
Abstract
Background
Online self-assessments are becoming more popular. They can serve as a screening tool for specific conditions or assess mental health more broadly but often lack in depth evaluation.
Methods
This study presents preliminary data from an online self-assessment tool for young people within the age range of 12–30 years (Link: redcap.hmri.org.au/surveys/?s = MK7RCELJ79). It covers key symptoms of mood and psychotic disorders and risk factors, such as eating issues, substance use, suicidality, and deliberate self-harming behaviours. Participants self-assessed their level of functioning, access to ongoing interventions, and satisfaction with the help received. Based on the severity of mental health problems and the level of risk, different recommendations of how to seek help were provided.
Results
Out of 303, 114 participants gave permission to analyse their data. A high-risk profile was defined by anxiety symptoms, panic attacks, suicidal ideation, and urges to self-harm. These individuals were more likely to report psychotic or depression symptoms, recreational substance use and low day-to-day functioning. Ongoing treatment and the satisfaction with it were not determined by the severity of symptoms.
Conclusions
These preliminary results suggest that the online self-assessment tool reaches the intended young audience, particularly those with some degree of mental health problems.
Plain language summary
Online self-assessments are becoming more popular particularly with young people. They can serve as a screening tool to assess mental health. We developed a new online self-assessment tool for young people 12 to 30 years of age (Link: redcap.hmri.org.au/surveys/?s=MK7RCELJ79). It covers key symptoms of mood and psychotic disorders and risk factors, such as eating issues, substance use, suicidality, and deliberate self-harming behaviours. The tool also asks for a self-assessment of their level of functioning, their access to professional help, and their satisfaction with the help received. The assessment concludes with recommendations how to seek help dependent on the severity of their mental health problems and level of risk. We had 303 young people visiting the tool and 114 gave permission to analyse their data. Young people with anxiety symptoms, panic attacks, suicidal ideation, and urges to self-harm were considered at high risk. They more likely to report psychotic or depression symptoms and recreational substance use and low day-to-day functioning. Ongoing treatment and the satisfaction with it were not determined by the severity of mental health problems. These preliminary results suggest that the online self-assessment tool reaches the intended young audience, particularly those with mental health problems.
Keywords
Introduction
Mental illness and substance use disorders account for the largest burden of illness among young people, based on Disability-adjusted Life Years estimates (Whiteford et al., 2015). The Australian Burden of Disease Study identified the age cohort between 12 and 25 years as the most affected by mental illness compared to all other medical conditions in the same age group (Australian Institute of Health and Welfare, 2022). In addition, 75% of all mental illnesses manifest before the age of 25 (McGorry & Mei, 2018). Attention and behavioural disorders can be diagnosed as early as 3 years of age, followed by anxiety disorders between the ages of 7 and 14, and emerging bipolar affective and psychotic conditions in adolescents and young adults (Kessler et al., 2007).
Young people with mental health problems are the least supported in the Australian health system, despite the fact that this cohort offers the best opportunity for early intervention before the conditions worsen if untreated (McGorry, 2007). Nonetheless, initiatives such as Headspace (Headspace, 2006) have established youth-friendly services outside state-run mental health service providers in Australia. However, the effective use of assessment services is still impeded by social stigma and limited mental health literacy (Easton et al., 2013).
Young people are increasingly relying on internet-based information (Odgers & Jensen, 2020). There are numerous mental health resources available online, such as Headspace, the Black Dog Institute (Parker, 2002), and Beyond Blue (Kennett, 2000) in Australia, as well as Mental Health America (Mental Health America, 1909) overseas, which offer a suite of online mental health self-assessments. For instance, Beyond Blue offers an Anxiety and Depression Test K10 (Beyond Blue, 2000), which is based on Kessler’s Psychological Distress Scale (K19; Andrews & Slade, 2001). After completing the test, participants receive feedback and possible contact points.
Another Australian online initiative is the government-funded Head to Health website, which initially launched as Mental Health Gateway in 2017 and became a fully functional website in 2022 (Head to Health, 2022). This platform not only provides information on mental health providers, but also offers online self-assessment tools. This self-assessment covers a wide range of psychological stress factors. Upon completion, participants receive a personalised PDF document with a summary of their mental health concerns, together with professional follow-up information.
Although these platforms provide cost-effective guidance for consumers, they have some limitations. Notably, they cannot be used as a substitute in situations that demand mental health professional intervention or vital support during crisis circumstances. In addition, these resources can occasionally be misleading due to the risk of inappropriate “self-diagnosing”.
Despite the availability of feasible online tools for mental health self-assessment, there is a need of studies to assess their utility on the young population. Balcombe and De Leo (2023) conducted a systematic review and a meta-analysis of digital mental health platforms and interventions. The final dataset consisted of 22 studies employing quantitative, qualitative, or both methods published between 2012 and 2022. The authors found evidence supporting the feasibility of online tools, but criticised the limited data, the heterogeneity in study designs, and the lack of focus on specific populations, such as young people.
In addition, most of studies focused on the self-evaluation of depression symptoms among the young population do not cover a diverse range of interventions and self-evaluation measures (Orchard et al., 2021). In addition, the influence of individual social environments and the cognitive ability for accurate self-assessment was a common limitation in those studies, thus highlighting the need to shed more light on the topic.
The psychological self-assessment and management tool MyHEARTSMAP (Virk et al., 2019) has been shown to successfully connect youth with appropriate mental healthcare. Virk et al. (2019) revealed good to excellent inter-rater reliability across all psychosocial sections of the assessment tool within diverse community samples.
Despite the prevalence of mental health issues in the young population, only approximately half of the youth in primary care are screened for mental health and risk behaviour issues (Martel et al., 2021). This systematic review showed that although electronic screening proved to be both feasible and acceptable for consumers and providers, raising sensitive issues with the provider continued to cause some discomfort. Overall, the authors concluded that the benefits outweigh drawbacks, including the resistance to implementing such screening by some clinicians. Therefore, there is a need of to improve self-assessment tools and study their feasibility and applicability.
The tool introduced in this study shares a similar goal of connecting young people with mental health concerns with professionals via their primary healthcare provider. Given the familiarity of young people with online tools, we consider our online approach to be youth-friendly. Additionally, the online self-assessment can be conducted privately and can provide valuable insights into the pathology of the reported symptoms, which may ultimately serve as a motivational catalyst for seeking professional help.
The purpose of the current study was to evaluate the usefulness and acceptance of a new online self-assessment tool as well as investigating the characteristics of this population of young people aged from 12 to 30 years, such as demographics, global function levels, psychopathology, illicit substance use, level of risk, access to mental health care, and their satisfaction with it.
Methods
Study design
The current study explores existing on-line data from a self-selected young population volunteering their data for research. Comparison groups were defined post hoc by predetermined criteria splitting the sample according their levels of risk.
Subjects
Data from 303 participants was collected from April 2021 to November 2022.
The study was approved by The University of Newcastle Human Research Ethics Committee (Reference: H-2016-0098; Chief Investigator: Professor (Emeritus) Ulrich Schall, Hunter Medical Research Institute, Healthy Minds Program). Participation in the study was voluntary, and no incentives were provided to participants. The Hunter Medical Research Institute and The University of Newcastle promoted the online-self-assessment tool through their official websites, as well as via social media platforms such as Facebook and Twitter (now X). Link: redcap.hmri.org.au/surveys/?s = MK7RCELJ79
Measures
The online self-assessment tool was developed from the Comprehensive Assessment of At-risk Mental State (CAARMS; Yung et al., 2005), which is a structured interview originally designed to identify young people at high-risk of developing severe mental illnesses, such as schizophrenia, as a starting point for the development of the online tool. The CAARMS evaluates the individuals’ functioning levels, psychopathological symptoms associated with emerging psychotic conditions, cognitive and behavioural changes, substance use, and emotional disturbances. When the CAARMS interview is conducted by trained health professionals, it can last for approximately 1 hour (Yung et al., 2005), which is not practical for an online self-assessment. Hence, in order to optimise CAARMS for its online use, CAARMS served as a starting point for item selection by mental health experts including psychiatrists and clinical psychologists, followed by the involvement of young people to keep the language simple and clear (Moss, 2016). Although youth-friendlessness per se was not formally tested, consumer feedback suggested its youth-friendly design. The REDCap software was used to program the tool (Harvey, 2018). The self-assessment can be completed in approximately 15 minutes.
Structure of the self-assessment tool
An initial privacy statement informed participants that no identifiable data would be collected. However, participants were given the choice to voluntarily disclose further personal information with informed written consent (i.e., recorded online with their data set). Otherwise, all data were deleted, with only the number of users and self-assessment completions recorded. The disclaimer was presented following the privacy statement (Figure 1). Disclaimer for the online self-assessment.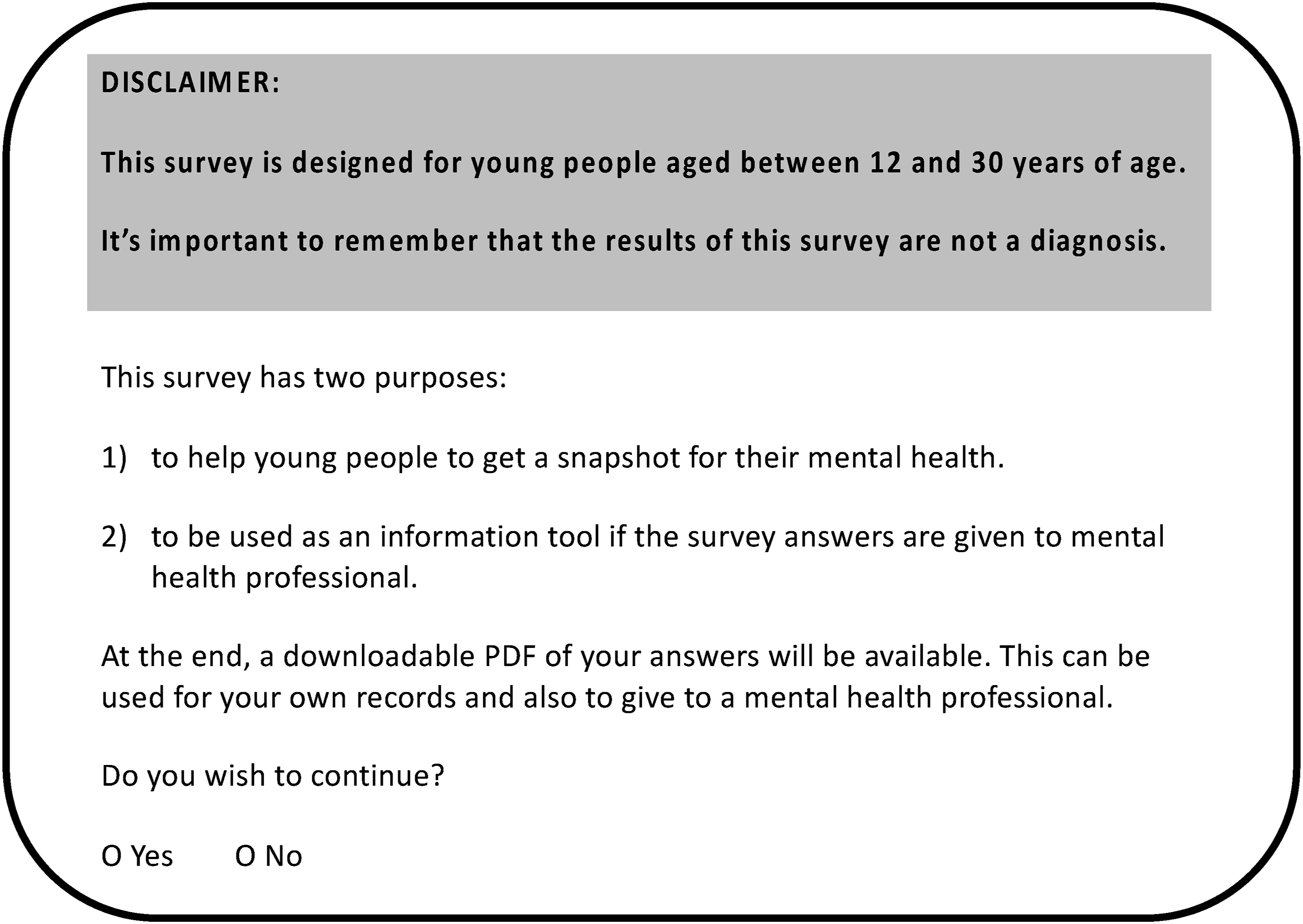
Participants were provided with a unique identification number, which was assigned to their individual copy of the questionnaire for their records. Upon agreeing to proceed, participants were asked to estimate their level of global functioning on a sliding scale from zero to 100, where a score of 100 indicated the lowest level of global functioning (2).
Participants who reported lower functioning levels had the opportunity to elaborate on their difficulties, including specifying the duration of these challenges in the preceding year. A duration exceeding one month per year was defined as an indication of a serious problem.
Unusual Thought Content and Form and Perceptual Phenomena.
Other Potential Mental Health Problems.
High-Risk Determination Items.
Recreational Substance-Use Items.
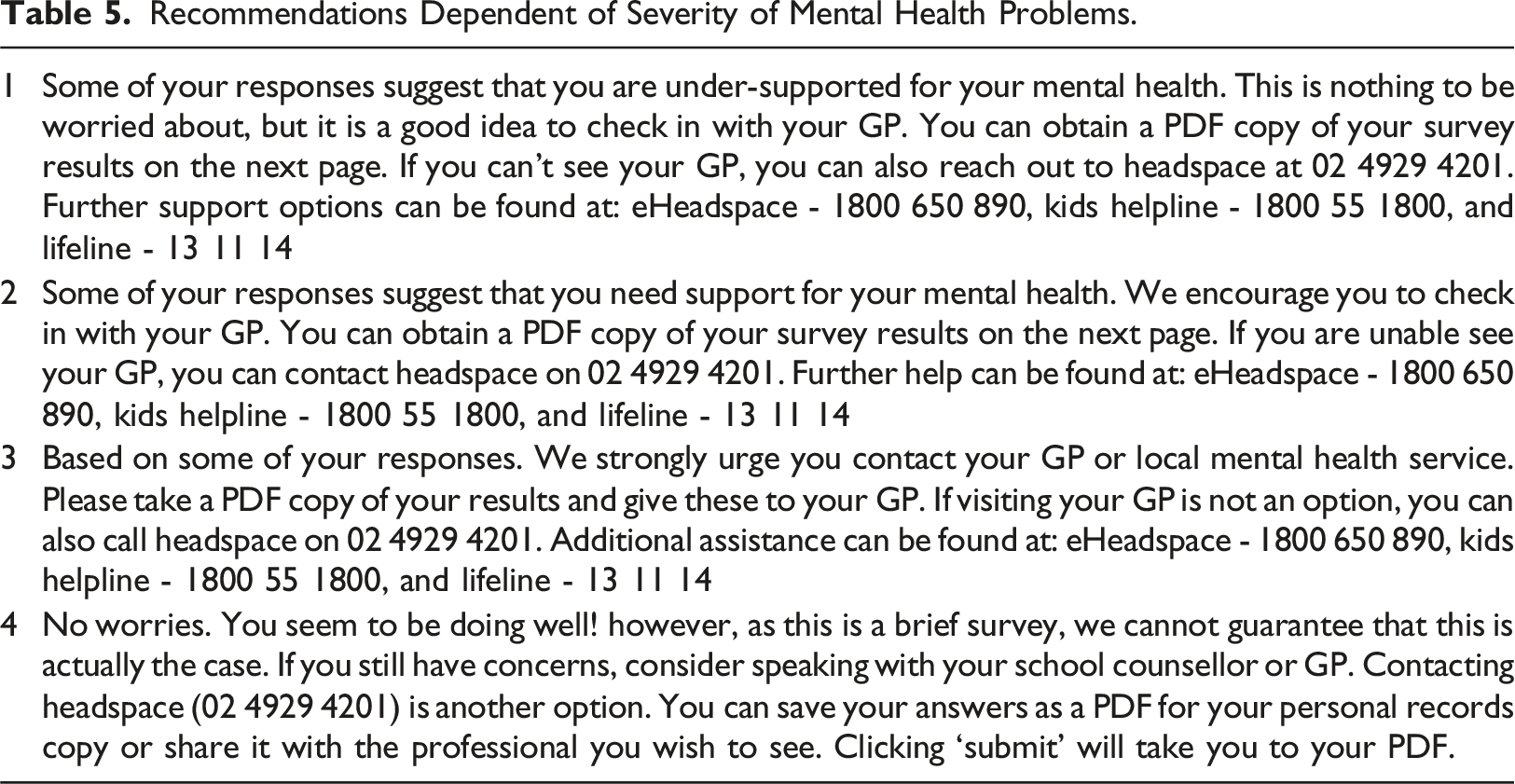
Recommendations Dependent of Severity of Mental Health Problems.
Category scores and group assignments
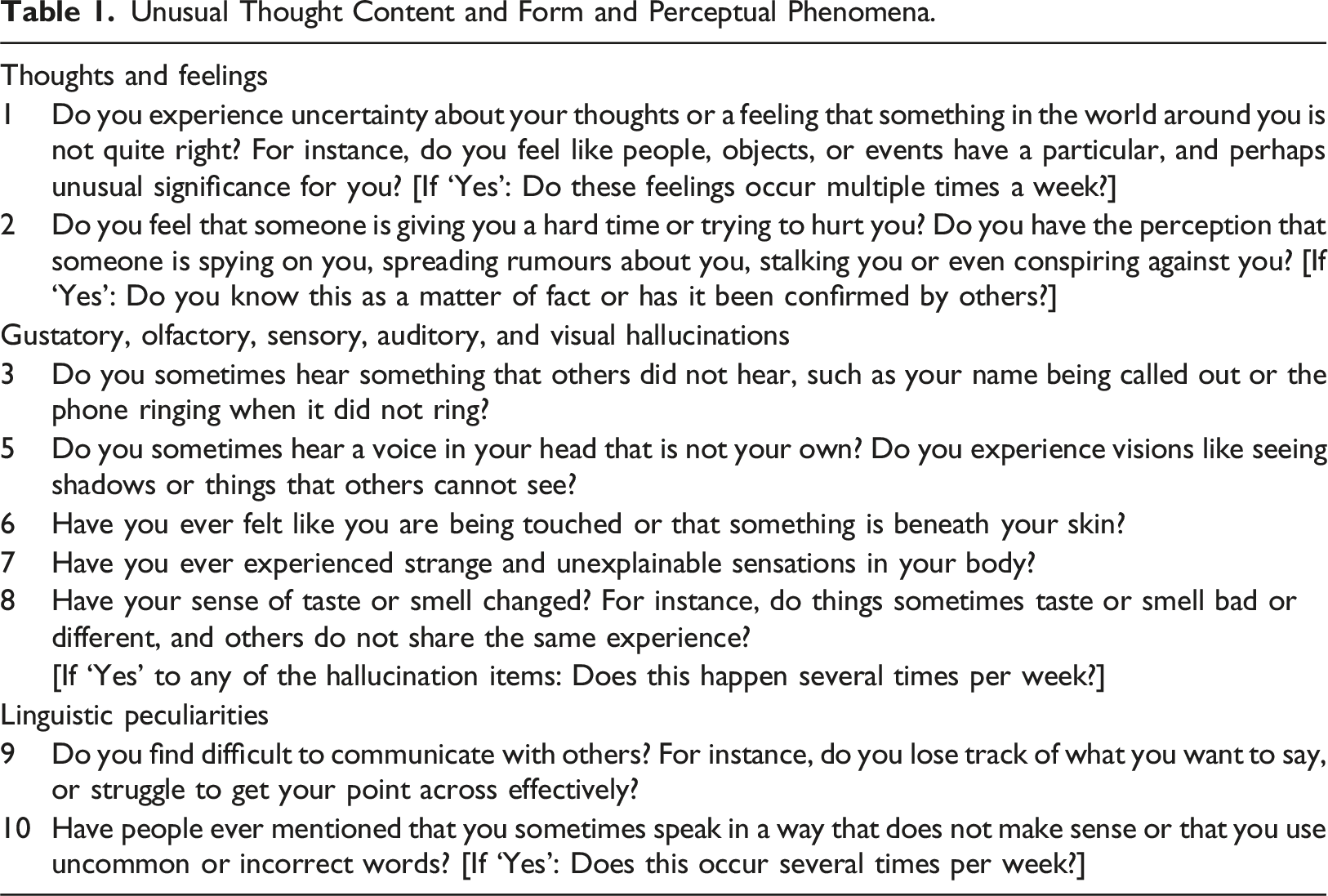
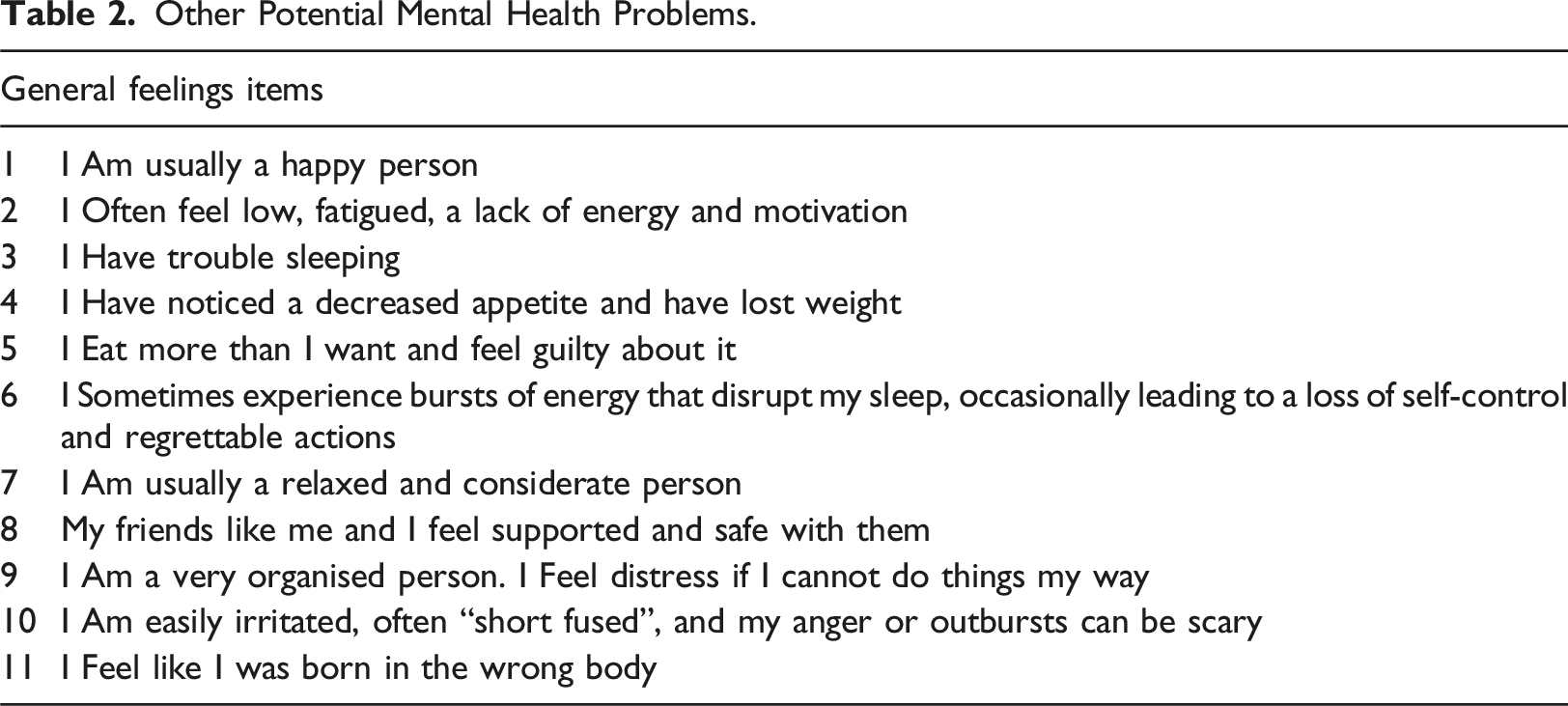
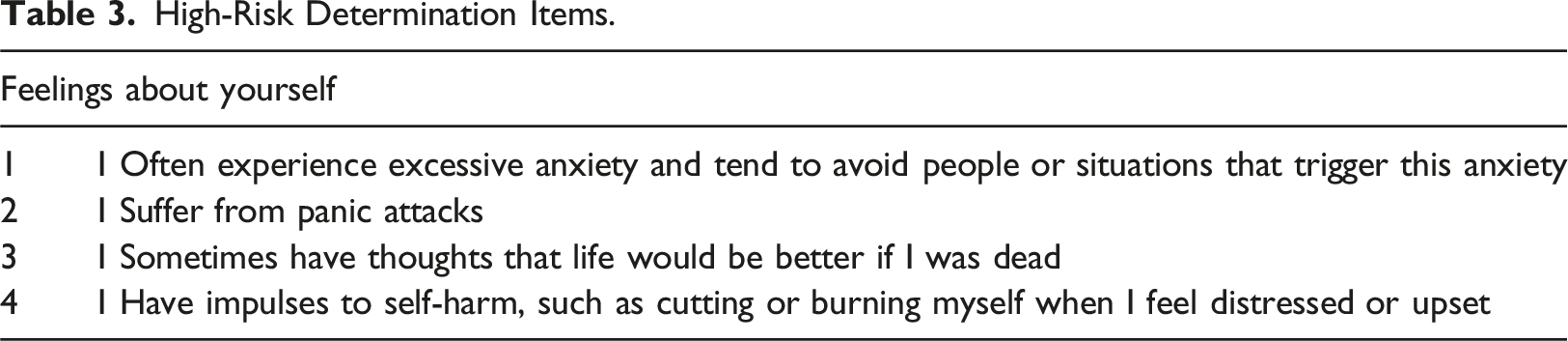
In order to categorise participants, variable categories were generated and sum scores assigned based on the number of affirmative responses in each category: psychosis (Table 1), general psychopathology and depression, respectively (Table 2), high risk (Table 3), and substance use (Table 4).
The Depression category (Table 2) comprised the following six items: “I am usually a happy person; I often feel low, fatigued, a lack of energy and motivation; I have trouble sleeping; I have noticed a decreased appetite and have lost weight; I am usually a relaxed and considerate person; I am easily irritated, often “short fused”, and my anger or outbursts can be scary.”
The high-risk group was defined by agreeing to more than one high-risk item (Table 3). Participants agreeing to only one or none of the high-risk items were classified as the “low-risk group”.
We hypothesised that the low versus high-risk groups differ in gender identity, self-harming behaviours, severity of depression, and their risk of psychosis. We further hypothesised that receiving care and being satisfied with it as well as the self-assessed function level is determined by substance use and severity of psychopathology.
Statistical analyses
Demographics and statistical analyses were performed with SPSS software (IBM © SPSS Statistics, Version 29). A significance level (α) was set at p < .05 (two-tailed). Item frequencies were assessed with 𝜒2Tests, while group comparisons were performed non-parametrically based on category sum scores using the Mann-Whitney U Test due to analysing ordinal data.
Spearman Correlation Coefficients and the Kruskal–Wallis Test was employed to test the association of the number of high-risk items (0–4; Table 3) with the sum scores for psychosis (Table 1), substance use (Table 4), and depression items (Table 2) as well as self-rated daily functioning (Figure 2). Level of self-assessed global functioning.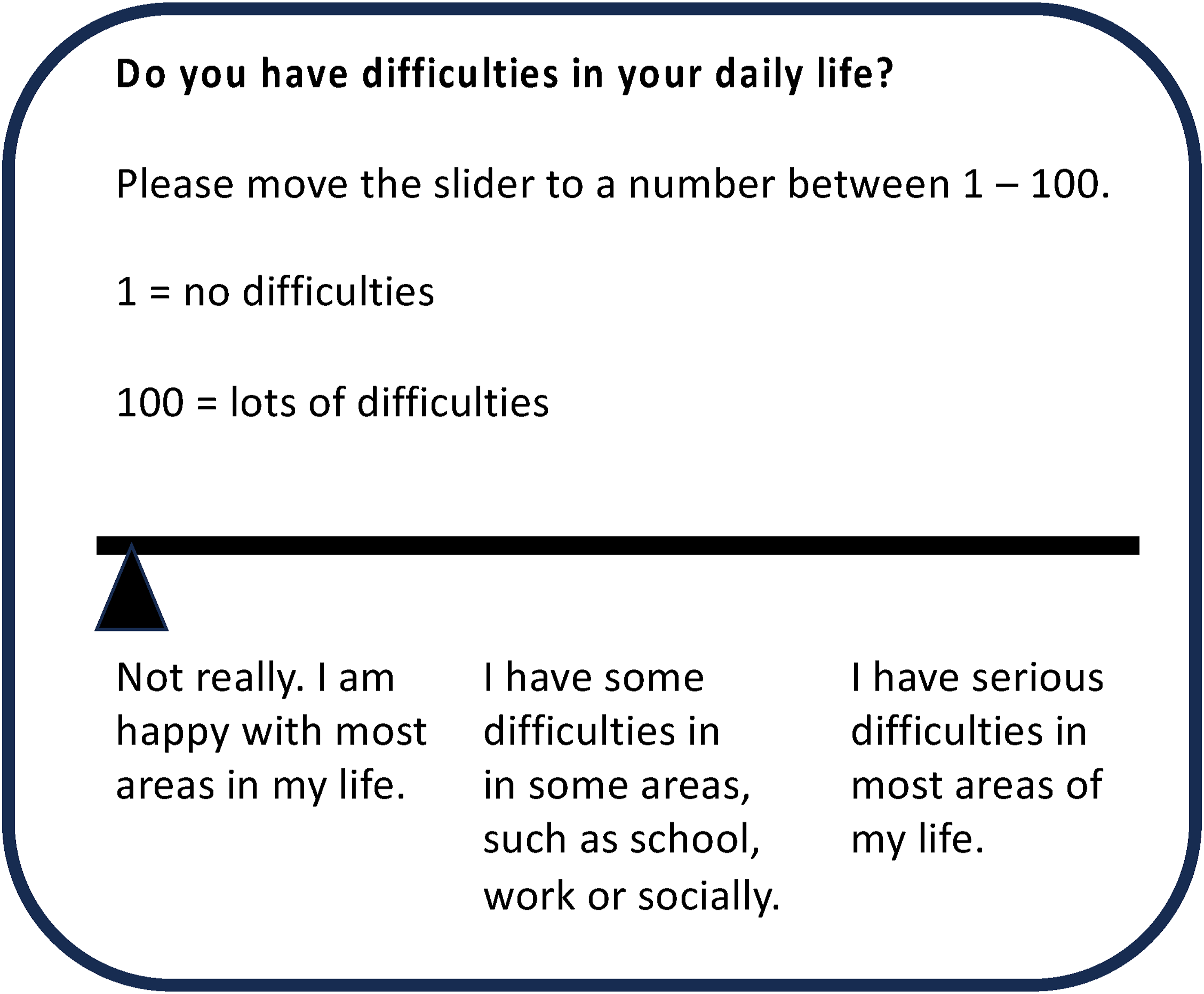
Regression analyses were employed to explore relationships of psychopathology and substance use with self-rated global function levels, engagement with health professionals and finding it helpful. Gender and age were included as moderator variables. The assumptions for linear regression (i.e., normality, linearity, homoscedasticity, and multicollinearity) were tested in SPSS. Boxplots were used to examine data for potential outliers. Statistical power was calculated post hoc as Partial Eta Square (η 2 ) for Mann-Whitney U and Kruskal-Wallis Tests. For 𝜒2Tests, Cramer’s V and phi (ϕ) was used.
Results
Sample selection and demographics
Out of the total 303 participants, 125 data sets were incomplete and 6 participants were over 30 years old. In addition, one data set was a test run by the programmer and 57 participants declined the use of their data for research. Therefore, the current study includes 114 data sets, consisting of 75 females, 30 males, and 9 individuals identifying as gender diverse (M = 18.6 years, SD = 4.0. However, 20 individuals did not reveal their age. Four individuals (3.5%) identified as indigenous, which corresponds to the proportion of indigenous people in the Australian population (Stoneham et al., 2014). Most participants resided in New South Wales, one in Western Australia, and 18 participants did not provide their postcode (Figure 3). Sample selection and demographics of final data set. See results section for further details.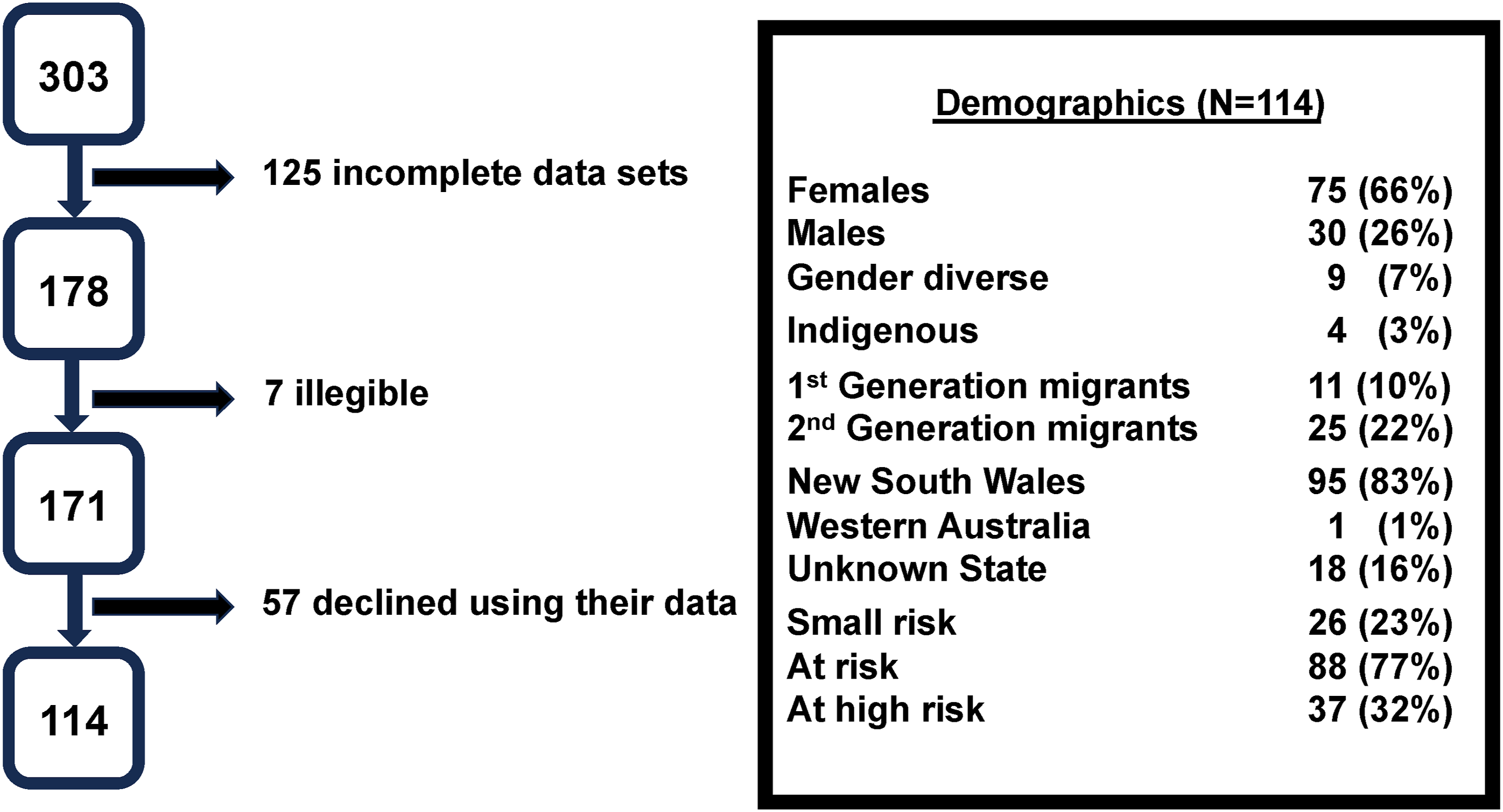
High risk sample characteristics
Among the participants, only 26 (23%) did not agree to any of the four high-risk items, whilst 101 (89%) admitted to at least one of the high-risk items (Table 3), and thus were recommended to seek professional help (Option 3 in Table 5).
Of the participants, 88 (77%) agreed to two or three of the high-risk items and 37 (32%) agreed to all four high-risk items. Of those, 36% were female, 20% male and 44% identified as gender diverse. In addition, 11 participants were first-generation migrants and 25 were second-generation migrants. There was no significant association of high-risk with migration status (𝜒 2 = 1.48, df = 2, p > .05). Finally, 44 participants (38%) reported undergoing mental health treatment (41% female, 27% male, and 56% gender diverse participants), with 30 of them (70%) expressing satisfaction with their treatment (60% female, 18% male, and 22% gender diverse participants).
There were no significant differences in gender identification (𝜒 2 = 0.01, df = 2, p > .05). However, the item “I feel like I was born in the wrong body” was associated with gender (9 females, 7 males and 5 gender diverse participants; 𝜒 2 = 10.8, df = 2, p < .01; Cramer’s V = .31).
Approximately half of the participants (51%) agreed with the statement “I eat more than I want and feel guilty about it”, with variations across gender (45 female, 6 male, and 7 gender diverse participants; 𝜒 2 = 16.55, df = 2, p < .001; Cramer’s V = .38).
Higher sums scores of psychosis, substance use, and depression items were associated with higher levels of risk, respectively (H = 12.67–44.17, df = 4, p = .013 - p < .001; η 2 = .36 -. 39). Higher levels of risk were also associated with lower self-rated function levels (H = 30.85, df = 4, p < .001; η 2 = .27). Migration status was not significantly associated with high risk (H = 1.67, df = 4, p > .05).
The substance use score was significantly higher in the high-risk group versus the low-risk group (U = 1324.50, p < .05; η
2
= 20; Figure 4(a)). Self-assessed global function levels were lower in the high-risk group (U = 737.00, p < .001; η
2
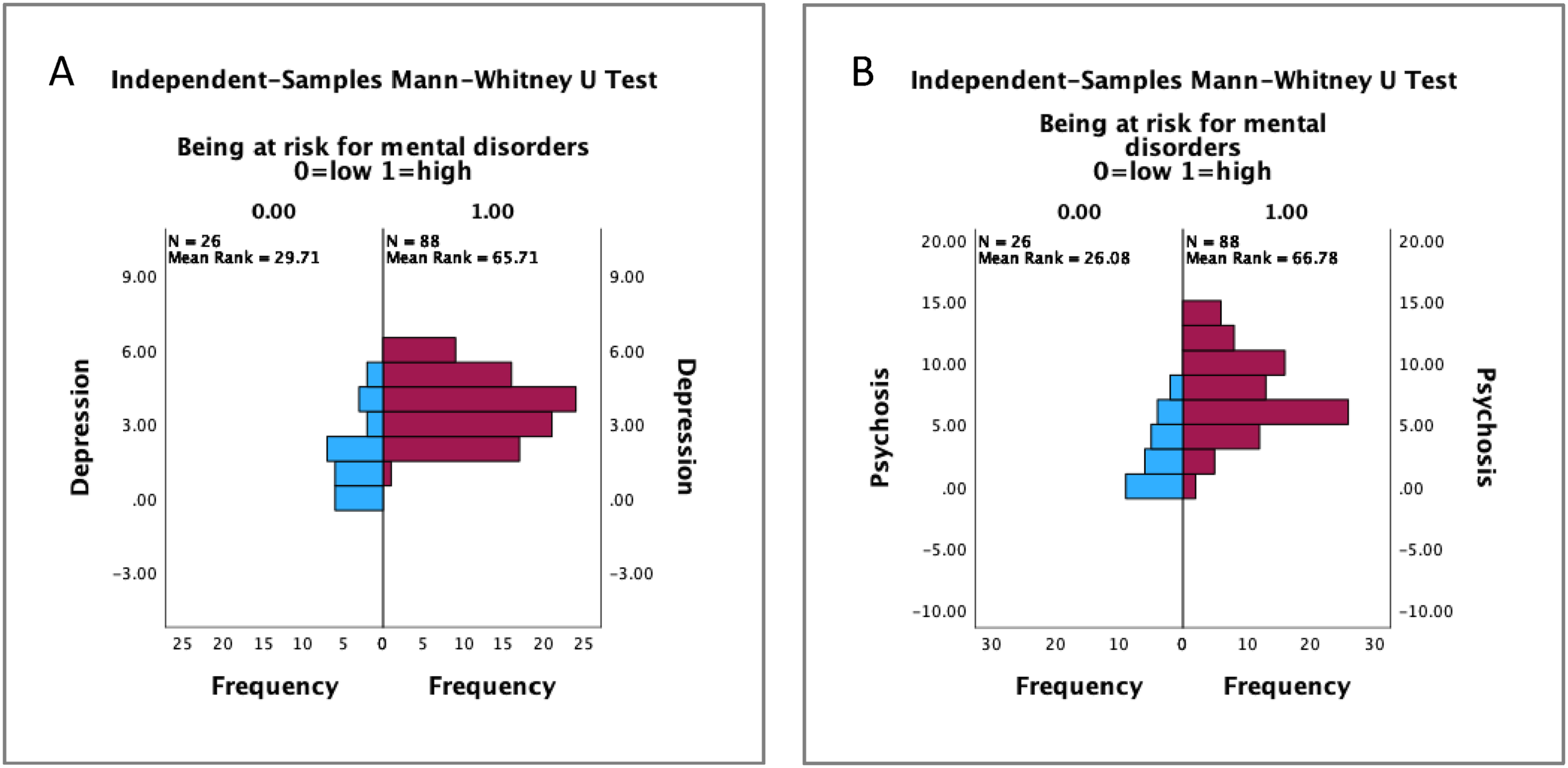
= .47; Figure 4(b)). The combined depression score was also significantly higher in the high-risk group (U = 704.50, p < .001; η
2
= .49; Figure 5(a)). Not agreeing to “I am usually a happy person” was significantly more frequent in the high-risk group (𝜒
2
= 15.78, df = 1, p < .001, φ = .37). Finally, the combined psychosis score was also higher in the high-risk group (U = 622.00, p < .001; η
2
= .53; Figure 5(b)). Agreeing to recreational substance use (H = 1.65, p > .05), depression (H = 1.54, p > .05) and psychosis-related (H = 0.69, p > .05) items did not differ between gender. (a) Recreational substance use and (b) global function levels of high versus low mental health risk. (a) Depression score and (b) psychosis score high versus low mental health risk.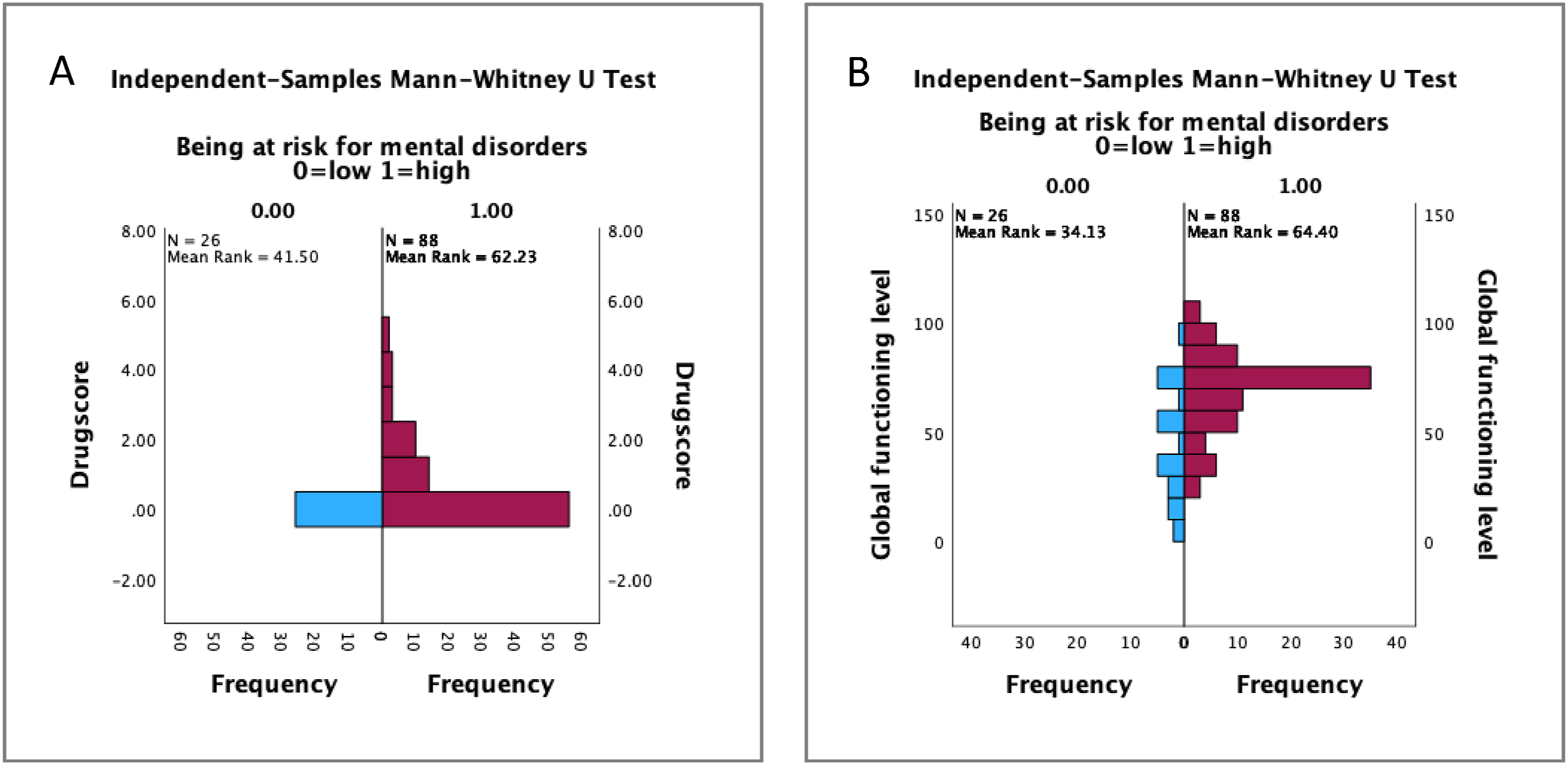
Global function levels and mental health
The mean value for the global level of functioning was 61.96 (SD = 22.32). The explorative regression analysis identified depression, psychosis and substance use combined to significantly predict self-assessed global function levels (ANOVA F = 25.44, p < .001; R
2
= 0.41) with depression items showing the strongest association (β = 0.63, p < .001; Figure 6), while elevated risk for psychosis predicted lower self-rated function levels (r
s
= 0.37, p < .001). Correlation (r
s
= 0.63, p < .001) of high depression score with low self-assessed global function levels.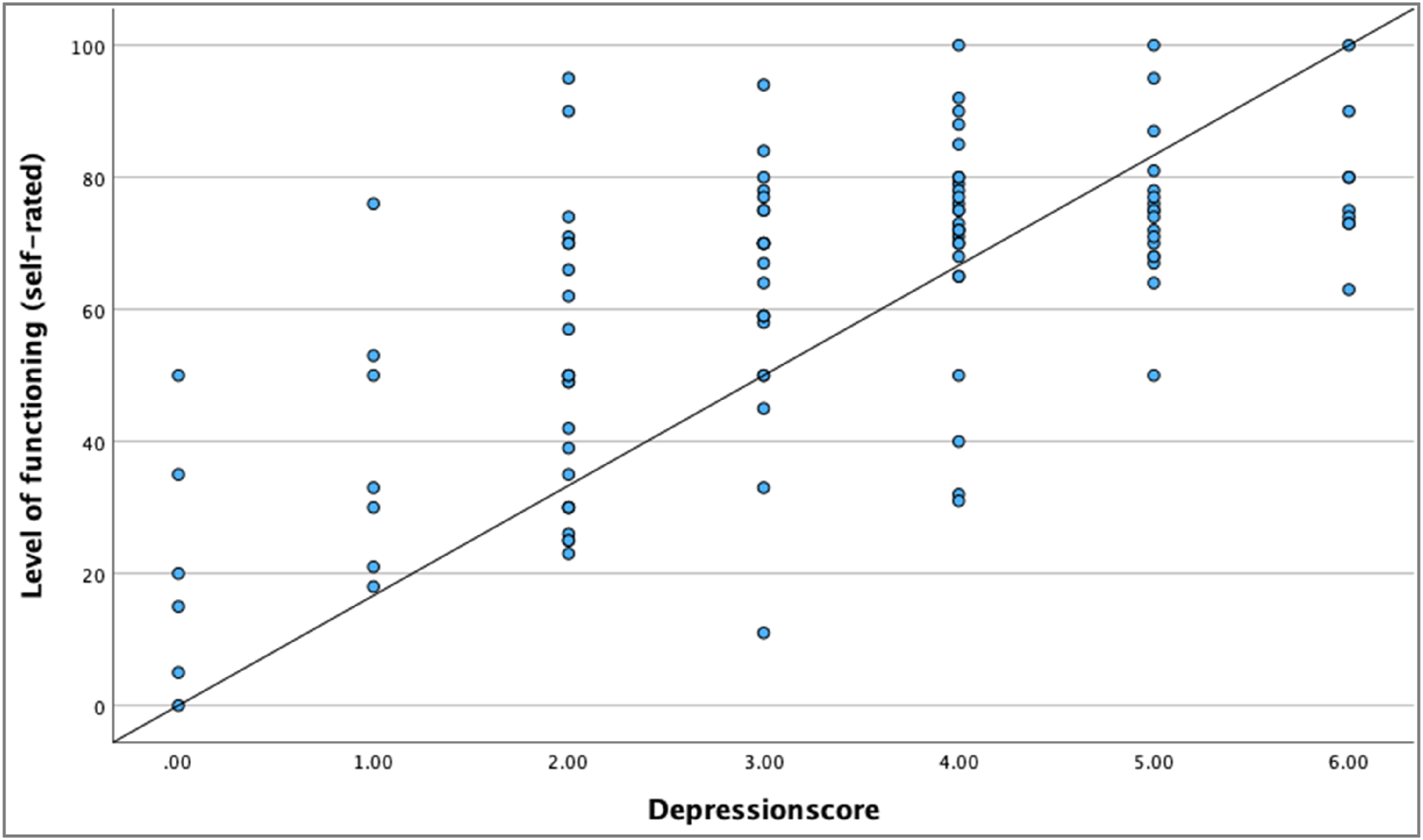
Discussion
The online self-assessment tool presented here effectively reached the intended young population with various levels of mental health concerns. Only six data sets were excluded because of the age exceeding the intended range of 12–30 years. Notably, predominantly women (65.7%) conducted the self-assessment of their mental health, suggestive of a higher motivation to seek help compared to their male counterparts, despite not differing in their risk levels. It is commonly observed that females report more often mental health problems than males (Tedstone Doherty & Kartalova-O'Doherty, 2010; Roberts, 1991). Similarly, Haavik et al. (2019) reported that female teenagers were more likely to not only identify psychological problems, but also to seek professional help.
In support of our hypotheses, a high-risk profile was associated with low global functioning, psychosis and depression items, and recreational substance use. High scores on depression, recreational substance use, and psychosis items were also associated with lower self-assessed global function levels. However, psychopathology and recreational substance use did not exhibit significant associations with ongoing treatment or satisfaction with treatment. Age and gender did not play a significant role in these associations.
When evaluating the findings of this study, it is necessary to acknowledge the inherent limitations of a self-selected sample, which is not representative of the general Australian young population. The cohort who voluntarily participated in the self-assessment for this study were burdened by a range of mental health problems. In addition, most of the data collection occurred during the COVID-19 pandemic, when schools were closed and day-to-day life was profoundly impacted by various levels of lock-downs, factors that may have influenced the participants mental health. Indeed, recent studies have reported negative impacts of the COVID pandemic on mental health, with rising levels of anxiety and increasing diagnoses of depression disorders at a population level (Fisher et al., 2020).
The self-assessment was based on the subjective experiences of potential mental health symptoms. Hence, we cannot extrapolate on potential diagnoses. However, the data provides valuable insights into how various symptom domains correlate with self-rated global functioning levels. Particularly, recreational substance consumption at concerning levels, symptoms indicative of depression, and perceptual phenomena together with unusual thought content were associated with lower self-rated global functioning and higher risk levels in our cohort. However, the actual impact on the socio-occupational functioning remains unknown. Hence, the addition of sections to the tool inquiring about areas of poor functioning in school, work, or social contexts would provide a more comprehensive understanding.
Finally, the lack of knowledge on whether the provided recommendations for seeking help were followed through is another limitation of the present study. The incorporation of a Likert scale to assess the likelihood of intending seeking help would be a meaningful addition to the tool.
In summary, our online mental health self-assessment tool was predominantly visited by the intended younger population. Of those completing the self-assessment and agreeing to have their data included in the current study, the level of psychopathology and risk was considerably high. However, only 38% reported receiving treatment for their mental health problems, indicating a disproportionally low participating rate in seeking professional help, particularly among male participants. The reasons for this were not assessed here and would require a more extensive database to identify potential barriers, including but not limited to factors such as rurality, financial limitations, stigma, and ethnicity.
Motivating young people with mental health problems or at risk of developing a severe mental illness, and providing appropriate youth-friendly services, are crucial to offer early evidence-based intervention. However, public mental health services are traditionally designed to provide care to patients with an established mental illness or in crisis. Hence, the threshold for young people accessing appropriate care is often too high and remains hidden below this access threshold. Offering internet-based pathways into care is a promising approach, provided that these pathways are also supported by appropriate services.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by Hunter Medical Research Institute (Project Grant ID: HMRI 13-61).