
Abstract
Obstructive sleep apnea (OSA) is a disorder characterized by a cessation of breathing during sleep, leading to poor sleep patterns and daytime somnolence. Daytime somnolence is of particular concern for commercial vehicle drivers, whose crash risk increases 50% with untreated OSA. The process of diagnosing and treating OSA in commercial drivers begins with effective and consistent screening. Therefore, the researchers screened drivers with both the STOP-Bang Questionnaire and the Obstructive Sleep Apnea Evaluation Worksheet (OSAEW) and compared the two tools. Drivers screening positive on the STOP-Bang Questionnaire, OSAEW, and both questionnaires were 28%, 23%, and 13%, respectively. Sleep study referrals were made for 50 drivers; 12 drivers were scheduled for sleep tests within 3 months. Health care provider referral rates for drivers screening at high risk (37%) and commercial driver monitoring rates (24%) were both low. Recommendations to improve OSA screening and testing practices include Federal Motor Carrier Safety Administration–mandated screening and referral guidelines, employee-facilitated sleep testing, and OSA awareness campaigns.
Keywords
Obstructive sleep apnea (OSA) is a disorder characterized by a cessation of breathing during sleep. The airway becomes obstructed when the muscles of the throat become overly relaxed, decreasing support to the soft tissue in the back of the throat. Recognizing a problem, the brain arouses the individual, often resulting in loud snoring, choking, or gasping sounds. This pattern repeats itself, preventing quality sleep (U.S. Department of Health and Human Services [USDHHS], National Heart, Lung and Blood Institute, 2012).
Obstructive sleep apnea may be mild, moderate, or severe, based on the number of times per hour individuals stop breathing or their oxygen levels decrease. Mild OSA is defined as 5 to 14 episodes of apnea hourly. Moderate OSA is apnea that occurs 15 to 29 times per hour. Severe OSA is diagnosed when apnea episodes occur more than 30 times per hour (USDHHS, National Heart, Lung and Blood Institute, 2012).
Individuals at highest risk of OSA are overweight or obese men. Obstructive sleep apnea is associated with, and is perhaps a causative factor for, other chronic health conditions (e.g., hypertension, coronary artery disease, heart failure, and heart arrhythmias). Individuals with OSA may exhibit symptoms of fatigue, nighttime wakefulness, daytime somnolence, and inability to focus mentally (USDHHS, National Heart, Lung and Blood Institute, 2012).
Commercial drivers with undiagnosed and untreated OSA pose a risk of motor vehicle accidents because untreated OSA is known to result in daytime sleepiness and fatigue, as well as impairment of drivers’ judgments and abilities (Garbarino, Nobili, Beelke, De Carli, & Ferrillo, 2001; Kales & Straubel, 2014; Tregear, Reston, Schoelles, & Phillips, 2009). An estimated 15% to 30% of commercial drivers are thought to have undiagnosed and untreated OSA (Kales & Straubel, 2014), which is associated with a 50% greater risk of vehicular accidents (Stoohs, Guilleminault, Itoi, & Dement, 1994). Noncommercial drivers with OSA have also been shown to be involved in more accidents than noncommercial drivers without OSA (Tregear et al., 2009).
For commercial drivers of large vehicles, crashes are more likely to result in fatalities. In 2012 alone, more than 3,000 fatal crashes involved a commercial vehicle. This number represents 12% of all fatal crashes (U.S. Department of Transportation [DOT], Federal Motor Carrier Safety Administration [FMCSA], Office of Analysis, Research, and Technology, 2014). Screening could lead to accurate diagnoses and appropriate treatment for OSA and potentially decrease crashes, injuries, and deaths.
Literature Review and Synthesis
Historically, health care providers screening drivers for OSA asked interview questions about loud snoring or witnessed apnea, as well as fatigue or daytime somnolence. Unfortunately, commercial drivers commonly underreport symptoms, due to the inconvenience and economic implications of additional testing and lost work time (Parks, Durand, Tsismenakis, Vela-Bueno, & Kales, 2009; Talmage, Hudson, Hegmann, & Thiese, 2008). Therefore, questionnaires to screen commercial drivers for OSA should include both subjective and objective data. Specifically, questionnaires should include assessments of body mass index (BMI) and neck circumference, history of hypertension (Talmage et al., 2008), and male gender (Young et al., 1993). Currently, the only two published articles about commercial drivers and screening for OSA used the Epworth Sleepiness Scale (ESS; Johns, 1990) and BMI.
Epworth Sleepiness Scale and Body Mass Index
In 2008, the DOT’s FMCSA accepted recommendations from an expert panel of physicians regarding OSA and commercial drivers’ safety. Experts recommended “actively screening” drivers for OSA, using the ESS and BMI. The ESS is a list of eight situations, for which the driver is asked to rate the likelihood of falling asleep. Talmage et al. (2008) screened 1,443 commercial drivers using the ESS and BMI and found 13% of drivers screened positive and 94.8% of those drivers were later diagnosed with OSA after sleep studies. Of the 127 commercial drivers diagnosed with OSA, 31.5% experienced mild OSA. Moderate and severe OSA was found in 26.8% and 41.7% of drivers, respectively. Fifty-six drivers were lost to long-term contact.
In 2009, Parks et al. (2009) found similar results when using the ESS and BMI. Fifty-three of 456 commercial drivers screened positive (12% of total drivers screened). Thirty-three drivers were lost to continuing contact, but of the 20 drivers who underwent sleep studies, all 20 tested positive. Interestingly, only one driver later demonstrated compliance with treatment.
When an estimated 15% to 30% of commercial drivers have undiagnosed OSA, but the recommended screening tool identifies only 12% to 13% of drivers at high risk of OSA, one must ask whether the ESS and BMI are the most appropriate tools for this population. Alternatives (e.g., Obstructive Sleep Apnea Evaluation Worksheet [OSAEW; U.S. Healthworks, 2015] and STOP-Bang Questionnaire [Chung et al., 2008a]) may be more effective screening tools.
Obstructive Sleep Apnea Evaluation Worksheet
The OSAEW is a company-developed OSA screening tool implemented in the authors’ clinic in May 2015. Although it is not a validated, well-published tool, the OSAEW is composed of various markers of OSA risk. Nine questions are completed by the driver, three of which relate to symptoms of OSA such as loud snoring, fatigue, and observed apnea. Additional information, including BMI, neck circumference, age, comorbidities, and Mallampati class are then measured by a health care provider. Mallampati classification is determined by a visual assessment of the driver’s airway, while the tongue is protruded (Mallampati et al., 1985). Modified Mallampati classes range from I to IV with the soft palate, uvula, and pillars becoming less visible as the class increases (Lamberg & Raghavendra, 2014). Although the Mallampati classification was originally developed as a way of predicting ease of intubation, Nuckton, Glidden, Browner, and Claman (2006) found Mallampati classification to be an independent predictor of OSA. Last, health care providers are instructed to refer for sleep testing anyone who has a BMI more than 35, as well as drivers with BMI less than 35, who show additional risk factors suggestive of OSA.
STOP-Bang Questionnaire
An alternative to the ESS is a validated, well-published OSA screening tool, the STOP-Bang Questionnaire. The STOP-Bang Questionnaire consists of eight questions, each question representing a letter in the word STOP-Bang: S for snoring, T for tired during the day, O for observed apnea during sleep, P for elevated blood pressure, B for elevated BMI, A for age over 50, N for neck circumference greater than 40 cm, and G for male gender. Answering yes to three or more of these questions is considered high risk.
In a systematic review of screening questionnaires for OSA, Abrishami, Khajehdehi, and Chung (2010) found the STOP and STOP-Bang Questionnaires support high-quality methodology and are easy to use. Although originally designed to screen presurgical patients, the STOP-Bang Questionnaire has demonstrated sensitivity of 92.9% for moderate OSA and 100% for severe OSA (Chung et al., 2008b). In addition, the STOP-Bang Questionnaire has a positive predictive value of 51% and a negative predictive value of 90.2% for moderate OSA, and positive predictive value of 31% and negative predictive value of 100% for severe OSA (Chung et al., 2008b). Chung et al. (2012) found that higher scores on the STOP-Bang Questionnaire indicated higher probability of OSA. Unfortunately, the STOP-Bang Questionnaire has not yet been used to identify OSA among commercial drivers.
For this project, all commercial drivers were screened with both the STOP-Bang Questionnaire and the OSAEW simultaneously. Researchers planned to determine the percentage of drivers who screened positive using the STOP-Bang, the percentage of drivers who screened positive using the OSAEW, and the percentage of drivers who screened positive on both tools.
Method
This quality improvement (QI) project was designed to identify a clinical practice problem and possible interventions as well as test interventions for effectiveness.
Setting and Sample
This QI project was implemented at an occupational health practice in southeastern North Carolina. This practice honors contracts with neighboring companies to provide health care for workers who had been injured during work hours. In addition, the practice offers various types of physical examinations, including sports physicals, preplacement physicals, DOT physicals, and Logistics Health Incorporated (LHI) examinations for military reservists and members of the National Guard. Last, the practice can be accessed for urgent care services. The population studied was all commercial vehicle drivers who presented for their DOT physical examinations during project implementation: August 10 through October 10, 2015. Exemption status was granted by Duke Medicine Institutional Review Board on July 21, 2015.
Measures
Outcome measures included provider-completed STOP-Bang Questionnaires and OSAEW as well as the percentage of drivers who screened positive/at high risk on either screening tool, requiring referral for sleep studies. In addition, researchers evaluated the percentage of referred drivers who returned to the clinic within 3 months after completing sleep studies, assessing how many drivers had abnormal sleep study examinations and a diagnosis of OSA.
Intervention
Implementation of the STOP-Bang Questionnaire to screen all commercial drivers began on August 10, 2015 and continued through October 10, 2015. During that period, all drivers were screened by FMCSA-registered medical examiners, using both the STOP-Bang Questionnaire and the OSAEW. Drivers who screened positive on either study were informed of their risk and the implications of untreated OSA, advised to complete a sleep study, and given a 3-month DOT card. A 3-month card allowed drivers time to have sleep testing performed, obtain results, and initiate treatment, if indicated. Once drivers with diagnosed OSA produced a 30-day compliance report that met DOT standards, they receive cards valid for 1 year.
Results
All drivers (N = 382) were screened with the OSAEW, and 369 (97%) were also screened with the STOP-Bang Questionnaire. One hundred sixty-one drivers (44% of all drivers screened) screened positive on the STOP-Bang, the OSAEW, or both. Twenty-three of those positive screens were from drivers who had known OSA and were already being treated; two positive screens were from drivers with previous negative sleep studies, leaving 136 undiagnosed/untested drivers (37% of all DOT drivers screened) with positive screens. As shown in Figure 1, the STOP-Bang produced 103 drivers (28%) with positive screens and the OSAEW produced 84 drivers (23%) with positive screens. Fifty-one drivers (13%) screened positive on both questionnaires.
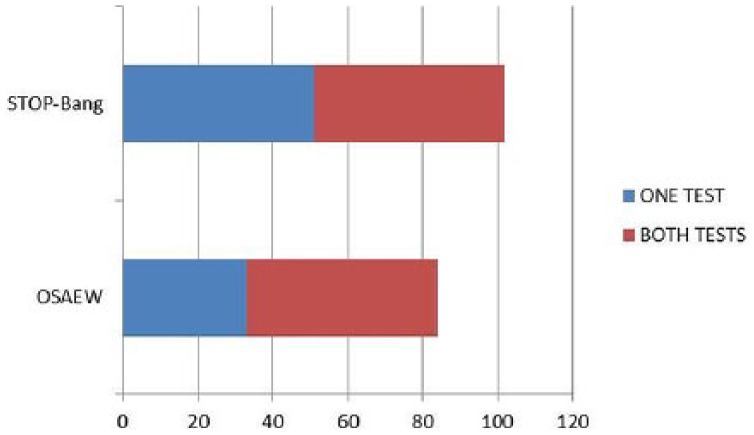
Number of drivers screening positive.
Of the 136 undiagnosed drivers with positive screens, only 50 commercial drivers were referred for sleep testing during project implementation. Of those 50 drivers, 12 drivers (24%) returned to the clinic with completed sleep studies within the 3-month window. Another driver returned to the clinic with a letter from a sleep specialist indicating no need to perform sleep testing, even though his BMI was more than 35. An additional 12 drivers showed evidence of sleep studies pending and were allowed an extension on their DOT cards (i.e., policy related to extending card validity has now changed, but at the time extensions were allowed). Unfortunately, 25 drivers (50% of the drivers referred) were lost to long-term contact.
As Table 1 indicates, 12 drivers did complete sleep testing, of which nine drivers (75%) tested positive for OSA. Of these nine drivers, three drivers (33%) were found to have mild OSA, four drivers (44%) moderate OSA, and only one driver (11%) severe OSA. One driver returned with a compliance report only, not the actual sleep study; therefore, his degree of OSA is unknown. The remaining three drivers tested negative or low risk.
Summary of Referred Drivers
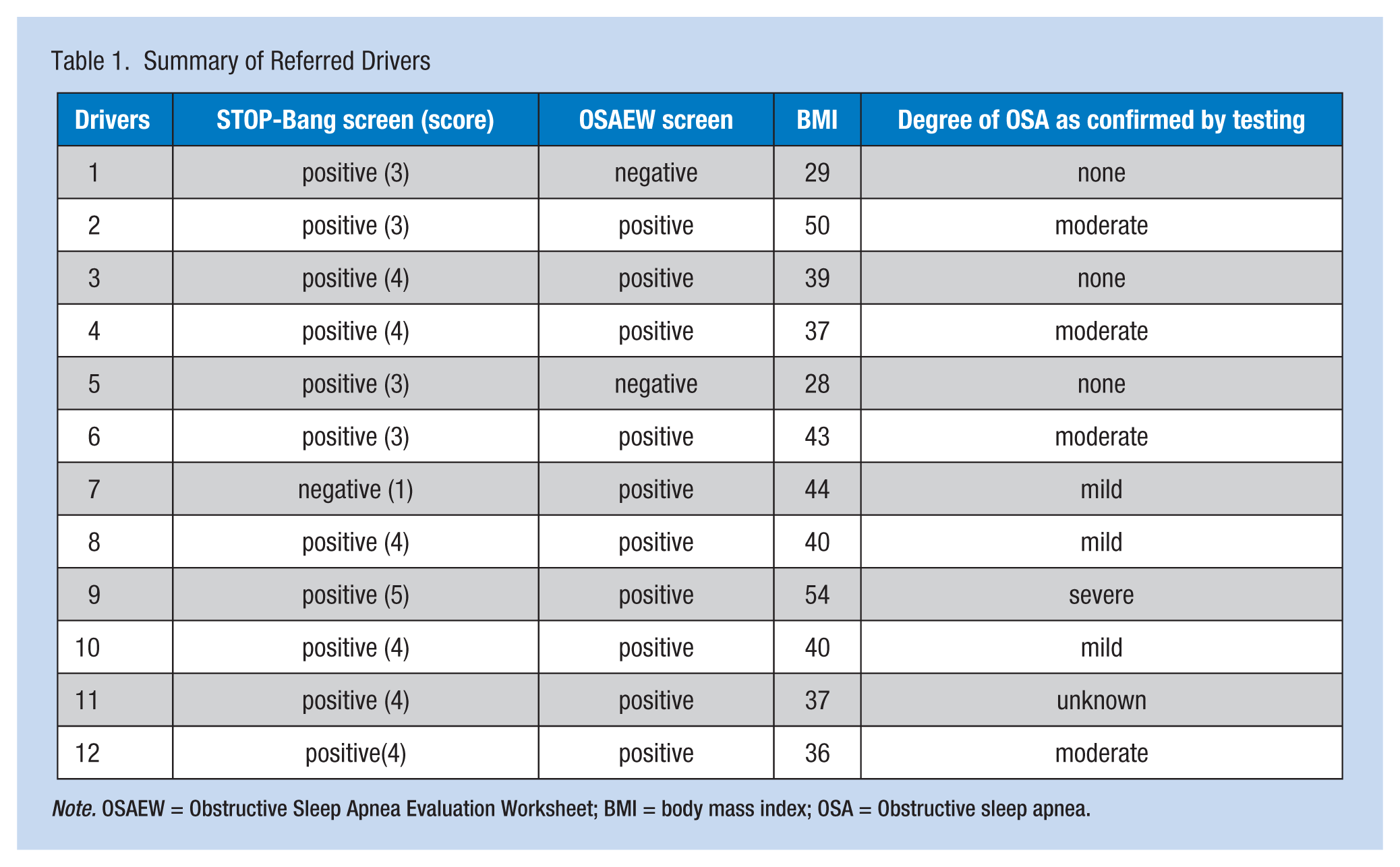
Note. OSAEW = Obstructive Sleep Apnea Evaluation Worksheet; BMI = body mass index; OSA = Obstructive sleep apnea.
Of the four referred drivers who screened positive on the STOP-Bang Questionnaire, but negative on the OSAEW, only two returned to the clinic following sleep studies. Both of those drivers had OSA risk profiles that included: male, more than 50 years of age, and history of hypertension. Both drivers’ sleep studies were negative.
Discussion
Researchers met the aims of this project: to implement the STOP-Bang Questionnaire to screen commercial drivers for OSA. Without additional benefit to practice, the clinic will continue to use the OSAEW. However, the more impressive issues uncovered by this study were (a) the reluctance of health care providers to refer for sleep testing those commercial drivers who screened high risk and (b) the reluctance of commercial drivers to cooperate with sleep testing and continuing contact.
Barriers to Provider Referral
Only 37% of the commercial drivers who screened high risk were referred for sleep testing. A review of provider feedback written on the screening forms indicated missed referrals due to BMI less than or close to 35, younger age, Mallampati class I or II, or lack of symptoms. Similarly, Parks et al. (2009) found a referral rate of 68% among their high-risk screens. The health care providers in their study indicated no referral necessary when hypertension was controlled or when symptoms occurred in isolated episodes.
Additional informal verbal feedback from providers included feelings of tension and stress when drivers made negative comments directed at the health care provider. Parks et al. (2009) also “experienced significant concern and even anger from some drivers, as well as some employers” (p. 280) when sleep testing referrals were made. Indeed, Durand and Kales (2009) found client retention and driver inconvenience to be among the reasons medical examiners declined screening (and subsequent referral) for OSA.
Barriers to Scheduling Sleep Studies
Many of the commercial drivers referred for sleep testing indicated no plans to actually have the sleep study done, primarily because they had no symptoms or because they no longer drive commercially and plan to let their commercial driver’s license (CDL) expire. Unfortunately, only 24% of commercial drivers returned to the clinic with completed sleep studies within 3 months. For comparison, Parks et al. (2009) had a 62% driver monitoring rate and Talmage et al. (2008) had a 71% driver monitoring rate. Talmage et al. (2008) found the primary barriers to long-term contact to be cost and lack of adequate insurance coverage. Rather than scheduling the sleep study, these drivers simply declined employment with the motor carrier who had requested the new DOT physical examination. Indeed, commercial drivers know they can have another DOT physical examination performed elsewhere, with registered medical examiners who adhere to different standards, a practice providers commonly call doctor shopping.
Recommendations for Quality Improvement
To improve provider compliance with referrals, as well as driver compliance with sleep testing, Parks et al. (2009) suggested the FMCSA standardize OSA screening and referral practices to prevent doctor shopping, as all providers would be working under the same guidelines. According to Durand and Kales (2009), fear of losing clients is a concern for examiners, causing them to forgo OSA screening and sleep test referrals. Unfortunately, barriers to FMCSA federal mandates are complex and “stem from politics, finances, liability, and legal concerns” (Zhang, Berger, Malhotra, & Kales, 2012, p. 1482).
Another recommendation from Parks et al. (2009) was employer-funded sleep testing. As cost and lack of health insurance are barriers to sleep testing for many drivers, employer-funded sleep studies could overcome these barriers. Unfortunately, a clear cost benefit to sleep testing is difficult to establish. Therefore, few employers currently fund sleep testing for their drivers. To curb costs, employers choose alternatives to standard referral and in-lab sleep testing, including mandatory online questionnaires to establish drivers’ risks, followed by employee-funded sleep testing (Berger et al., 2012) or at-home overnight monitoring (Zhang et al., 2012). From a mandatory online questionnaire followed by an employee-funded in-lab sleep test, Berger et al. (2012) established a 21% OSA rate among the drivers they studied. Alternatively, at-home OSA testing is more convenient and costs less. However, researchers question the validity of portable monitoring for commercial drivers, primarily related to data loss and lack of physician interpretation protocols (Zhang et al., 2012).
Last, OSA awareness campaigns could educate drivers and employers, as well as health care providers (Parks et al., 2009). Durand and Kales (2009) recommended education strategies for health care providers regarding OSA and driver safety, when their 2009 survey of health care providers indicated lack of knowledge was the primary reason for not properly screening drivers for OSA. Furthermore, Healthy People 2020 (2014) set a goal to increase public awareness of OSA, advising treatment for sleep disorders to improve health and wellness as well as safety on the roads.
This project used a small sample size, which limits generalizability.
Both the STOP-Bang Questionnaire and the OSAEW were useful tools for OSA screening of commercial drivers. However, screening drivers is useful only when drivers found to be at high risk are referred for sleep testing and drivers actually schedule sleep tests. The real problem is the overall inconsistency of provider referrals (37%) and commercial driver sleep testing (24%). Barriers to consistent, standardized provider referrals include concerns over losing business from doctor shopping, potential for angering drivers, and lack of physical driver characteristics typically noted in OSA. Barriers to driver sleep testing are cost and lack of health insurance as well as lack of recognizable symptoms. Recommendations to remove these barriers include clear FMCSA screening and referral guidelines, employer-facilitated and employer-funded sleep testing, and OSA awareness campaigns directed toward drivers, employers, and medical examiners.
In Summary
Commercial drivers with untreated obstructive sleep apnea (OSA) are at a 50% increased crash risk.
Screening drivers for OSA should include both interview questions and a physical exam measuring body mass index, Mallipatti class, blood pressure, and neck circumference.
Lack of sleep study referrals and lack of driver testing likely leaves many drivers with undiagnosed and untreated OSA still driving professionally.
Standardized OSA screening of all commercial drivers, educating drivers and employers about crash risk, and employer-financed sleep testing may result in more drivers screened and tested for OSA.
Footnotes
Acknowledgements
Dr. Whitmer was the onsite, subject matter expert and was instrumental in the early stages of this project. Unfortunately, he passed away before project completion. He deserves special thanks and is sorely missed.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Kelly A. Evans is an occupation health nurse practitioner, Southern Regional AHEC, Fayetteville, NC.
Tracey Yap is an associate professor at the Duke University School of Nursing.
Barbara Turner is an Elizabeth P. Hanes professor of nursing and chair of the Health of Women, Children, and Families Division of the Duke University School of Nursing.