
Abstract
Background:
There are strong links between obstructive sleep apnea (OSA), chronic disease, mental health, job performance, and motor vehicle accidents. Corporate wellness clinics and health monitoring programs present ideal settings to educate and screen employees for OSA.
Methods:
In January 2020, the Stop-Bang Sleep Apnea Questionnaire was added to the yearly health monitoring program of 571 State of Texas air, water, and hazardous waste workers as part of routine care. Medium- and high-risk (HR) scoring employees were counseled to seek follow-up care from a primary-care provider (PCP). The January 2021 exams provided an opportunity to determine the success of counseling efforts.
Findings:
Of the 479 returning employees in 2021, 24 (49%) of HR and 17 (21.8%) of intermediate risk (IR) had discussed OSA with a PCP. Seven (14.3%) HR and 1 (<1%) IR employee underwent a sleep study and 4 (8.2%) were prescribed continuous positive airway pressure (CPAP).
Conclusions/Application to Practice:
Screening for OSA at the workplace was inexpensive and, when diagnosed and treated, can mitigate associated chronic disease, improve worker productivity, and reduce associated accidents and injuries. The described OSA screening delivered value to the employer and employees. The screening was performed at a very low cost, involved little time on the part of the nurse practitioner and employees, brought signs and symptoms of OSA to the consciousness level of 571 employees, encouraged at-risk participants to discuss OSA with a PCP and led to 4 (8.2%) being prescribed CPAP.
Background
Sleep is one of the most vital human functions necessary to maintain a positive state of health. Quality of life, physical and mental health, and safety in the workplace are directly linked to the amount and quality of sleep an individual obtains. Regardless, many individuals are sleep deficient. Sleep deficiency, as defined by the National Heart, Lung, and Blood Institute (2021) occurs when there are insufficient types or quantity of sleep, or a disorder is present, such as obstructive sleep apnea (OSA). Contributing factors to sleep deficiency involve work schedules/shift duration/work intensity and/or the presence of health conditions, including diabetes, atrial fibrillation, obesity, heart failure, depression, gastroesophageal reflux, asthma, or dementia (Gottlieb & Punjabi, 2020). The prevalence of OSA in patients with hypertension, heart failure, coronary artery disease, pulmonary hypertension, atrial fibrillation, or stroke is as high as 40% to 80% (Yeghiazarians et al., 2021).
Sleep deficiency is responsible for absenteeism, diminished productivity, increased health care costs, accidents, and other occupational costs associated with exhausted employees, many of whom have undiagnosed and untreated sleep disorders. Regardless, screenings for sleep disorders in the workplace are rarely performed (Roy, 2017).
Liu et al. (2020) defined OSA as a respiratory disorder characterized by repetitive episodes of upper airway obstruction caused by partial or complete collapse of the upper airway. Prevalence rates of OSA in the general population widely vary depending on the research. Garbarino et al. (2018) reported that the prevalence of OSA is 3% to 7% in adult men and 2% to 5% in adult women with expected future increases as the population ages and gains weight. Peppard et al. (2013) reported the prevalence of OSA was a mean of 22% in men and 17% in women in 11 epidemiological studies published between 1993 and 2013. OSA with excessive daytime sleepiness occurred in 6% of men and in 4% of women. Interestingly, the prevalence increased over time and OSA was reported in 37% of men and in 50% of women in studies from 2008 and 2013, respectively. The American Academy of Sleep Medicine estimated that the increased prevalence rates of OSA over the last 20 years is related to the obesity epidemic. Furthermore, AASM estimates 26% of adults between 30 and 70 years have OSA. Finally, and more recently, Yeghiazarians et al. (2021) indicated that approximately 34% and 17% of middle-aged men and women, respectively, meet the diagnostic criteria for OSA.
Motamedi et al. (2009) believed more than 85% of patients with clinically significant OSA have never been diagnosed. Underdiagnosis may be the result of patients not being aware of their snoring or nocturnal awakenings. Principal features of OSA include signs of disturbed sleep, such as snoring and restlessness, interruptions of regular respiratory patterns during sleep, and daytime symptoms, such as fatigue or trouble concentrating that are attributable to disrupted sleep patterns at night.
Regardless of the cause, health consequences are significant. Tasali et al. (2008) found less than 5 hours of sleep per night results in a three-fold increased risk for type-2 diabetes mellitus, a less-active immune system, increased colorectal cancer rates, cardiovascular disease, hypertension, dementia risk, and obesity. The incidence of heart disease, diabetes, obesity, and even COVID-19 are amplified. Tasali et al. (2008) also indicated the majority of patients with type-2 diabetes have OSA. Independent of sociodemographic, behavioral, cardiometabolic, and mental health factors, Sabia et al. (2021) found a 30% increase in dementia among 50, 60, and 70-year olds with persistent short sleep duration—less than 6 hours per night.
Most recently, after adjusting for age, sex, and other risk factors, such as diabetes, obesity, heart disease, and hypertension, Finnish researchers (Strausz et al., 2021) found OSA patients had the same risk of contracting COVID-19 as non-OSA individuals. However, the authors found that OSA carried a higher risk for severe COVID-19. For example, OSA patients who contracted COVID-19 had a five-fold hospitalization rate compared to non-OSA individuals.
Sleep deprivation and OSA in the occupational setting present significant concerns, including lost work productivity, automobile/truck accidents, impaired mental and motor skills, poor decision-making with increased risk taking, and lost productivity (AASM, 2014). The AASM (2014) estimates the annual cost of sleep-related workplace accidents and mistakes at $31 billion and 26% of adults between the ages of 30 and 70 have sleep apnea. While the workplace is an ideal setting to screen for OSA, few employers do so unless mandated by law or agencies such as the Federal Motor Carrier Safety Administration (FMCSA).
Berger et al. (2012) described an employer-based sleep apnea screening and diagnosis study conducted among 19,371 commercial truck drivers. Employees from several employers were mandated to complete an on-line proprietary screening tool (SomniSage). Based on scores, each employee was assigned to an OSA high-risk (HR) or low-risk group. Screening results were referred to the employers who subsequently encouraged drivers in the HR group to seek further testing via a polysomnogram (PSG). Results showed of the 19,371 screened employees 5,908 (30%) were at HR for OSA. Among individuals in the HR group, 2,103 (35.6%) chose to be tested with a PSG. Endpoints of the PSG testing of the HR group revealed 1,424 (67.7%) individuals tested positive for OSA, 253 (12%) possibly had OSA, and 426 (20.3%) were negative for OSA.
Karimi et al. (2015) found the motor vehicle accident risk ratio was 2.45 higher in patients with OSA than controls and most prominent in elderly patients 65 to 80 years old. With the use of continuous positive airway pressure (CPAP) >4 hours/night, there was significant reduction (7.6 to 2.5) in accidents.
Burks et al. (2016) evaluated the effect of an employer mandated OSA program on the risk of serious preventable truck accidents. In a retrospective study, 1,613 truck drivers diagnosed with OSA were matched with 403 non-OSA drivers, who served as the control group. The authors monitored the use of CPAP machines for full adherence (n = 682), partial adherence (n = 571), or no adherence (n = 360). Results showed that the no adherence group had an accident rate five times greater than the control group. The full adherence group accident rate was equal to the matched controls.
Ononye et al. (2019) conducted a study on screening for OSA in a primary care setting with the intent to evaluate and refer patients as needed. Prior to conducting the study, only 3% of patients were screened and 0% were referred. Of the 187 patients screened, 114 (61%) scored moderate to severe on the STOP-Bang questionnaire, and 45 (39%) of the moderate to severe patients went on to receive a PSG. Thirty (67%) of the 45 patients with moderate to severe questionnaire results were actually diagnosed with OSA resulting in a cohort (187) positivity percentage of 16%. Such positive findings are a strong indication that screening for OSA in the primary care setting yields significant new diagnosis of OSA. The 67% specificity of the STOP-Bang questionnaire results in the Ononye et al. (2019) study is lower than findings by Chung et al. (2014). Chung et al. (2014) showed a sensitivity and specificity for identifying moderate–severe OSA of 87% and 31%, respectively.
The purposes of this multiphased project were to screen an adult working population for OSA during annual health monitoring examinations, educate individuals at risk, recommend primary-care provider (PCP) follow-up when appropriate and, 1 year later, determine whether individuals actually followed up with the PCP and, if needed, received testing and treatment.
Methods
The project screened and educated 571 environmental health field workers for OSA with the STOP-Bang questionnaire during routine health monitoring exams. Medium and HR scoring employees were counseled to seek follow-up care from a PCP. Data were gathered between January 2020 and April 2021. The program population, as described elsewhere (Mackey, 2019), comprised State of Texas environmental air, water, and waste disposal workers. Annual health monitoring exams were required by the State of Texas for all field investigators to determine fitness for duty and detect undiagnosed work-related illnesses. Employees range in age from 21 to 75 years, receive full health insurance benefits, have incomes between $35,000 to $80,000, and are employed on a full-time basis.
Screening Tool
In response to the serious nature of OSA various state, federal and national organizations have guidelines/recommendations related to screening. For example, the United States Preventive Services Task Force (USPSTF, 2017) found insufficient evidence to screen for OSA in asymptomatic adults or individuals with unrecognized symptoms.
Qaseem et al. (2014) developed two guidelines for OSA screening for the American College of Physicians (ACP). Both were weak recommendations with low to moderate quality evidence: a sleep study for patients with unexplained daytime sleepiness and a polysomnography (PSG) for diagnostic testing in patients suspected of OSA. Without significant comorbidities, the ACP recommends portable sleep monitors as an alternative if PSG is not available for diagnostic testing. The FMCSA (2015) issued recommendations on OSA screening for medical examiners. Recommendations include requiring diagnostic evaluations on drivers with a body mass index of 35 or higher and immediate disqualification for persons with excessive sleepiness while driving, who have experienced a crash associated with falling asleep, have an apnea-hypopnea index (AHI) greater than 20, have undergone surgery and are pending the findings of a postoperative evaluation and have been noncompliant with treatment for OSA.
Amra et al. (2018) performed an extensive literature review of articles published on OSA screening questionnaires between 2010 and 2017. Among four validated screening tools evaluated the STOP-Bang Questionnaire was the most sensitive for detecting mild and severe OSA. The anacronym STOP-Bang represents snoring, tired during the day, observed apnea during sleep, elevated blood pressure, elevated body mass index, age over 50, neck circumference >40, and male gender. Positive answers for three or more questions are considered intermediate (3–4) or high (5–8) risk (Evans et al., 2017).
Suniega El Thoma et al. (2019) describes the same screening tools reporting poor sensitivity with the ESS and 76% to 77% on the Berlin Questionnaire. The STOP-Bang questionnaire had a sensitivity of 83.6% to 100% for mild, moderate, and severe OSA. The STOP-Bang questionnaire (see Figure 1) was chosen for this study because of the simplicity of administration (eight questions) and high sensitivity reported in the literature.
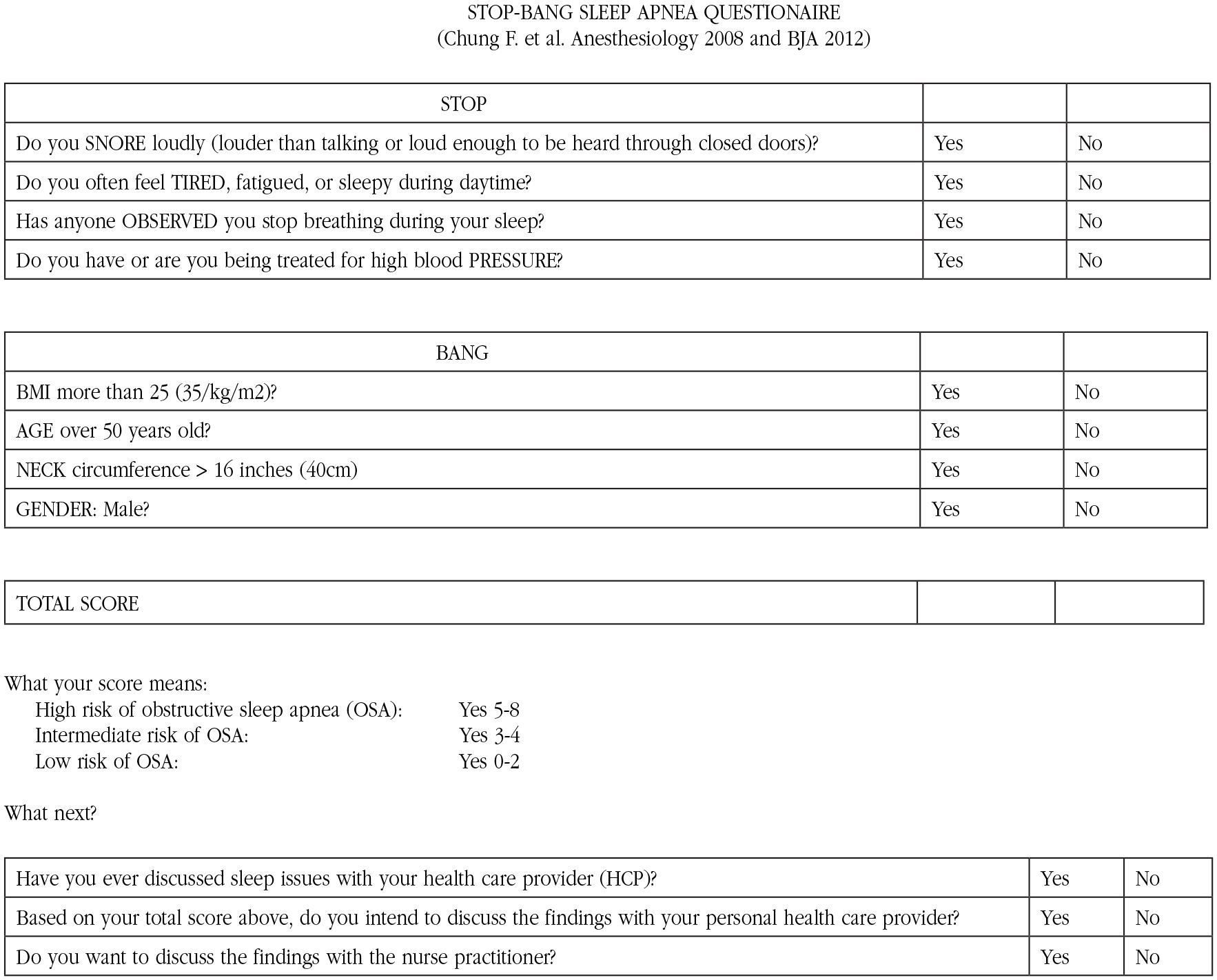
This is a screening tool for sleep apnea and is not a mandatory part of your health monitoring exam.
Initial Data Collection
Using the STOP-Band questionnaire data were gathered between January 2020 and April 2021. The program population, as described elsewhere (Mackey, 2019), comprised State of Texas environmental air, water, and waste disposal workers. Annual health monitoring exams are required by the State of Texas for all field investigators to determine fitness for duty and detect undiagnosed work-related illnesses. While all employees drive company-owned vehicles, none are required to possess a commercial driver’s license. Therefore, screening for sleep apnea was not required. Field investigators’ job duties included driving cars and trucks for distances up to 8 hours a day. Consequently, falling asleep due to OSA while driving can be a significant issue. Employees ranged in age from 21 to 75 years, received full health insurance benefits, have incomes between $35,000 to $80,000, and are employed on a full-time basis. Each year, the health monitoring exams included complete work and personal health history, vital signs, chest X-ray, spirometry, electrocardiography, audiometry, laboratory work (complete blood count, 24 chemistries, lipids, cholinesterase, and lead levels), workplace-appropriate immunizations, a physical examination, and a consultation with a nurse practitioner (NP). Most years the NP adds additional screening (cardiovascular risks, smoking, and skin cancer prevention) related to some primary care or work-related issue. In 2020, the NP added screening for OSA via the STOP-Bang questionnaire (see Figure 1). During the exam process, the NP assessed the completed STOP-Bang questionnaire and if the employee’s score was three or greater asked additional questions: (a) Have you ever discussed sleep issues with your health care provider? (2) Based on your total score above, do you intend to discuss the findings with your personal health care provider? and (3) Do you want to discuss the findings with the NP? The NP was not an employee of the company and therefore unable to make direct referrals for further OSA testing.
In 2020, the NP discussed the STOP-Bang questionnaire results with each participant and made appropriate recommendations based on scoring. Intermediate risk (IR) and HR scorers (see Figure 1) received education related to OSA and a recommendation to see a PCP for further discussion and, if needed, testing. Regardless, any employee scoring in the IR or HR categories was provided further information on OSA by the NP.
Since screening for OSA with the STOP-Bang instrument was part of the NP routine care no consent forms or Institutional Review Board (IRB) approval were indicated. As with other parts of the examination (spirometry and chest X-ray) workers could choose to decline participation in the OSA screening.
Additional Follow-Up
The 2021 exams provided an opportunity for the NP to follow-up with individuals scoring in the IR and HR categories who had been recommended to see a PCP. The NP asked follow-up questions (see Figure 2) to determine if employees heeded the advice given during the 2020 exam. The questions included: Did you discuss OSA with your PCP? Did your PCP recommend a sleep study? Did you get a sleep study? Were you prescribed CPAP? Are you using CPAP now >4 hours/night?
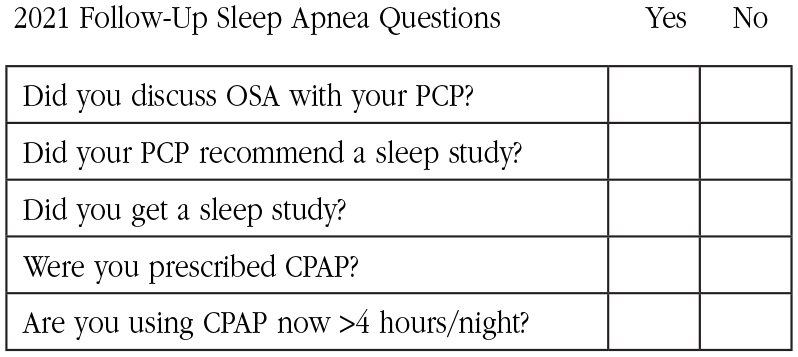
Follow up screening questions.
Findings
The screening was performed at a very low cost, involved little time on the part of the NP or employee, raised 571 employees’ awareness of OSA, resulted in 24 HR and 17 IR employees discussing OSA with a PCP, and 7 HR and 1 IR completing a sleep study with four prescribed and using CPAP.
The 2020 initial screening was performed on 571 employees between the ages of 21 and 75 years: 297 males and 274 females and 194 above the age of 45. Of the 571 employees screened (Table 1), 97 scored in the HR category (score of 5–8) for OSA, 115 scored in the IR category, and 359 scored in the low-risk category. Of the 571 screened, 110 had previously discussed OSA with a PCP. However, after the screening, 159 indicated an intent to have a discussion. A small proportion of the screened population already used CPAP and were not included in the results reported. When prompted with a question about discussing OSA with the NP at the end of the exam, 226 voiced an interest.
2020 Sleep Apnea Screening Results (N = 571)
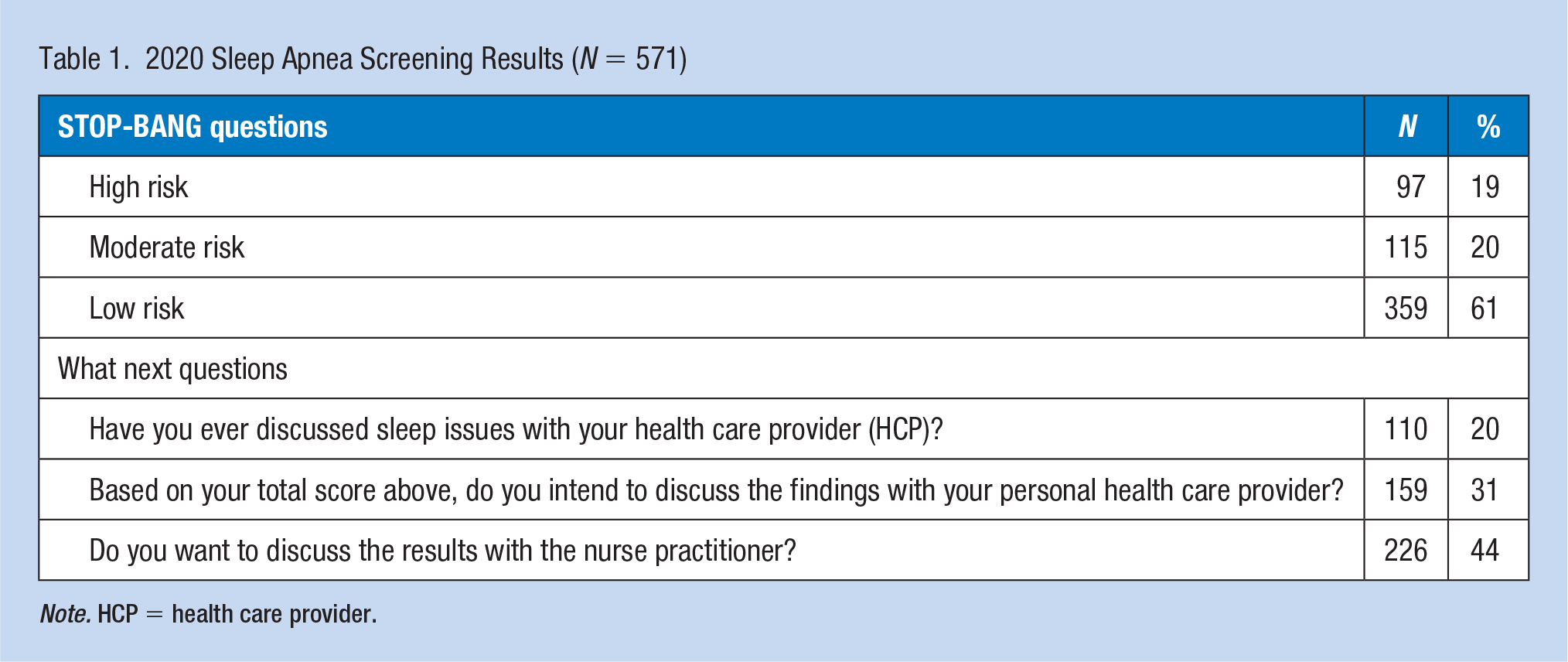
Note. HCP = health care provider.
Employees could opt to decline the health monitoring exam in 2021 owing to COVID-19 precautions. Consequently, for the 479 employees who did return in 2021, a follow-up questionnaire was conducted on 49 HR and 78 IR (n = 127) individuals from 2020. Thus, 127 individuals were asked a series of five follow-up questions (Table 2). When asked “Did you discuss OSA with your PCP?” 17 of the IR and 24 of the HR individuals responded affirmatively. The PCP recommended three of the IR individuals receive further testing while 22 of the HR persons were advised to schedule a sleep study. Only one of the IR and seven of the HR employees obtained an OSA study. No individuals in the IR and only four in the HR group were prescribed or using CPAP. Collectively, four individuals were prescribed and using CPAP based on the NP’s 2020 recommendation to discuss the issue with a PCP and pursue further diagnostic testing during the health monitoring examination.
2021 Follow-Up Sleep Apnea Questions (N = 127)
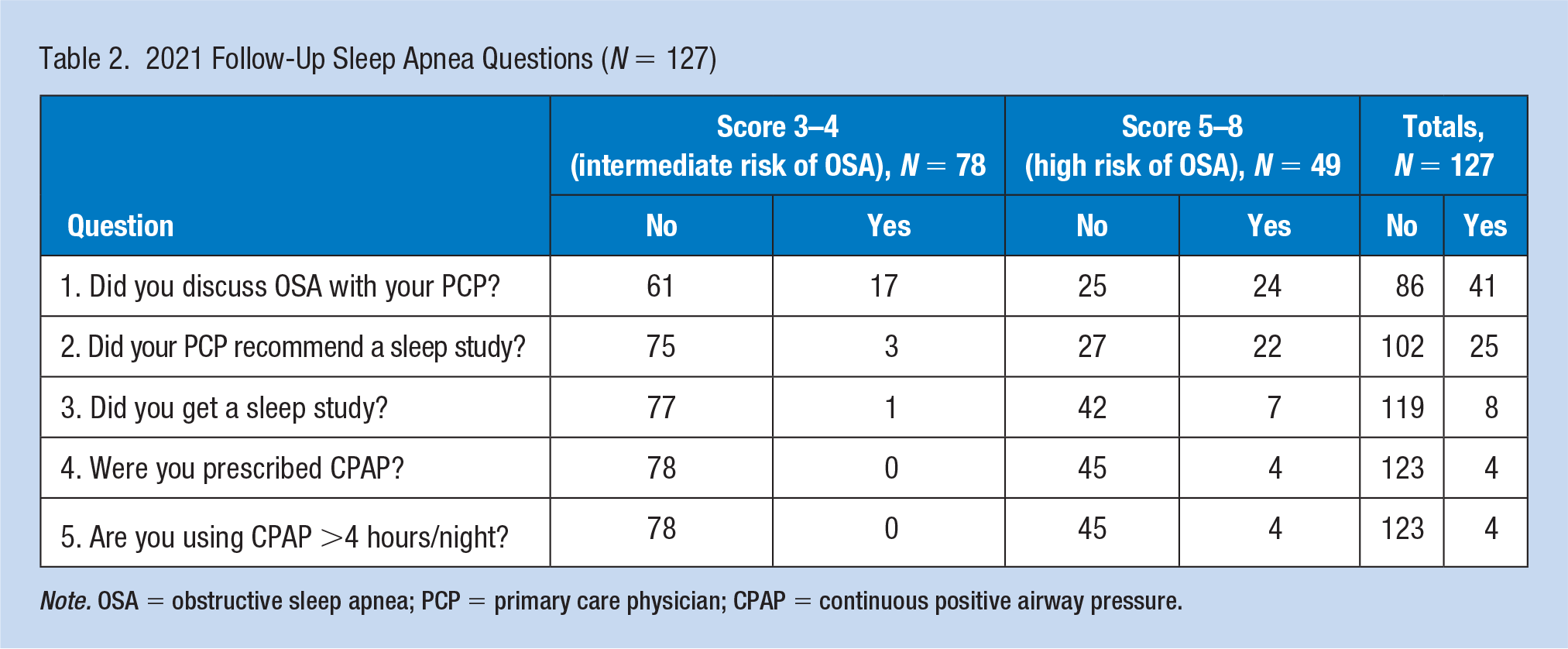
Note. OSA = obstructive sleep apnea; PCP = primary care physician; CPAP = continuous positive airway pressure.
The years 2020 and 2021 presented unprecedented challenges due to the COVID-19 pandemic. Employees screened indicated interpersonal contact was limited, and routine matters such as seeking advice from a health care provider diminished. Consequently, many employees referred to a PCP by the NP may have decided to avoid contact with the health care system despite possible benefits. The most frequent reason given for not following up with a PCP related to the restrictions as well as an inability to make an appointment and/or travel to a medical office. Several participants indicated follow-up was not possible but intended to have a discussion with their PCP during the next visit.
In addition, employees could opt to forgo health monitoring in 2021 due to COVID-19 precautions. As a result, many employees who scored in the HR and IR categories in 2020 did not return in 2021. Several employees in the two categories who did return but had not spoken with a PCP about their high score indicated they had no opportunity during the year to visit with a health care provider.
Jackson et al. (2017) indicated the prevalence of OSA in the general population in 2014 was 8.1%. The current program used the STOP-Bang questionnaire to screen for OSA in a working population. The questionnaire was not intended to make a diagnosis but simply to screen. Regardless, the STOP-Bang questionnaire had a sensitivity of 83.6% to 100% for mild, moderate, and severe OSA (Suniega El Thoma et al., 2019). A total of 49 HR individuals returned in 2021 for follow-up, yet only four had received a diagnosis of OSA (Table 2). Even at the low end of sensitivity (83.6%), the expected number of OSA cases in the current population would be 41.
In a previous study, Berger et al. (2012) found 30% of 19,371 employees tested were at HR for OSA and chose to be further tested for OSA. Of those tested, 67.7% were confirmed to have OSA, 12% possibly had OSA, and 20.3% had negative results. Based on a 67.7% positivity rate, the expected number of positive OSA cases in this screening would be 12.9. The 2021 follow-up only yielded four confirmed new OSA diagnoses. The unexpected low yield may be a result of employees opting out of the exam and a lack of follow-up with a PCP due to COVID restrictions.
Discussion
The purposes of the project were to screen an adult working population for OSA during annual health monitoring examinations, educate individuals at risk, recommend further diagnostic screening when appropriate and, one year later, determine whether diagnostic screening was actually performed. The health monitoring process has been the same every year and made it relatively simple to add OSA screening and accomplish the stated study purposes.
Evans et al. (2017) screened 369 commercial drivers with the STOP-Bang questionnaire and found 103 (37%) to be positive. Fifty drivers were referred, but only 12 (24%) scheduled a sleep study within a 3-month period of time. The current project screened 571 and found 41 (7.1%) to be positive—all of whom were referred for discussion with a PCP. Of the 41 referred, only eight (19.5%) actually completed a sleep study, while four were prescribed CPAP. The difference in screening rates may be due to the populations screened. Evans et al. (2017) screened commercial drivers who had a screening mandate while this study screened noncommercial drivers without an obligation.
Zhang et al. (2012) discussed multiple barriers to OSA screening including politics, finances, liability, and legal concerns. Talmage et al. (2008) added the issues of time, costs, and simple inconvenience as barriers to screening. Consequently, the low rates of follow-up with a PCP and completion of obtaining a sleep study were not surprising. The year 2020 and 2021 suffered an additional barrier—COVID-19. Many individuals reported a lack of follow-up with a PCP because of COVID-19 restrictions. The COVID-19 quarantine and fear of going to a medical office were reasons given for a lack of follow-up. Thus, some results may be skewed because of the pandemic and further limit the project outcomes.
Other study limitations included the population selected and provider performing the screenings. There were no employment consequences for the lack of follow through with a referral as may have occurred with commercial truck drivers who were required to be screened and tested. The same NP administered the health monitoring exams for many years. Consequently, familiarity with employees may have influenced the results in one direction or another. Sudhakar-Krishnan and Rudolf (2007) suggested continuity of providers contributed to better compliance with medical recommendations. Other settings without a known provider or continuity could yield different results.
Screening programs are often judged on worth and value. Worth refers to the financial benefit/gain to an individual or organization. Value, on the contrary, refers to issues other than direct patient care and include quality, health care system savings, and even patient relationships (Mackey, 2009). The present OSA screening program delivered value to the employer and employees. The cost to screen and educate 571 employees about OSA was minimal. The NP and employees’ time were the only significant resources involved. On the contrary, costs associated with untreated OSA compared to those without OSA are doubled. Effective treatment of OSA can significantly reduce health expenditures and motor vehicle accidents to that of drivers without OSA (Berger et al., 2012).
This low-cost study was useful to identify OSA in the selected population. When screened and counseled to follow-up for possible OSA, the current screening program did not persuade the majority of at-risk employees to seek further testing from PCPs. These low-yield positive diagnostic findings were probably attributed to societal restrictions related to COVID-19 as many HR and IR employees avoided visits to PCPs for follow-up testing. Regardless, there was significant value to employees and employers in providing a brief intervention and educating at-risk employees regarding the need for further screening.
Application to Professional Practice
Screening for OSA at the workplace is inexpensive and, when diagnosed and treated, can mitigate associated chronic disease, improve worker productivity, and reduce associated accidents and injuries. The present OSA screen delivered value to the employer and employees. The screening was performed at a very low cost, involved little time on the part of the nurse practitioner and employees, brought OSA to the consciousness level of 571 employees, resulted in eight persons getting a sleep study and four with a confirmed diagnosis and prescribed CPAP.
Footnotes
Author’s Note
The paper is a program evaluation of routine care. Human subjects review was not required.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Dr. Thomas A. Mackey is professor of clinical nursing in the Cizik School of Nursing at the University of Texas Health Science Center at Houston, former Associate Dean for Practice and Director of the University of Texas Health Services.