
Abstract
Background:
The aim of this study was to assess work system factors and nurse and physician well-being across professionals (nurse vs. physician) and geographic locations (rural vs. urban) during COVID-19 pandemic.
Methods:
This study invited nurses and physicians within four hospitals from one large healthcare system to participate: one urban academic medical center and three rural hospitals. We measured work systems factors using the National Academy of Medicine (NAM) framework and the National Institute for Occupational Safety and Health (NIOSH) survey. Wellbeing was measured using the 2-question summative burnout score, Patient Health Questionnaire (PHQ-9) to measure depression, and post-traumatic stress disorder (PTSD) checklist (PCL) to measure PTSD symptoms. Statistical analyses were conducted using Chi-square (for Likert-scale items) and t-tests (for continuous scales) as appropriate. Statistical significance was set at the .05 level, two-tailed.
Results:
Overall, our results suggested that nurses and physicians working in the urban settings experience more impeding work system factors and are more burned out, depressed, exhibit more PTSD symptoms, and face greater overall well-being issues, when compared to nurses and physicians working in the rural settings.
Conclusions/Applications to Practice:
This study examined a comprehensive set of work system factors and well-being measures to better understand differences between rural and urban settings, and nurses compared to physicians. By examining this entire set of measures, we were able to provide a greater insight into the key differences, highlighting opportunities for policy-level contributions to prevent work related impairments from reaching the healthcare workforce.
Background
With more than 4 million nurses (American Association of Colleges of Nursing, 2023) and 1 million physicians in the U.S. (American Medical Association, 2024), these two groups represent the largest healthcare workforce segments affected by the COVID-19 pandemic. Evidence suggests an extremely high burden on clinician (physicians and nurses) well-being for those who responded to the pandemic (Matsuo et al., 2020; Salazar de Pablo et al., 2020). The pandemic markedly worsened the concerns about clinician well-being that had been growing over the last decade (National Academies of Sciences, Engineering, and Medicine et al., 2019; Shreffler et al., 2020). In 2018, the National Academy of Medicine (NAM) identified key dimensions of clinician well-being, with burnout and depression being the two most common issues. NAM also emphasized the importance of focusing on overall or composite well-being (CWB; National Academies of Sciences, Engineering, and Medicine et al., 2019).
During the early stages of the pandemic, urban and rural healthcare organizations had to rapidly shift operations to accommodate changes and disruptions in supply chains and patient healthcare needs. Crisis standards of care remained in place longer than initially anticipated, adding more stress to clinicians (Short & Mammen, 2020). Additionally, clinician worries about exposing their families to COVID-19 added extra pressure as they tried to balance the responsibilities to their families, and obligations to their organizations and patients (Sasangohar et al., 2020). Nurses and physicians also witnessed their colleagues getting sick and dying in unprecedented numbers. By the end of 2020, nurses had the highest rate of death by occupation (484/3148) and physicians had the third highest (248/3148; The Guardian, 2024). In 2019, the National Academy of Medicine declared “crisis levels” of burnout among healthcare professionals, with nurse burnout rates reaching up to 54% (Kelly et al., 2021).
Before the pandemic, rates of burnout, depression, and suicide were much higher among nurses and physicians than in the general worker population (Dall’Ora et al., 2020; National Academies of Sciences, Engineering, and Medicine et al., 2019). Since its recognition in the 1970s, the prevalence of burnout has greatly increased in nurses and physicians (Reith, 2018). In a study of more than 6,000 US physicians from 2011 to 2014, the prevalence of burnout increased from 45% to 54% (Shanafelt et al., 2015). A recent meta-analysis examining 113 studies of nurse burnout over three decades studies, yielding a total of 45,539 nurses across 49 countries, found the pooled-prevalence rate was 11.23% for high burnout symptoms, suggesting one-tenth of the nurses worldwide suffered high burnout symptoms (Woo et al., 2020). In fact, the World Health Organization (2019) declared burnout as an “occupational phenomenon” in the International Classification of Diseases 11th revision (ICD-11), recognizing burnout as a serious health issue.
During the pandemic, both depression and suicide rates increased (O’Riordan, 2020; The Guardian, 2024). Evidence also suggests that the pandemic elevated rates of post-traumatic stress disorder (PTSD) in nurses and physicians (Andhavarapu et al., 2022; Cramer et al., 2022; d’Ettorre et al., 2021; Lake et al., 2022). Even before the COVID-19 pandemic, at least 30% of nurses reported PTSD (Melnyk et al., 2018). During the pandemic, the prevalence of depression in the general population increased threefold (Ettman et al., 2020) and for clinicians, depression levels rose to around 50%, leading to cases of suicide in some instances (O’Riordan, 2020; Salari et al., 2020; Wu et al., 2021). Thus, the pandemic experience for healthcare workers has increasingly been recognized as traumatic, with many professional ethical conflicts associated with PTSD (Chen et al., 2020; d’Ettorre et al., 2021; Greenberg, 2020).
Additionally, the pandemic impacted an already complex and interdependent healthcare work system (Carayon et al., 2021) with context-dependent factors affecting clinician well-being. Post-pandemic, approximately 48.2% of physicians and 56% of nurses reported experiencing some level of burnout, down from 53% and 64% in 2022, respectively (American Medical Association, 2024; Office of the Surgeon General, 2022). While this suggests that physician and nurse burnout has fallen since its peak in late 2021, the extent of the problem remains an alarming reality that demands ongoing attention, especially among those at the highest risk.
Thus, there is a need to assess work system factors (e.g., work environment, safety culture, health promotion, social support) and nurse and physician overall well-being (e.g., burnout, depression, PTSD) during and after the COVID-19 pandemic. These factors may vary across professionals (nurse vs. physician) and geographic locations (rural [those not located within a metropolitan area] vs. urban). Our study responds to the National Occupational Research Agenda (NORA)/National Total Worker Health strategic goal to advance research by identifying and investigating the work system factors contributing to worker safety, health, and overall well-being. Our results have potential to inform future larger studies to evaluate the impact of targeted improvement interventions, aimed at work system factors, on clinician well-being across diverse healthcare populations and settings.
Methods
Conceptual Model for Assessing Nurse and Physician Well-Being
Healthcare professionals’ well-being is a key component of the Quadruple Aim for improving healthcare quality (Bodenheimer & Sinsky, 2014). The Quadruple Aim framework was designed to help healthcare organizations improve patient experience of care, improve population health, reduce healthcare costs, and improve healthcare professionals’ well-being (Institute for Healthcare Improvement, 2024). The fourth aim of well-being was developed to address the unintended consequences of the 2007 Triple Aim, which resulted in significant strain on healthcare professionals. In particular, the frequent changes in work processes to meet the Triple Aim goals resulted in high burnout, decreased joy in work, and diminished well-being (Dyrbye et al., 2017; Shanafelt et al., 2016).
Thus, our study is guided by the National Academy of Medicine (NAM) framework which posits that clinician well-being is affected by work system factors situated within three levels: front-line care delivery, healthcare organization, and the external environment (National Academies of Sciences, Engineering, and Medicine et al., 2019). In the NAM framework, the risks to well-being come from heavy workloads, workplace violence, racism, unclear or conflicting demands, lack of involvement in decisions or input in how the work is done, poor communication, lack of support from managers and co-workers, poorly managed organizational changes, job insecurity, and non-stop demands that continue after work hours (Brigham et al., 2018).
Our study also integrates the National Institute for Occupational Safety and Health (NIOSH) worker well-being framework which holistically includes five domains important for worker well-being that contribute to total worker health (Chari et al., 2018; Sorensen et al., 2021). The NIOSH worker well-being framework and subsequent NIOSH well-being questionnaire (WellBQ) provides an in-depth integrated assessment of the five dimensions affecting worker well-being. The NIOSH WellBQ includes not only work-place factors but also individual’s circumstances outside of work that may affect their well-being at work. Worker well-being is affected by physical and safety features of the work environment, organizational policies, programs, and practices, individuals’ physical and mental health and welfare, individuals’ experiences and evaluations relating to the quality of their work life, and the external context that are situated outside of work but may still influence worker well-being (Chari et al., 2018).
Together these two synergistic frameworks provide structure for examination of the influence of work system factors from the environment, hospital and unit, as well as individual clinician factors on clinician well-being. Among clinicians, nurses and physicians are the largest healthcare workforce groups, thus examining, nurse and physician overall well-being and their work system factors during a pandemic is an urgent public health concern (American Association of Colleges of Nursing, 2023).
Using validated survey instruments, this study invited all nurses and physicians within four hospitals from one large healthcare system to participate: one urban academic medical center and three rural hospitals. Patients or the public were involved in the design, or conduct, or reporting, or dissemination plans of our research.
Study Participants
We administered the survey (May 2022–November 2022) to all nurses and physicians working in the respected hospitals (n~1,400; physicians included advanced providers: nurse practitioners and physician assistants).
Data Collection
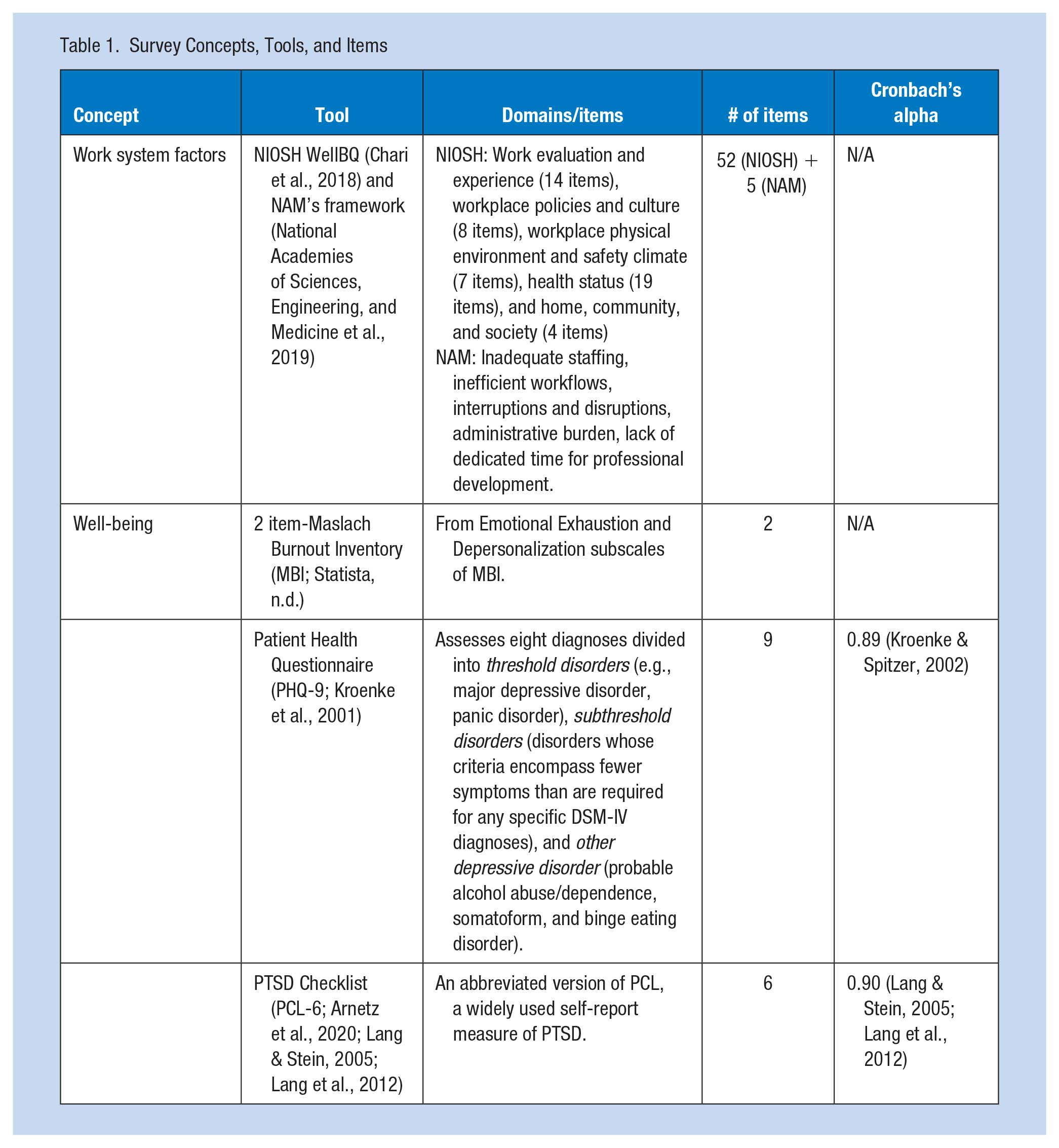
Based on the proposed conceptual framework, we measured work systems factors and the overall well-being of nurses and physicians using a set of validated concepts, tools, and items as depicted in Table 1.
Survey Concepts, Tools, and Items
National Academy of Medicine Survey
The NAM survey included five critical factors related to nurse and physician burnout that were not systematically addressed in the NIOSH WellBQ survey (National Academies of Sciences, Engineering, and Medicine et al., 2019). These five items included, staffing levels, workflow efficiency, interruptions and disruptions, administrative burden, and lack of dedicated time for professional development. Participants were asked to rate the extent to which they felt these specific factors contributed to burnout, using a scale from 1 (strongly disagree) to 7 (strongly agree). For data analysis, scores of 1 to 3 were categorized as “negative” responses, 4 as an “intermediate” response, and 5 to 7 as “positive” responses. Higher values indicated a stronger agreement that the factor contributed to burnout.
NIOSH WellBQ
The NIOSH WellBQ validated survey included 68 items along with additional demographic questions (Chari et al., 2018; Sorensen et al., 2021). Each domain includes several constructs measured using a combination of single-item and scale questions with most questions utilizing various Likert-scale responses (e.g., Strongly Disagree-Strongly Agree, Never-Always, etc.). For data analysis, low scores (or high scores on negatively worded questions) represented “negative” responses, while high scores represented “positive” responses. Domain 1 represents Work Evaluation and Experience and includes 14 constructs (16 items). Domain 2 represents Workplace Policies and Culture and includes six constructs (14 items). Domain 3 represents Workplace Physical Environment and Safety Climate and includes six constructs (10 items). Domain 4 represents Health Status and includes 19 constructs (23 items). Finally, domain 5, Home, Community, and Society, includes four constructs (5 items). This survey is designed to assess various industries, not just healthcare environments.
Burnout
We used validated 2-question summative burnout score that correlates with the full Maslach Burnout Inventory-Human Services Survey (MBI-HSS; Li-Sauerwine et al., 2020). The two survey items were: (i) “I feel burned out from my work” (representing emotional exhaustion) and (ii) “I have become more callous toward people since I took this job” (representing depersonalization; DP1). Responses to these items were measured using a 7-point Likert-scale (from Strongly Disagree to Strongly Agree). For each item, a score >3 was defined as burned out (marked as “negative” for data analysis).
Patient Health Questionnaire (PHQ)
We used validated Patient Health Questionnaire (PHQ-9), which is the 9-item version of the full PHQ, with depression being diagnosed if 5 or more of the 9 depressive symptom binary (yes/no) criteria have been present at least “more than half the days” in the “past 2 weeks” (thus, marked as “negative” for data analysis; Kroenke et al., 2001).
Post Traumatic Stress Disorder (PTSD)
We used validated PTSD checklist (PCL), a self-report measure of PTSD symptoms (Arnetz et al., 2020; Lang et al., 2012). Specifically, we used the PCL-6, which includes 6 out of the 17 items from the PTSD Civilian version. Responses to survey items were measured on a 5-point scale to evaluate severity of PTSD symptoms (from 1 representing “not at all” to 5 representing “extremely”). A total score of 14 or more suggests difficulties with post-traumatic stress and is marked as a “negative” result for data analysis.
Data Analysis
The objective of the analysis was to quantitatively assess differences in work system factors and over all well-being between nurses and physicians, and between geographic locations (rural vs. urban). We received 222 total responses (approximately 16% response rate), with a breakdown of sample characteristics (e.g., rural vs. urban; nurses vs. physicians; gender, and race) summarized in Table 2. Across all the collected measures of work systems factors and wellbeing, descriptive statistics and comparisons using the negative, intermediate, and positive results were conducted using Chi-square (for all Likert-scale items) and t-tests (for the few WellBQ items using continuous scales) as appropriate. Statistical significance was set at the .05 level, two-tailed. Our study adhered to Institutional Review Board (IRB) protocols for participant recruitment and consent acquisition. All participants in this research gave informed consent before taking part of this study.
Sample Characteristics (n = 222)
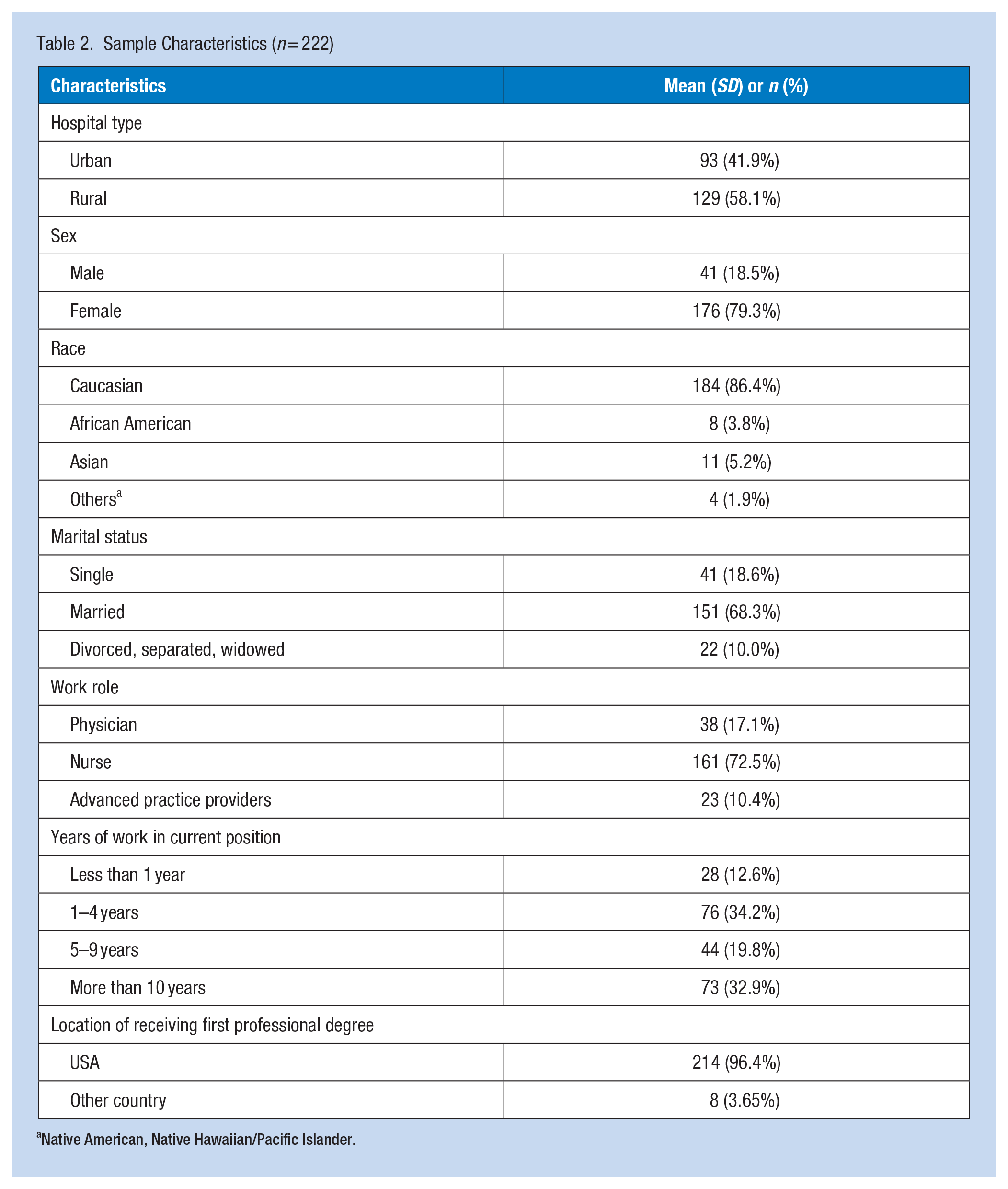
Native American, Native Hawaiian/Pacific Islander.
Results
Our study had a response rate of about 22% (222 clinicians) across hospitals with 93 from the urban hospital, and 129 from the three rural hospitals. The distribution of nurses and healthcare providers was 161 and 61, respectively (see Table 2 for demographic information of the sample).
Work System Factors
NAM’s Framework
Results (see Table 3) indicated that the participants’ burnout from the urban hospital was more affected by staffing issues, inefficient workflows, interruptions and distractions, and administrative burden than participants from the rural settings. There were no statistically significant differences regarding lack of time for professional development requirements. Results also indicated that nurses felt significantly less stress because of interruptions and distractions than physicians.
NAM Framework: Comparison Between Physicians and Nurses in Urban Versus Rural Settings, n (%)
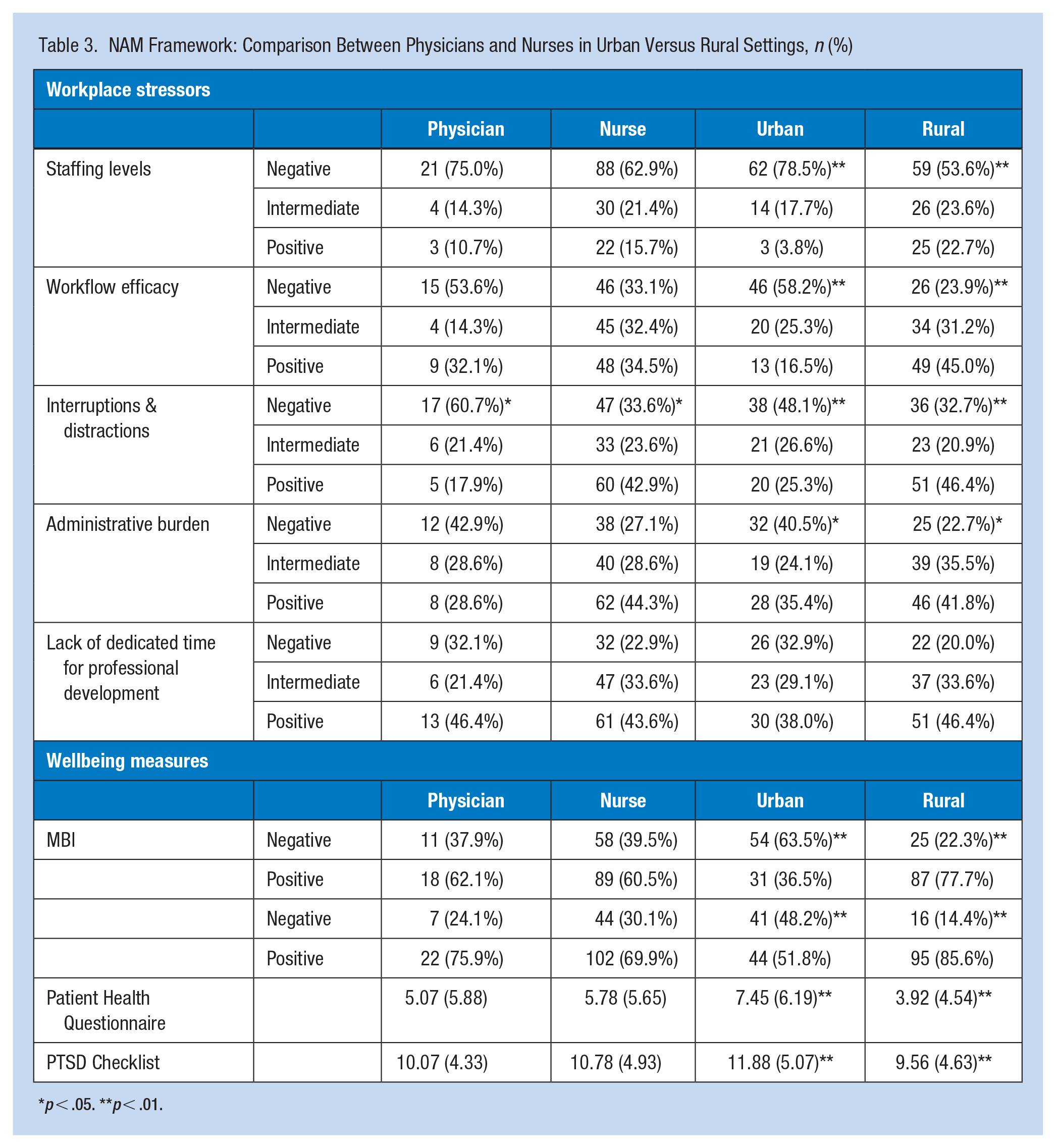
p < .05. **p < .01.
NIOSH WellBQ
Figures 1 and 2 visually present results regarding NIOSH WellBQ survey. Specifically, Figure 1 outline results for items using Likert scales, comparing rural versus urban settings and nurses versus physicians, respectively. Figure 2 present results for items using variable scales, also comparing rural versus urban and nurses versus physicians. In the following sections, we examine the results of the NIOSH WellBQ survey in detail, mapping individual survey questions (Q) to the corresponding figures.
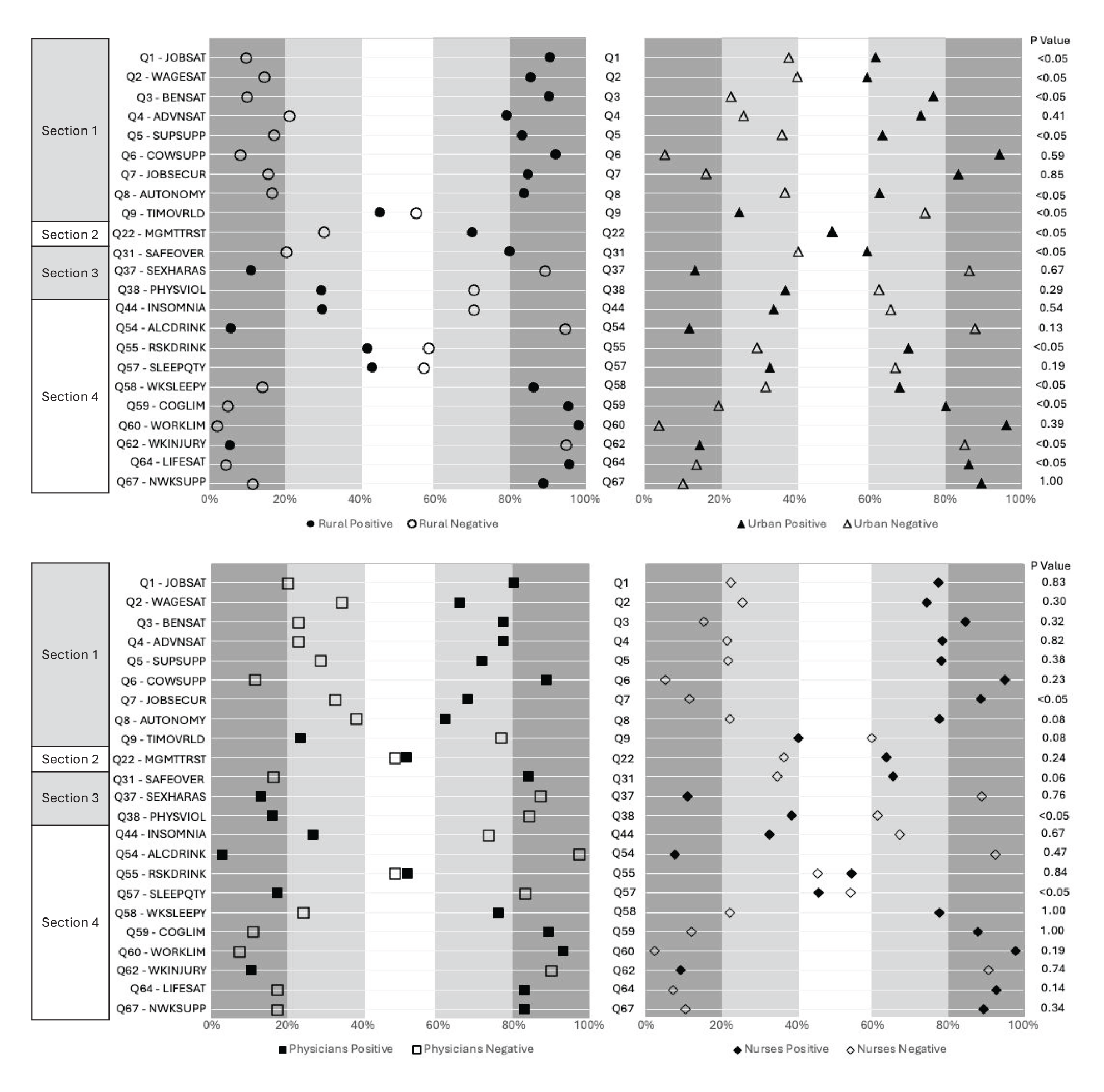
Top: WellBQ survey results: Rural versus urban (Likert scale items only (N = 222)). Bottom: WellBQ survey results: Physicians versus nurses (Likert scale items only (N = 222)). Graph on the left shows percent positive responses (e.g., scores 3 [agree] and 4 [strongly agree] on the 5-point Likert scale) versus percent negative responses (e.g., scores 2 [disagree] and 1 [strongly disagree] on the 5-point Likert scale) results for rural hospitals. Same results are shown on the right side for the urban hospitals.
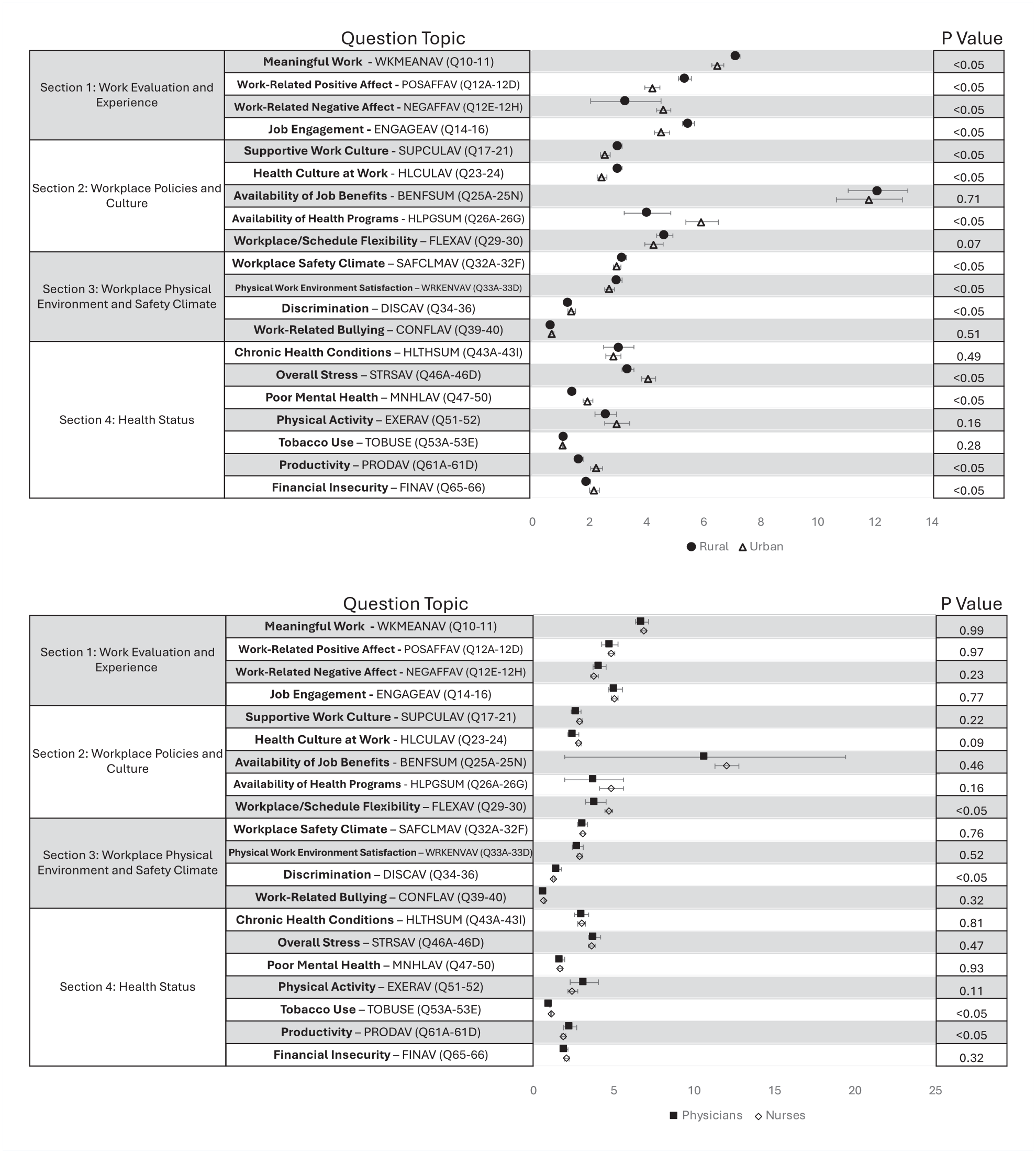
Top: WellBQ survey results: Rural versus urban (non-Likert scale items only (N = 222)). Bottom: WellBQ survey results: Physicians versus nurses (non-Likert scale items only (N = 222)). As items are based on different scales and different processing calculations, mean and standard errors are presented with corresponding p-values.
Section 1 (work evaluation and experience; Q1 to 9 shown on Figure 1; Q10 to 16 shown on Figure 2): Eleven out of 14 items indicated significantly more negative results for the participants from the urban hospital (79%; job satisfaction (Q1), wage satisfaction (Q2), benefits satisfaction (Q3), supervisor support (Q5), job autonomy (Q8), time paucity/work overload (Q9), meaningful work (Q10–11), work-related positive affect (Q12 A–D), work-related negative affect (Q12 E–H), work-related fatigue (Q13), and job engagement (Q13–16)) than participants from the rural settings. Three of 14 items (21%; satisfaction with advancement opportunities (Q4), coworker support (Q6), and job security (Q7)) indicated statistically no differences. Results also indicated that nurses felt significantly (i) more job security (Q7), (ii) more job autonomy (Q8), and (iii) less work-related fatigue (Q13) than physicians.
Section 2 (workplace policies and cultures; Q17–30): Two out of eight items indicated significantly more negative results for the participants from the urban hospital (25%; availability of job benefits (Q25 A–N) and non-work to work conflict (Q27–28)) than participants from the rural settings. Remaining 6 out of 8 items (75%; supportive work culture (Q17–21), management trust (Q22), health culture at work (Q23–24), availability of health programs at work (Q26 A–G), work to non-work conflict (Q27), and workplace/schedule flexibility (Q29–30)) indicated statistically no differences. Results also indicated that nurses felt (i) significantly less effect of job demands disturbing their personal lives (Q27) and (ii) more schedule flexibility (Q29–30) than physicians.
Section 3 (workplace physical environment and safety climate; Q31–40): Four out of seven items indicated significantly more negative results for the participants from the urban hospital (48%; overall workplace safety (Q31), workplace safety climate (Q32 A–F), physical work environment satisfaction (QQ33 A–C), and discrimination (QQ34–36)) than participants from the rural settings. Three out of seven items (42%; work related sexual harassment (Q37), work related physical violence (Q38), work related bullying (Q39–40)) indicated statistically no differences. Results also indicated that nurses (i) felt significantly less discriminated (Q34–36) against because of age, race, and gender, and (ii) experienced significantly more physical violence (Q38) than physicians.
Section 4 (health status; Q41–63): Seven out of 19 items indicated significantly more negative results for the participants from the urban hospital (37%; overall stress (Q46 A–D), poor mental health (Q47–50), risky drinking (Q55), feeling sleepy at work (Q58), cognitive functionating limitations (Q59), productivity (Q61 A–D), and work related injury (Q62)) than participants from the rural settings. Twelve out of 19 items (63%; overall health (Q41), days of poor physical health (Q42), chronic health conditions (Q43 A–I), insomnia (Q44), days of poor mental health (Q42), physical activity (Q51–52), tobacco use (Q53 A–E), alcohol consumption (Q54), healthy diet (Q56), sleep hours (Q57), work limitations (Q59), and injury consequence (Q63)) indicated statistically no differences. Results also indicated that nurses used significantly more tobacco products (Q53 A–D), got on average significantly more hours of sleep per night (Q57), felt significantly more productive (Q61 A–D; e.g., staying focused, being careful, working when supposed to work, getting things done) than physicians.
Section 5 (home, community, and society; Q64–68): Three out of four items indicated significantly more negative results for the participants from the urban hospital (75%; life satisfaction (Q64), financial insecurity (Q65–66), and activities outside the work (Q68 A–G)) than participants from the rural settings while support outside work indicated no differences. No statistically significant differences between nurses and physicians were noted in this section.
Wellbeing Measures
Burnout (2-Item Inventory)
Results (see Table 3) indicated that participants from the urban hospital felt significantly more burned out and callous toward people compared to those from rural settings. Specifically, 63.5% of nurses and 48.2% of physicians in urban settings experienced emotional exhaustion and depersonalization, respectively. No statistically significant differences between nurses and physicians were noted.
PHQ-9
Results (see Table 3) indicated that participants from the urban hospital felt significantly more depressed than participants from the rural settings, with depression levels interpreted as “mild” in urbans settings and “minimal” rural settings. No statistically significant differences between nurses and physicians were noted.
PTSD (PLC-6)
Results (see Table 3) indicated that participants from the urban hospital reported significantly more PTSD symptoms compared to those from rural settings. However, both groups scored below the threshold (=>14) that would suggest difficulties with post-traumatic stress and need for further assessment or possible referral for treatment. No statistically significant differences between nurses and physicians were noted.
Discussion
Urban Versus Rural Results
Nurses and physicians in the urban setting felt significantly more impacted by staffing issues, inefficient workflows, interruptions and distractions, and administrative burden than participants from the rural settings. There are also differences between urban and rural settings in factors related to work evaluation and experience (e.g., job satisfaction, job engagement), workplace physical environment and safety climate (e.g., workplace safety and safety climate), and health status (e.g., stress, mental health, productivity). The only exception was time for professional development requirements which indicated no difference between the two settings. Furthermore, nurses and physicians working in the urban settings indicated less overall life satisfaction, less financial insecurity, and less engagement with activities outside the work (Jansen, 2020). Overall, these findings are mostly aligned with prior research, suggesting that job satisfaction/engagement, safety climate, and stress-related factors are typically factors associated with nurse and physician wellbeing and retention (Bice & Hepworth, 2024; Harry et al., 2024; Pressley & Garside, 2023).
While not statistically significant between urban versus rural settings, we found that approximately 11% (rural) and 14% (urban) of survey participants were sexually harassed (Acquadro Maran et al., 2022; National Academies of Sciences, Engineering, and Medicine et al., 2018); 30% (rural) and 38% (urban) experienced physical violence (Andersen et al., 2023; Jones et al., n.d.; Lim et al., 2022); and 66% (rural) and 69% (urban) experienced some form of bullying, all at work (Boudrias et al., 2021; Gupta et al., 2020). These findings are concerning and confirm the results from previous studies published between 2013 and 2023 on increasing rates of workplace violence against healthcare professionals worldwide (Crabtree, 2022; Yusoff et al., 2023).
Well-being related measures also indicated that the nurses and physicians working in the urban settings indicated higher levels of burnout, depression, and PTSD symptoms. These results are in disagreement with number of prior findings suggesting that nurses and physicians in urban settings experience similar burnout levels (Bethea et al., 2020; Singh et al., 2015; Ward et al., 2021). For example, a national study of 2,790 medical practitioners found no difference in burnout between rural and urban settings (Ward et al., 2021). Similarly, prior studies reported no difference in rates of burnout among mental health nurses (Singh et al., 2015) across rural and urban settings, and comparable rates to national rates in both rural trauma nurses (Bethea et al., 2020) and nurses in Critical Access Hospitals.
Nurse Versus Physician Results
Considering the NAM’s framework, our results indicate that nurses felt significantly less stress from interruptions and distractions compared to physicians. Prior studies have linked interruptions and distractions with suboptimal levels of human performance and patient safety (Sanderson et al., 2019). Thus, it is worrisome to note that approximately 60% of participating physicians (compared to 33% of nurses) in our study were negatively affected by such conditions. No statistically significant differences between nurses and physicians were noted in the well-being measures (burnout, PHQ-9, PTSD (PLC-6)). This finding is to some degree surprising in comparison to previous studies measuring related concepts (Lluch et al., 2022). For example, Sexton et al. (2022) measured one aspect of burnout, emotional exhaustion (EE), among US healthcare professionals and found that nurses had significantly higher levels of EE than did attending physicians both prior to (nurses: 40.6%, 95% CI [38.4, 42.9], physicians: 30.6%, 95% CI [30.6, 36.5]) and during the COVID-19 pandemic (nurses: 49.2%, 95% CI [46.5, 51.9], physicians: 40.1%, 95% CI [36.2, 44.4]). Lin and Yeh (2023) concluded that hospital-based nurses appear to be at higher risk for developing post-traumatic stress disorder during the COVID-19 pandemic. Thus, further longitudinal research is needed to better understand the long term effect of COVID-19 pandemic on mental health issues.
Nurses felt significantly more job security and autonomy, and less work-related fatigue than physicians. This finding is in alignment with recent findings suggesting that nurses suffer most due to lack of staffing shortages and lack of shared values with leadership where physicians suffer most due to lack of control over workload (while affected by staffing shortages during COVID-19 pandemic) and chaotic work environments (Bice & Hepworth, 2024). For example, a recent qualitative study of physicians’ work environments and work-related well-being suggests that physicians are tired, slighted, and frustrated about their work conditions during the pandemic (Buchbinder et al., 2023). Patient behaviors were challenging, lack of or poorly qualified nurse staffing was dangerous, tensions between nurses and physicians grew, and physicians expressed frustration with their organizational policies and work conditions. Results also indicated that nurses felt significantly less discriminated against because of age, race, and gender, and experienced significantly more physical violence than physicians. Overall, workplace violence has been a consistent and worrisome concern, especially during and after the pandemic (Caruso et al., 2022; Molero Jurado et al., 2023).
Finally, results also indicated that nurses used significantly more tobacco products, got on average significantly more hours of sleep per night, and felt significantly more productive (e.g., staying focused, being careful, working when supposed to work, getting things done) than physicians. These findings are mostly in agreement with prior findings confirming that working under the influence of many these symptoms significantly impairs work productivity and leads to occupational accidents and errors (Shaik et al., 2022; Trojak et al., 2023). Thus, our results suggest that overall productivity (e.g., staying focused, being careful, working when supposed to work, getting things done) is more suboptimal in physicians. While not controlled these conditions can take a heavy toll on patient care due to the increased risk of medical errors (Garcia et al., 2019).
Limitations
Considering that nurses and physicians were extremely busy with patient care during COVID-19 pandemic, there was a relative low response rate on surveys. There was also limited diversity among hospital settings (one academic medical center and three rural hospitals from one healthcare system) and survey participants (most white, non-Hispanic; 86.4%). With this relatively small sample size and limited diversity among survey participants, there are shortcomings with generalizability of our findings. We encouraged survey participation by asking participating organization to offer protected time, send reminders, and enlisting encouraging communication from local champions. There is also an inherent risk of bias in our results attributable to the lack of psychological safety to share views, experiences, and feelings regarding survey items. Despite the limitations, we believe that the results offer important insights of the views, experiences, and feelings of the nurses and physicians, especially within participating institutions for the one healthcare system. Data collection took place from September to December 2022, coinciding with a time when clinicians were still grappling with the significant workloads resulting from the COVID-19 pandemic. During this period, they were also exposed to several similar surveys evaluating work-related stress and job satisfaction. The relatively extensive nature of our survey may have added to the strain on these already occupied healthcare professionals, which could have led to a diminished response rate. Future investigations might consider streamlining the number of survey items to better align with clinicians’ workloads. Furthermore, research should strive to incorporate larger and more representative samples to facilitate a more thorough analysis of clinician well-being in both rural and urban environments. Longitudinal studies are also essential to identify causal relationships among the various factors affecting clinician well-being as well as possible associations of well-being with clinical outcomes.
Implications for Occupational Health Nursing Practice
Overall, unlike other studies that often focus on a subset of measures, this study examined an entire set of work system factors and well-being measures to better understand differences between rural and urban settings, and nurses compared to physicians. By examining this entire set of measures, we were able to provide a greater insight into the key differences, highlighting opportunities for policy-level contributions to prevent such harms from reaching the healthcare workforce. Our results suggest that nurses and physicians working in the urban setting experienced more work system factors impeding them when compared those in rural settings. There are especially stark differences between urban and rural settings in factors related to job satisfaction, job engagement, workplace physical environment and safety climate, and overall mental health status impeding productivity. Our findings indicate that nurses and physicians working in the urban setting are more burned out and depressed, exhibit more PTSD symptoms, and face greater overall well-being issues. This can result in suboptimal life satisfaction, worries of financial insecurity, and decreased engagement in activities outside of work (Jansen, 2020). Thus, based on these results, a comprehensive study with larger sample sizes and participation of healthcare systems across various U.S states is needed to further evaluate effective interventions to improve well-being of nurses and physicians in urban settings. Finally, our data revealed concerning and unacceptable issues related to sexual harassment, physical violence, and bullying at work (Boudrias et al., 2021; Gupta et al., 2020).
Applying Research to Occupational Health Practice
Evidence suggests an extremely high burden on physicians and nurses’ well-being for those who responded to the pandemic. The pandemic markedly worsened the concerns about clinician well-being that had been growing over the last decade. Our results suggest that nurses and physicians working in the urban setting experienced more work system factors and wellbeing issues impeding them when compared those in rural settings. There is a need for a comprehensive study with larger sample sizes and participation of healthcare systems across various U.S states is needed to further evaluate effective interventions to improve well-being of nurses and physicians in urban settings.
Footnotes
Acknowledgements
We would like to thank the UNC Health and the Carolina Center for Healthy Work Design and Worker Well-Being for supporting this research project. We also want to thank Cody Mitchell (medical student) for generating the Figures and Gwen Fenny (PhD student) in participating in our data analysis sessions.
Author Contributions
LM, MB, KA, BE, and SMB contributed to the original conception and design of the work. All authors contributed to the analysis and interpretation of data for the work. Manuscript was drafted and approved by all authors.
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: None related to this project. LM is (i) a founder and president of MaiaZura, LLC providing teamwork training for healthcare professionals and (ii) advisor to Communify, LLC providing project management and improvement software for healthcare industry.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Institute for Occupational Safety and Health (NIOSH 1U19OH012303).
Ethical Approval
This study obtained an ethics approval via the institutional review board (#21-2592) at the University of North Carolina. All participants in this research gave informed consent before taking part of this study. Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.