
Abstract
Background:
The construction industry, known for its high-risk environment, increasingly acknowledges the psychological risks to workers. Despite well-documented physical hazards, mental health challenges within this workforce have garnered attention. This systematic review provides a scholarly synthesis of literature on psychological risks and their causative factors affecting construction workers, adhering to PRISMA protocols.
Methods:
An exhaustive literature search was conducted across PubMed, Scopus, PsycINFO, and Google Scholar using relevant keywords. Rigorous screening of selected studies focused on the psychological aspects of construction work, with systematic data extraction and analysis.
Findings:
From 1992 to 2022, 68 studies met inclusion criteria, identifying key psychological harm factors: job insecurity, long working hours, high demands, poor work-life balance, and workplace bullying. A lack of mental health support and awareness in the sector was noted, with a significant correlation between these factors and increased stress, anxiety, and depression levels among workers.
Conclusions:
The review highlights the urgent need for industry recognition of psychological hazards and the relationship between work conditions and mental health issues. It calls for supportive policies, awareness programs, and counseling services, with a suggestion for future longitudinal research on the long-term impacts and intervention efficacy.
Application to Practice:
This study provides an overview of psychological risks in the construction sector from 1994 to 2022, aiming to identify causative factors for mental health issues. It seeks to pave the way for targeted interventions and policy changes to improve mental health outcomes in the industry.
Background
Construction workers often operate in stressful environments with intense job demands, long working hours, precarious job security, and physically challenging work conditions (Sommovigo et al., 2021; M. Turner & Lingard, 2016). This contributes to a high risk of psychological harm, including stress, anxiety, depression, and in severe cases, suicidal ideation (Langdon & Sawang, 2018; Ross et al., 2021; Windsor-Shellard & Gunnell, 2019). Recently, there has been a growing focus on comprehending and addressing the physical health hazards associated with construction work (Sousa et al., 2014). Understanding the causative factors and risks associated with psychological harm of construction workers is critical for designing effective mental health interventions and improving workers’ wellbeing (Westerhof & Keyes, 2010).
In Australia, recent changes have been made to the model work health and safety (WHS) laws, which now include regulations on psychosocial hazards (Boland, 2019). Psychosocial hazards in the workplace are defined as anything that could cause psychological harm, such as affecting someone’s mental health (Safe Work Australia [SWA], 2022). Researchers revealed and reflected a growing awareness of the significance of psychological hazards and injuries in the workplace and aim to provide better guidance to workers and employers on managing the risk of psychological injuries and illnesses (Sun et al., 2022).
The impact of substance use, particularly alcohol among construction workers, is another notable concern, significantly contributing to mental health issues and occupational fatalities (Shockey & Esser, 2020; Stahre et al., 2014), however, the link between job-related stressors and substance use is not well-understood. Many studies have implied a relationship between safety behavior and job stress in construction workers (Ross et al., 2022; Sunindijo & Zou, 2012; Wu et al., 2018), which may indirectly influence their psychological wellbeing. This systematic review aims to comprehensively review existing literature, within the construction industry to our understanding of mental health challenges to examine the causative factors and risk of psychological harm among workers in construction. By drawing upon a broad range of scholarly works and utilizing the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews methodology (Tricco et al., 2018).
The question driving this review is how do specific workplace factors within the construction industry contribute to the psychological wellbeing of its workers, and what evidence-based interventions can effectively mitigate these psychological risks? Answers to this question align with the World Health Organization’s call for a coordinated, comprehensive response from social sectors and health to address the global burden of mental disorders (Funk et al., 2010; World Health Organization [WHO], 2011). Further, it paves the way toward creating healthier workplaces and improving the quality of life among workers in construction (Zabeer et al., 2019). For the purposes of this review, Employees, project-based hires, and day laborers were all considered as worker categories. Additionally, the review encompassed licensed professionals with formal recognition and specialized expertise, typically aligned with legal and regulatory standards, as well as skilled laborers possessing broader, albeit less formalized, expertise.
Methods
The execution of this systematic review took place over a span of 8 months in 2023, from February to September. This was achieved by closely adhering to the protocols and guidelines outlined in the PRISMA checklist (Moher et al., 2015; Page et al., 2021; Panic et al., 2013; Tricco et al., 2018). To gather the pertinent research publications, we turned to international databases such as Scopus, Web of Science, ScienceDirect, Google Scholar, Medline/PubMed, and ProQuest. The investigation was guided by specific keywords that fell into three categories mentioned in the Table 1 below:
Keywords Used in Investigating Psychological Wellbeing and Harm Among Construction Workers
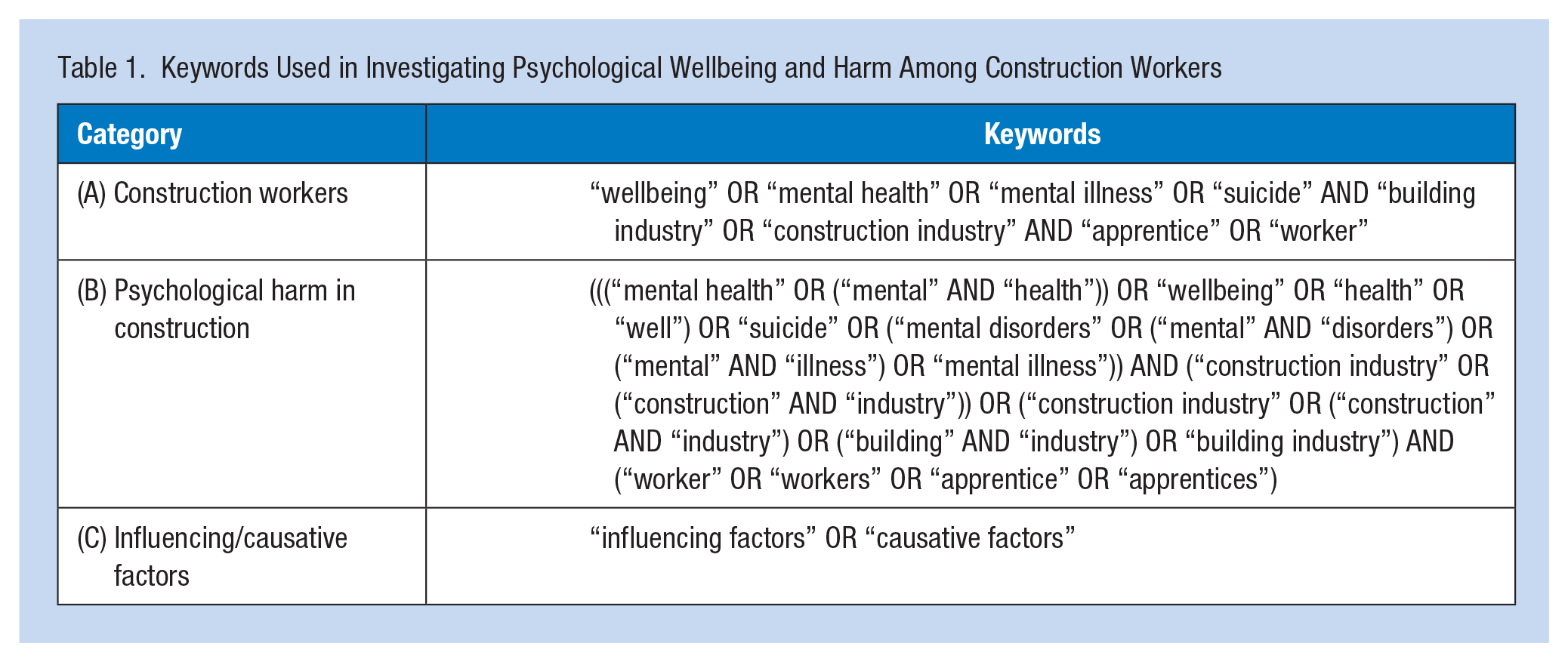
The database search strategy was based on the Boolean approach that combined these different sets of keywords (Scells et al., 2020). After the completion of the search process, a comprehensive list of all research studies, including the authors, year of publication, and titles, was assembled. This was followed by a rigorous screening process to weed out duplicate entries, and to remove any articles that were deemed irrelevant or not directly related to the topic of interest.
Eligibility Criteria: Inclusion
To maintain the novelty and uniqueness of our systematic review we have established the following inclusion criteria for studies:
• Only peer-reviewed studies published in English were included.
• Study participants were construction workers, embracing a variety of roles within the construction sector.
• Studies that explicitly explored the risk and causative factors contributing to psychological harm among construction workers, encompassing aspects such as stress, job dissatisfaction, and mental health outcomes.
• Publication date ranges from 1991 to July 2021.
• Studies using principles of occupational psychology, occupational health, or related fields to evaluate the psychological harm experienced by construction workers.
• Epidemiological studies of construction workers (e.g., case-control, cross-sectional, cohort studies, or specific case studies), which explore the relationship between risk factors and psychological harm.
Eligibility Criteria: Exclusion
To preserve the distinctiveness of our systematic review, we excluded studies based on the following criteria:
• Studies that failed to specify a clear study population or possess an overly broad focus and scope
• Non-scientific publications, such as editorials or commentaries
• Studies that primarily focused on pain treatment, and cadaver studies
• Review articles or literature reviews without new empirical data
This strategy ensured the credibility and validity of our research while providing fresh perspectives on the risk and causative factors of psychological harm among construction workers.
Methodological Quality
To evaluate the research quality of the various study designs we utilized four different assessment tools. These studies were assessed based on nine elements covering selection, comparability, and outcomes, as per Stang (2010) as presented in Table 2. For cohort studies, we followed Wells et al. (2014) as depicted in Table 3. For case studies, the evaluation was based on Murad et al. (2018) as displayed in Table 4. Longitudinal studies were evaluated based on Murad et al. (2018) as presented in Table 5. Details covered during the data abstraction phase, from all reviewed articles are presented in Table 6.
Methodological Quality Scores of Case-Control Studies as per Newcastle-Ottawa Scale as Per Stang (2010)
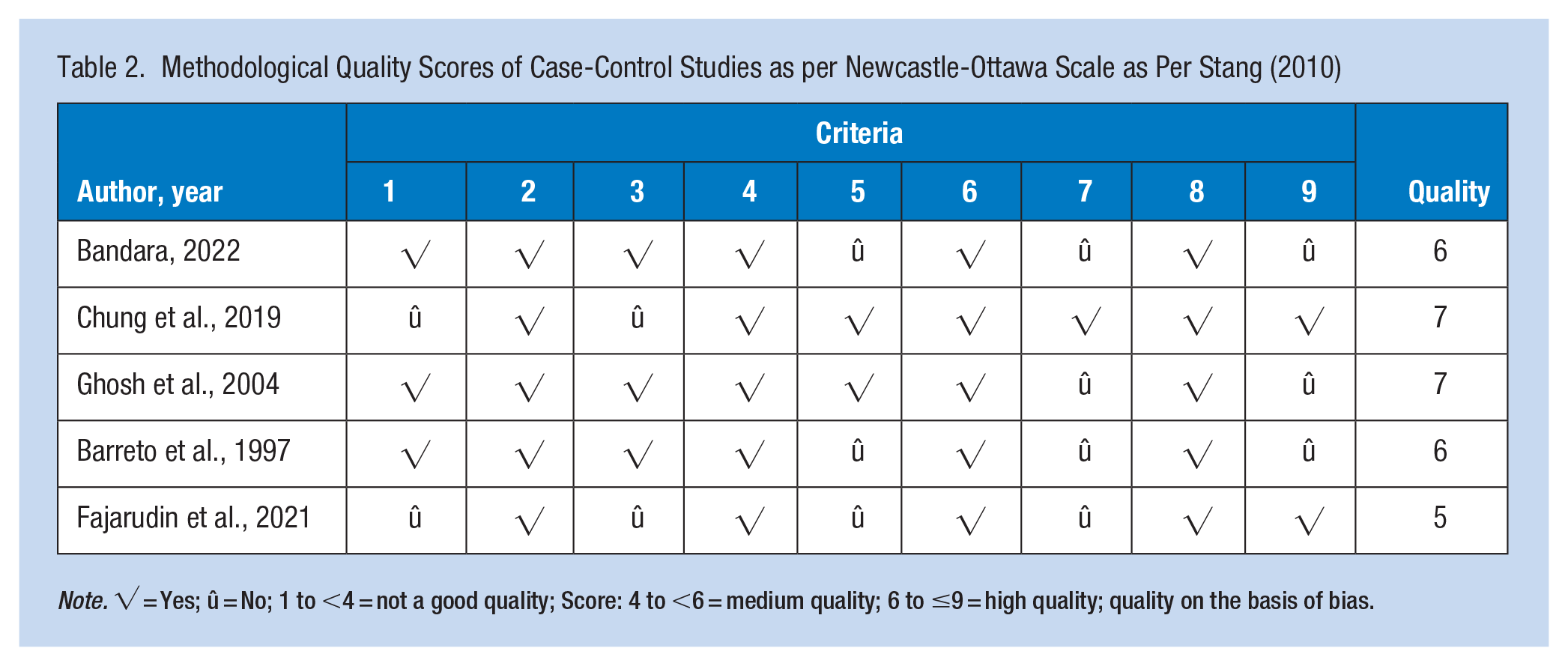
Note. √ = Yes; û = No; 1 to <4 = not a good quality; Score: 4 to <6 = medium quality; 6 to ≤9 = high quality; quality on the basis of bias.
Methodological Quality Scores of Cohort Studies (Newcastle-Ottawa Scale) as per Wells et al. (2014)
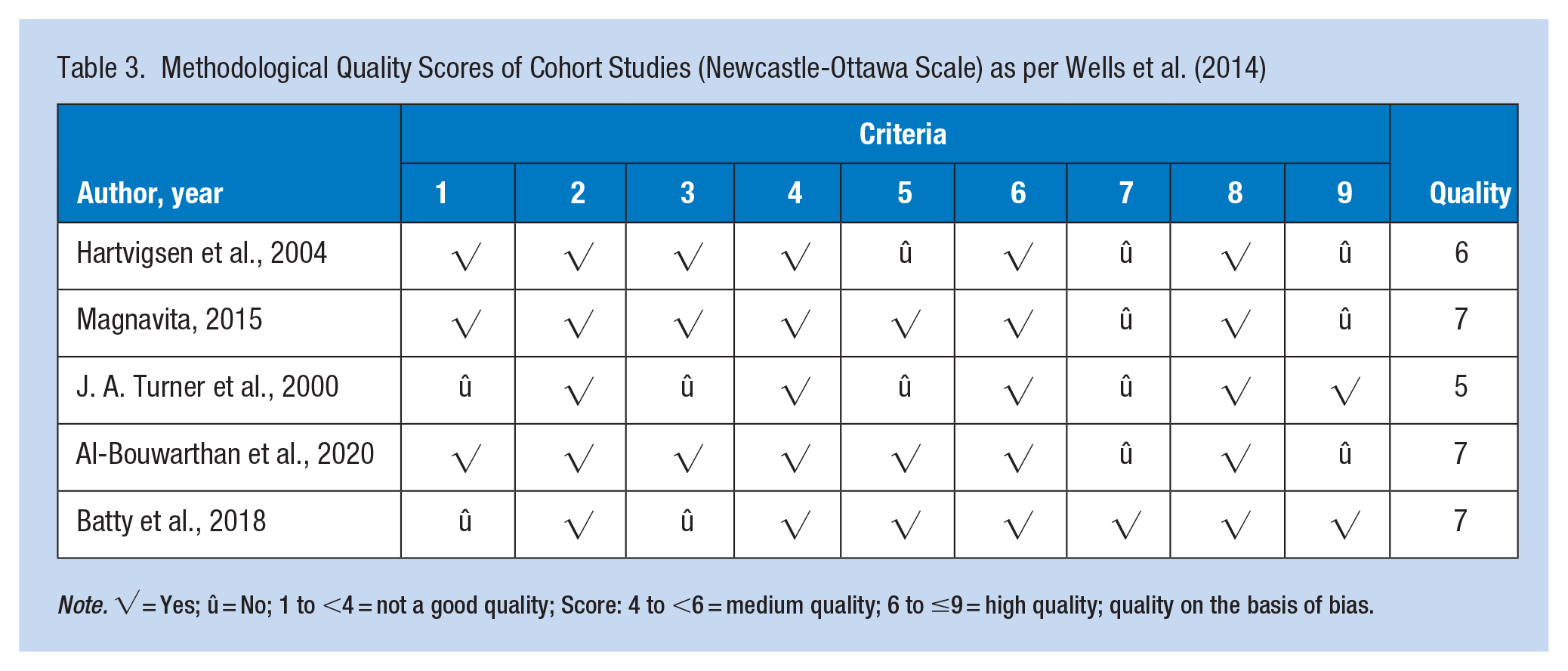
Note. √ = Yes; û = No; 1 to <4 = not a good quality; Score: 4 to <6 = medium quality; 6 to ≤9 = high quality; quality on the basis of bias.
Methodological Quality Scores of Case Studies as per Murad et al. (2018)
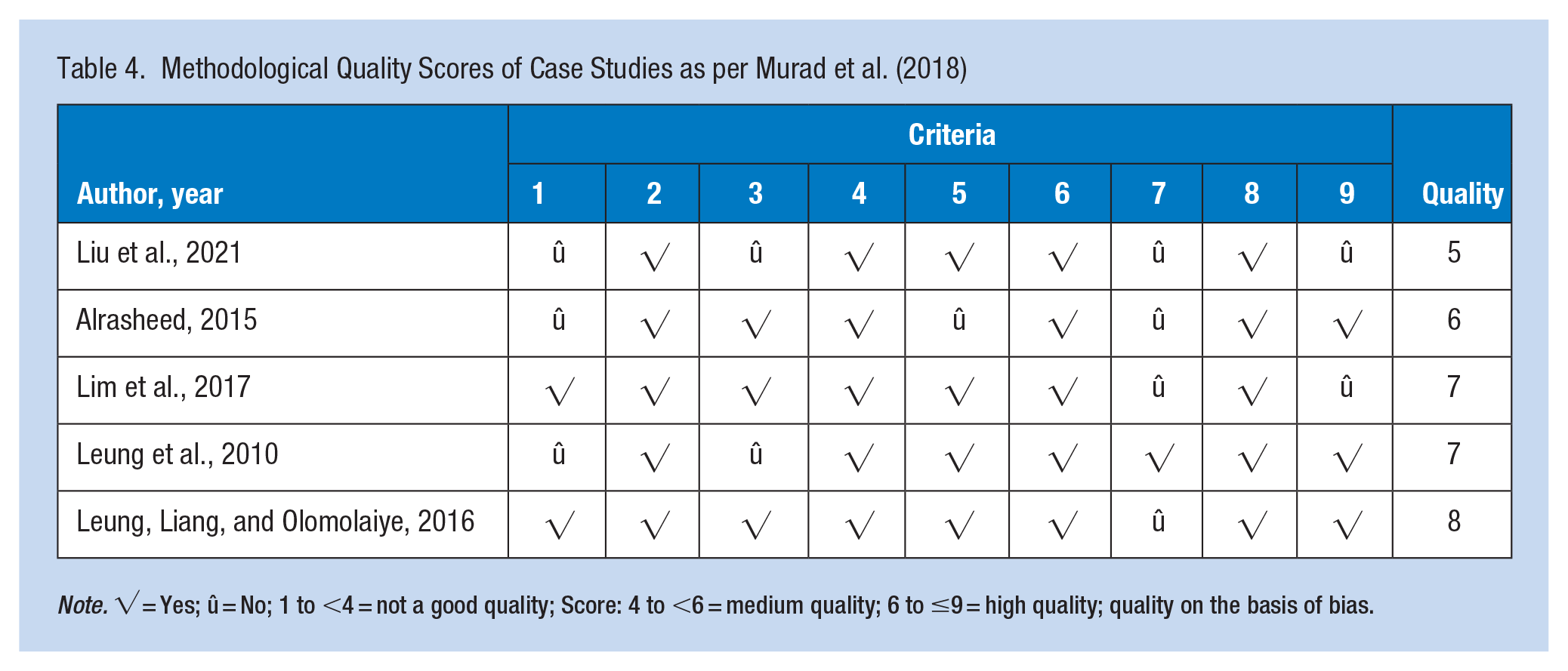
Note. √ = Yes; û = No; 1 to <4 = not a good quality; Score: 4 to <6 = medium quality; 6 to ≤9 = high quality; quality on the basis of bias.
Methodological Quality Scores of Longitudinal Studies as per Murad et al. (2018)
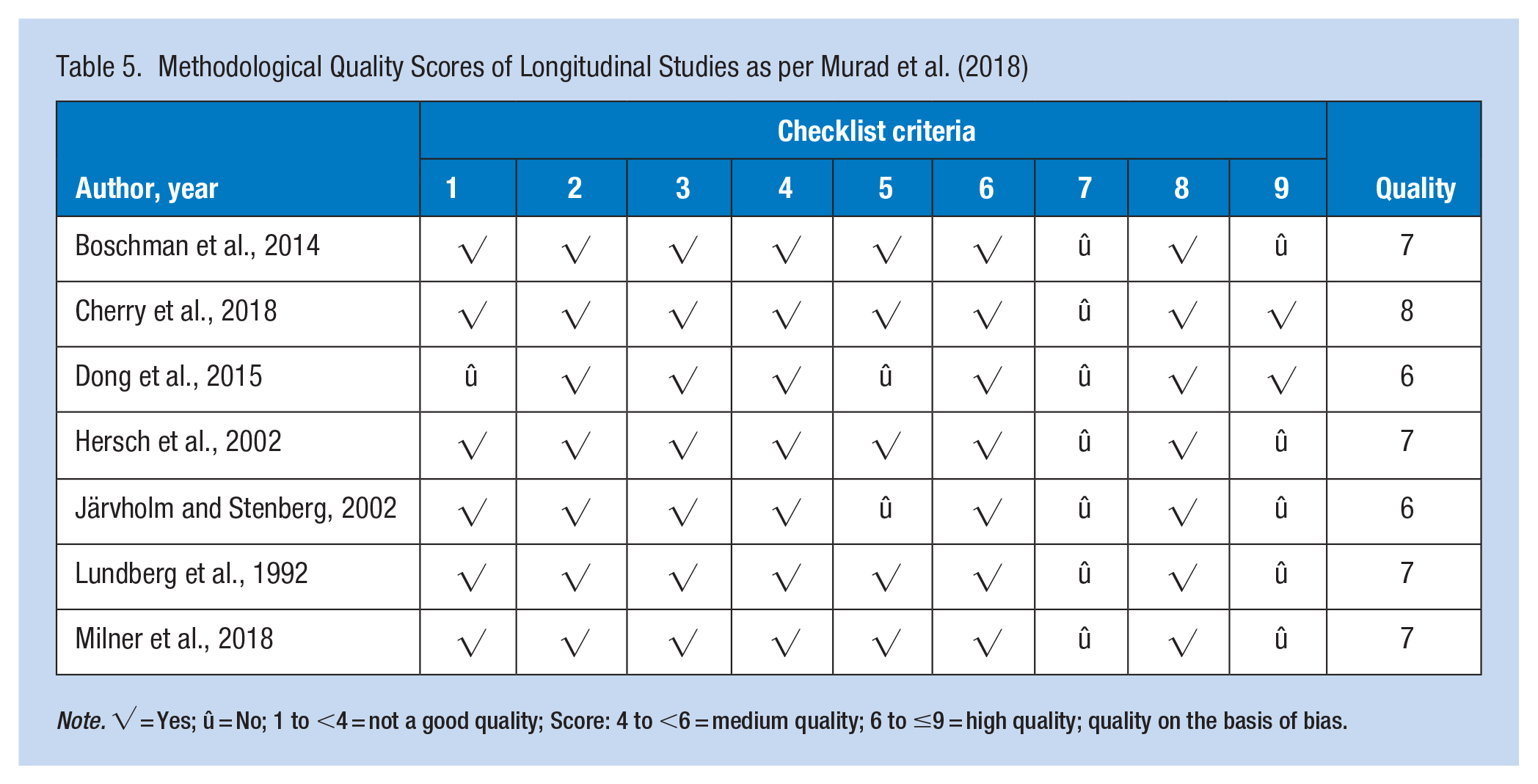
Note. √ = Yes; û = No; 1 to <4 = not a good quality; Score: 4 to <6 = medium quality; 6 to ≤9 = high quality; quality on the basis of bias.
Study Summary; Author, Year, Country, Study Type, and Factors Influencing Psychological Harm
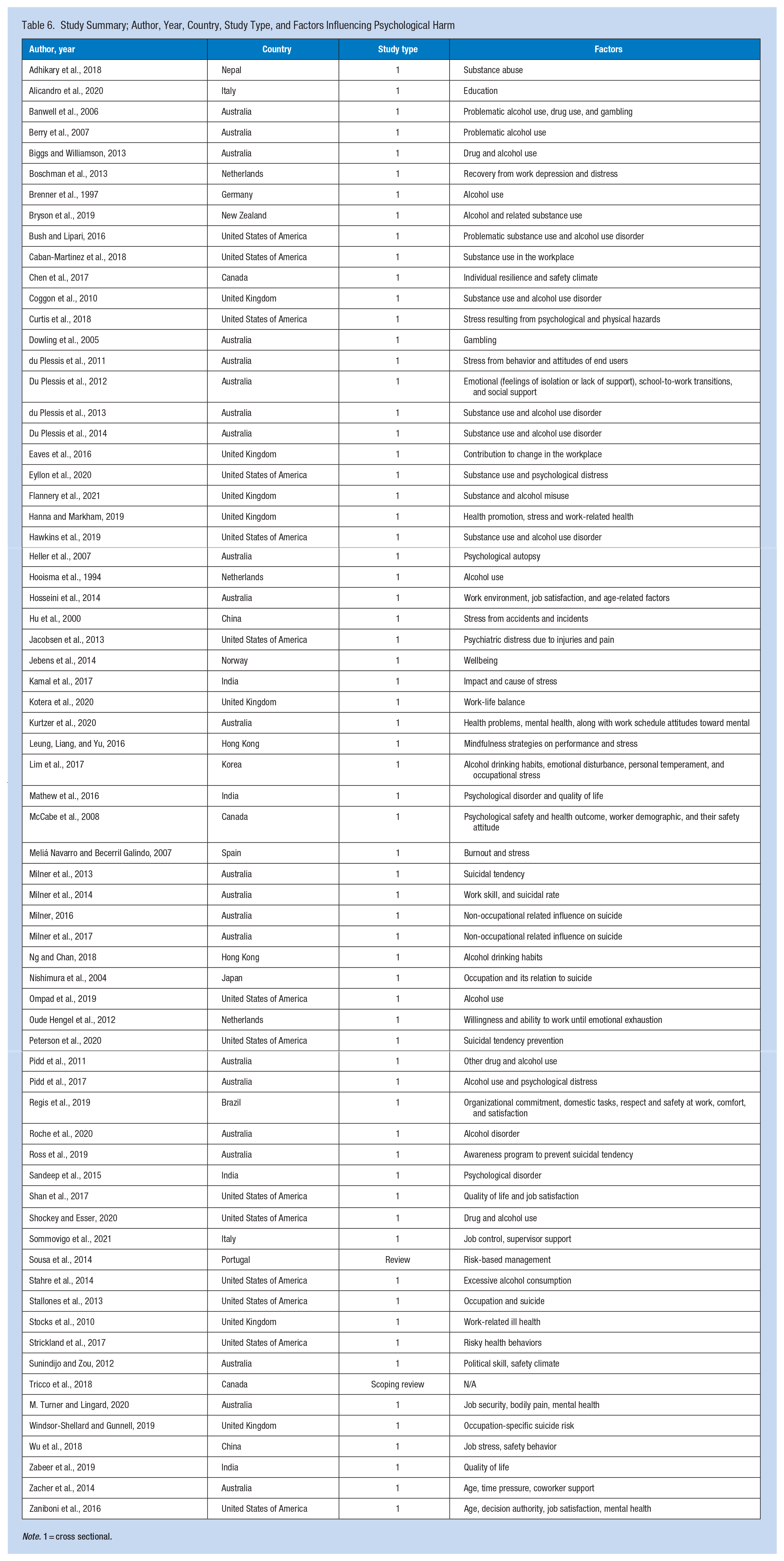
Note. 1 = cross sectional.
Results
Description of the Search for Studies
The search for studies pertaining to psychological harm and its risk and causative factors among construction workers involved an extensive exploration of multiple scientific databases. The chosen databases were PubMed, PsycINFO, Scopus, Web of Science, and Google Scholar. The search strings were adapted according to the requirements of each database. In order to ensure comprehensive coverage, the reference lists of all included studies were manually checked for additional potentially relevant articles. Peer-reviewed articles were preferred, but grey literature, including theses, dissertations, and reports, were not outright excluded during the initial search.
Initial screening involved reading the title and abstract of the retrieved articles to check for relevance to the topic of psychological harm in construction workers. Studies not related to this were immediately excluded. Full texts of the remaining articles were retrieved and assessed for eligibility based on predetermined inclusion and exclusion criteria. These included criteria pertaining to the population (construction workers), outcome (psychological harm or mental health issues), and study design (qualitative, quantitative, or mixed-method studies). Studies not directly addressing these criteria deemed to be of poor methodological quality, as assessed by Hoy et al. (2012) were excluded. All included studies underwent a detailed data extraction process, with pertinent information such as author(s), year, country, study design, sample size, key findings, and quality assessment outcomes recorded for further analysis. This systematic review was designed and executed in accordance with the PRISMA checklist (Figure 1).
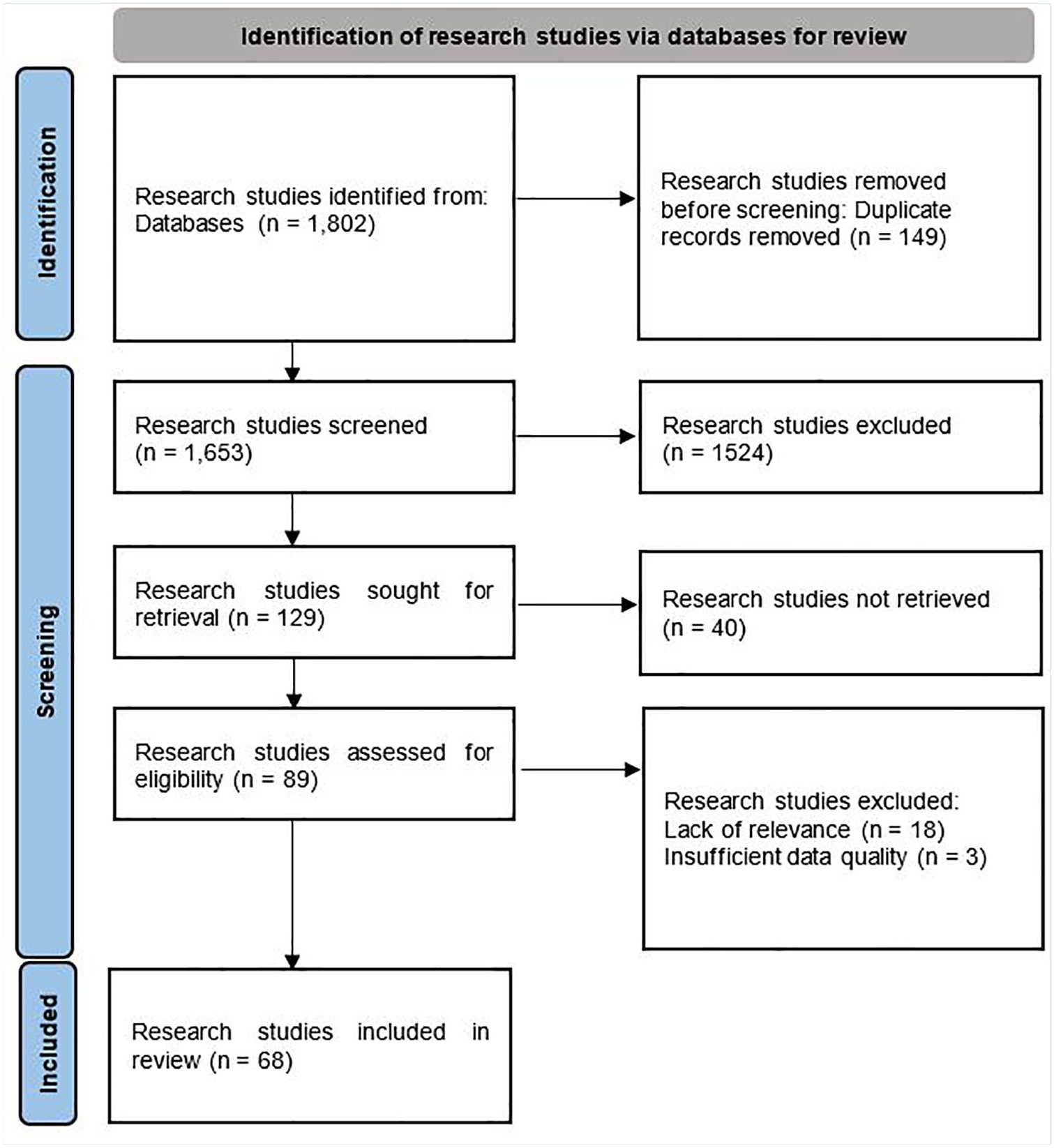
PRISMA flow diagram representing the systematic review selection process
Throughout this study process, any disagreements regarding study inclusion or methodological quality were resolved by consensus or the input of a third reviewer. This rigorous and systematic approach aimed to minimize bias and ensure the credibility and reliability of this study’s findings.
Quality of the Article Reviewed
We evaluated articles on a set of standards concerning potential risks to the reliability and applicability of longitudinal observational research. The checklist criteria concerned with the following (1) recruitment, (2) generalizability (3) data collection, (4) study population, (5) biases, (6) study rationale, (7) descriptive issues, (8) data Integrity, and (9) data analysis. An overview of the evaluated articles on a set of standards is presented in Table 7.
Methodological Quality Scores of Cross-Sectional Studies as per Hoy et al. (2012)
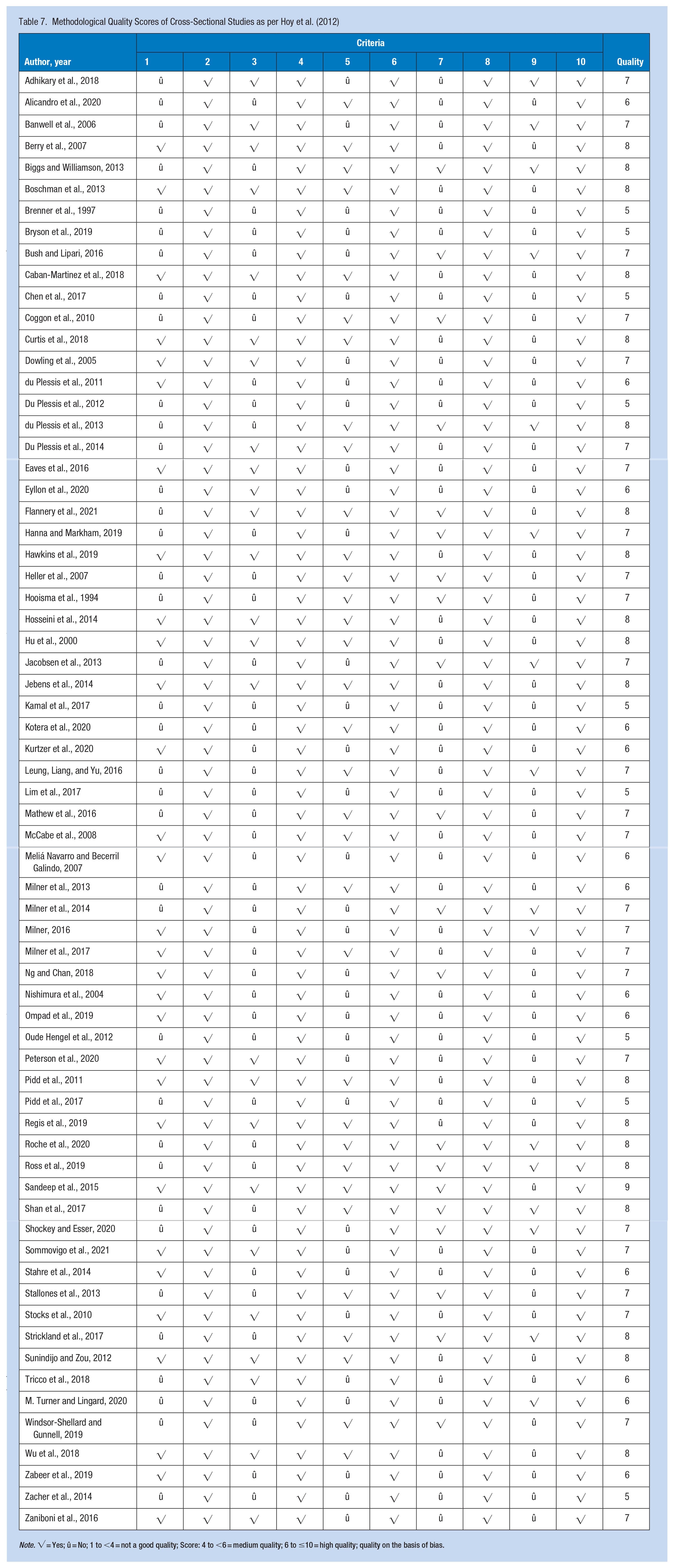
Note. √ = Yes; û = No; 1 to <4 = not a good quality; Score: 4 to <6 = medium quality; 6 to ≤10 = high quality; quality on the basis of bias.
Study Characteristics
The literature selected for analysis comprehensively illuminate psychological harm in construction workers and highlight various causative factors. Several studies associate high-risk behaviors like excessive alcohol consumption and drug use with mental health issues and suicide among construction workers (Shockey & Esser, 2020; Stahre et al., 2014; Wilcox et al., 2004; Windsor-Shellard & Gunnell, 2019). In contrast, the role of socio-occupational aspects, such as job control, supervisor support, job security, and co-worker support, has been elucidated in the context of worker wellbeing (Sommovigo et al., 2021; M. Turner & Lingard, 2016; Zacher et al., 2014).
Several studies examined the interplay between physical and mental health. For example, M. Turner and Lingard (2020) investigate the interaction between bodily pain and mental health, while Stocks et al. (2010) address work-related ill health. Research offers theoretical perspectives on mental health and wellbeing across the lifespan (Westerhof & Keyes, 2010), while also pointing toward the quality of life and wellbeing of migrant workers (Zabeer et al., 2019). The impact of stress has been highlighted in the context of job stress and safety behavior (Wu et al., 2018), while Sousa et al. (2014) underscore the importance of risk-based management in the construction industry. These studies reveal the interplay of individual, occupational, and socio-cultural factors contributing to the psychological harm of construction workers. While the current review offers a broad understanding, it is evident that further in-depth, context-specific research is required.
Limitations in the data exist due to the absence of detailed methodologies and specific sample sizes. Therefore, it is crucial for future research to ensure rigorous and comprehensive methodological approaches. This study also implies the need for interventions that address socio-occupational and cultural factors to improve mental health and wellbeing among construction workers. This is crucial for reducing work-related stress and improving safety, as these environments are often high-stress and high-risk. By focusing on factors like job security, work-life balance, and reducing the stigma associated with poor mental health, the industry can significantly enhance the mental wellbeing of its workers (Table 6).
Discussion
Mental Health Issues and Suicidal Tendencies in the Construction Industry
Mental health in the construction industry is an under-researched but significant concern. Construction workers often experience high levels of stress, job dissatisfaction, and adverse mental health outcomes due to the unique and challenging nature of their work environment (M. Turner & Lingard, 2016, 2020). Notably, the construction industry is characterized by high physical demands, variable working hours, job insecurity, limited control over tasks (Sousa et al., 2014) and has a frequently changing work environment (Lingard et al., 2012). Several studies highlighted the role of job stress in the construction industry, with adverse impacts on worker safety behavior and overall mental wellbeing (Strickland et al., 2017; Wu et al., 2018). Stress occurs from many sources, such as high workloads, tight deadlines, and physical strain from the labor-intensive work. Several studies, such as those by Kamal et al. (2017), and Meliá Navarro and Becerril Galindo (2007), highlighted the role of stress as a significant cause of poor mental wellbeing.
Many studies highlighted high rates of alcohol and drug use within this workforce (Banwell et al., 2006; Berry et al., 2007; Biggs & Williamson, 2013; Burns & Teesson, 2002). Substance abuse, as stated by Biggs and Williamson (2013), Chapman et al. (2021), and Bush and Lipari (2016), is particularly prevalent in the construction industry. The construction industry has the second-highest rate of heavy alcohol use and substance use disorders (Bush & Lipari, 2016). Similarly, Chapman et al. (2021) reported patterns of illicit drug use in construction workers which can potentially be a coping mechanism for stress or mental health issues. Mental health problems are often exacerbated by substance use disorders, including alcohol and drug abuse leading to a higher risk of death (Shockey & Esser, 2020; Stallones et al., 2013; Wilcox et al., 2004). For example, Hawkins et al. (2019) showed a link between opioid-related overdose deaths and construction industry occupations. In numerous countries globally, drug testing is generally incorporated into a detailed health and safety policy, which is often included in employment contracts or staff handbooks. Employers are advised to restrict testing to essential situations, carry out tests on a random basis, and refrain from targeting individual employees unless their job responsibilities warrant it. In Australia, some companies have policies to test their workers for alcohol and illicit substances, particularly if a worker could kill or seriously injure themselves or someone else (SWA, 2022).
Suicide rates in the construction industry are a growing concern. According to Bachmann (2018) and Bryson et al. (2019), the risk of suicide is high compared to other sectors across different countries (Stallones et al., 2013; Windsor-Shellard & Gunnell, 2019). Construction workers have a suicide rate of 53.2 per 100,000, which is the second-highest suicide rate across all industries in the US and higher than in any other occupation in the United States. Often combined with mental health disorders. There is also a considerable body of research, suggesting a link between occupation in the construction industry and suicide such as Heller et al. (2007), Järvholm and Stenberg (2002), Milner (2016), and Milner et al. (2017, 2018).
Another factor that may be associated with poor mental health and higher suicide rates is the mental health stigma that seems to be prevalent in the construction industry. Eyllon et al. (2020) found that the fear of stigma could deter construction workers from seeking mental health support. The macho culture within the industry may perpetuate this stigma. Moreover, the culture of masculinity and stigmatization of mental health issues can contribute to worsening psychological health and discourage seeking help (Milner, 2016; Milner et al., 2013, 2014, 2017, 2018). leading to untreated mental health problems which could potentially increase the risk of suicide (Eyllon et al. (2020).
Factors Contributing to Reduced Psychological Wellbeing
Several factors in the construction industry could potentially harm the psychological wellbeing of construction workers. Key factors of concern are listed below:
Work-related Stress: Several studies listed, such Kamal et al. (2017), and Meliá Navarro and Becerril Galindo (2007), highlight the role of work-related stress as a significant factor.
Work-life Balance: Kotera et al. (2020) suggest that maintaining a healthy work-life balance is critical for construction workers. Long working hours, irregular schedules, and physical demands can leave workers with little time or energy for personal or family life, leading to potential psychological harm.
Unsafe Conditions: The construction industry is notorious for its high rate of workplace accidents and injuries. McCabe et al. (2008) suggest that unsafe conditions and fear of injury can lead to increased anxiety and stress among construction workers.
Job Insecurity: Many construction jobs are project-based or contractual, leading to job insecurity. Leung, Liang, and Olomolaiye (2016) discuss how this lack of job security can contribute to stress and negatively impact mental health. Those involved in project-based work report poorer health outcomes (M. Turner & Lingard, 2016). Insecurity of employment may lead to chronic job stress, contributing to adverse mental health outcomes and perpetuating a cycle of stress and mental health problems.
For a more complete understanding and analysis, the full content of the articles should be reviewed.
Demographic Factors and Health
Construction workers’ psychological health is significantly impacted by demographic factors, such as age, job roles, and migrant status. Age is a noteworthy factor in the context of mental health in construction. It is suggested that age and occupational wellbeing have a curvilinear relationship, which is mediated by time pressure and coworker support (Zacher et al., 2014). Furthermore, older workers may experience decreased decision-making authority, which negatively impacts job satisfaction and mental health (Zaniboni et al., 2016). This highlights the necessity to provide age-specific support within the construction industry. Job roles within the construction industry can also influence mental health outcomes. Research has pointed out that certain occupation groups within the industry may be more prone to risky behaviors such as binge drinking (Shockey & Esser, 2020), which can exacerbate psychological stress and elevate the risk for mental health disorders.
The migrant status is another vital demographic factor. Migrant construction workers face often challenges such as language barriers and lack of social support, thereby compromising their quality of life and mental wellbeing (Zabeer et al., 2019). Furthermore, migrant construction workers often face challenging living and working conditions, including isolation from families, social exclusion, and cultural differences. These circumstances have been shown to negatively impact their quality of life (Zabeer et al., 2019), which can in turn harm their psychological wellbeing. Migrant workers often report higher levels of stress and mental health problems compared to non-migrant workers, which have been shown to negatively impact their quality of life (Zabeer et al., 2019) and can also harm their psychological wellbeing. Moreover, they have often limited access to healthcare services, which collectively undermines their mental wellbeing (Zabeer et al., 2019).
In summary, demographic characteristics of construction workers, such as age, and migrant status significantly affect their psychological wellbeing. These factors should be considered when designing mental health interventions and preventative measures for construction workers.
Psychological Factors
The construction industry, despite its economic significance, is associated with several stressors that can significantly impact the psychological wellbeing of construction workers. Hanna and Markham (2019) pointed out structural constraints in promoting health and wellbeing within the UK construction industry, suggesting a potential systemic issue that affects workers’ mental health. Similarly, Jacobsen et al. (2013) concluded that a high prevalence of mental distress among construction workers was associated with their pain and injuries, pointing to the psychological impact of the physical hardships endured by workers in this industry. Moreover, the construction industry is characterized by a high-risk work environment that can lead to traumatic experiences, which may affect the mental health of workers. Hu et al. (2000) noted posttraumatic stress disorder among co-workers following exposure to a fatal construction accident in China, indicating how workers can be affected by accidents involving colleagues.
Social support or lack thereof at work can significantly influence workers’ mental health (Love et al., 2010) as well as job satisfaction. Social support is “the perception or experience that one is loved and cared for by others, esteemed and valued, and part of a social network of mutual assistance and obligations” (Taylor, 2011, p. 189). Hosseini et al. (2014) and Jebens et al. (2014) discuss the relationship between job satisfaction, work conditions, and the overall mental wellbeing of construction workers and highlight that factors associated with job satisfaction can significantly impact their psychological health (Hosseini et al., 2014).
Lastly, difficulty in maintaining work-life balance can also impact mental health. Mostert et al. (2011) discuss how work-home interference in the construction industry can influence worker wellbeing. Negative Work-home interference (WHI), exacerbated by high job demands, contributes to burnout, while positive WHI, supported by job resources, enhances work engagement. This relationship highlights the crucial role of WHI in influencing both stress and motivation among construction workers (Mostert et al., 2011). Overall, the evidence points to several psychological risks associated with the construction industry. Therefore, the need for interventions and support systems, is paramount in protecting and improving the mental health of construction workers.
Implications
The research literature presented herein provides significant implications for both the construction industry and policy makers. These implications fall into several broad categories, including health and safety regulations, workplace interventions, mental health support services, and future research directions. Mental wellbeing, as opposed to merely the absence of mental illness, involves a state of thriving mental health characterized by positive emotions, life satisfaction, and effective functioning in daily life (Westerhof & Keyes, 2010). In the construction industry, achieving and maintaining mental wellbeing is a complex task due to numerous factors intrinsic to the nature of the work. Improving mental wellbeing among construction workers requires a multifaceted approach, encompassing improvements in working conditions, fostering a supportive work environment, offering professional mental health support, and promoting resilience.
Peer support systems can serve as a protective factor against stress and can contribute to the overall mental wellbeing of workers. However, the reliance on peer support should not overshadow the need for formal systems including regular mental health screenings, psychological risk assessments, and the implementation of mental health and wellness programs at the workplace. The regulatory framework needs to acknowledge and address the substantial burden of mental health disorders among construction workers.
The complexity of mental health issues among construction workers underlines the importance of taking a holistic approach when addressing this issue. The workplace itself can be a potent lever for promoting mental health. Acknowledging the interplay of individual, job-related, and social factors is essential to effectively mitigate psychological harm among construction workers (Funk et al., 2010; WHO, 2011; Westerhof & Keyes, 2010). Factors like job control, supervisor support, and job security can greatly impact workers’ psychological wellbeing (Sommovigo et al., 2021; Sunindijo & Zou, 2012; M. Turner & Lingard, 2020). Employers should, therefore, focus on creating supportive work environments that mitigate stress and promote job satisfaction. This can be achieved through practices such as providing more decision-making power to employees, ensuring fair treatment and respect, and implementing measures that enhance job security. Future interventions should aim to improve work conditions and provide comprehensive mental health support and substance abuse counseling to the workers in this industry.
The findings also highlight the need for accessible tailored mental health services including counseling, stress management programs, substance abuse treatment, and suicide prevention initiatives. Given the high prevalence of alcohol and drug use disorders among construction workers (Shockey & Esser, 2020; Wilcox et al., 2004), specialized addiction services should be a core component of these support structures. Research highlights also the importance of mindfulness in stress reduction, which has been shown to be effective in reducing anxiety, depression, and stress (Khoury et al., 2015). Leung, Liang, and Olomolaiye (2016) developed a mindfulness-stress-performance model specifically for construction workers. A tool that has been employed successfully for other occupations (Gold et al., 2010).
There is an urgent need for effective strategies to improve mental health and wellbeing within the construction industry (Broadbent & Papadopoulos, 2014; Campbell & Gunning, 2020). This includes promoting awareness of mental health, providing mental health support services, and creating a culture that encourages open conversations about mental health. Addressing the issue of mental health in the construction industry requires a multi-pronged approach, including providing adequate mental health support, implementing preventive measures, fostering a supportive work culture, reducing the stigma associated with mental health issues and promoting awareness of mental health issues and available resources.
Finally, findings also highlight the need for more comprehensive studies that explore the relationships between various occupational stressors and mental health outcomes among construction workers. For example, understanding the mechanisms through which job stress impacts safety behavior (Wu et al., 2018), or how the interaction between physical pain and mental health influences the workers’ overall wellbeing (M. Turner & Lingard, 2020), can provide valuable insights for creating effective intervention strategies.
In conclusion, the current body of research calls for a multi-pronged approach that combines regulatory action, workplace interventions, specialized mental health services, and further research to address the complex issue of psychological harm among construction workers. Taking these steps will likely have also positive effects on safety, productivity, and retention in the construction industry.
Limitations
Despite this studies’ strengths, several limitations should be acknowledged. First, several studies used a cross-sectional design, which only provides a snapshot in time and cannot establish causality between risk factors and psychological harm (Stallones et al., 2013; Stocks et al., 2010; Strickland et al., 2017). Second, the self-reported nature of many data sources can lead to response bias, which might result in either overestimation or underestimation of certain factors. The use of more objective measurements or triangulation of data sources could help mitigate this limitation (Shockey & Esser, 2020; Wu et al., 2018). Thirdly, numerous studies fail to comprehensively address the concept of intersectionality. This concept involves understanding the intricate and compounded manner in which various forms of discrimination, including racism, sexism, and classism, intertwine and overlap. Factors such as race, gender, socioeconomic status, or migrant status may intersect with occupational exposure, thus modulating the risk and impact of psychological harm (Zabeer et al., 2019). Fourth, research focuses heavily on individual-level factors. Therefore, there is a need for more research that looks at organizational culture, policy, and practices and how they contribute to mental health issues (Sunindijo & Zou, 2012; M. Turner & Lingard, 2016). Lastly, there appears to be a focus on the negative aspects (risks, harm) and less on protective factors or resilience among construction workers. Understanding what helps workers cope with stress and maintain good mental health in this challenging industry could be instrumental for prevention and intervention efforts (Zacher et al., 2014). Considering these limitations, while the existing research provides a solid foundation, future research would benefit from methodological diversity and a broader perspective that includes both risk and protective factors. Furthermore, studies are required to develop comprehensive and inclusive strategies to tackle psychological harm in the construction industry.
Conclusion
This systematic review illustrates the critical state of mental health among construction workers and calls for a coordinated response from social sectors and health to address this significant yet overlooked issue. This review sheds light on the risk and causative factors of psychological harm among construction workers. The construction industry presents unique challenges that can significantly impact mental health and wellbeing. High levels of stress, job dissatisfaction, and adverse mental health outcomes are prevalent in this occupational group, often exacerbated by factors such as high physical demands, variable working hours, job insecurity, and limited control over tasks. This study emphasizes the importance of considering the interplay of individual, job-related, social, and organizational factors in understanding the psychological harm experienced by construction workers. Factors such as occupational stress, lack of supervisor support, job insecurity, substance abuse, social isolation, and the transient nature of work contribute to the complex mental health landscape within the industry.
Addressing psychological harm requires a comprehensive and multifaceted approach. Health and safety regulations should be strengthened to integrate mental health considerations, such as regular screenings and psychological risk assessments. Workplace interventions should focus on creating supportive work environments, enhancing job control, providing supervisor support, and promoting job security. Mental health support services tailored to the unique needs of construction workers, including counseling, stress management programs, substance abuse treatment, and suicide prevention initiatives are essential.
Ultimately, addressing the psychological harm experienced by construction workers is crucial not only for their wellbeing but also for the overall health and productivity of the industry. By prioritizing mental health and implementing evidence-based interventions, we can create a safer and more supportive construction environment that protects the health and psychological wellbeing of its workers. This can also be achieved with the support of occupational health professionals. The benefits of the support of occupational health professionals on construction sites have already been highlighted. For instance, Minna and Mika (2012) propose that occupational health personnel visit construction sites to assess work performance as part of a multifactorial intervention that includes a modification of behavioral and lifestyle factors and ergonomic modification to reduce musculoskeletal disorders among construction workers. The authors propose that this approach should be extended to occupational health nurses who play a pivotal role in identifying and addressing mental health needs. For construction workers, this could be achieved by conducting mental health screenings, implementing early interventions, and offering ongoing support to manage stress and prevent psychological harm. Further to this, occupational health nurses can contribute to expanding the understanding of the mental health risks within the construction sector by conducting studies that explore effective interventions and strategies to mitigate psychological harm, including research on the impact of job design, social support systems, and work-life balance on mental health outcomes. To achieve this, there is a need to integrate mental health awareness and management into the training and professional development of occupational health nurses. This includes preparing nurses to recognize early signs of mental distress and equipping them with the tools to support workers through evidence-based mental health interventions. Moreover, fostering a deeper understanding of the construction industry’s unique demands will empower nurses to better serve this vulnerable workforce. By enhancing mental health literacy, occupational health nurses can become key advocates for mental health in workplace settings, ultimately improving worker wellbeing and safety.
In Summary
Mental wellbeing in the construction industry is influenced by job satisfaction, autonomy, and co-worker support, with studies showing a positive relationship between decision authority, job satisfaction, and mental health among workers. However, high job demands, job insecurity, and risky health behaviors present significant challenges.
Supervisor support and the role of supervisors are critical in mitigating stress and contributing to mental health deterioration, indicating the necessity for supportive environments and enhanced job control to buffer negative job stress impacts.
The resilience among construction workers, bolstered by a strong camaraderie culture, acts as a protective factor against stress, highlighting the importance of peer support but also pointing to the need for formal mental health support systems, including regular screenings and wellness programs.
Improving mental wellbeing requires a comprehensive approach, integrating mental health into health and safety regulations, promoting supportive work environments, and providing accessible mental health services tailored to construction workers, underscoring the importance of a holistic strategy in addressing psychological harm.
Footnotes
Author Contributions
Azizur substantially contributed to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work. Katrin reviewed the draft critically for important intellectual content. Kennedy reviewed the draft critically for important intellectual content.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.