
Abstract
Background:
This quality improvement project aimed to increase the screening rate for OSA in individuals aged 18 and above with obesity (body mass index [BMI] ≥30).
Methods:
This quality improvement study occurred from March 2023 to August 2023 using a two-independent pre-implementation post-implementation design. The STOP-Bang Questionnaire (SBQ) was implemented during annual exams, chronic disease management visits, and Department of Transportation (DOT) physicals.
Findings:
There were 946 patients involved in the study, including 471 in the pre-implementation group and 475 in the post-implementation group. OSA screening increased from 14.1% to 71.6% after implementing the screening protocol in the general population and 26.7% to 90.4% in the commercial driver’s license (CDL) holder population. Of the CDL holders screened in the pre-intervention group, 15 (65.2%) were at intermediate to high risk for OSA (SBQ ≥3), and in the post-intervention group, 33 (50%) had an SBQ score of ≥3.
Conclusions/Application to Practice:
Standardized OSA screening is crucial because it is common but underdiagnosed. Screening for OSA during DOT exams promotes community safety. Earlier identification of at-risk patients leads to earlier diagnosis and treatment of OSA to prevent long-term complications, reduce healthcare costs, improve patient outcomes, and improve community safety.
Keywords
Background
Obstructive sleep apnea (OSA) is the most common sleep-related breathing disorder, characterized by 10 or more seconds during sleep of recurrent partial or complete upper airway obstruction, leading to hypoxia, hypercapnia, and intermittent arousals (Faria et al., 2021). OSA severity is quantified by the apnea-hypopnea index (AHI), including mild, moderate, and severe. Mild is defined as 5 to 15 events an hour, moderate as 15 to 30, and severe as greater than 30 events an hour (Zheng et al., 2022). An estimated 12% of adults in the United States suffer from OSA, with a staggering 80% of these yet to be diagnosed (Martin et al., 2024). Untreated OSA increases the risk of atherosclerosis, metabolic dysfunction, immune dysfunction, resistant hypertension, arrhythmias, heart failure, neurocognitive deficits, memory problems, lower attention, and decreased executive function (Caporale et al., 2021; Faria et al., 2021; Gottlieb & Punjabi, 2020; Lee & Sundar, 2021). Severe OSA results in a two-fold increase in stroke risk and is an independent predictor of cardiovascular and all-cause mortality (Fattal et al., 2022; Mitra et al., 2021; Salman et al., 2020).
Obesity is well-established as a significant risk factor for the development of OSA. The percentage of commercial motor vehicle drivers with obesity (a BMI of 30 or higher) was roughly 33% when self-reported but 53% when an objective measurement was used (Gurubhagavatula et al., 2020). OSA prevalence in professional truck drivers was 40.1% for mild OSA, 16.2% for moderate, and 7.2% for severe (Huhta et al., 2021). A recent cohort study showed an OSA prevalence of 77.9% in a population of truck drivers with an average body mass index (BMI) of 30.14 and a mean age of 48.02 years (Pimentel et al., 2024). Commercial motor vehicle (CMV) drivers with untreated OSA experience fragmented, nonrestorative sleep, increasing the risk of excessive daytime sleepiness, also known as hypersomnia (Gusman et al., 2023). Obese CMV drivers had 1.2 to 1.7 times more fatigue while driving and 1.3 times the risk of involvement in a safety-related incident than non-obese drivers (Mabry et al., 2022).
In the U.S., in 2015, the annual estimated cost related to workplace accidents, motor vehicle accidents, comorbid diseases, and loss in productivity associated with OSA was about $150 billion. This included the direct cost of managing sleep disorders and the comorbid conditions as well as the indirect costs (work-related injuries, loss of productivity, and motor vehicle accidents; Arsic et al., 2022). Burks et al. (2020) found that the odds of a driver with untreated OSA having a crash rate of 243% higher than one without. When treated, the rates are lowered to those without OSA. This validates the strong association between motor vehicle accidents in those with untreated OSA in both non-commercial and commercial drivers (Chen et al., 2021). OSA screening during a DOT exam has been lacking and sporadic because there is no standardized screening protocol, drivers and medical examiners are less aware of OSA symptoms, drivers underreport OSA symptoms, and the screening tool used is inconsistent. The Federal Motor Carrier Safety Administration’s Medical Review Board (FMCSA; MRB) released OSA screening recommendations in 2016, but no formal regulations were finalized (Wilcox et al., 2020).
The guidance for routine screening of OSA in asymptomatic adults is conflicting. The U.S. Preventative Service Task Force (USPSTF) concluded that insufficient evidence exists to screen asymptomatic adults for sleep apnea. The USPSTF does recognize that older adults (aged 40–70), men, and those with higher BMI are at increased risk for OSA. The American Academy of Sleep recommends screening in higher-risk populations, including but not limited to heart failure, resistant hypertension, type 2 diabetes, arrhythmias, and stroke (Kapur et al., 2017). Barriers to sleep apnea screening in primary care stem from a knowledge deficit of the disease, the importance of early detection and treatment, and the management of OSA (Devaraj, 2020; Pendharkar et al., 2021). Less than 25% of primary care providers routinely screen for OSA (Orbell et al., 2023).
The purpose of this quality improvement project was to increase the screening rate for OSA in adults over 18 with obesity (BMI ≥30) and compare rates of individuals identified as intermediate to high risk for OSA in the CDL holder population pre-implementation versus post-implementation.
Methods
The problem at the project site was identified as a deficiency of OSA screening among higher-risk groups (i.e., male gender, obesity, craniofacial or oropharyngeal abnormalities) in the general population and CDL holders (Mitra et al., 2021). An educational session was held with the clinical team at the quality improvement site to discuss the implementation of the OSA screening protocol, including the use and scoring of the SBQ and the patient criteria for screening. Frequent verbal reminders at team meetings and posted signs throughout the clinical site reinforced OSA screening. Knowledge gaps, barriers to screening, and the need for additional training were monitored throughout the project (Ten Ham-Baloyi, 2022). The United States Department of Health and Human Services recognized that OSA is underdiagnosed by adding an objective to the Healthy People 2030 initiative to increase screening in adults with sleep apnea symptoms (Office of Disease and Health Promotion, 2023).
The two-independent group pre-post quality improvement (QI) project was conducted at an on-site health clinic in Palm Beach County, Florida. The clinic serves as a primary care and occupational health center for the county’s employees, spouses, and dependents. All DOT physicals for the employees and new hires (bus drivers/CDL holders) occur at this location. A family physician, a family nurse practitioner, and a float nurse practitioner provide these services and treat approximately 500 patients monthly.
Study Population and Recruitment
The population was a convenience sample of adults 18 and older with a BMI ≥30 who presented for an annual physical, DOT exam, or chronic disease management (CDM) follow-up at the on-site clinic from March 2023 through August 2023. Exclusions included a previous diagnosis of sleep apnea, pregnant women, or those who completed a sleep study within the past year (n = 61).
Construction of Study Variables
Before implementing the innovation, the project leader completed a chart review on all adult patients presenting to the clinic ≥18 years of age during annual exams, CDM, and DOT physicals from March 2023 to May 2023. Research Electronic Data Capture (REDCap), a secure web application, was utilized to store data (Patridge & Bardyn, 2018). Data included age, gender, BMI, diagnosis of hypertension (0 = no, 1 = yes), SBQ administration (0 = no, 1 = yes) and score if applicable, polysomnogram ordered if applicable (0 = no, 1 = yes), and type of exam (0 = DOT, 1 = chronic disease management, 2 = annual physical). If a patient has a repeat visit within 3 months, they were only counted once. The same data were collected after implementing routine SBQ use from June 2023 to August 2023.
Instrument
The STOP-Bang Questionnaire (snoring, tiredness, observed apneas, high blood pressure, age, neck circumference, and gender) consists of four objective and four subjective questions with dichotomous answers with 0 for no and 1 for yes. SBQ score of 0 to 2 indicates low risk for OSA, 3 to 4 indicates intermediate risk, and ≥5 indicates high risk for OSA (Chen et al., 2021). Multiple screening tools have been validated for OSA screening, but there is no consensus on which tool to use routinely. The STOP-Bang Questionnaire (SBQ) is a widely used OSA screening tool initially designed for use in the preoperative setting (Chen et al., 2021). Overall, the tool has a 90% sensitivity and high negative predictive value (NPV) 77% in moderate to severe OSA and 91% in severe OSA (Pivetta et al., 2021). In the commercial driver population, using a cutoff of an SBQ ≥3, Chen et al. (2021) and Adami et al. (2022) found high pooled sensitivity (88%–98%) and NPV of (87%–99%), while specificity was poor at 29% to 44%.
Study Protocol
During the implementation period, the SBQ was administered to patients by staff on paper who met the criteria for screening. The results were then entered into the built-in screening tool in the project site’s electronic health record (EHR). The investigator reviewed the EHR records weekly and entered the data into REDCap. Scores on the SBQ ≥3, indicating intermediate risk for OSA, prompted a discussion about a referral to a sleep study, typically a home sleep test (HST). The sleep study referrals were tracked, and results were reported if known (Figure 1).
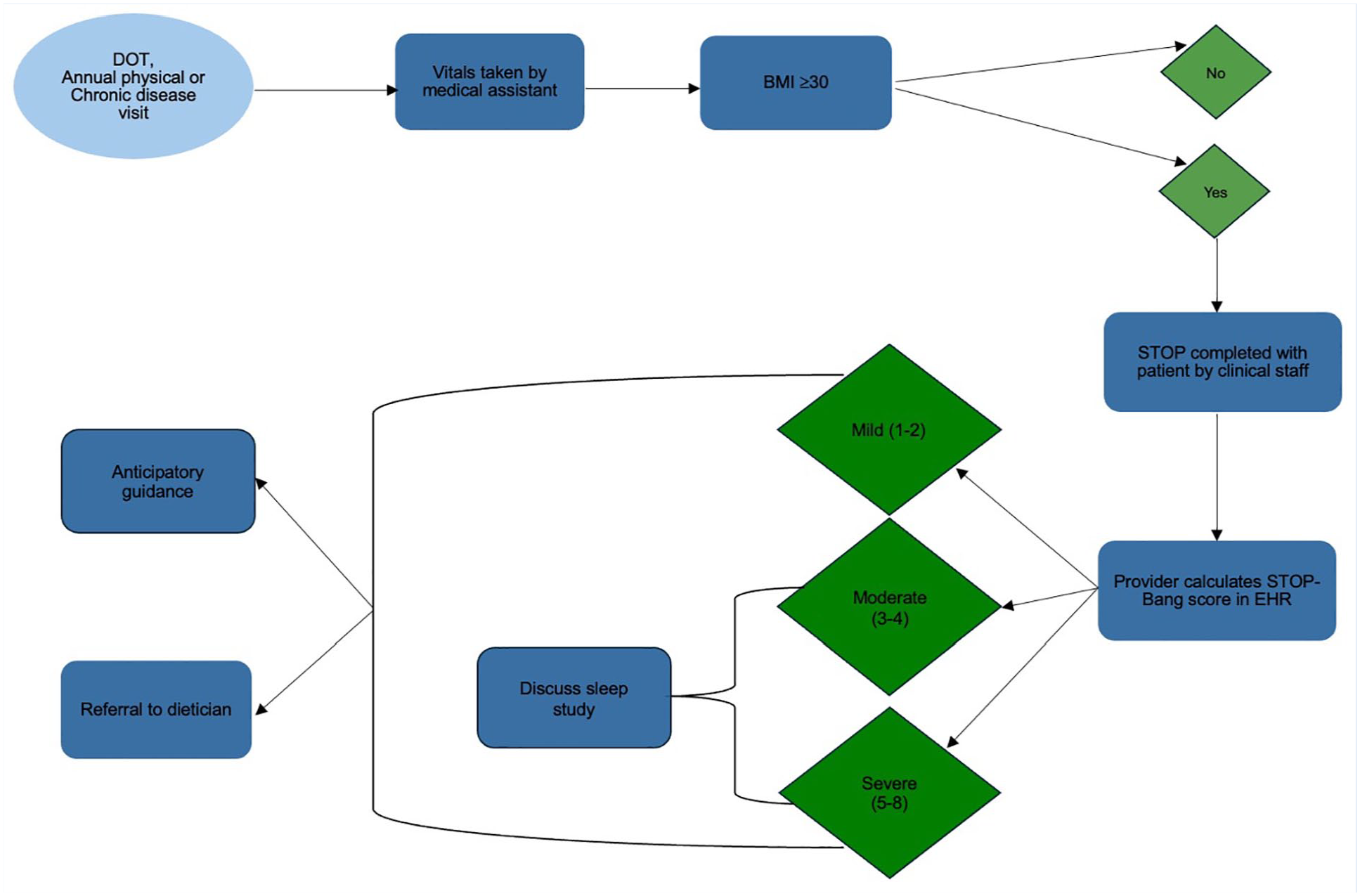
Process flow diagram
All patients in the project were offered anticipatory guidance and an educational pamphlet from the American Academy of Sleep Medicine (AASM, 2022) entitled The Link Between Obesity and Obstructive Sleep Apnea [Fact sheet]. Participants were also offered a referral to the registered dietician at no cost. Those with SBQ scores indicating intermediate to high risk for OSA were also given printed material from the American Thoracic Society (June 2019) entitled What is Obstructive Sleep Apnea in Adults? [Fact sheet] and from the AASM (2019) entitled Diagnostic Testing for Obstructive Sleep Apnea in Adults [Fact sheet].
Analysis Approach
All data were de-identified and kept in an encrypted secure file at the clinical site. The project deemed a QI project, did not require IRB approval or participant consent. Data were analyzed using Fisher’s Exact test for significance data using IBM SPSS v28.
Results
There were 946 patients involved in the project: 471 in the pre-implementation group (PRE) and 475 in the post-implementation group (POST). The mean age was 51.07 (SD = 11.86) for PRE and 51.23 (SD = 11.37) at POST, p = .870. The mean BMI was 31.20 (SD = 7.64) for the PRE and 31.28 (SD = 7.55) for the POST (p = .839). Gender was similar among groups (p = .205), as was race (p = .089) and ethnicity (p = .653). Chronic conditions were comparable: diabetes p = .137, hypertension p = .745. The visit type was most commonly DOT for PRE (41.8%) and POST (35.8%), p = .158 (Table 1).
Gender, Race, Ethnicity, Chronic Conditions, Visit Type, and STOP-Bang Scores
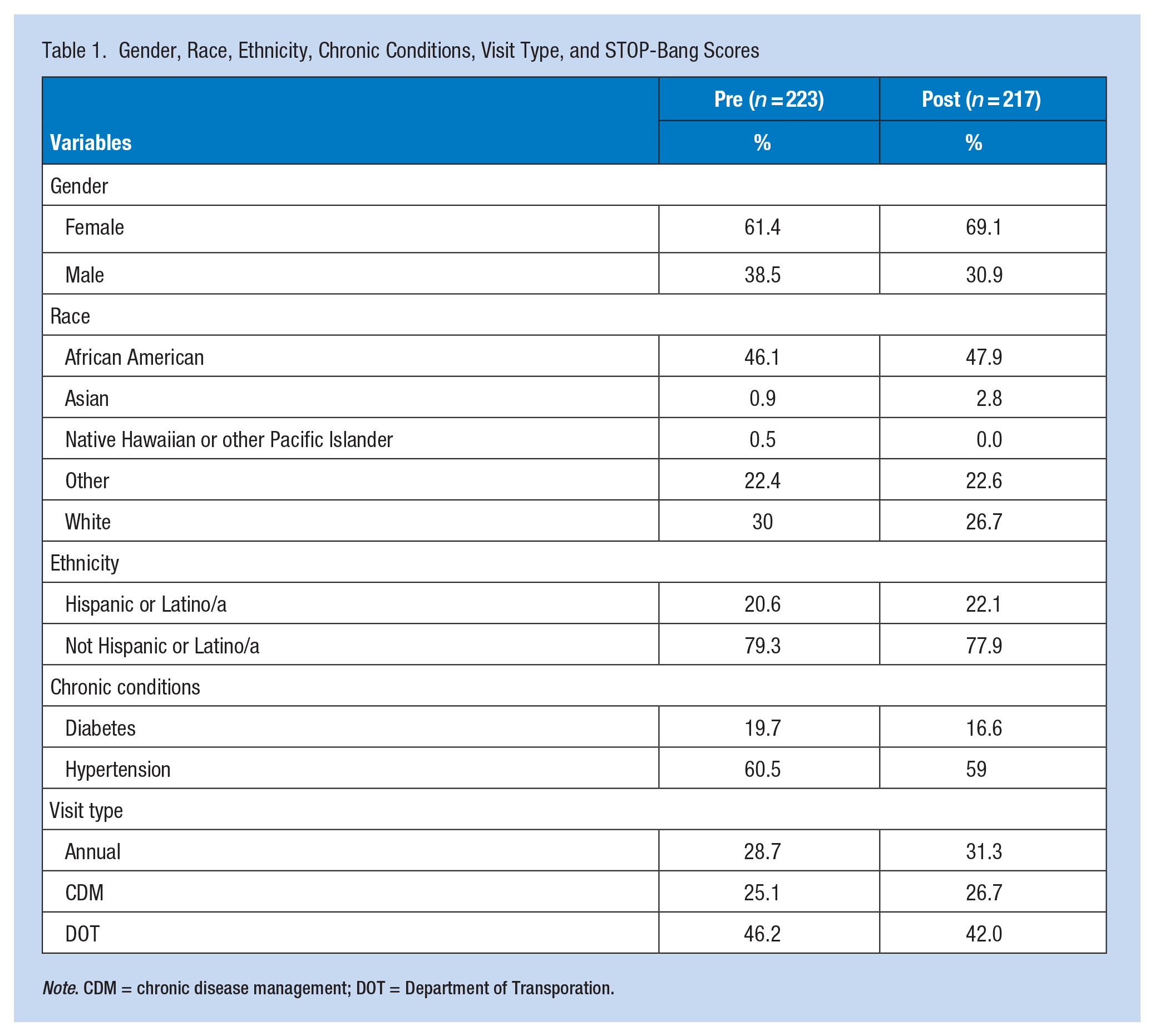
Note. CDM = chronic disease management; DOT = Department of Transporation
There were 198 patients eligible for screening in the PRE and 190 eligible in the POST. A Fisher’s exact test showed a statistically significant increase in OSA screening from 14.1% (n = 28) to 71.6% (n = 136), p < .001. Table 2 below shows the scores for the SBQ screening.
Total Population Screening Rates and HST Results
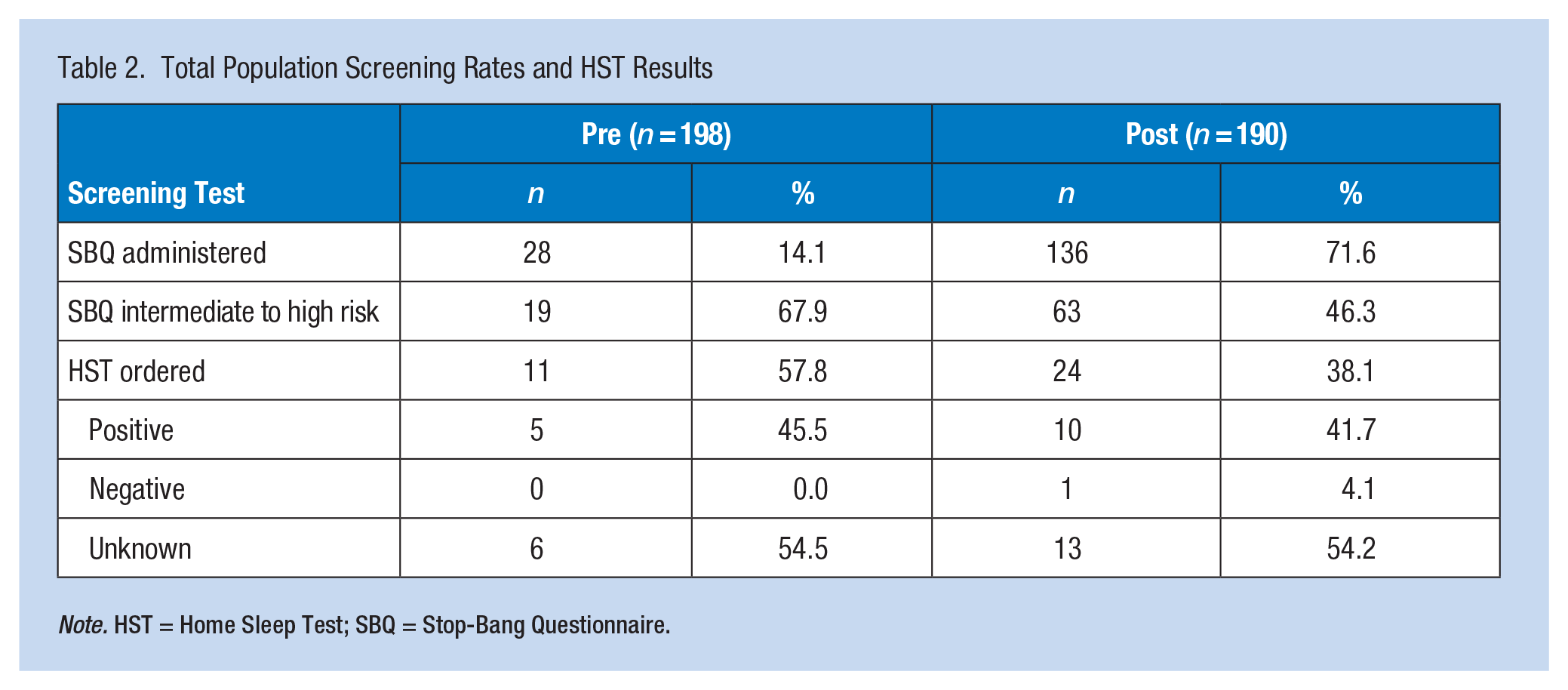
Note. HST = Home Sleep Test; SBQ = Stop-Bang Questionnaire.
In the PRE, 67.9% (n = 19) were intermediate to high risk. In the POST, 46.3% (n = 63) were intermediate to high risk based on a score of 3 or higher, showing a decrease, although it was not statistically significant (p = .060).
Standardized OSA screening rates significantly improved for the CDL holder patients: 26.7% (n = 23) versus 90.4% (n = 66; p < .001). Of the 23 screened in the PRE, 15 were intermediate to high risk (65.2%), p = .328, with a score of ≥3, including two patients with a score of 5; in the POST, 33 (45.2%) of the 66 screened were intermediate to high risk, including six patients with a score of 5 and two patients with a score of 6. For those who were intermediate to high risk, 40% were ordered a sleep study in the PRE; in the POST, nine out of the 15 patients who were intermediate to high-risk were ordered a sleep study (27.3%), which was a non-significant increase in sleep study orders (p = .137). In the PRE, one patient was diagnosed with severe sleep apnea. In the POST, two patients were diagnosed with moderate sleep apnea and one with severe sleep apnea (AHI = 101; Table 3).
Commercial Driver’s License Holder Screening Rates and HST Results
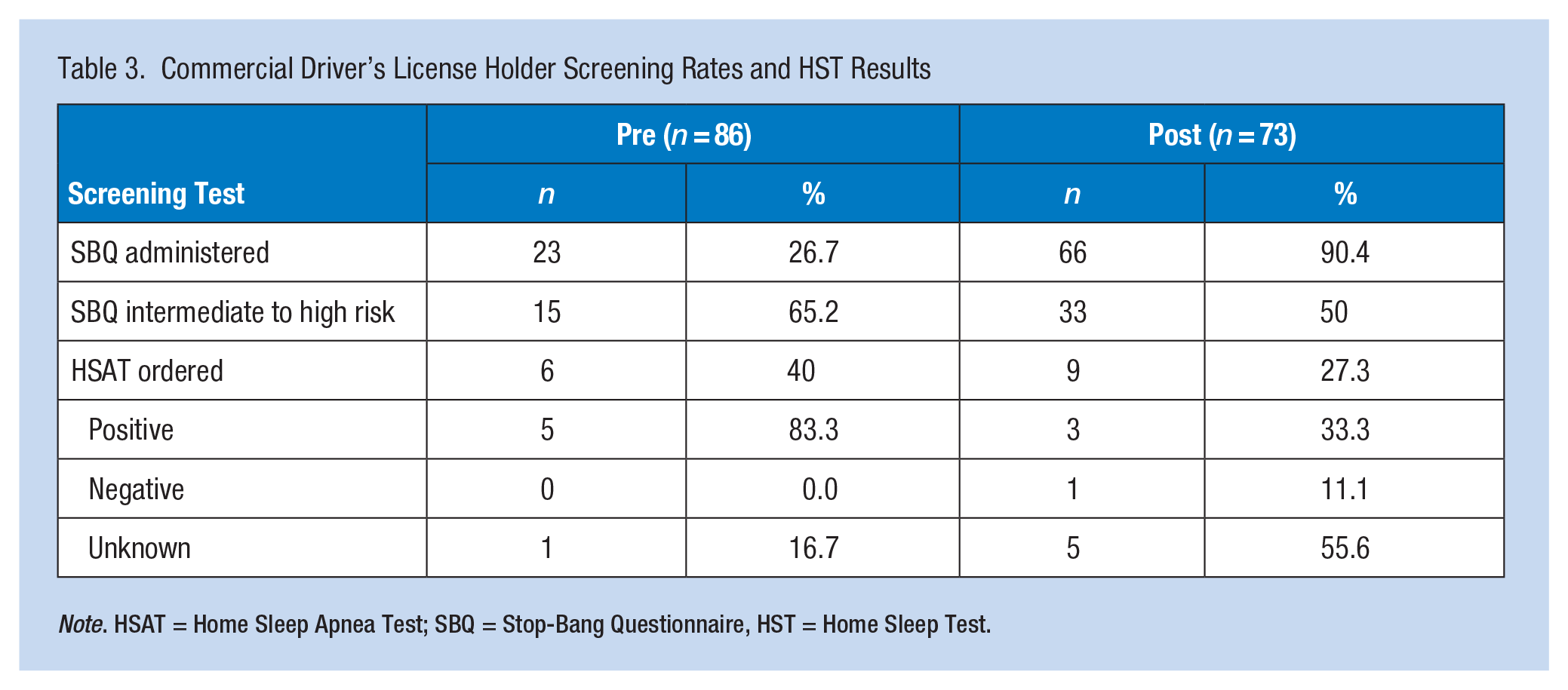
Note. HSAT = Home Sleep Apnea Test; SBQ = Stop-Bang Questionnaire, HST = Home Sleep Test.
Discussion
The researchers met the project’s aim by increasing OSA screening rates in the general population and CDL holders. Fewer individuals at intermediate-high risk for OSA were found in both groups from PRE to POST, but this was not statistically significant. The number of individuals screened for OSA in the POST group almost tripled from PRE, diluting the results in the larger sample. The healthcare provider knowledge gap about sleep apnea screening was overcome at our site. The increased awareness of screening for OSA has been sustained by all providers at the onsite clinic, resulting in earlier diagnosis and treatment of OSA. Employer funding for sleep studies would remove the financial barrier. It is imperative to public safety that the DOT population be identified and treated as early as possible to mitigate the risk of accidents.
Before implementation, CDL holders were screened based on the provider’s discretion using their preferred screening tool, mainly after symptoms indicative of OSA were reported. In the study population, 52.3% of CMV drivers in the PRE group and 53.5% of the POST group were found to have obesity as defined by BMI ≥30. Given that obesity increases the risk of developing OSA and impacts severity, adding an alert to the quality metrics in the EHR to complete the SBQ during all DOT exams if the patient has a BMI ≥30 could lead to an earlier diagnosis of OSA. There is no FMCSA regulation specifically regarding sleep apnea; however, they do state that a person with a medical history or clinical diagnosis of respiratory dysfunction likely to interfere with their ability to control and drive safely cannot be medically qualified to operate a commercial motor vehicle (Das et al., 2022). The routine screening for OSA with a validated tool would help identify at-risk individuals sooner and ultimately improve health outcomes and public safety.
This quality improvement project had several limitations. The study duration of 6 months did not allow enough time to follow up on all the sleep studies to be completed. A longer duration is needed to evaluate sustainability and generalizability. It was also challenging to convince CDL holders to complete sleep studies partly due to a lack of understanding of reasons for sleep testing and potential complications of untreated OSA. OSA is negatively viewed by some CDL holders who falsely believe a positive diagnosis negatively affects their jobs. Individuals were also met with difficulties with sleep testing, including financial barriers and coordination of care for testing. CDL holders who screened intermediate to high risk on the SBQ were referred to their PCP for evaluation and possible sleep testing. Many of the providers did not feel sleep testing was warranted. When trying to gain insight into this barrier, it was found that none of those providers were certified medical examiners. Hence, they were not familiar with FMCSA guidelines.
The clinical staff used a multidisciplinary approach to address all aspects of OSA. Anyone at risk for OSA was referred to the registered dietician onsite. After completing the project, previsits were initiated for all CDL holders to ensure all necessary paperwork was completed before the DOT exam appointment. A clinical staff member updates a spreadsheet with this information daily, which has improved follow-up on pending sleep studies. We also worked with the employer to lower the copay costs of a sleep study and treatment supplies, thereby removing the financial barrier. The clinic staff has sustained the intervention by routinely completing the SBQ during all DOT exams for individuals with a BMI ≥35.
Applying Research to Occupational Health Practice
Integrating OSA screening into health maintenance reminders in an EHR would improve earlier recognition of the disorder to prevent potential complications of untreated OSA. For individuals with risk factors for OSA, multidisciplinary team collaboration is vital to address barriers to care and increase patient engagement. This study highlighted the need to incorporate routine sleep apnea screening during DOT exams in accordance with FMCSA regulations for driver physical qualifications. The routine use of the SBQ and identifying those at risk for OSA would prompt earlier referral and treatment, improve quality of life, and lower safety risks and long-term adverse health outcomes.
Footnotes
Appendix
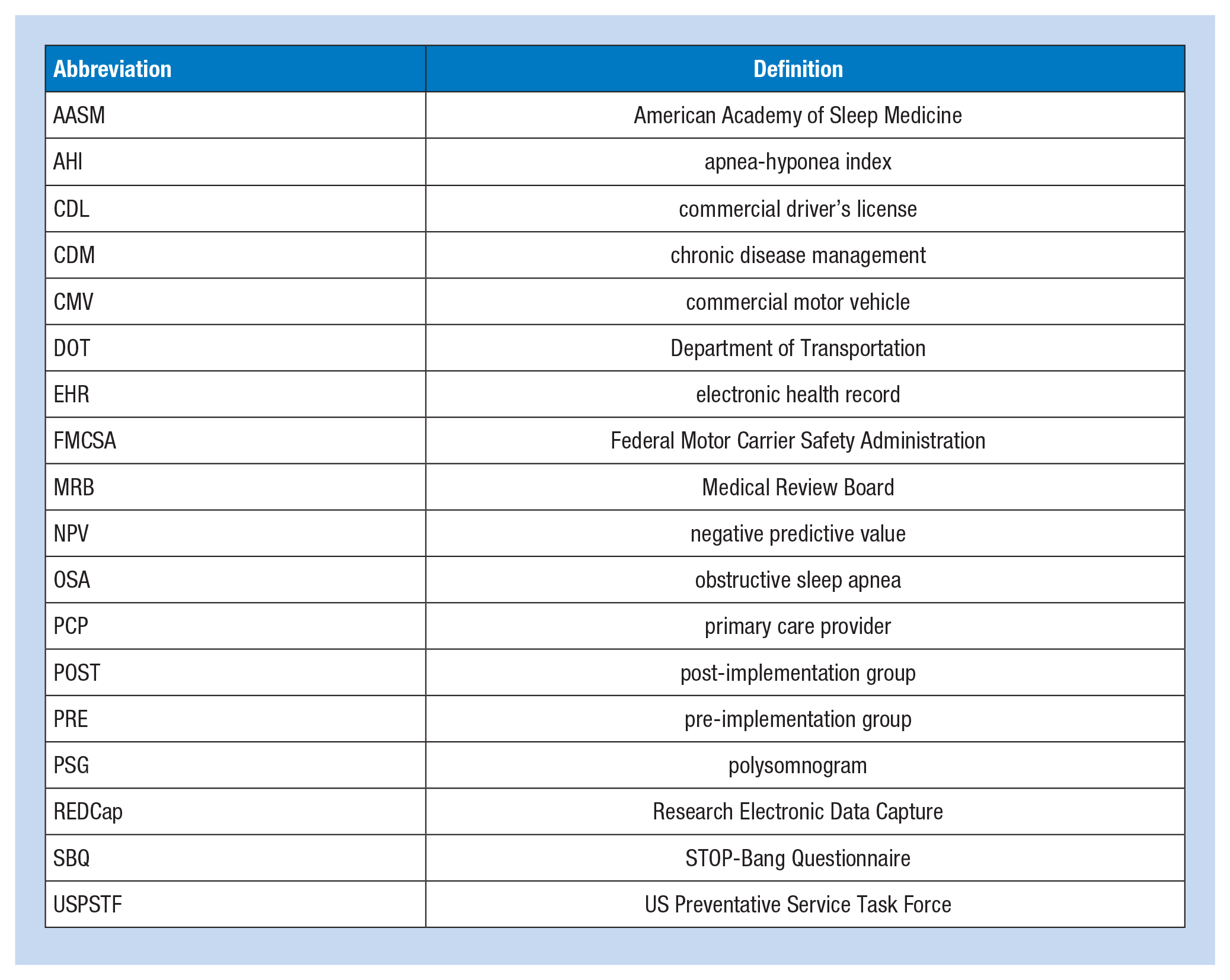
| Abbreviation | Definition |
|---|---|
| AASM | American Academy of Sleep Medicine |
| AHI | apnea-hyponea index |
| CDL | commercial driver’s license |
| CDM | chronic disease management |
| CMV | commercial motor vehicle |
| DOT | Department of Transportation |
| EHR | electronic health record |
| FMCSA | Federal Motor Carrier Safety Administration |
| MRB | Medical Review Board |
| NPV | negative predictive value |
| OSA | obstructive sleep apnea |
| PCP | primary care provider |
| POST | post-implementation group |
| PRE | pre-implementation group |
| PSG | polysomnogram |
| REDCap | Research Electronic Data Capture |
| SBQ | STOP-Bang Questionnaire |
| USPSTF | US Preventative Service Task Force |
Acknowledgements
The authors thank Julie Thompson, PhD., for consulting on statistical analysis and Dr. Joshua McNatt for guidance and support on-site throughout the project. His patience and expertise have been invaluable.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All data was de-identified and kept in an encrypted secure file at the clinical site. The project, deemed a quality improvement initiative, did not require IRB approval or participant consent.