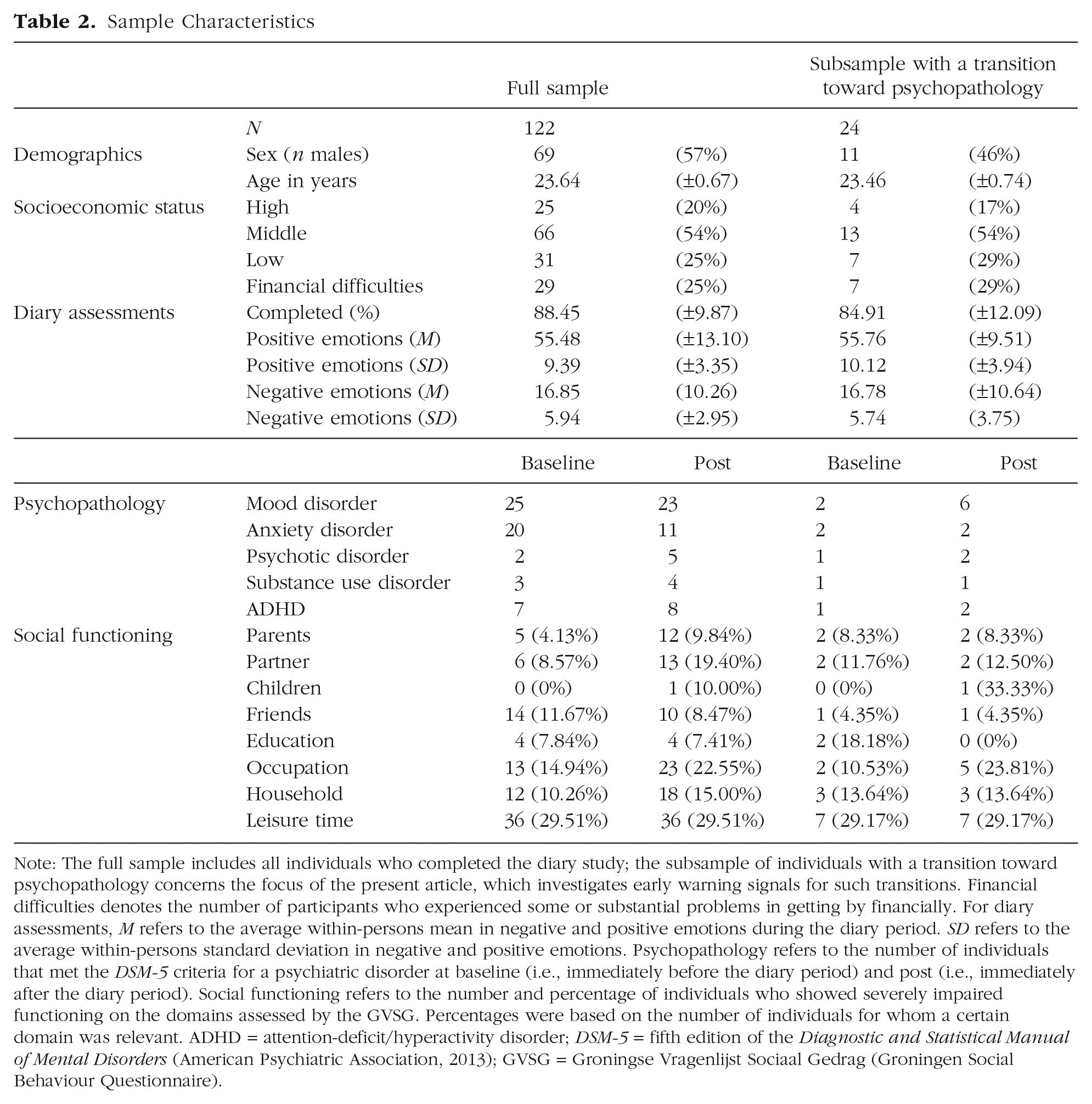
Note: The full sample includes all individuals who completed the diary study; the subsample of individuals with a transition toward psychopathology concerns the focus of the present article, which investigates early warning signals for such transitions. Financial difficulties denotes the number of participants who experienced some or substantial problems in getting by financially. For diary assessments, M refers to the average within-persons mean in negative and positive emotions during the diary period. SD refers to the average within-persons standard deviation in negative and positive emotions. Psychopathology refers to the number of individuals that met the DSM-5 criteria for a psychiatric disorder at baseline (i.e., immediately before the diary period) and post (i.e., immediately after the diary period). Social functioning refers to the number and percentage of individuals who showed severely impaired functioning on the domains assessed by the GVSG. Percentages were based on the number of individuals for whom a certain domain was relevant. ADHD = attention-deficit/hyperactivity disorder; DSM-5 = fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013); GVSG = Groningse Vragenlijst Sociaal Gedrag (Groningen Social Behaviour Questionnaire).
Transitions in mental health
Change-point analyses indicated that 51 individuals (41.80%) experienced a transition in mental (ill) health. Of these individuals, 24 (47.06%; 19.67% of the full sample) showed a transition toward psychopathology—indexed either by a drop in mental health (N = 13), an increase in mental ill health (N = 9), or a combination of both (N = 2). Given that two individuals experienced both a drop in mental health and an increase in mental ill health, there were 26 transitions toward psychopathology. For detailed information regarding the type of transitions that we found, see Table S3 in the Supplemental Material. On average, transitions happened halfway through the diary period (M = 100.23 days, SD = 45.91; range = 38–159). Transitions varied in magnitude, with a mean effect size of 0.65 (SD = 0.47; range = 0.004–1.61).
Individuals who experienced a transition toward psychopathology did not differ from the full sample in terms of sex, χ2(1) = 0.55, p = .46; age, t(144) = 1.23, p = .22; or the number of completed diary ratings, t(144) = 1.55, p = .12. Furthermore, the within-persons mean and variability of the diary ratings did not differ between individuals with a transition toward psychopathology and the full sample; positive emotions: M: t(144) = 0.10, p = .92; SD: t(144) = 0.95, p = .34; negative emotions: M: t(144) = 0.03, p = .97, SD: t(144) = 0.28, p = .78. Of those individuals who experienced a transition toward psychopathology, six met diagnostic criteria at baseline and eight individuals at post. The likelihood to meet diagnostic criteria at baseline or post did not differ between individuals who experienced a transition toward psychopathology and the full sample: at baseline, 25.00% vs. 30.33%, χ2(1) = 0.21, p = .65; at post, 33.33% vs. 27.87%, χ2(1) = 0.09, p = .77. Finally, participants who experienced a transition toward psychopathology did not differ from the full sample in their likelihood to experience severe problems in functioning in at least one domain at baseline (45.83% vs. 50.82%), χ2(1) = 0.05, p = .82, or post (50.00% vs. 55.74%), χ2(1) = 0.09, p = .77; or in the number of domains wherein they experienced problems at baseline (Ms = 0.79 vs. 0.74), t(144) = 0.27, p = .49, or post (Ms = 0.88 vs. 0.96), t(144) = 0.36, p = .72.
Overall sensitivity, specificity, and predictive values of EWSs
Depending on the method that was used to derive EWSs, most to all of the 26 transitions toward psychopathology were preceded by EWSs in at least one out of 52 emotions (ARGAM range = 85%–92%, ARMW = 100%, SDMW = 100%). An example of these EWSs is illustrated in Figure 1. Across emotions and individuals, the sensitivity of EWSs derived through generalized additive models (ARGAM range = 6%–10%) was considerably lower than the sensitivity of EWSs derived through moving-window analyses (ARMW range = 24%–30%, SDMW range = 30%–38%; Table 3). In terms of specificity, however, generalized additive models outperformed moving-window analyses (ARGAM range = 95%–98%, ARMW range = 70%–76%, SDMW range = 60%–67%). A similar pattern of results held for transitions toward well-being (see Section 7 in the Supplemental Material). The different detection rates of generalized additive models and moving-window analyses are further illustrated by differences in the average number of EWSs found in individuals. Specifically, generalized additive models detected around 4.72 EWSs on average per person depending on the settings used before transitions toward psychopathology (range = 1–18; Table 3). Moving-window analyses, in contrast, detected approximately 3 times as many EWSs in the autoregressive coefficient (±14.49, range = 4–29) and 4 times as many EWSs in the standard deviation (±18.11, range = 3–41, depending on the model settings) before transitions toward psychopathology.
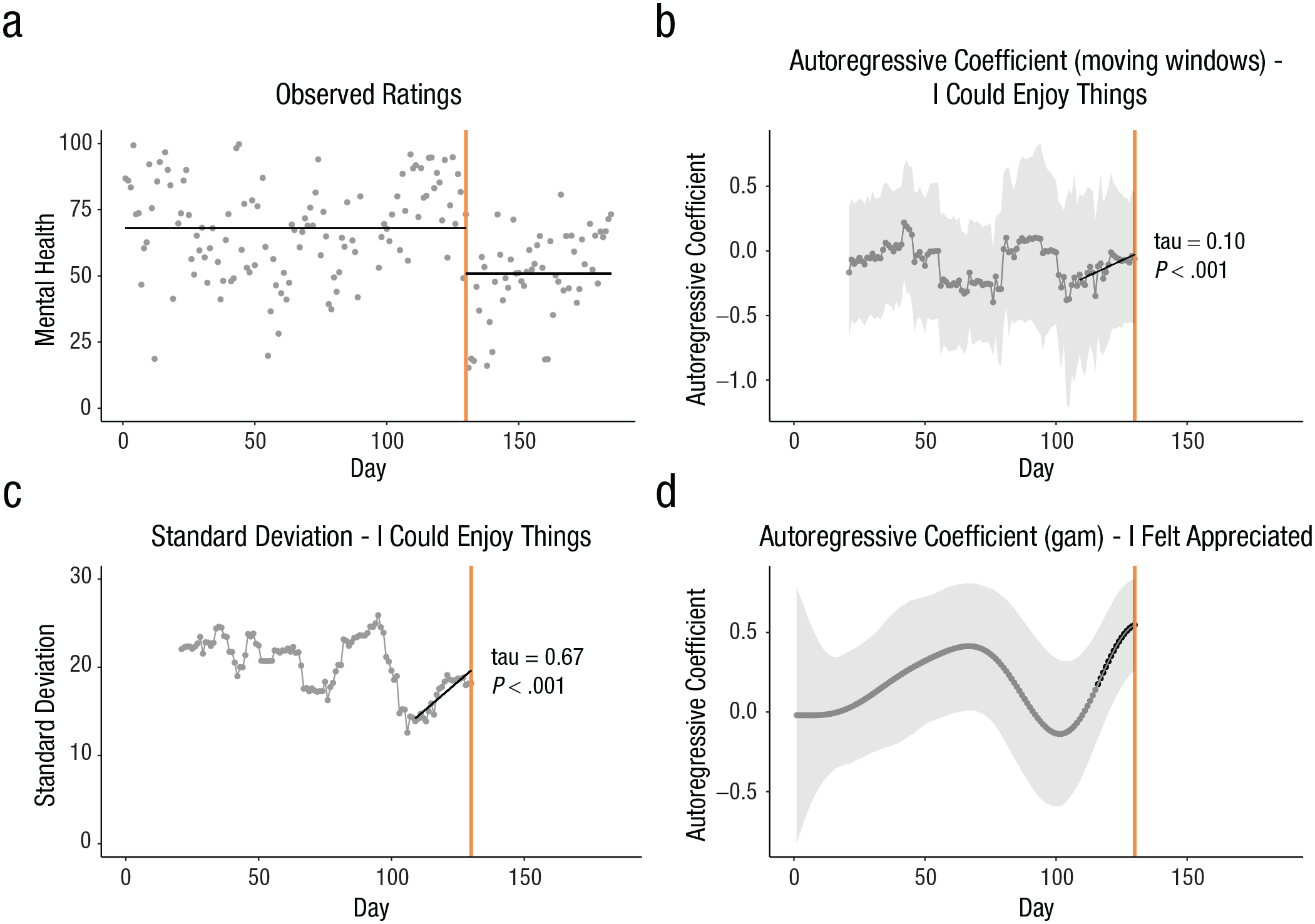
Empirical example of early warning signals (EWSs) in a single participant who experienced a transition toward psychopathology—indicated by a sudden drop in mental health represented by the orange vertical line—at day 130. (a) Observed scores of mental health (gray dots) and the mean mental-health score (horizontal black line) before and after the transition. (b) Changes in the autoregressive coefficient (ARMW) of “I could enjoy things” detected by moving-window analyses (window size and proximity of EWSs set to 3 weeks). The ARMW showed a rise before the transition (τ = .10, p < .001). Gray bands depict 95% confidence intervals. (c) Changes in the standard deviation (SDMW) of “I could enjoy things” detected by moving-window analyses (window size and proximity of EWSs set to 3 weeks). The SDMW showed a rise before the transition (τ = .67, p < .001). (d) Changes in the autoregressive coefficient (ARGAM) of “I felt appreciated” detected by generalized additive models (conservative estimation, proximity of EWSs set to 2 weeks). The black dots denote the estimates that were significantly rising before the transition. Gray bands depict 95% confidence intervals (plot B) or credible intervals (plot D).
Sensitivity, Specificity, and Predictive Values of EWSs as Predictors of Transitions Toward Psychopathology Across Methodological Settings
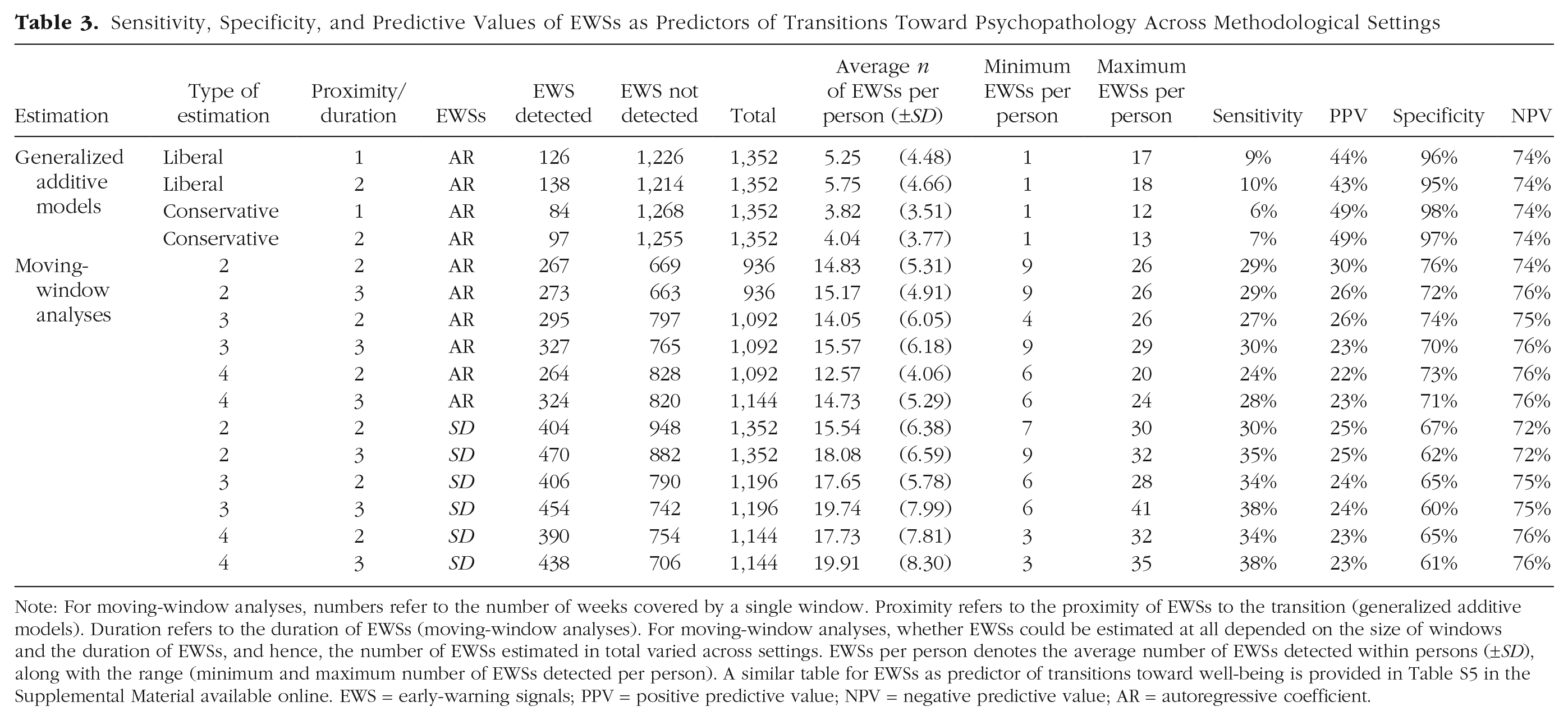
Note: For moving-window analyses, numbers refer to the number of weeks covered by a single window. Proximity refers to the proximity of EWSs to the transition (generalized additive models). Duration refers to the duration of EWSs (moving-window analyses). For moving-window analyses, whether EWSs could be estimated at all depended on the size of windows and the duration of EWSs, and hence, the number of EWSs estimated in total varied across settings. EWSs per person denotes the average number of EWSs detected within persons (±SD), along with the range (minimum and maximum number of EWSs detected per person). A similar table for EWSs as predictor of transitions toward well-being is provided in Table S5 in the Supplemental Material available online. EWS = early-warning signals; PPV = positive predictive value; NPV = negative predictive value; AR = autoregressive coefficient.
Whereas the sensitivity and specificity of EWSs indicate how often transitions are preceded by EWSs, predictive values indicate how often EWSs can be trusted. For instance, positive predictive values indicate how often EWSs reflect a true (as opposed to a false) alarm and varied between 43% and 49% (ARGAM), 22% and 30% (ARMW), and 23% and 25% (SDMW). Negative predictive values indicate the probability that a transition will not occur, given that EWSs are absent, and were comparable across indicators (ARGAM = 74%, ARMW range = 74%–76%, SDMW range = 72%–76%). In conclusion, EWSs indexed by ARGAM very seldomly anticipated transitions toward psychopathology but did raise the probability of a transition from 29% to 34% (prevalence 5 ) to 43% to 49% (positive predictive value). EWSs indexed by ARMW and SDMW, in contrast, often occurred before both transitions and nontransitions and therefore had low predictive utility.
Impact of methodological decisions
As depicted in Figure 2 and Table 3, the average sensitivity, specificity, and predictive values of EWSs varied considerably across settings used for estimating EWSs. Compared with a conservative estimation, a liberal estimation of the ARGAM led to a slightly higher sensitivity (9%–10% vs. 6%–7%) at the cost of specificity (95%–96% vs. 97%–98%). Differences in predictive values across settings were small (positive predictive values: 43%–44% vs. 49%) or absent (negative predictive values: 47% vs. 47%), and hence, the conservative and liberal estimation provided largely similar results. Varying the proximity of EWSs had little impact on the predictive capacities of EWSs indexed by the ARGAM. Conceptually, however, smaller proximities can be considered favorable because they suggest more precise warning signals (i.e., warning signals that are more proximal to the outcome they are supposed to forecast). In sum, whereas EWSs indexed by the ARGAM had limited predictive capacities in all settings, an estimation with a proximity of 1 week worked best in the current sample.
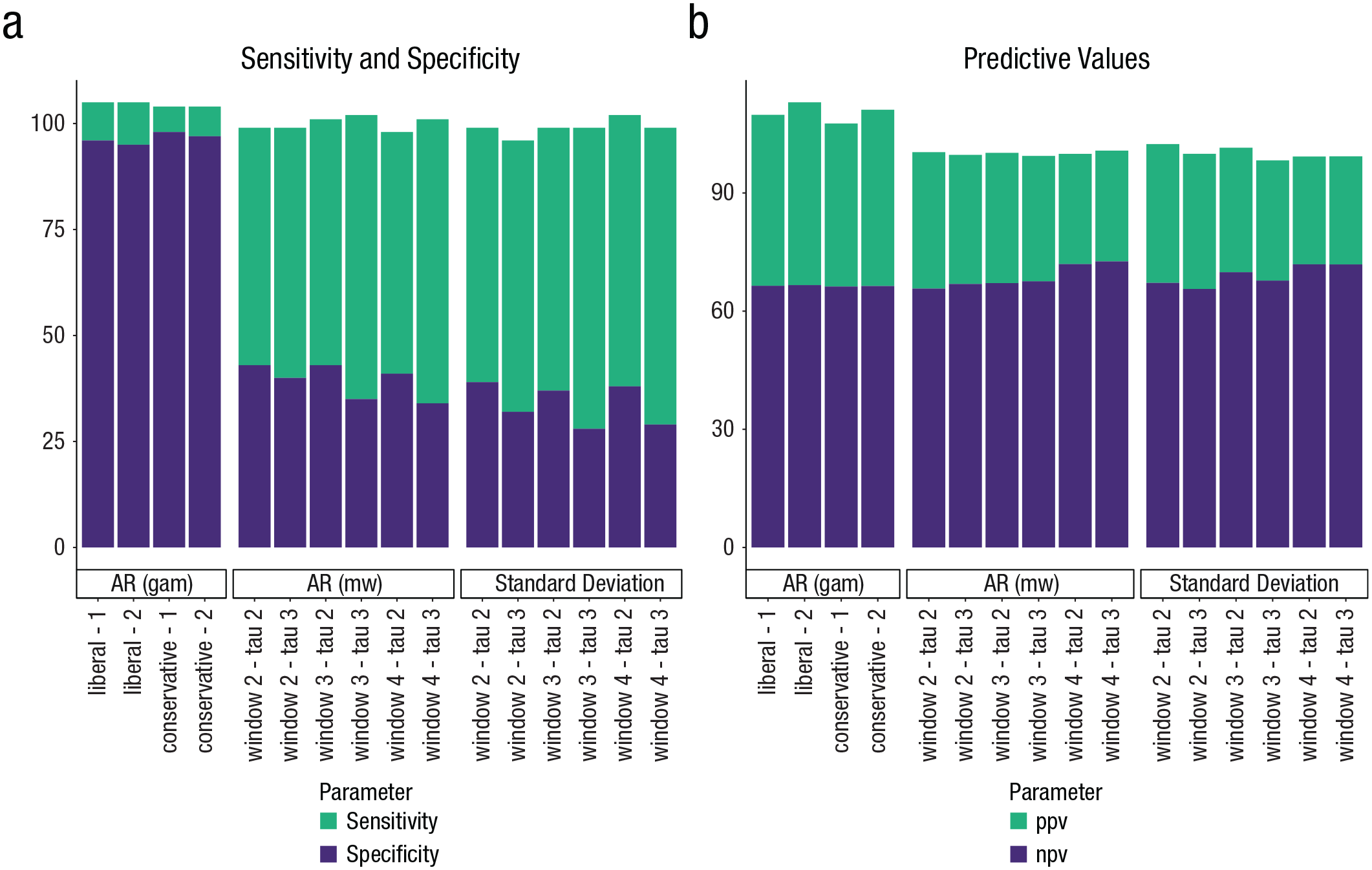
Predictive capacity of early warning signals (EWSs) across items and individuals for different methodological settings. (a) Sensitivity and specificity of EWSs, which illustrate the probability that EWSs are (not) detected given that a transition toward psychopathology does (not) unfold. (b) Positive predictive value (ppv) and negative predictive value (npv) of EWSs, which illustrate the probability that a transition toward psychopathology will (not) follow given that EWSs are (not) detected.
For the moving-window method, more proximal EWSs had a lower sensitivity—but a higher specificity—compared with more distant EWSs. To illustrate, setting the duration of EWSs to 3 weeks instead of 2 weeks led to an average increase in sensitivity from 27% to 29% (ARMW) and from 33% to 37% (SDMW) and similarly affected the specificity of EWSs (ARMW from 74% to 71%, SDMW from 66% to 61%). Increasing the sizes of windows affected the sensitivity and specificity of EWSs indexed by the ARMW versus the SDMW in opposite ways. Specifically, the sensitivity and specificity of EWSs indexed by the ARMW slightly decreased with larger window sizes (sensitivity from 29% to 26%, specificity from 74% to 72%), whereas the sensitivity of EWSs indexed by the SDMW improved as windows increased (32% vs. 36%) and had negligible impact on specificity (64% vs. 63%). For both EWSs, however, the differences in sensitivity and specificity across settings were generally small, and the presence of EWSs barely increased the probability of a future transition toward psychopathology. Having said that, in the current sample, the optimal setting for EWSs indexed by the ARMW appeared to be a window size of 2 weeks and a duration of 3 weeks, whereas the optimal setting for EWSs indicated by the SDMW was a window size of 3 weeks and a duration of 2 weeks.
Impact of items
Across individuals and settings, the valence of emotions in which EWSs were (not) detected had little impact on the predictive capacities of EWSs (Fig. 3; also see Table S4 in the Supplemental Material). As an example, the sensitivity of EWSs indexed by ARGAM was on average 9% for negative emotions and 8% for positive emotions (average specificity: 96% vs. 97%; positive predictive value: 33% vs. 34%; negative value: 84% vs. 84%). Similar negligible differences were found for EWSs indexed by ARMW and SDMW (see Table S4 and Fig. S2 in the Supplemental Material).
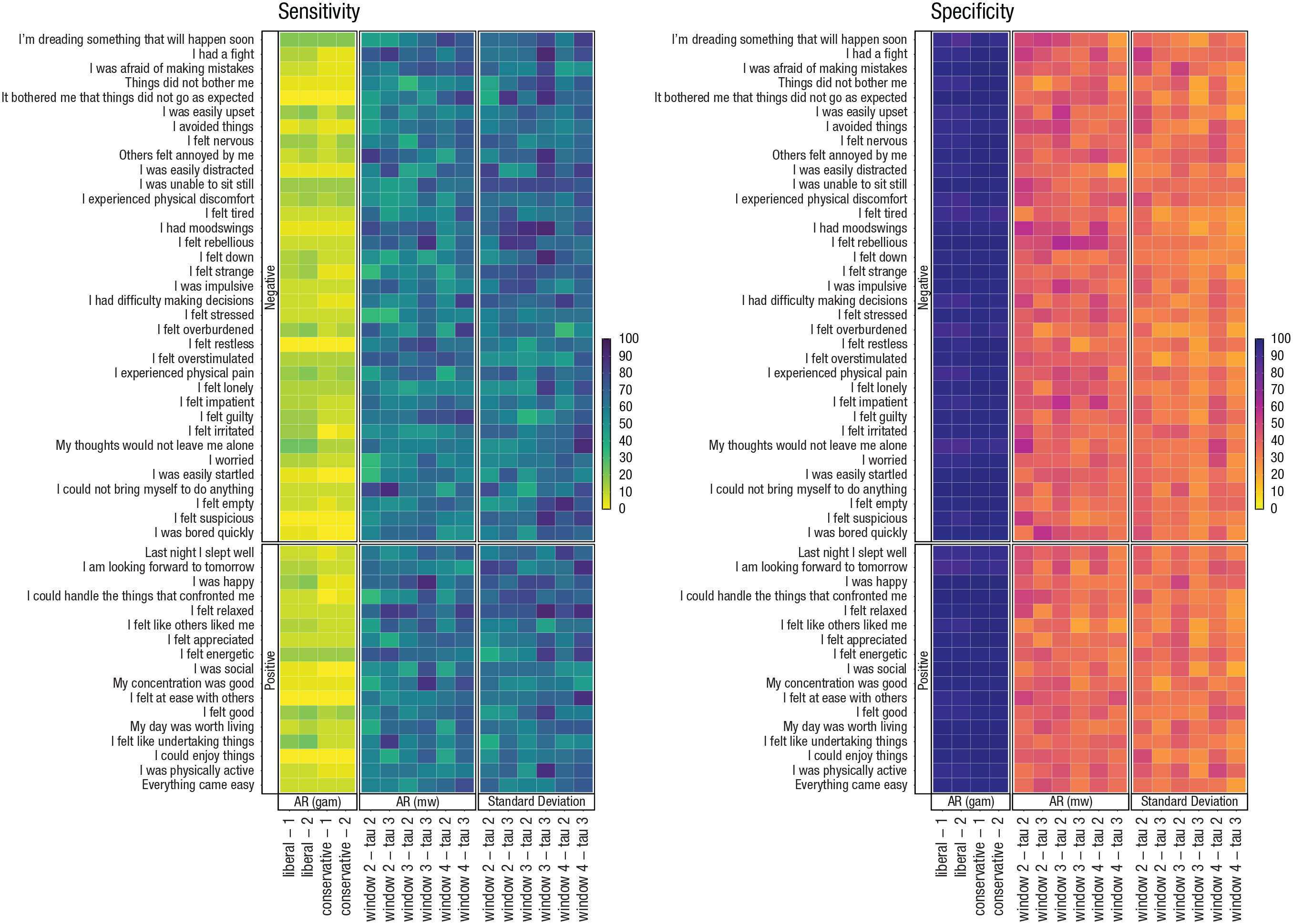
Sensitivity and specificity of early warning signals (EWSs) indexed by the autoregressive (AR) coefficient (ARGAM, ARMW) and the standard deviation (SDMW) across methodological settings and items. This plot relates only to transitions toward psychopathology. Similar figures for positive and negative predictive values and transitions toward well-being are provided in the Supplemental Material available online (Fig. S3, Fig. S4). GAM = general additive models; MW = moving-window analyses.
Agreement between EWSs
Across methodological settings, there were a total of 1,352 potential warning signals for transitions toward psychopathology (i.e., 26 transitions × 52 emotions). In only 44 (3%) of these occasions, ARGAM, ARMW, and SDMW unanimously provided a warning signal (Fig. 4). For 380 (28%) of the cases, there were two warning signals, and in 604 (45%) of the cases, there was a single warning signal. For transitions toward well-being, these numbers were roughly similar (see Fig. S5 in the Supplemental Material). In case no transition occurred, EWSs indexed by the ARGAM, ARMW, and SDMW were unanimously absent in 535 (14%) out of 3,692 cases (i.e., 71 nontransitions × 52 emotions). For nearly all other cases (85%), one or two types of EWSs were present, and in 48 instances (1%), all three indicators falsely provided a warning signal.
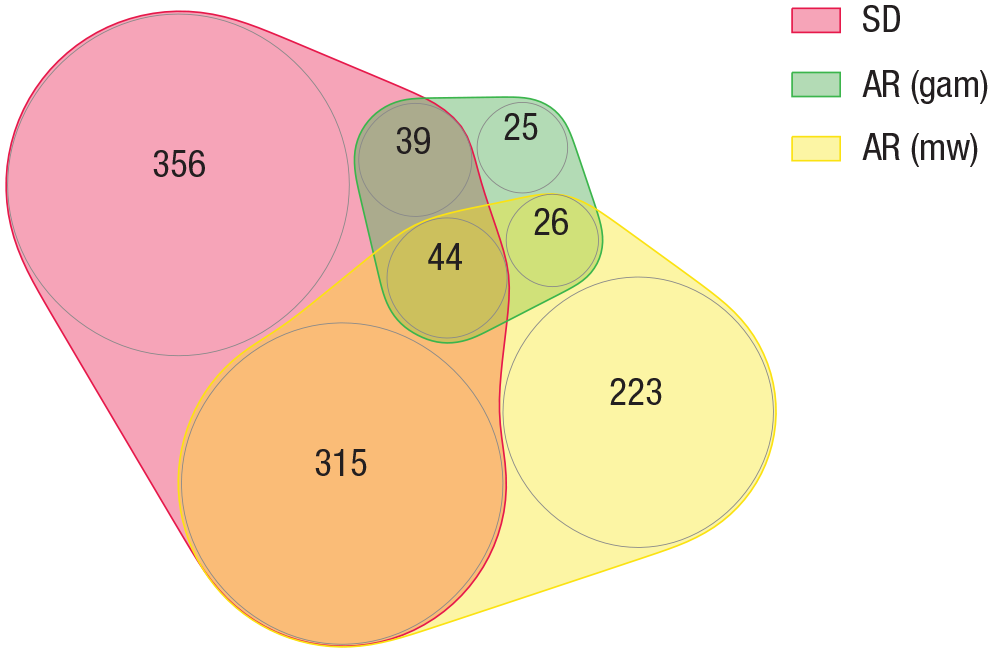
Agreement between early warning signals (EWSs) indexed by the ARGAM, ARMW, and SDMW illustrated in an Euler diagram. Numbers denote the number of instances (i.e., emotions across individuals) in which the indicators anticipated a transition toward psychopathology. A similar figure for transitions toward well-being is provided in Figure S5 in the Supplemental Material available online. AR = autoregressive coefficient; GAM = generalized additive models; MW = moving-window analyses.
Discussion
EWSs—and complex-systems principles in general—have been suggested to hold great promise for mental-health research and clinical practice. In particular, rising autocorrelations and standard deviations have been introduced as potential personalized warning signs that could enable foreseeing the sudden onset of psychiatric disorders (Wichers et al., 2016, 2020). This would mean that by monitoring and analyzing individuals’ emotions, clinicians could know whether a specific individual at a specific moment in time is at high risk for developing psychopathology. The present study concerns one of the first empirical investigations of EWSs—conceptualized as rising trends in the autoregressive coefficient and standard deviation of daily assessed emotions—as predictors of transitions toward psychopathology. Using daily diary data collected for a period of 6 months in 122 at-risk young adults, we identified 24 individuals who experienced transition toward psychopathology. We investigated whether these transitions were anticipated by EWSs in three different indices (ARGAM, ARMW, SDMW), each in 52 emotions, using various methodological settings, and found that the predictive capacities of EWSs were rather limited. Generally, EWSs indexed by the ARGAM were seldomly present but did occur more often in individuals with versus without a transition toward psychopathology. In contrast, EWSs found through moving-window analyses (ARMW and SDMW) were often found but were equally likely in individuals with versus without transitions. Different methodological settings shifted the trade-off between sensitivity and specificity, but none of these alternative settings yielded findings that could substantiate the clinical promise that EWSs were suggested to entail. Thus, it seems that anticipating transitions toward psychopathology in the current sample through EWSs remains beyond reach.
Present findings contradict two earlier single-case studies, which reported that EWSs anticipate relapses in depression (Wichers et al., 2016, 2020). The discrepancies between present and earlier findings might be attributed to differences in the severity of psychopathological symptoms—and relatedly, the magnitude of transitions—that individuals experienced. Specifically, earlier case studies included individuals diagnosed with major depression who showed a sudden increase in weekly symptom reports of depression (effect size = 2.51 6 ). In contrast, the present study concerned sudden drops in day-to-day mental health or increases in mental ill health reported by individuals with a history of mental-health problems before the age of 11 but who did not necessarily have a recent clinical diagnosis (mean effect size = 0.65). Hence, the presently studied transitions were smaller than and qualitatively different from the relapses experienced by individuals with a history of major depression. This is a critical point because support for EWSs before transitions has mostly been found in the context of large—potentially irreversible—shifts in systems, such as the extinction of a species (ecosystems) or market crashes (financial systems). Including individuals without clinically significant symptoms, for whom transitions in mental health were smaller than those previously studied, may thus have lowered our power to detect EWSs. Nonetheless, we believe that going beyond the previously studied “systems” (i.e., individuals with relapse into depression) is not a limitation but rather an essential merit of the current work. A first reason is that EWSs have been proposed to be generic and, hence, could be expected to occur regardless of the specific type of system under consideration. It was thus well possible that the utility of EWSs would extend beyond the specific systems previously studied. This extension of EWSs was important to investigate because clinical implementation of EWSs is warranted only if the utility of these signals would hold on a larger scale. A second reason is that from a clinical perspective, the implementation of EWSs is particularly promising in at-risk youths, who may have much to gain from early detection of emerging or worsening psychopathology. With this study, we have shown that this clinical implementation of EWSs is currently not supported: EWSs do not reliably anticipate transitions toward psychopathology in at-risk youths, and hence, EWSs are less generic than often proposed.
Putting EWSs into perspective
Although research into EWSs as predictors for transitions in mental health is still in its infancy, other fields yielded valuable insight in EWSs that can help to put current findings into perspective. Although numerous studies from various fields showed that transitions, for instance observed in ecological or financial systems, are preceded by EWSs (Dakos et al., 2008; Drake & Griffen, 2010; Veraart et al., 2012), other studies did not support this (Diks et al., 2018; Gsell et al., 2016; Guttal et al., 2016). This led to the conclusion that EWSs might be less generic than initially proposed (Boerlijst et al., 2013). Rather, the presence and detectability of EWSs depend on numerous requirements. For instance, EWSs are not expected when (a) instability accumulates too quickly to be captured by EWSs, (b) the transition is caused by a strong external trigger instead of gradually accumulated instability in the system (Boettiger & Hastings, 2012b; Dakos et al., 2015), (c) the instability of the system manifests in other variables than the variables for which EWSs are examined (Boerlijst et al., 2013), (d) the measurement frequency does not match the timescale at which the dynamics of interest operate (Haslbeck & Ryan, 2021; Wen et al., 2018), (e) the alternative state following from the transition is only temporary and does not fulfill the (mathematical) requirements of an equilibrium (Boettiger et al., 2013; Dakos et al., 2015), or (f) the system is exposed to nonstochastic fluctuations (Dutta et al., 2018; Guttal et al., 2016; Scheffer et al., 2012). All of these conditions could play a role in the detection of EWSs before transitions in mental health. These transitions are still poorly understood, and therefore, the extent to which mental health meets the aforementioned requirements remains speculative. We discuss this in-depth below and refer back to the aforementioned requirements. First, transitions in mental health may follow from rapidly accumulating vulnerability—which cannot be captured by EWSs (Requirement a)—or from major external events (e.g., traumatic events; Requirement b) rather than from gradually accumulating instability. It is still unknown what defines a gradual buildup of instability in psychiatry: Whereas earlier studies assumed that such a buildup occurs over several months (Wichers et al., 2016, 2020), in the current study, we assumed a faster time frame (i.e., 1–3 weeks), reasoning that the hypothesized clinical implementation of EWSs would benefit from relatively quick signals. Provided that there is a gradual buildup of instability and that what gradual means in this context is known, not all emotions might be equally affected. That is, EWSs might manifest only in certain emotions (Requirement c), and which emotions are most relevant may vary across individuals. In the present study, we addressed this by examining EWSs in a broad variety of emotions. Yet little is known about the variables wherein vulnerability to mental ill health actually manifests, and it could therefore be that other types of variables (e.g., physiological) are more suitable for detecting EWSs. The detection of EWSs—particularly those indexed by the autoregressive coefficient—further depends on the frequency of assessments: If the time interval between observations is too long, the correlation between adjacent observations (autocorrelation) is no longer informative of critical slowing down (Requirement d). This might explain why the current study—which adopted daily assessments and, hence, assumed relatively slow dynamics—found fewer EWSs compared with former case studies (Wichers et al., 2016, 2020)—which adopted three to 10 assessments per day, hence assuming faster dynamics. In line with this reasoning, it has been suggested that momentary assessments (e.g., How are you feeling right now?) are more suitable for detecting EWSs compared with the retrospective assessments used in the current study (e.g., How did you feel during the past day?; Dablander et al., 2020). At the same time, however, EWSs have been found in daily measures (Curtiss et al., 2019). Furthermore, studies that analyzed autocorrelations on very different timescales, ranging from second-to-second (Kuppens et al., 2012), minute-to-minute (Koval et al., 2013), hourly (Koval et al., 2012), to daily intervals (Brose et al., 2015), all yielded very similar conclusions. Thus, assessment frequency indisputably affects autocorrelation estimates, but its consequences for our inferences and conclusions require further research. Until the uncertainty concerning the optimal measurement frequency for detecting critical slowing down is solved, it might be best to focus on warning signals that are less reliant on timescales (e.g., standard deviations) and to keep in mind the eventual implementation of EWSs in clinical practice. Regarding the latter, it may be unfeasible to ask at-risk individuals to monitor their emotions every hour for a considerable period of time (e.g., 6 months). Hence, it is valuable to investigate EWSs on a timescale that could eventually be used for real-time monitoring—supporting the daily assessments adopted in the present study. Two final prerequisites for detecting EWSs relate to the states between which transitions may occur. In some systems, these states represent temporally stable equilibria with clear boundaries (e.g., greenhouse- vs. icehouse-climate states). In mental health, however, alternative states may be less clear-cut. Rather, the progression from mental health to ill health may involve temporary “in-between” stages (McGorry et al., 2006). Humans may shift back and forth between such stages, and hence, transitions in mental health might involve transient states instead of distinct stable equilibria (Requirement e; Schreuder et al., 2021). Even if mental (ill) health can be described as an equilibrium, the events to which people are exposed—which lead to temporary departures from equilibrium (i.e., dips and uplifts in their mood)—may not occur stochastically (Requirement f). That is, humans can exert some control over the events they experience, and therefore, these events do not happen completely at random. As individuals become more vulnerable to symptoms of anxiety, for example, they may increasingly avoid certain triggers. This complicates the detection of critical slowing down (and hence, EWSs): One cannot assess slowed recovery from perturbations if there are few(er) perturbations to recover from. In summary, little is known about the extent to which mental health meets the requirements for anticipating sudden transitions through EWSs. This knowledge gap is to be addressed in the future.
One of the most compelling properties of EWSs is that they may anticipate system behavior—such as sudden transitions—even though little is known about the mechanisms that underlie system behavior (e.g., biological, social, psychological). This is highly attractive in the context of mental health, in which changes in individuals—such as the onset or progression of symptoms—are still poorly understood from a mechanistic point of view (e.g., in terms of the biological, social, and psychological causes). Yet, although EWSs do not necessitate such traditional mechanistic understanding, they do require an alternative level of understanding mental health. That is, from the list of requirements outlined above, it follows that EWSs require insight in the dynamics that govern psychopathology. This entails delineation of the type of transitions that take place, the characteristics of the states between which such transitions may occur, and the timescale at which dynamics such as EWSs unfold. This could ultimately help with figuring out which, if any, types of changes in mental health may be formally recognized as transitions that are preceded by critical slowing down.
Taken together, this study found little support for the notion that rising autocorrelations or standard deviations in emotions could be used as reliable, personalized risk markers for impeding transitions toward psychopathology. Yet it is too early to reject this idea, and follow-up studies with different populations, types of transitions, and warning signals (e.g., multivariate warning signals; Scheffer et al., 2015) are needed. Multivariate extensions of EWSs could, for instance, indicate the type of symptoms for which a specific individual is most vulnerable (or least resilient; Boerlijst et al., 2013; Weinans et al., 2019; Wichers et al., 2019). Such insight might then inform preventive intervention efforts. In sum, the hypotheses and clinical promises that follow from a complex-systems approach to mental health range far beyond what could be addressed in the present study, although the current findings indicate new angles for future research.
Strengths, limitations, and future directions
The unique data analyzed in the present study—which covered, on average, 161 daily diary assessments in 122 at-risk young adults—offered the possibility to provide one of the first large-scale intraindividual studies into EWSs (i.e., rising autocorrelations and standard deviations in daily assessed emotions) as predictors of transitions toward psychopathology. By analyzing EWSs not only in individuals with transitions in mental (ill) health but also in individuals without such transitions, we could examine both the sensitivity and specificity of EWSs. The latter is seldomly reported in empirical literature yet is highly relevant from a clinical point of view (for a more elaborate discussion on this topic, see Boettiger & Hastings, 2012a).
An important consideration in evaluating the merits and generalizability of the current research concerns our operationalization of transitions in mental (ill) health. These transitions were smaller than previously studied transitions toward psychopathology (Wichers et al., 2016, 2020). This limitation touches on a broader issue—that fairly little is known about the transitions that individuals experienced (e.g., in terms of the clinical meaning of these transitions, the driving causes of transitions, the timescale at which they unfolded, their supposed nonlinearity). Yet such characteristics are crucial for the presence of EWSs (Boerlijst et al., 2013). A more elaborate exploration of transitions in mental health—for instance, observed as a sudden onset or relapse of psychopathology—therefore concerns an important avenue for further research. As an example, recent work showed that the majority of remission trajectories occur in a stepwise fashion, as opposed to (log)linearly (Helmich et al., 2020). In addition, further studies are needed to define the periods before and after transitions in mental health. When and for whom do such periods resemble stable equilibria as opposed to transient, intermittent states? Finally, future studies could look beyond the traditional application of EWSs (i.e., as timely warning signs) and examine whether EWSs can inform on the type of symptoms for which individuals may be most vulnerable (Weinans et al., 2019).
Conclusion
In young adults at risk for psychopathology, rising autocorrelations and standard deviations in daily assessed emotions—which have been considered personalized warning signs—hardly predict transitions toward psychopathology. Unlike earlier studies, which tested EWSs on group level (van de Leemput et al., 2014), this study investigated EWSs within individuals. In contrast to two case studies (Wichers et al., 2016, 2020) that reported promising clinical utility of EWSs, we found little support for using EWSs to address clinical goals. This highlights the need to investigate under what circumstances complex-systems principles are useful for understanding the progression of mental-health problems (e.g., type of complaints, characteristics of the transition). In conclusion, EWSs do not provide a simple solution to predicting who will experience a transition toward psychopathology at what moment in time. Although complex systems offer a novel perspective on vulnerability and resilience to mental disorders, the usefulness of this perspective to clinical practice still awaits empirical support.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026221103138 – Supplemental material for Anticipating Transitions in Mental Health in At-Risk Youths: A 6-Month Daily Diary Study Into Early-Warning Signals
Supplemental material, sj-docx-1-cpx-10.1177_21677026221103138 for Anticipating Transitions in Mental Health in At-Risk Youths: A 6-Month Daily Diary Study Into Early-Warning Signals by Marieke J. Schreuder, Catharina A. Hartman, Robin N. Groen, Arnout C. Smit, Marieke Wichers and Johanna T. W. Wigman in Clinical Psychological Science
Footnotes
Acknowledgements
We are grateful to Laura Bringmann and Casper Albers, who shared their expertise in generalized additive models and helped us with applying these models. Furthermore, we thank everyone who participated in this research or worked on this project in any way.
Transparency
Action Editor: Aidan G. C. Wright
Editor: Jennifer L. Tackett
Author Contributions
M. Wichers developed the study concept. Data were collected by M. J. Schreuder and R. N. Groen. M. J. Schreuder performed analyses. A. C. Smit helped with detecting transitions in mental (ill) health. M. J. Schreuder, C. A. Hartman, and J. T. W. Wigman interpreted the results. and M. J. Schreuder drafted the manuscript. All of the authors revised the manuscript. M. Wichers and J. T. W. Wigman shared final authorship. All of the authors approved the final manuscript for submission.
Correction (March 2023):
Article updated to include the Preregistration badge and the Open Practices statement.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.