
Abstract
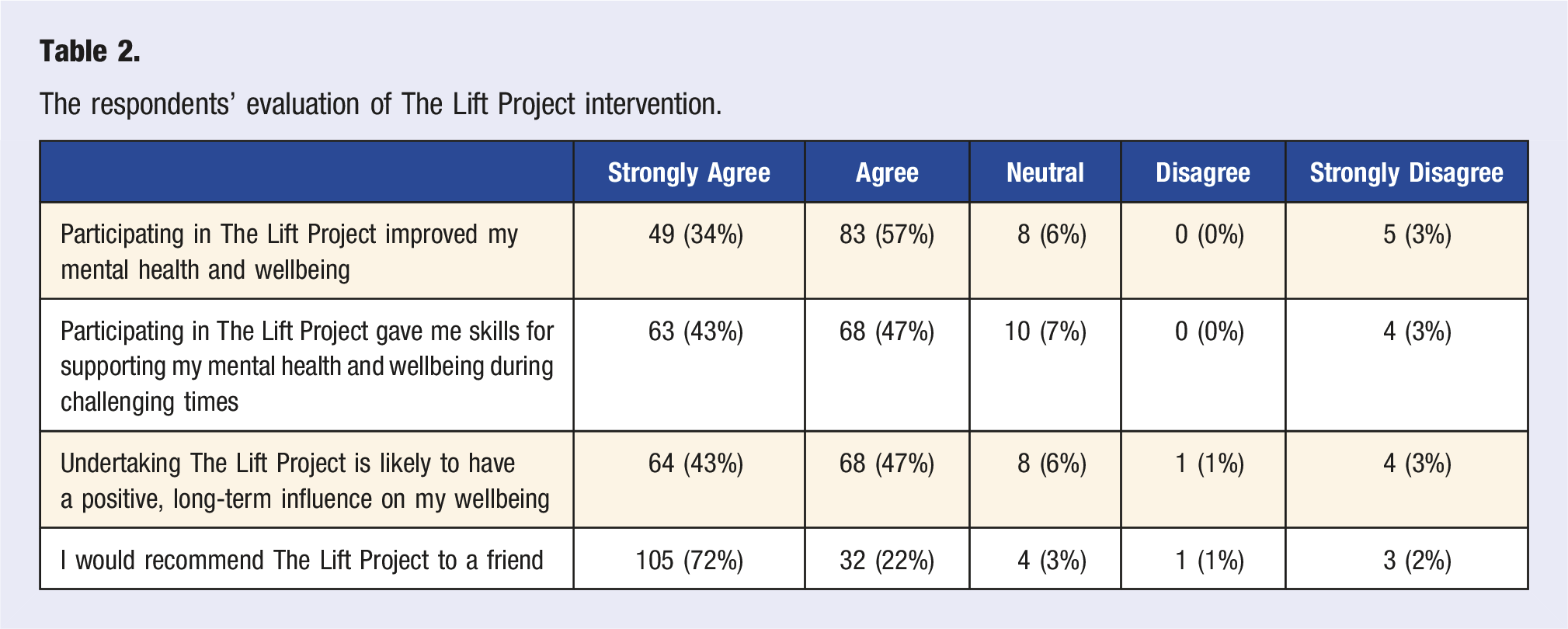
In the wake of COVID-19, the American College of Lifestyle Medicine offered its members an online 10-week multicomponent mental health and wellbeing program (The Lift Project), and extended the invitation to members from sister organizations associated with the Lifestyle Medicine Global Alliance. A total of 1785 members registered for the program, representing 39 countries. The website hosting the program recorded 9815 total visits over the 10 weeks. In a post-program questionnaire completed by 145 participants, 91% agreed or strongly agreed that the program supported their mental wellbeing, and participants reported their wellbeing as higher after the program as compared to its commencement (X2 = 80.8, P < .01). Ninety-four percent of respondents indicated they would recommend the program to a friend. Thematic analysis of open-ended responses included in the post-program evaluation indicated that the participants liked: the structure of the program and content covered; the style of the video presentations; and the practical application of the program. Some participants indicated they would have liked more time to engage with the program and would have enjoyed the provision of group meetings. In conclusion, healthcare organizations can support their members’ mental health and wellbeing by offering large-scale, evidence-based interventions.
‘The findings of this study suggest that offering an online mental health and wellbeing program to the member-base of a healthcare organization can be well-received and beneficial’.
Introduction
The world is experiencing a mental health and wellbeing crisis. 1 The Global Burden of Disease Study reported that mental health disorders are a leading and growing concern 2 that the COVID-19 pandemic has further exacerbated.3,4 The annual global economic burden of mental health disorders has been estimated at 5 trillion (USD), 5 yet the crisis is not abating. The 2022 World Mental Health Report concluded that ‘business as usual for mental health simply will not do’, and that there is an urgent need for novel solutions to address the mental health pandemic.
There is growing evidence that lifestyle-based therapies confer mental health benefits, 6 which demonstrates that the pillars of Lifestyle Medicine benefit the brain as well as the body. Indeed, this has led to the emergence of ‘Lifestyle Psychiatry’, 7 which advocates healthy lifestyle behaviours as frontline therapies for affective mood disorders. Similarly to Lifestyle Medicine, the discipline of Positive Psychology has experienced exponential growth since its inception in the late 1990s, 8 and Positive Psychology Interventions (PPIs) have demonstrated efficacy for increasing mental health and wellbeing. 9 More recently, there has been an awakening to the benefit of combining strategies from Lifestyle Medicine and Positive Psychology to create multidisciplinary and multi-modal interventions for alleviating the mental health burden. 10
Healthcare providers face unique vocational challenges and are not immune to the widespread mental health crisis. Globally, there is a dearth of mental health services, which results in a lack of treatment options for mental health patients and clients, and places pressure on health professionals. 1 The demands of COVID-19 also placed increasing strain on healthcare providers, 11 and a 2022 survey of over 13,000 physicians found that nearly half (47%) reported feeling burnt out. 12 Indeed, burnout among health professionals is a recurrent theme within the medical literature. 13
In response to the alarmingly high rates of burnout amongst healthcare providers, the National Academy of Medicine instigated an Action Collaborative on Clinician Wellbeing and Resilience. The Collaborative identified a key objective to ‘advance evidence-based, multidisciplinary solutions to improve patient care by caring for the caregivers’. 14 Indeed, ‘caring for the carers’, through the provision of skills and resources for practising self-care, is being actively promoted by organizations such as the American Medical Association. 15 A pertinent question is how to most effectively deploy ‘evidence-based, multidisciplinary solutions’ to benefit clinician wellbeing.
The aim of this study was twofold. Firstly, to examine the acceptability and benefits of a multidisciplinary mental health and wellbeing intervention (The Lift Project) for health professionals associated with the Lifestyle Medicine community. To date, The Lift Project intervention has demonstrated efficacy and acceptability among university students,16,17 community cohorts,18–23 and patients in a clinical setting. 24 However, the appropriateness of the intervention for healthcare professionals has not been investigated. The second aim of the study was to explore the utility of a model for delivering an online mental health and wellbeing program on a large-scale by offering it to an organization’s entire member-base – in this case, the American College of Lifestyle Medicine (ACLM) and members of the Lifestyle Medicine Global Alliance (LMGA).
Methods
Study Design
The study was a single cohort mixed methods design. The 10-week intervention commenced in February 2022 and concluded in April 2022, after which the participants were invited to respond to a post-program evaluation involving both quantitative and open-ended questions. The study was approved by the Avondale University Human Research Ethics committee (No. ETH.2021.007).
Participants
The Lift Project was promoted as a free offering to all ACLM members (through the ACLM newsletter) for 1 month before the program’s commencement. Approximately 2 weeks before the program commenced, ACLM extended the offer to members of Lifestyle Medicine sister organizations affiliated with the Lifestyle Medicine Global Alliance. Interested members registered on a customized registration webpage, which remained open for 2 weeks after the program commenced.
A total of 1785 individuals registered for the program, representing 39 countries. Most participants were from the United States (72%, N = 1288), followed by Australasia (11%, N = 203). India, Poland, Chile and Pakistan each recorded over 20 participants (N = 63, 56, 38 and 21, respectively), with the following countries recording fewer than 20 registrations each: Nigeria, Hong Kong, Singapore, United Kingdom, Canada, Hungary, Columbia, Japan, Kenya, Argentina, Brazil, Mexico, Philippines, Sudan, Korea, Mongolia, United Arab Emirates, Albania, Botswana, El Salvador, Ethiopia, Jamaica, Lithuania, Oman, Lebanon, Peru, Puerto Rico, Romania, Sri Lanka, Sweden and Turkey.
Intervention
The intervention was a customized version of The Lift Project, 25 which is a 10-week educational program that experientially explores evidence-based strategies from the disciplines of Lifestyle Medicine and Positive Psychology for increasing mental health, wellbeing and resilience. The Lift Project is used in healthcare systems, clinics, workplaces, educational contexts (universities and schools) and community settings. Previous research using The Lift Project demonstrates that participants experience significant reductions in depressive symptoms, anxiety and stress.16–18,20,24 This is coupled with significant improvements in positive attributes of mental wellbeing, such as vitality, life satisfaction and flourishing. 19
The Lift Project intervention overview.
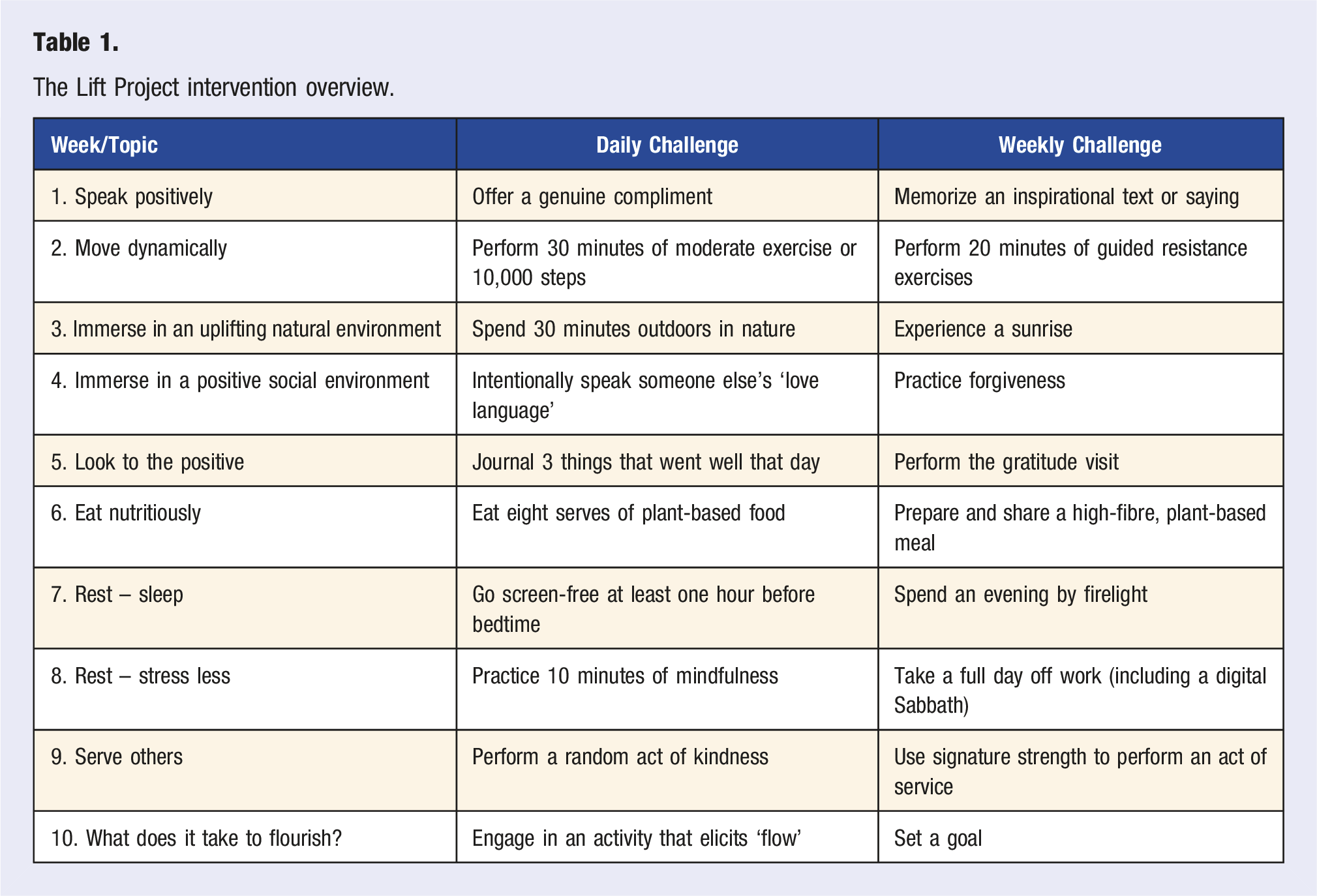
Participants accessed the program online through a customized course page, which contained links to the 10 lessons that were released once-weekly throughout the 10 week intervention duration. The participants received 2 email communications each week. The first email, sent at the beginning of the week, notified the participants that the next lesson had become available. The participants were directed to the course page to access the lesson. Content from previous weeks remained accessible to the participants, and all 10 lessons remained available for 2 weeks after the intervention completion. The second email sent each week, referred to as a ‘mid-week lift’, encouraged the participant to engage with the lesson’s challenges.
Measurements
The respondents’ evaluation of The Lift Project intervention.
Data Analyses
Data were analyzed using IBM SPSS Statistics (version 24). Descriptive statistics are presented as cell counts, relative percentages, mean and standard deviation. Pearsons Chi-square was used to assess changes to the respondents’ self-reported rating of their wellbeing pre- and post-program. Repeat-measures General Linear Modelling was used to analyze differences between the participants’ ratings of the benefits of the lessons and weekly challenges on their wellbeing. The qualitative data were analyzed by coding the participants’ responses to the 2 open-ended questions, which were then collated into themes (using Microsoft Excel).
Results
Program Visits
The 1785 individuals who registered for the program visited the online course page a total of 9815 times throughout the program. In the first week of the program, during which the participants were orientating themselves, there were 2804 visits to the first lesson. Figure 1 shows the number of visits to the weekly lesson pages following the initial orientation week (i.e., Weeks 2-10). The number of lesson visits decreased over the duration of the intervention, with attrition mostly occurring in the first few weeks. Lessons 8 to 10 recorded around 500-600 visits each. Webpage visits to the weekly lesson.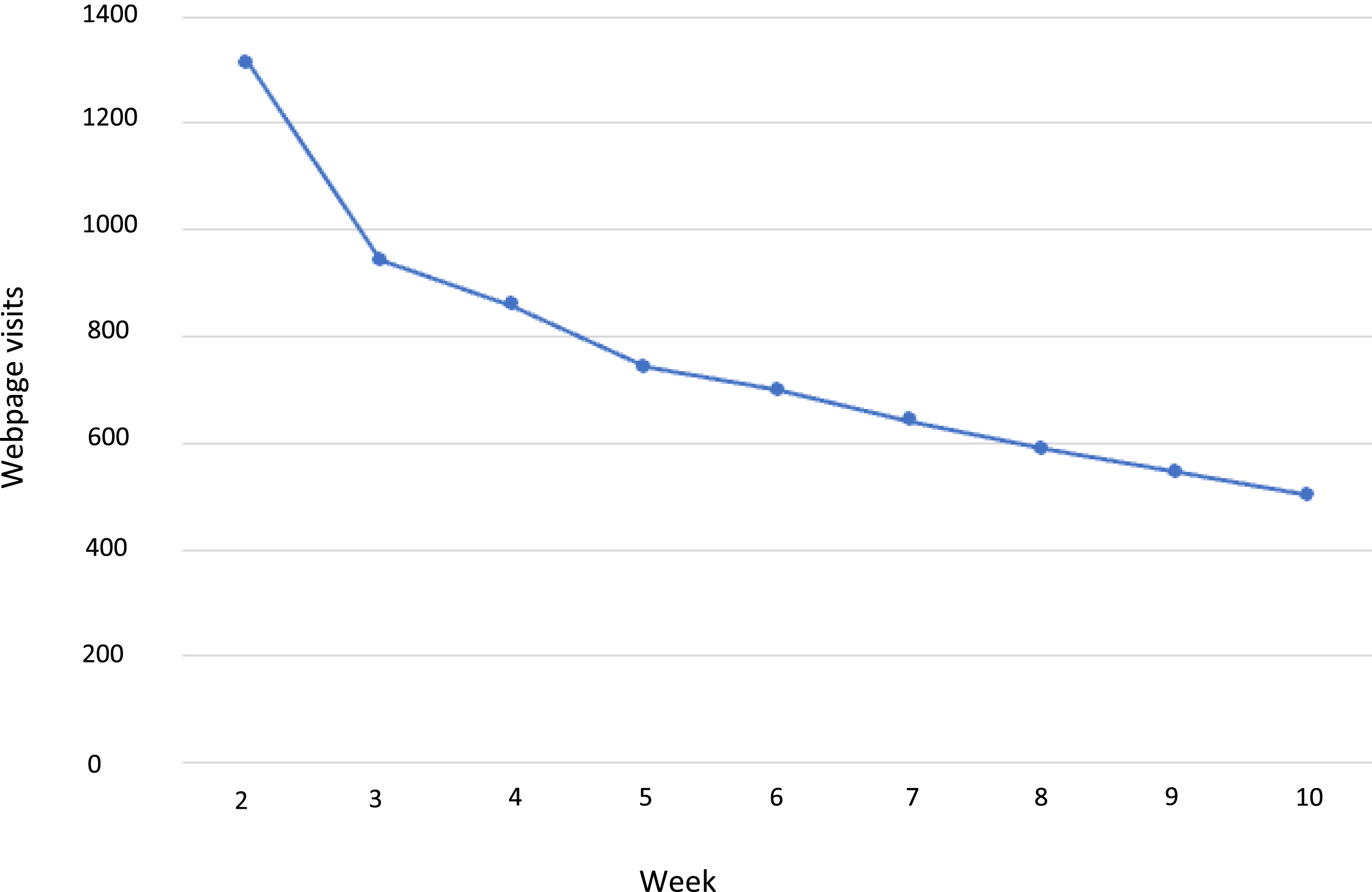
Post-Program Evaluation – Quantitative Responses
One hundred and forty-five participants responded to the post-program evaluation, 116 (80%) females and 29 (20%) males. Approximately two-thirds of the respondents (61%) were between the ages of 30 to 50 years: 21-30 yrs, N = 6 (4%); 31-40 yrs, N = 48 (33%); 41-50 yrs, N = 41 (28%); 51-60, N = 30 21%); 61-70, N = 19 (13%); 71-80, N = 1 (1%). Most respondents (72%) indicated that they engaged with the program independently, while 18% stated that they participated with a friend, and 10% as part of an online or face-to-face group. The participants were encouraged to invite their families to join them, and 28% of respondents indicated that they did this.
The respondents’ self-reported mental health and wellbeing before (pre) and after (post) The Lift Project intervention.
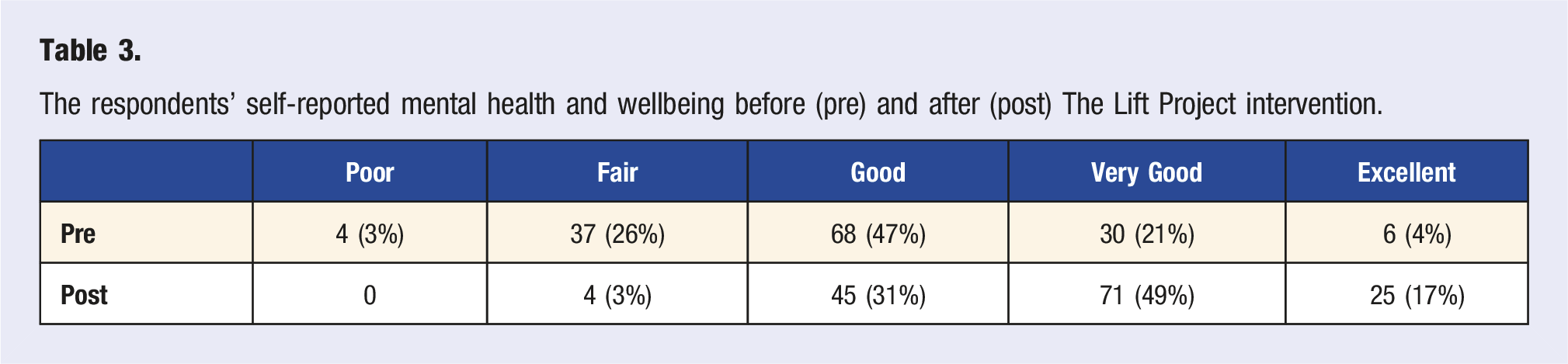
Figure 2 illustrates the respondents’ rating (mean, standard deviation) of the influence of the weekly challenges on their wellbeing. The mean rating for all the weekly challenges was between ‘small positive effect’ to ‘large positive effect’, but there was no difference in the mean rating observed between the challenges (F = 1.19, P = .297). Effect of the weekly topics/lesson on participants mental health and wellbeing.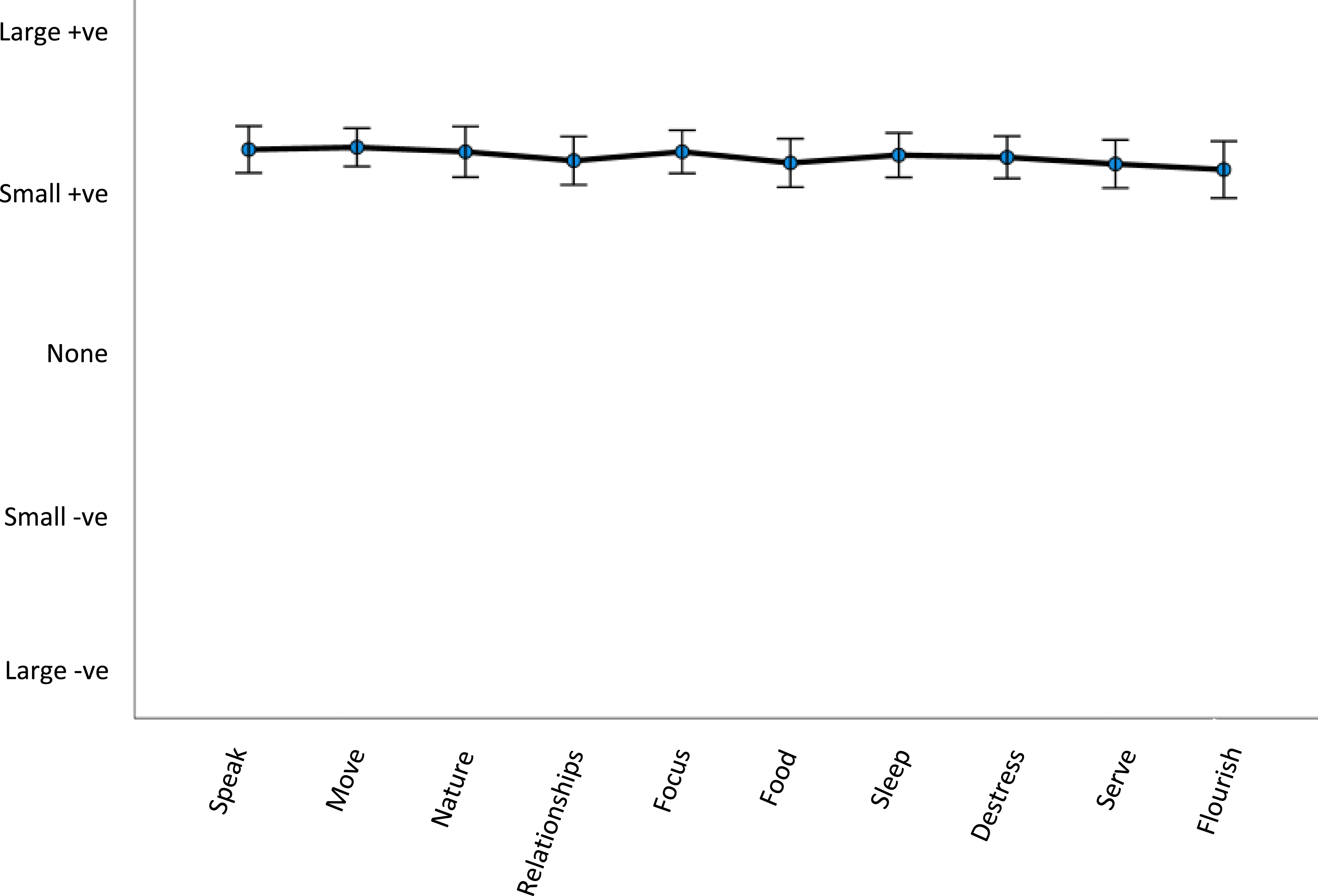
Post-Program Evaluation – Qualitative Responses
Of the 145 participants who responded to the post-program evaluation, 130 (90%) responded to the question ‘What did you like about The Lift Project?’ and 112 (77%) responded to the question ‘What didn’t you like about The Lift Project?’ Of those who responded to the ‘What didn’t you like’ question, 45 indicated ‘nothing’, which left 67 codable responses.
What Participants Liked
Themes of what participants liked about The Lift Project intervention.
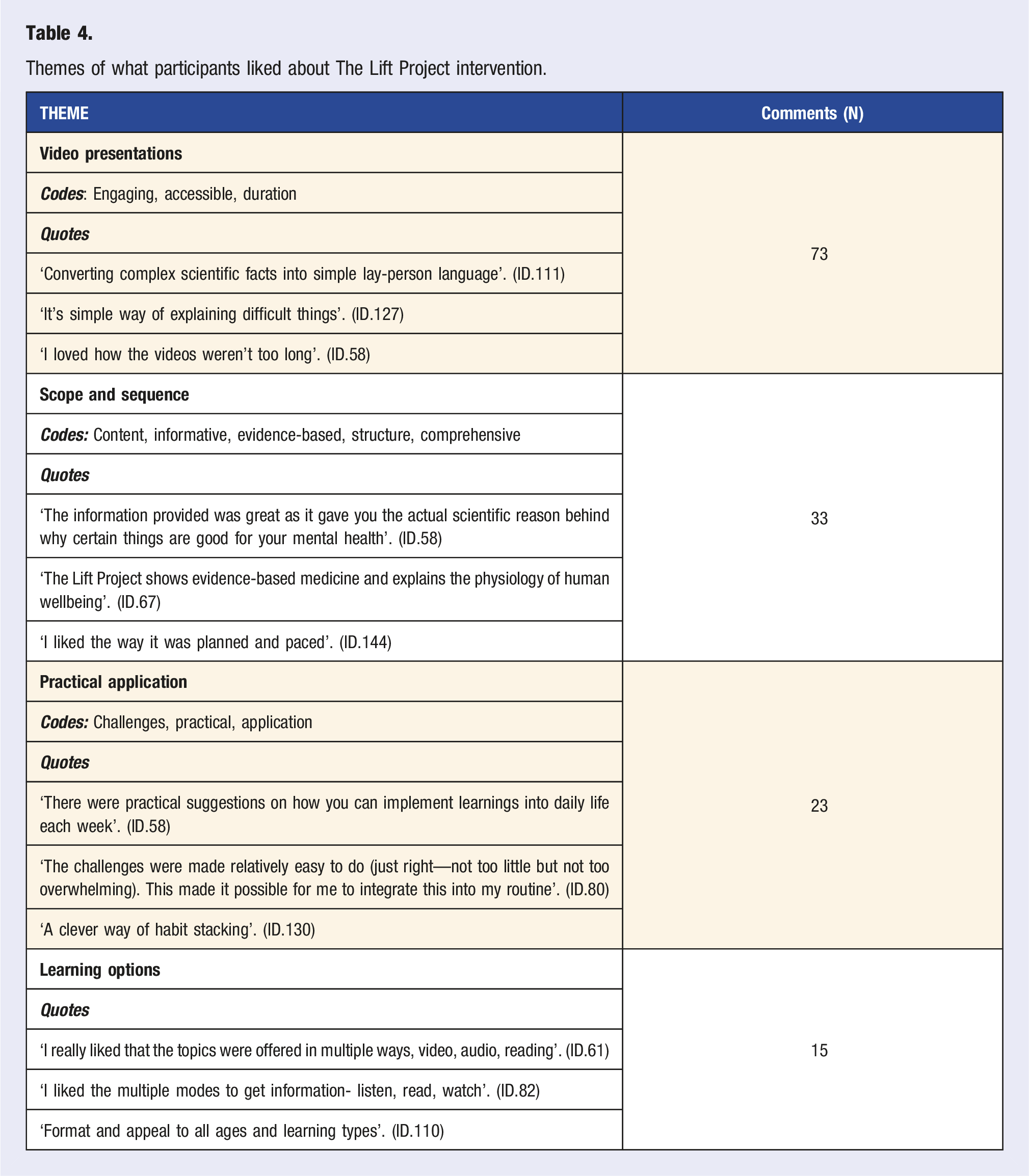
Lesser reported elements of the program that participants indicated they liked included: the mid-week email communication, the catchy phrases for the lessons, the positive focus of the program, and the included workbook and other resources.
What Participants Didn’t Like
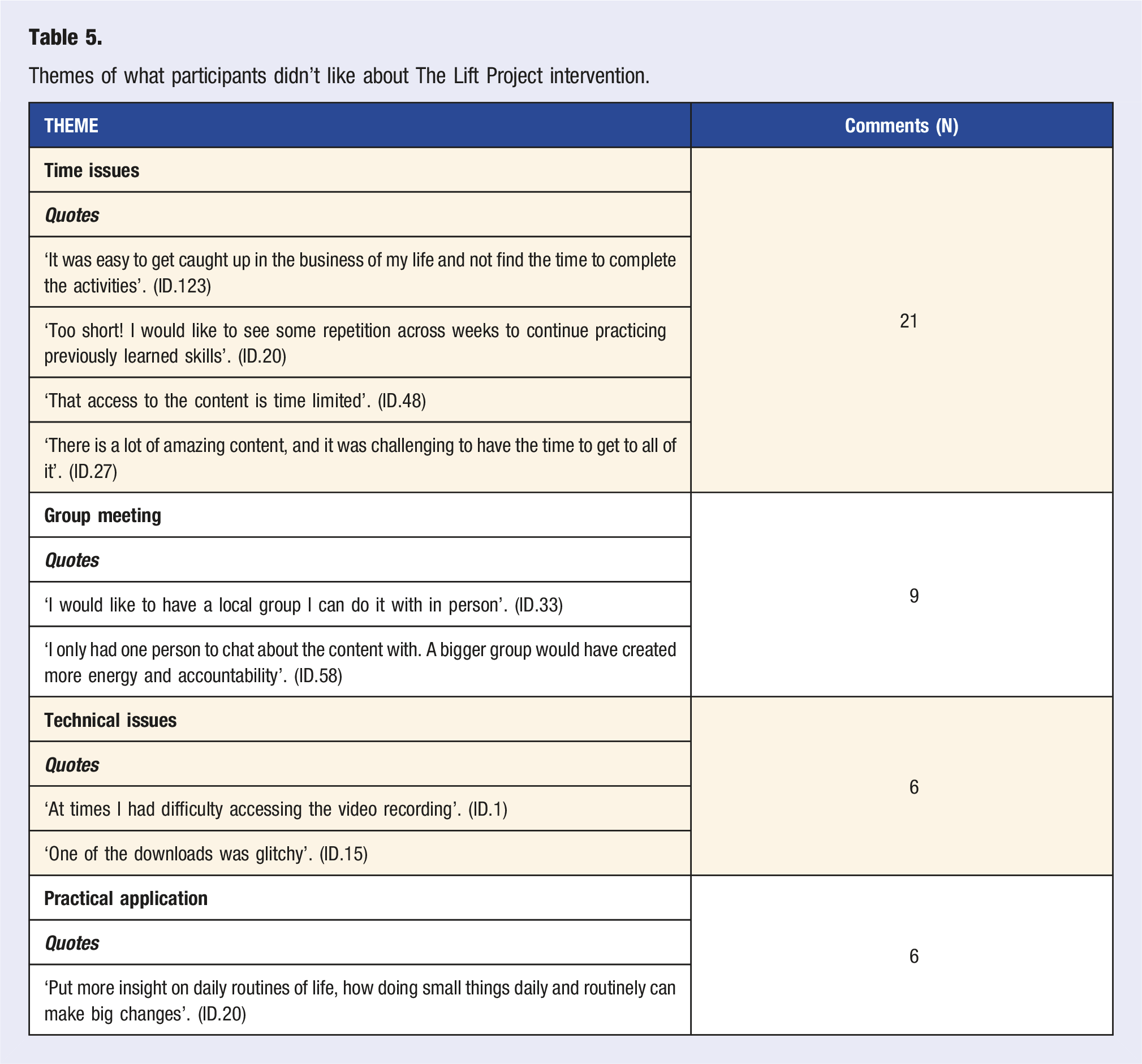
Themes of what participants didn’t like about The Lift Project intervention.
Discussion
The findings of this study suggest that offering an online mental health and wellbeing program to the member-base of a healthcare organization can be well-received and beneficial. The model of delivery used in this study may provide an exemplar for providing large-scale mental health support and education through professional organizations, particularly healthcare member groups suffering high levels of stress and burnout.
An encouraging observation of the current study is the extent to which the Lifestyle Medicine community is international in scope, with the initiative attracting participants from nearly 40 countries. It is unremarkable that most participants were enlisted from the American College of Lifestyle Medicine, as this was the hosting organization and has the largest membership worldwide. The high level of interest from Australasia (Australia and New Zealand) was also not surprising given that a member of the Australasian Society of Lifestyle Medicine created the program. Certainly, the extent of representation from different countries was encouraging, especially since the program was only offered to Lifestyle Medicine Global Alliance members 2 weeks before it commenced.
It would be informative to replicate this study for different healthcare professional organizations and compare the level of interest and uptake. Undoubtedly, the Lifestyle Medicine community represents a unique cohort of providers aligned with lifestyle-based interventions. Hence, members of Lifestyle Medicine professional organizations may be more open to participation in a lifestyle-based intervention than the typical healthcare provider. However, Lifestyle Medicine enthusiasts might be less likely to personally engage in a wellbeing program due to a perception that they will already be familiar with the program’s content, information, and strategies. Further, healthcare providers aligned with Lifestyle Medicine might be more likely to be already practising healthy lifestyle behaviours and doing better regarding their personal wellbeing, and therefore not in need of additional support. Notwithstanding, it is notable that over 40% of the respondents reported their mental health and wellbeing at the time of registering for the program as ‘poor’ or ‘fair’ (Table 3).
The challenges around engagement and attrition when delivering large-scale, online, wellbeing interventions are well documented.21,23,26,27 In the current study, the decrease in engagement over the 10 weeks of the program was anticipated (see Figure 1). One factor that might be important for enhancing engagement and reducing attrition is social support,21–23 and some participants in the current study indicated that they would have benefited from group interaction throughout the program. The predominance of female participation in the current study is consistent with what is commonly seen in wellbeing interventions,28,29 including studies that have used the same intervention as in the present case. 30 Engaging males remains an ongoing challenge but may be aided by reducing stigma, promoting enjoyable activities and increasing social cohesion. 31 The Lift Project intervention is intentionally framed positively to alleviate stigma and the challenges are designed to enhance enjoyment, but clearly it still attracted predominantly female participants.
The Lift Project has been utilized in a similar format to the current study in several geographical locations around the world as a community development initiative, with one program in New York State recording over 5000 registrations. 32 While studies of these community-targeted programs have reported high levels of acceptability among the participants, comparable to that observed in this study, 33 the level of uptake is substantially less. Typically, when the program is offered to a defined community group, such as a local county or region, approximately 1-2% of the targeted population register. By contrast, when conducting the current study, the ACLM membership totalled around 7,000, indicating that nearly 20% of members registered for the initiative. This highlights that professional organizations may be uniquely positioned to offer mental health and wellbeing programs as they have well-established communication channels with large numbers of individuals. Moreover, professional organizations are concerned with adding value to their members and offering mental health and wellbeing programs is well aligned with this mandate.
An important limitation of the current study was the way the participants were asked how beneficial they found the program retrospectively. Clearly, a pre- and post-test methodology, coupled with a randomized controlled design, would be ideal. A previous randomized controlled trial of The Lift Project found that compared to a control group, participants in the intervention experienced significant improvements in various mental health and wellbeing metrics, with the benefits persisting at 6 months.18,19 Another limitation of the present study is the low response rate – approximately 30% of those who completed the program responded to the post-program questionnaire – although the open-ended responses added to the depth of the data analysis.
Conclusions
The outcomes of this study suggest that an online mental health and wellbeing program can be effectively offered on a large scale to the members of a professional healthcare organization. Given the mental health and burnout challenges faced by healthcare professionals, the provision of mental health and wellbeing interventions through professional organizations appears to represent a useful and impactful model of providing support and enhancing the wellbeing of the healthcare workforce.
Footnotes
Acknowledgements
The authors would like to acknowledge the work of Leticiia Maguire from The Lift Project for supplying and customizing the intervention used in this study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DM is the Director of the profit-for-purpose Trust that own the intervention used in this study. He has recievned no financial reimbursement. MR and SM have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.