
Abstract
Internationally, nurses and midwives played a major role in the care of patients with COVID-19. More qualitative studies now exist, but still little is known about the psychosocial impact. The aim of this study was to assess the psychosocial impact of the COVID-19 pandemic on nurses and midwives in Denmark. A cross-sectional survey completed by nurses and midwives employed at a university hospital in Denmark between May and June 2020 was conducted. Psychological distress was assessed using the Depression, Anxiety and Stress Scale (DASS-21). The study was conducted in accordance with the STROBE guidelines. A total of 1416 (37.9%) nurses and midwives completed the survey, 61% (n = 843) felt at risk of getting COVID-19, and 27% (n = 377) felt more stressed than usual. Overall, nurses and midwives did not experience psychological distress at the beginning of the pandemic. However, exposure to COVID-19 was associated with symptoms of depression, anxiety, and stress.
Background
Internationally, nurses and midwives have played a major role in the treatment and care of patients with COVID-19, as they are the largest clinical discipline in a healthcare sector and have more direct and continuous contact with patients than other clinical groups. Many nurses have experienced an increase in workload and work intensity during the COVID-19 pandemic and have often had to implement and adapt to new ways of working 1 and changes in work tasks and redeployment to other wards or areas. 2
COVID-19 was not known before the outbreak in Wuhan, China in December 2019. In March 2020, there were around 300,000 confirmed cases of COVID-19 worldwide and the World Health Organization declared the COVID-19 outbreak a pandemic. 3 Denmark had its first COVID-19 patient at the end of February 2020 and by June 2020, Denmark had around 12,000 cases, around 2300 patients had been hospitalized and 582 were dead. 4 Mortality among people infected with this new coronavirus varies across countries. In June 2020, Denmark had 10.1 deaths per 100,000 people, while the corresponding figures were 10.5 in Germany, 45.7 in Sweden, 5.8 in Finland, and 4.5 in Norway. 5 In February 2021, there were over 111 million cases and more than 2,400,000 deaths from COVID-19 worldwide. 6
In March 2020, many countries around the world, including Denmark, implemented initiatives to manage the outbreak of COVID-19 and reduce the impact on health services. These initiatives included the closure of non-essential services and schools. In Denmark, health services implemented several infection control strategies aimed at protecting staff and ensuring high-quality patient care including personal protective equipment (PPE) for healthcare workers, restrictions on visitors to hospitals, the implementation of telehealth services, and a reduction in face-to-face consultations.
Healthcare professionals have experienced great concerns with respect to the risk of being infected as well as the risk of infecting other patients and family, relatives, and society. 7 Furthermore, data have shown a substantial number of cases of COVID-19 among frontline staff, especially nurses. 8
Studies on infectious disease outbreaks, such as Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS), demonstrate that nurses often have a high level of concern for their personal and relatives’ health during infectious outbreaks but at the same time feel obliged to treat ill patients,1,9 and experience high levels of occupational stress. 10 Thus, several studies have reported a negative psychological impact of COVID-19 on healthcare staff, e.g. nurses,9,11,12 and that healthcare workers’ wellbeing deteriorated as the pandemic continued. 13 Several qualitative studies have demonstrated that nurses have worked under great pressure during the pandemic.14–17 Nevertheless, to date, mostly only smaller studies have been conducted in Denmark, and the psychosocial impact of COVID-19 on nurses and midwives in Denmark is not well understood.2,16,18–20 The number of COVID-19 cases and deaths in Denmark has been low compared to other European and high-income countries. 21 Still, there is a lack of knowledge to inform responses to future outbreaks of infectious diseases and other ‘crises’/adverse events. Understanding of nurses’ and midwives’ COVID-19-related psychosocial concerns and the impact of the pandemic on their work will help in the development and implementation of appropriate support initiatives. Thus, the aim of this study was to investigate the psychosocial impact of COVID-19 on nurses and midwives in Denmark. The specific objectives of the study were to assess: 1) symptoms of depression, anxiety, and stress among nurses and midwives; 2) the proportions of nurses and midwives with depression, anxiety, and stress evaluated by DASS-21; and 3) factors significantly associated with higher levels of DASS-21 sub-scale scores (Depression, Anxiety, and Stress).
Methods
This study was based on a quantitative design and an anonymous self-administered cross-sectional survey was carried out among nurses and midwives employed at a large university hospital in Denmark at one time point. This study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 22
Setting
Nurses and midwives in the survey were recruited from a large university hospital in Denmark with 1100 beds and 100,000 discharges a year, covering most medical specialties. The total number of nurses and midwives employed at the university hospital is approximately 3740.
Denmark has around 5.8 million inhabitants. Healthcare is tax-based and treatment in hospital is free for Danish citizens.
At the time of the study, Denmark had implemented COVID-19 restrictions including restrictions of public and private gatherings and the closure of schools and non-essential workplaces. Danish health services had implemented a number of strategies to protect patients and their staff such as the use of PPE, restrictions on the number of visitors allowed into the hospital, the use of telehealth services, and increasing or reducing non-urgent face-to-face patient appointments. 5
At the study hospital, specific COVID-19 wards were established, and staff were redeployed from other wards and outpatient clinics where activities were reduced. Only the Intensive Care Unit continued to care for both critically ill patients as well as patients with COVID-19.
Recruitment
All nurses and midwives employed at the study health service, including nurse/midwife managers and nurse/midwife researchers, were invited to participate in the study; no exclusion criteria were included. Invitations were sent to nurses and midwives using the hospital's group email address. A reminder was sent two weeks later. The email included the plain language statement and a link to the survey. The survey took approximately 15 minutes to complete.
Data collection
Data were collected using an online anonymous survey hosted on RedCap (an online survey platform) managed by OPEN (Open Patient data Explorative Network), University of Southern Denmark. 23 Data were collected in the period 13 May 2020 to 12 June 2020.
The questionnaire
The questionnaire used in this study was originally developed and tested by a research group from Deakin University in Australia for a similar study about the psychosocial impact of COVID-19 on Australian hospital clinical staff. 9 The questionnaire has been used with consent from the Australian research group and using the principles of backward and forward translation was translated from English into Danish. 24 The questionnaire was based on similar studies about the impact of infectious diseases such as SARS and MERS on health service staff's psychosocial wellbeing.10,25–29 Furthermore, a widely used validated psychometric instrument DASS-21 30 was included in the questionnaire. The DASS-21 is a 21-item validated self-report instrument that assesses symptoms of depression, anxiety, and stress. 30 The scale has been used in a number of different studies, e.g. early life stress and adult emotional experiences.31,32 The translation of the DASS-21 from English to Danish was carried out by Dr Mikael Thastum from the University of Aarhus. 33
In total, the survey included 80 mostly fixed-response questions, and assessed the following five domains:
Sociodemographic and employment characteristics: sex, age, living with school-aged children, occupation, employment status, and years of clinical experience. Health status: general health status (excellent, very good, good, fair, or poor), COVID-19 contact status (no direct contact, contact with people who had COVID-19 resulting in self-isolation and tests, diagnosed with COVID-19, or not known), and psychological wellbeing (the 21-item Depression, Anxiety and Stress Scales [DASS-21]).
30
Scores on each of the DASS-21 subscales range from 0 (no distress) to 21 (most distressed). Clinical cut-off points identified by the instruments’ authors are as follows: depression (mild 5–6, moderate 7–10, severe 11–13, extremely severe 14 or more), anxiety (mild 4–5, moderate 6–7, severe 8–9, 10 or more), and stress (mild 8–9, moderate 10–12, severe 13–16, 17 or more).
30
Concerns about and impact of COVID-19: six items about personal COVID-19 concerns such as the impact on personal and family health (5-point Likert scale; not concerned to extremely concerned), and 15 items on the impact of COVID-19 on work (3-point scale; disagree, neither agree nor disagree, and agree) Health service's response to COVID-19: assessed perceptions about the response of the health service including concern and support for the psychological wellbeing of staff (5-point Likert agreement scale). Free text: respondents were invited to make free-text comments.
Data analysis
Data were analyzed using STATA 16. Descriptive statistics were used to summarize the data. The DASS-21 subscale scores and proportion of respondents scoring in the clinical cut-off ranges were calculated as specified by the instrument's authors 30 in order to identify the number of nurses and midwives who reported ‘normal’, ‘mild’, ‘moderate’, ‘severe’, or ‘extremely severe’ depression, anxiety, or stress by characterizing the degree of distress. One-sample t tests were used to compare DASS-21 scores with scores reported for Danish combat soldiers and military personnel. 34 Cohen's d is reported: small (0.20), medium (0.5), large (0.8), and very large (1.3). 35
Associations between DASS-21 subscale scores and sociodemographic variables were investigated: employment characteristics, self-rated general health, concerns about and impact of COVID-19 as well as perceptions of the health service's response to COVID-19. DASS-21 subscale scores were all non-normally distributed; therefore, Mann–Whitney U tests, Kruskal–Wallis tests, or Spearman's ρ coefficients were used. The Bonferroni correction for multiple tests was conducted to adjust for significant values in the post-hoc pairwise comparisons.
Preliminary analyses were conducted before the hierarchical regression models with DASS-21 Depression, Anxiety and Stress subscale scores as outcome variables. All variables included in the model were significantly associated with any of the subscale scores (p < 0.05), and for multicollinearity was not violated. Hierarchical regression models were conducted and included (if significantly associated). Step 1: sociodemographic and employment characteristics, and health status; Step 2: concerns about and impact of COVID-19 on staff (concern scale, six items α = 0.88); Step 3: contact with COVID-19, impact of COVID-19 (impact scale, 15 items α = 0.68), and health service response ratings (seven items, α = 0.83). 9
We planned to do a sub-group analysis to identify differences between nurses and midwives. Unfortunately, this was not possible due to small numbers (midwives) and protection of anonymity.
Free-text comments were analyzed using content (thematic) analysis. 36 All inputs were read repeatedly to obtain an overview of the data. Relevant themes and subthemes were identified. The inputs were coded accordingly to the themes, read again, and coded according to the subthemes. The findings have been used to complement the quantitative data.
Ethical considerations
Completion of the survey was taken as implied consent. The email invitation and participant information sheet included details about the project and what participation involved. Potential participants were informed that it was possible to withdraw from the study at any time until the survey was completed and submitted, without giving a reason. Non-participation would not affect their employment at the hospital. Once completed and submitted, survey responses would be included in the analyses.
All investigations were carried out to a high ethical standard and in accordance with the Helsinki Declaration. All the data and forms were kept according to approval from the Danish Data Protection Agency (20/19028). Only the researchers had access to stored information.
Results
Approximately 3740 nurses and midwifes are employed at the university hospital and 1416 (37.9%) completed a survey. Of the respondents, 26 were excluded due to missing values about their professional role. Hence, 1390 were included in the analyses.
Respondents’ characteristics
The majority of the respondents were nurses (n = 1330, 95.9%). Most respondents were female (n = 1332, 96.2%); the average age was 44.1 years for respondents who were nurses and 42.1 years for those who were midwives. A higher proportion of midwives lived with school-aged children (58.5%) compared to nurses (39.3%). More than half of the nurses and midwives were full-time employees and about one in ten (7.6% and 10.9%, respectively) reported being in a managerial position. The average number of years in clinical practice was 17.5 years for nurses and 14.1 years for midwives (Table 1).
Respondents’ sociodemographic characteristics and self-rated health.

Note. Values are given as n (%) unless otherwise indicated.
Not reported due to low numbers (<5).
Impact of COVID-19 on work
More than 60% of nurses and midwives felt at risk of getting COVID-19 at work and more than one-quarter felt more stress at work because of COVID-19. In addition, almost half stated that they had done tasks that were not part of their usual role and one-quarter reported having to retrain or do training courses in order to undertake a role they normally would not do. More than one-quarter did not feel very ready to care for patients with COVID-19 and a small proportion (12%) had considered resigning because of COVID-19 (Table 2).
The impact of COVID-19 on work.
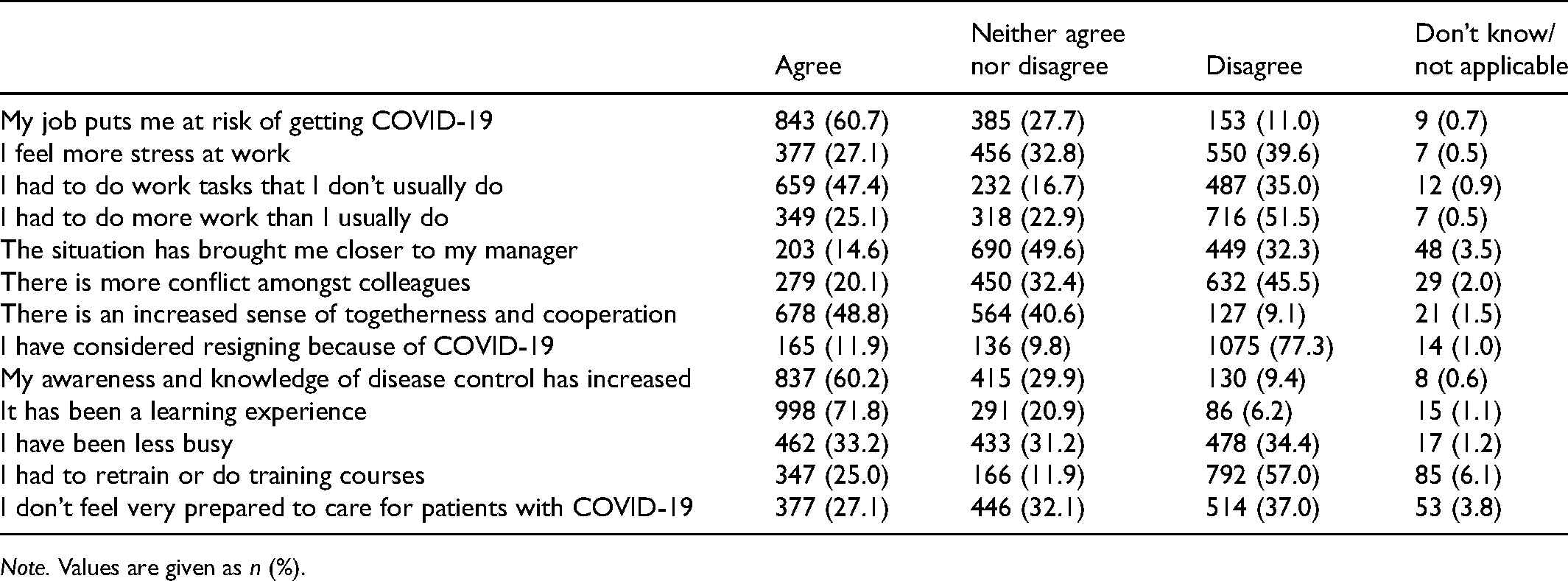
Note. Values are given as n (%).
Psychological wellbeing
The mean DASS-21 Depression subscale score for nurses was statistically significantly lower than the data from the comparison data (combat soldiers), whereas the DASS-21 mean subscale scores for Anxiety and Stress were statistically significantly higher than the comparison data; effect size was negligible for the Depression subscale, and small for Anxiety and Stress subscales. For midwives, there were no significant differences with the comparison data for the Depression and Anxiety mean subscale scores, but the mean Stress subscale score was significantly higher than the comparison data, with medium effect sizes (Table 3). Only 8.9% (n = 124) of nurses and midwives reported mild to extremely severe symptoms of depression; similarly, 9.3% (n = 129) reported mild to extremely severe symptoms of anxiety, whereas 11.5% (n = 160) reported mild to extremely severe levels of stress (Table 3).
Respondents’ scores on the DASS-21.

Lovibond & Lovibond, 1995.
Data on nurses and midwives combined due to the small number of midwives
Crawford, Cayley, Lovibond, Wilson, & Hartley, 2011.
Factors associated with higher DASS-21 subscale scores (Depression, Anxiety, and Stress)
All independent variables were highly significantly associated (p < 0.001) with at least one subscale score and therefore were included in the hierarchical regression models shown in Table 4.
Hierarchical regression models showing factors associated with DASS-21 Depression, Anxiety, and Stress subscale scores.

Note. CI, confidence interval.
More years of experience was significantly associated with lower DASS-21 Depression (p = 0.011), Anxiety (p = 0.006), and Stress scores (p = 0.001); however, these associations were not significant once controlled for all other variables (step 3). Not being in a managerial position was associated with lower DASS-21 Stress score (p = 0.026) when controlled for all variables (step 3). Higher self-rated general health scores were significantly associated with lower DASS-21 Depression, Anxiety, and Stress scores (p < 0.001 for all), and the same was found in higher Concerns scores (less concerned) (p < 0.001 for all) (Table 4).
Having a direct contact with persons who were tested positive for COVID-19 was significantly associated with higher DASS-21 Depression (p = 0.004), Anxiety (p < 0.001), and Stress scores (p = 0.002) when all other variables were controlled for. In addition, higher impact score (agree) was significantly associated with DAS-21 Depression (p < 0.001), Anxiety (p = 0.002), and Stress score (p < 0.001). Finally, higher Health Service Response scores (a positive perceived response) were significantly associated with having lower DASS-21 Depression (p < 0.001), Anxiety (p = 0.003), and Stress scores (p < 0.001) (Table 4). However, step 3 (in all models) did not offer a significant improvement over step 2 for DASS-21 Depression, Anxiety, and Stress scores.
Free-text comments (n = 218) highlighted the impact of COVID-19 on work, especially in relation to information and communication, and the stress factor of the changed work environment. The free-text comments were categorized into five main themes (Table 5):
‘Management and communication at the hospital’ included comments about nurses’/midwives’ need for information and involvement in decisions with respect to COVID-19, and the need for recognition during a difficult time. As one informant commented ‘Communication between management and employees has been poor….’. ‘New clinical practice guidelines’ included respondents’ frustrations about the ongoing change to COVID-19 guidelines, and difficulties in not being able to adhere to the guidelines. One of the informants said: ‘The most frustrating thing is that there have been new guidelines every time I have had time off’. ‘Organizational impact’ included frustrations related to redeployment and one respondent stated ‘It takes mental resources to handle tasks, you are not used to do … and with the risk of making errors’. There were also comments about frustrations with visitor restrictions at the hospital, and increased social and physical distance from colleagues. ‘Social distance from colleagues has affected the work environment’. Conversely, there were also comments about a feeling of increased unity in the hospital ‘… experience of unity across departments’. ‘Personal protective equipment (PPE)’ included frustrations about the lack of protective equipment available at the hospital, especially at the beginning of the pandemic, the importance of well-functioning PPE on a busy day, and frustrations about the extra time required to use PPE as one respondent commented: ‘FFP (filtering face piece) masks affect my ability to do my work, it takes longer time’. ‘Staff's health’ included comments about the psychological impact of COVID-19 on staff including concerns about the impact on colleagues, pregnancy, and the risk of COVID-19, and that access to tests provides a sense of security. One respondent stated: ‘It was a psychological pressure not to know the extent of the pandemic and not knowing if your work plan would suddenly change due to heavy workload, fortunately it is more calm now…’.
Themes and sub-themes of the free-text comments analysis.

Note. PPE, personal protective equipment.
Discussion
This is one of the first studies to examine the psychosocial impact of the COVID-19 pandemic on Danish nurses and midwives. Our findings indicate that most hospital-based nurses and midwives in Denmark did not experience any immediate psychological distress due to the COVID-19 pandemic. However, approximately one in ten nurses and midwives reported mild to severe symptoms of depression, anxiety, or stress, particularly those who had had contact with a someone infected with COVID-19.
Nurses reported significant lower mean DASS-21 Depression scores than comparison data (combat soldiers), whereas the DASS-21 subscales for Anxiety and Stress were statistically significantly higher. For midwives only, the Stress scores was significantly higher than comparison data. However, it is important to acknowledge that the comparison data are derived from a Danish study among elite soldiers; a very highly selected and trained (to emergency situations in warzones) group 34 who may be less likely to experience psychological distress in stressful situations. Unfortunately, no normative data about Danish nurses and midwives either before or during the COVID-19 pandemic are available. Nevertheless, the Danish nurses and midwives in this study had lower mean levels of depression, anxiety, and stress compared to Swedish midwives before the pandemic (5.64, 2.83, and 8.33, respectively).37,38 These populations are estimated to be comparable due to similarities in their healthcare systems. In addition, we found lower DASS-21 scores compared to other studies conducted during the COVID-19 pandemic, including in both Australia 9 and Belgium. 11 However, a study from Singapore also found low mean DASS scores (2.54, 2.45, and 3.82, respectively). 39
In general, the level of psychological wellbeing (WHO-5) in Denmark during the COVID-19 pandemic has been shown to be affected negatively by the COVID-19 pandemic. 40 Furthermore, a systematic review has shown that psychological wellbeing during the COVID-19 pandemic was significantly worse for women, those with poor-self-related health, and those who had relatives with COVID-19. 12 Hence, one explanation for our low mean DASS scores could be high self-rated heath (89.7% rated their health as very good or good, 9.4% as average, and only 0.9% as poor or very poor). Furthermore, the healthcare services’ response could be important to the DASS outcome as well. 39 Denmark is known for having a decentralized and well-functioning healthcare system where all residents are entitled to publicly financed care, which can also be of importance for the outcome of the DASS scores. 41
Despite the relatively low level of psychological distress reported by many respondents in this study, more than one-quarter (27.1%) reported feeling more stress at work during the COVID-19 pandemic. During the pandemic, several areas/wards in the study hospital – such as the outpatient clinics – were closed or reduced and many nurses were redeployed to other areas and cared for patients with COVID-19. Undertaking duties that they would not normally perform or working with unfamiliar colleagues may have been stressful for some of the nurses. Daily routines may have been changed to unknown tasks, and in many places, nurses had to change from face-to-face treatment to, for example, video consultations and still ensure to maintain a high-quality level and at the same time close contact with the patients. Relatives are an important partner in nursing, hence the study (free-text comments) found that the staff missed the relatives in caring for the patients, especially the lack of relationship to patients and relatives. During COVID-19, most relatives had no access to hospitals, and in many situations, nurses had to stand in for them and be the close link to the patient.
The risk of getting sick from COVID-19 and new ways of working have been potentially stressfully for many nurses and emotional reactions are difficult to avoid. A Danish study has described these reactions in three different reaction categories: the ‘devoted’ (those who are motivated by caring for seriously ill patients, and are able to adapt and learn new skills), the ‘concerned’ (those who react with fear, and are concerned about becoming ill themselves or infecting family members, or uncertain of own competences), and the ‘noisemakers’ (those who articulate their concerns about working conditions, salary, rights, lack of tests, and protection equipment; they also dislike the frequent changes to routines and procedures). 42 In particular, the ‘concerned’ could be at risk of subsequent psychological distress due to fear and concerns about becoming infected or infecting their family members. The ‘concerned’ also included those who were uncertain of their own competences. Thus, our study found concerns to be associated with the mean DASS-21 scores. It is important to be aware of the different reactions to be able to assist nurses in the best way in the future.
Consistent with other studies, having contact with and taking care of patients with COVID-19 was significantly associated with DASS-21 Anxiety and Stress subscale scores. A recent Australian study found that hospital clinical staff who had had direct contact with patients with COVID-19 had significantly higher DASS-21 Anxiety subscale scores than staff who had not had contact. 9 In a Portuguese study on COVID-19, nurses’ concerns about being infected and infecting their family or friends were associated with higher levels of depression, anxiety, and stress. 43 Furthermore, these findings are consistent with those from a Canadian study conducted during the 2003 SARS outbreak that reported that healthcare workers’ fears of infection and infecting family, friends, and colleagues led to anxiety, frustration, and anger. 44 Worries about becoming infected and infecting family members are also reported.44,45
Positive perceptions of the health service's COVID-19 response, including communication and support initiatives, appear to be associated with better mental health. The nurses and midwives in this study generally felt that their health service had reacted well to the pandemic in relation to the availability of PPE and communication. However, many of the free-text comments indicate that some nurses and midwives were concerned that PPE was not provided quickly enough and was annoying to wear and time-consuming to put on. In addition, many of the free-text comments suggest that some staff felt that it would have been beneficial if communication had been distributed more quickly and was more accurate.
It is important to note that the psychological consequences can be delayed. Nurses and midwives may be focused on provision of care during the crisis, but nurses and midwives may experience depression and anxiety once the pandemic is over.
Limitations
The cross-sectional observational study design used in this study does not enable causal relationships to be determined. However, the findings improve understanding of the impact of the COVID-19 pandemic on nurses and midwives at a particular point in time.
The response rate was good given the critical situation for nurses and midwives working at a busy hospital during the pandemic and is consistent or higher compared to the response rate for similar studies performed during pandemics. 9 The use of nurses’ and midwives’ work email addresses enabled potential participants to be contacted quickly and easily. However, we were not able to compare groups due to a low response among midwives and the just claim of anonymity. It is a limitation as the psychosocial impact might differ between the groups due to different workload and task. Furthermore, it is possible that the nurses and midwives who experienced more psychological distress during the pandemic did not participate in the study due to a lack of time and mental energy and this could potentially underestimate the psychological impact of COVID-19 on Danish nurses and midwives.
The use of a validated instrument (the DASS-21) to assess symptoms of depression, anxiety, and stress in the past week is a strength of this study. The instrument has been used in several studies with respect to a pandemic in international settings.9,11,39,45–47
The data collection was performed in a hospital setting, which may be a limitation to generalizability to other areas. Furthermore, levels of depression, anxiety, and stress evaluated by the DASS-21 in this sample before the pandemic are unknown, and the cross-sectional design does not give the opportunity to evaluate psychological wellbeing over time.
Implications for future health service practice
It is important to take these findings into consideration for future strategies with respect to pandemics. Even though the COVID-19 pandemic will come under control due to mutations and vaccine efforts among other things, it will be important to keep the lessons learnt for future strategies towards pandemics. In this study, we have crossed the acute phase, and despite relatively low levels of mild to extremely severe symptoms of depression, anxiety, and stress among nurses and midwives, it appears that supportive wellbeing initiatives would be of benefit. The findings will be used to inform health service responses to the current COVID-19 pandemic in order to prevent a negative psychosocial impact among nurses and midwifes. The COVID-19 pandemic has had a major impact on healthcare with the risk of long-term consequences. Hence, it will probably be important to focus on psychosocial impact years ahead of the pandemic. Furthermore, we need future research on the effect of intervention concerning mental and physical wellbeing among hospital staff including longitudinal cohort studies about nurses’ and midwives’ wellbeing to determine the long-term effects of pandemic.
Conclusion
Although most nurses and midwives do not appear to have experienced any immediate psychological distress during the COVID-19 pandemic in Denmark, a small proportion, particularly those who had direct contact with people who had a diagnosis of COVID-19, did report symptoms of depression, anxiety, and stress. The findings suggest that nurses and midwives would benefit from support and wellbeing initiatives focused on their concerns and needs, and clear communication about the risks of COVID-19 and caring for patients who have been diagnosed with COVID-19.
Footnotes
Author contributions
MMS, MJR, and BR analyzed and interpreted the data from the questionnaire. MMS and MJR were major contributors in writing the manuscript. MJR, SH, and KW performed all statistical analysis. SH and KW were major contributors in language proof-reading. All authors read and approved the final manuscript.
Acknowledgments
The authors thank all nurses and midwives who participated in the study; electronic data were managed and stored by OPEN (Open Patient data Explorative Network), University of Southern Denmark, accessible only to the researchers; and Frederik Kristensen and Camilla Stryhn, CIMT, Odense University Hospital for help with the questionnaire.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.