
Abstract
Introduction:
Tobacco is the leading modifiable risk factor for cancer and other chronic diseases. The workplace provides an opportunity to advance tobacco cessation efforts. Combining tobacco cessation with complementary components addressing mental health, physical activity, and healthy eating has demonstrated effectiveness in non-workplace settings. This scoping review examines the literature on multicomponent workplace tobacco cessation interventions to identify core components and implementation facilitators and barriers to support uptake in the workplace setting.
Methods:
A scoping review was conducted following PRISMA guidelines for Scoping Reviews and Arksey and O’Malley’s five-step process. Peer-reviewed literature published in the past 20 years was searched across 9 databases. A search for relevant gray literature (i.e., conference papers/proceedings) was also completed. Articles were screened by two independent researchers for inclusion. Included studies evaluated workplace interventions recruiting individuals to participate in a tobacco cessation program alongside a complementary component (i.e., physical activity, mental health, healthy eating).
Results:
Most of the 12 included studies paired tobacco cessation with mental health or stress reduction interventions. Most complementary components targeted the individual versus organizational or policy levels. The synthesized facilitators indicated that multicomponent interventions should be incentivized and tailored to adequately meet the needs of different workplaces and employees.
Discussion:
This scoping review synthesizes studies integrating multiple complementary program components into workplace tobacco cessation efforts. Future interventions should implement tobacco cessation interventions at multiple levels, combining complementary components to maximize effectiveness and overcome barriers (e.g., weight gain and stress) to successful outcomes.
Introduction
Tobacco use is the leading modifiable risk factor for cancer and other chronic diseases (Islami et al., 2018; World Health Organization [WHO], 2009, 2020). In 2003, the Member States of the WHO made a commitment to reducing tobacco use by adopting the WHO Framework Convention on Tobacco Control (WHO, 2003). Globally, government-led actions have led to declines in tobacco use over the last two decades (WHO, 2024). However, member states are still not on track to meet the WHO global target of a 30% reduction of tobacco use among people aged 15 or older by 2025, with the reduction calculated relative to each country’s 2010 tobacco use prevalence (WHO, 2013).
The WHO recommends taking a settings-based approach to tobacco cessation by designing and implementing tobacco cessation programs in the places where individuals live, work, learn, and seek health care (World Health Organization, 2003; 2024). The workplace is particularly underutilized for tobacco cessation efforts and present opportunities to implement health promotion activities for diverse populations, including subpopulations that are difficult to engage through traditional health promotion activities (Ayaz et al., 2024; Goetzel & Ozminkowski, 2008; Upson, 2015; WHO, 2010). Workplaces also provide access to large and relatively stable populations (Organisation for Economic Co-operation and Development, n.d.). Furthermore, workplaces have higher tobacco cessation participation rates than other settings and allow for peer group support, access to professional support through occupational health staff, and reduced participation costs (Cahill & Lancaster, 2014).
Workplace environments can be health-promoting or constraining as they directly influence the physical, mental, economic, and social well-being of individual employees (Goetzel et al., 2014). For example, employment in a workplace with a poor psychosocial environment is associated with heavier tobacco use (Dobson et al., 2018). Studies suggest that employees experiencing job strain were more likely to smoke tobacco and smoke more cigarettes than those not experiencing job strain (Habibi et al., 2015; Heikkilä et al., 2012; Khorrami et al., 2021).
Neither tobacco use nor cessation efforts should be viewed in isolation from the complex system of factors in which they occur. Research demonstrates support for implementing multilevel tobacco cessation approaches that go beyond targeting just individual and interpersonal levels (Asfar et al., 2021). It is also important to consider community, institutional, and policy-level factors that contribute to tobacco use among individuals. Multiple authors have proposed that individual-level disparities in tobacco use may be due to a stress-mediated pathway between institutional, community, or structural determinants and increased tobacco use (Drope et al., 2018; Heikkilä et al., 2012; Parnia & Siddiqi, 2020; Sorensen et al., 2004; U.S. National Cancer Institute, 2017). Addressing environmental and social factors in workplaces that create conditions leading to job stress and poor mental health of individual employees may help reduce individual-level disparities in tobacco use.
Multicomponent interventions (i.e., interventions that combine a group of health promotion activities) have also demonstrated effectiveness in reducing tobacco use in the workplace (Mache et al., 2019). For instance, mental health and stress, as discussed earlier, must be considered in the intervention design to help support employees’ attempts to quit using tobacco and maintain abstinence. Multiple researchers have also identified the importance of addressing weight gain, particularly among women who are trying to quit smoking (Hartmann-Boyce et al., 2021; Levine et al., 2010; Perkins et al., 2001; Shang et al., 2015). Weight gain associated with tobacco cessation is caused by removing nicotine’s effect on the brain’s central nervous system (Komiyama et al., 2013; Schmidt et al., 2019). Often, individuals quitting smoking will substitute the hand-to-mouth sensation of smoking with eating, which can lead to an increase in caloric intake throughout the day (Chao et al., 2019; Rodin, 1987). Others might use food to cope with withdrawal symptoms (e.g., headaches and dizziness) experienced in the first few days after quitting tobacco use (Bush et al., 2014; Jo et al., 2002).
The association between weight gain and tobacco cessation can thus create barriers to cessation attempts (Bush et al., 2014; Hartmann-Boyce et al., 2021; Jain et al., 2020; Prochaska et al., 2008). As such, research recommends weight management interventions include approaches such as counseling (Bush et al., 2016; Levine et al., 2010; Perkins et al., 2001) and focus on healthy eating (Copeland et al., 2006; Jain et al., 2020) or physical activity (Jain et al., 2020; Vickers et al., 2009) to reduce post-cessation weight gain (Aveyard et al., 2012; Hartmann-Boyce et al., 2021; Jain et al., 2020). Therefore, tobacco cessation interventions that are designed also to prevent weight gain (i.e., physical activity and/or healthy eating) can both increase participation and lead to successful cessation outcomes (Hartmann-Boyce et al., 2021; Jain et al., 2020; Spring et al., 2009).
Research exploring a multicomponent approach that combines tobacco cessation interventions with interventions addressing other modifiable risk factors has consistently demonstrated effectiveness in a variety of non-workplace settings (Apollonio et al., 2016; Barth et al., 2015; Bock et al., 2019; Prochaska et al., 2008), although fewer studies have explored the effectiveness of this approach within workplace settings. The objective of this current review is to scan existing literature to explore the intervention components of a workplace tobacco cessation program that would include multiple, complementary components including healthy eating, physical activity, or mental health interventions. The review will also synthesize implementation facilitators and barriers and describe how multi-component programs have been adapted to meet the needs of unique workplace populations.
Methods
This scoping review methodology was informed by the PRISMA Extension for Scoping Reviews (PRISMA-ScR) checklist (Tricco et al., 2018) and Arksey and O’Malley’s (2005) five-step process for conducting scoping studies. The review was also guided by a multidisciplinary advisory committee that included public health practitioners with subject matter expertise in tobacco cessation, nutrition, addictions and mental health, work and health, and physical activity. The advisory committee worked collaboratively with members of the research team to refine research questions, search terms, inclusion criteria, and the extraction template. Findings from this review were reported to this advisory committee to inform program development.
Information Sources and Search
The search strategy was developed around the three main concepts: (a) workplace setting, (b) tobacco cessation, and (c) a complementary program component (i.e., physical activity, healthy eating, or mental health). Two researchers identified seminal literature (N = 7) that were analyzed using the MeSH analyzer to extract additional keywords that were incorporated into the search. A trained research librarian conducted the search across nine databases for relevant literature published between 2001 and 2023: MEDLINE (Ovid), EMBASE, Cochrane Database of Systematic Reviews, PsycINFO, PubMed, CINAHL, MEDLINE (Ebsco), Psychology & Behavioural Sciences Interventions, and Web of Science. In addition, a search for relevant gray literature (e.g., conference papers/proceedings) and internal documentation was also completed using Alberta Health Services Insite, OAISter, Google, and Google Scholar. An additional filter was applied to remove any articles that were not available in English. The first iteration of this search was completed on December 8, 2021. A second iteration was completed on September 18, 2023, to update the corpus of articles to include literature published during the time the synthesis and writing of the manuscript occurred. The database search was supplemented by hand searching the reference lists of relevant systematic reviews for additional pertinent literature.
Eligibility Criteria
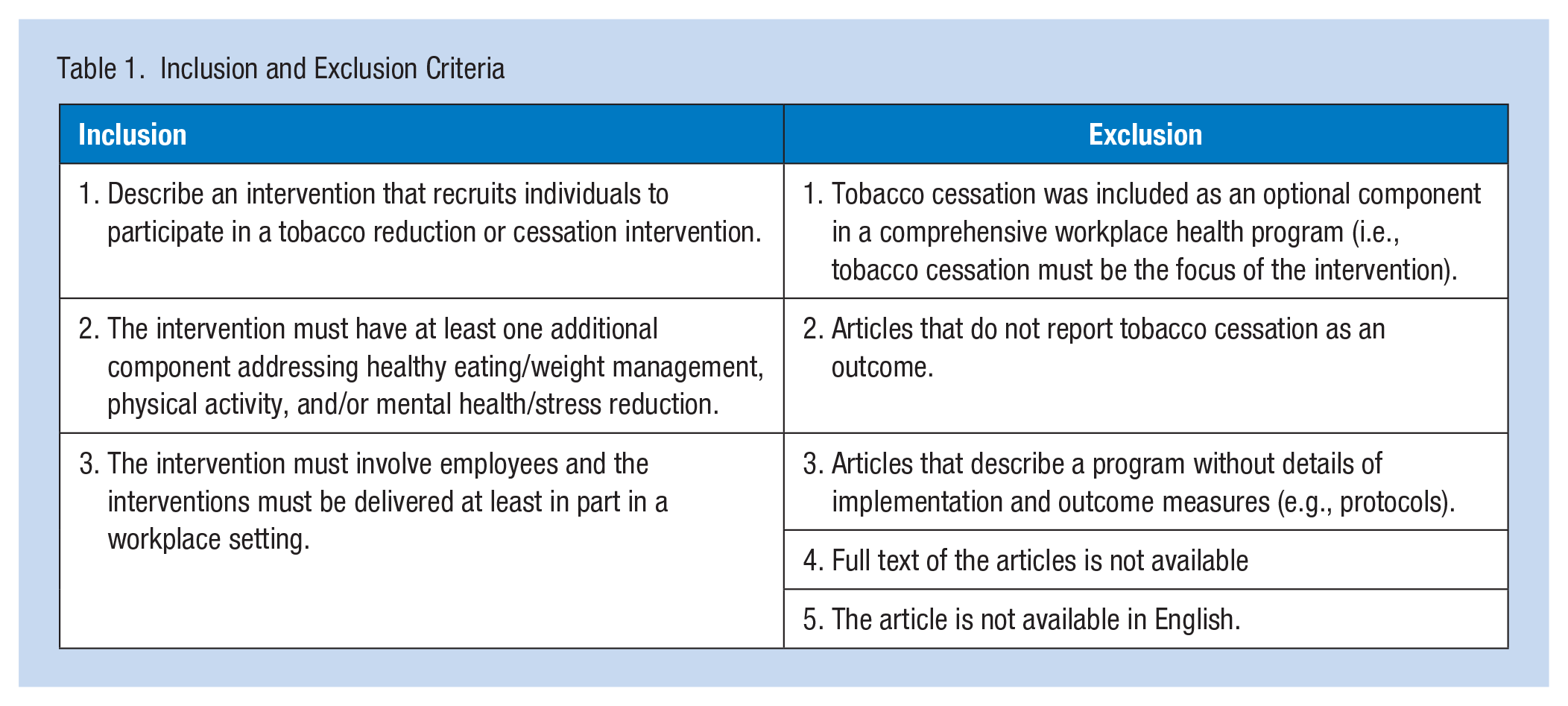
Eligibility criteria required studies to have a tobacco reduction/cessation intervention, have at least one additional intervention component (e.g., mental health, physical activity, healthy eating), and be conducted with employees at least partly in the workplace, although some components, such as telephone counseling or personal training sessions, may have taken place outside of the workplace. These criteria were developed a priori and applied to all articles extracted from the search. A full list of inclusion and exclusion criteria is outlined in Table 1.
Inclusion and Exclusion Criteria
Selection of Sources of Evidence
Article (n = 296) titles and abstracts were reviewed for inclusion by two independent reviewers resulting in 39 eligible articles selected for full-text screening and with an interrater reliability of 85%. Any disagreements were discussed with a third author to make a final inclusion decision. All final included articles were reviewed and approved by all research team members.
Data and Charting Process
The data extraction table was developed by two independent reviewers using a variety of article descriptors alongside the guidance of the project’s advisory committee. The table included: article characteristics (e.g., year, author, purpose/objective, population/sample size, setting, and methodology), individual or institutional characteristics (e.g., occupational gender distribution, industry, language, education, age, and income), intervention design components and multicomponents (e.g., tobacco cessation, physical activity, mental health/stress reduction, and healthy eating/weight management), reported outcome measures (i.e., service, implementation, and client outcome) outlined by Proctor et al. (2011), as well as facilitators and barriers identified by authors. Finally, intervention components were mapped to the five levels of the Social Ecological Model (SEM): intrapersonal (i.e., individual knowledge, attitudes, and skills), interpersonal (i.e., social networks and support systems), institutional (i.e., social institutions and rules and regulations), community (i.e., relationships of organizations and institutions within a defined boundary), and policy (i.e., local, provincial, or national policies and laws; McLeroy et al., 1988). All revisions to the data extraction template were made prior to full-text screening.
Synthesis of Results
Each article was summarized by providing an overview of the focal workplace and the intervention design, grouped by complementary elements included in the intervention. We also synthesized the service, implementation, and client outcomes, as well as subpopulation outcomes. The level of each intervention component targeted according to the SEM was then synthesized. Finally, stated facilitators or barriers to implementation were summarized to capture how interventions were tailored to meet the unique needs of the participants.
Results
The PRISMA diagram (Figure 1) illustrates the article selection process. The initial search identified 2,002 articles for review. Of these, 1,706 articles were removed (1,617 for duplicates and 89 for other reasons such as articles not accessible, not available in English, etc.) leaving 296 articles for eligibility review using the title and abstract screening resulting in 257 exclusions. Of the 39 articles screened for full-text eligibility, 27 were excluded: two articles were unavailable, two failed to meet the workplace criteria, and the remaining 23 articles did not incorporate a multicomponent intervention design. Following full-text screening, 12 articles were included for qualitative synthesis.
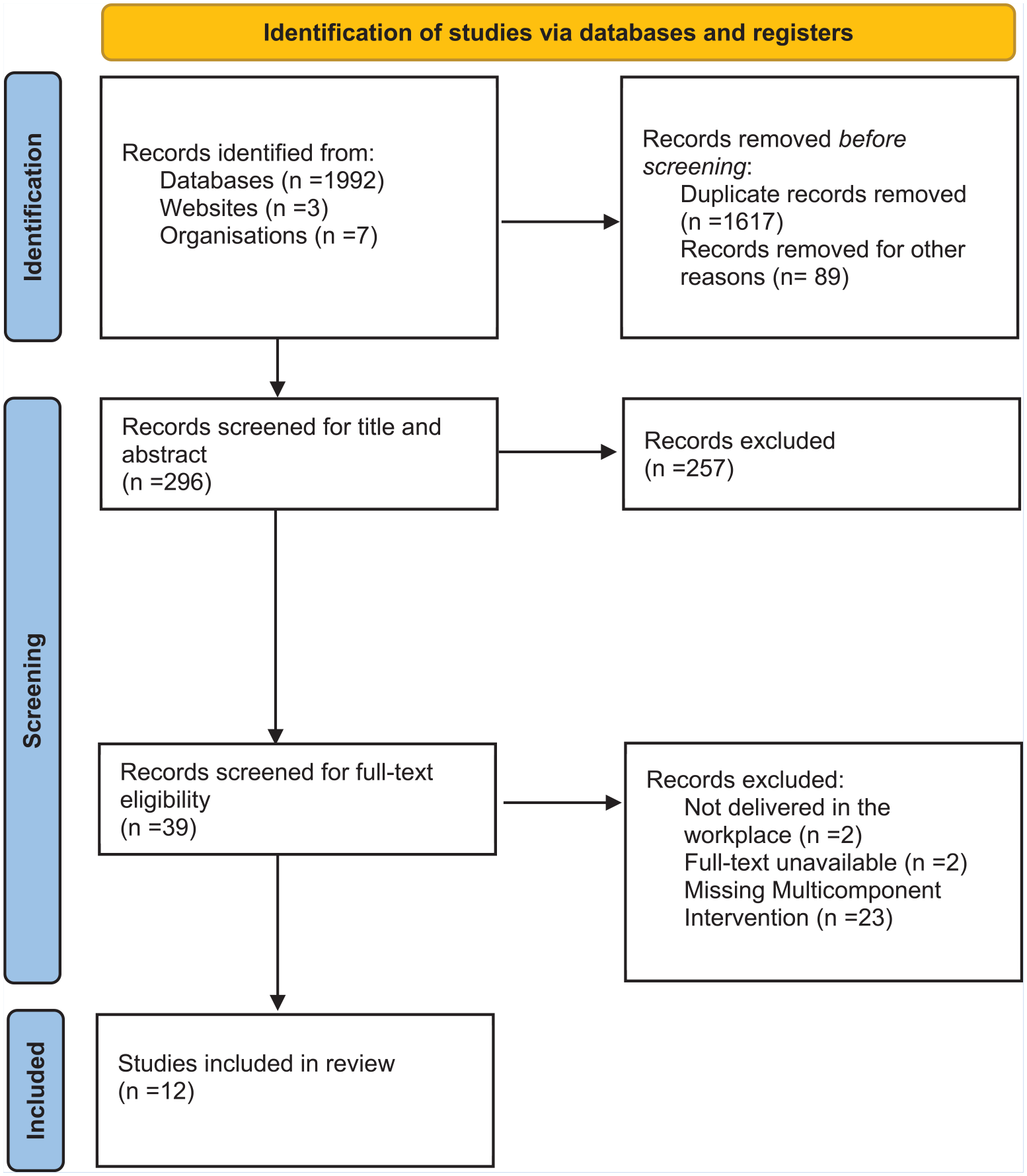
PRISMA—ScR—Workplace Tobacco Cessation and Multicomponent Interventions
Characteristics of the Intervention and Workplace
The characteristics of each study are outlined in Table 2. Six of the included articles were prospective cohort studies (Hausherr et al., 2017; Hwang et al., 2012; Pimple et al., 2012; Quintiliani et al., 2010, 2012; Yasin et al., 2011), three were randomized control trials (Sorensen et al., 2007; Weng et al., 2021, 2022), and the remaining three were quasi-experimental studies (H. Kim & Lee, 2021; S. K. Kim et al., 2022; Mache et al., 2019). Of the 12 included articles, sample sizes ranged from 64 to 2,674 employee participants. Sorensen et al. (2007) was the oldest article that was included, and both Weng et al. (2022) and S. K. Kim et al. (2022) were the most recent. The included studies represented interventions delivered in six countries.
Summary of Included Articles and Intervention Types
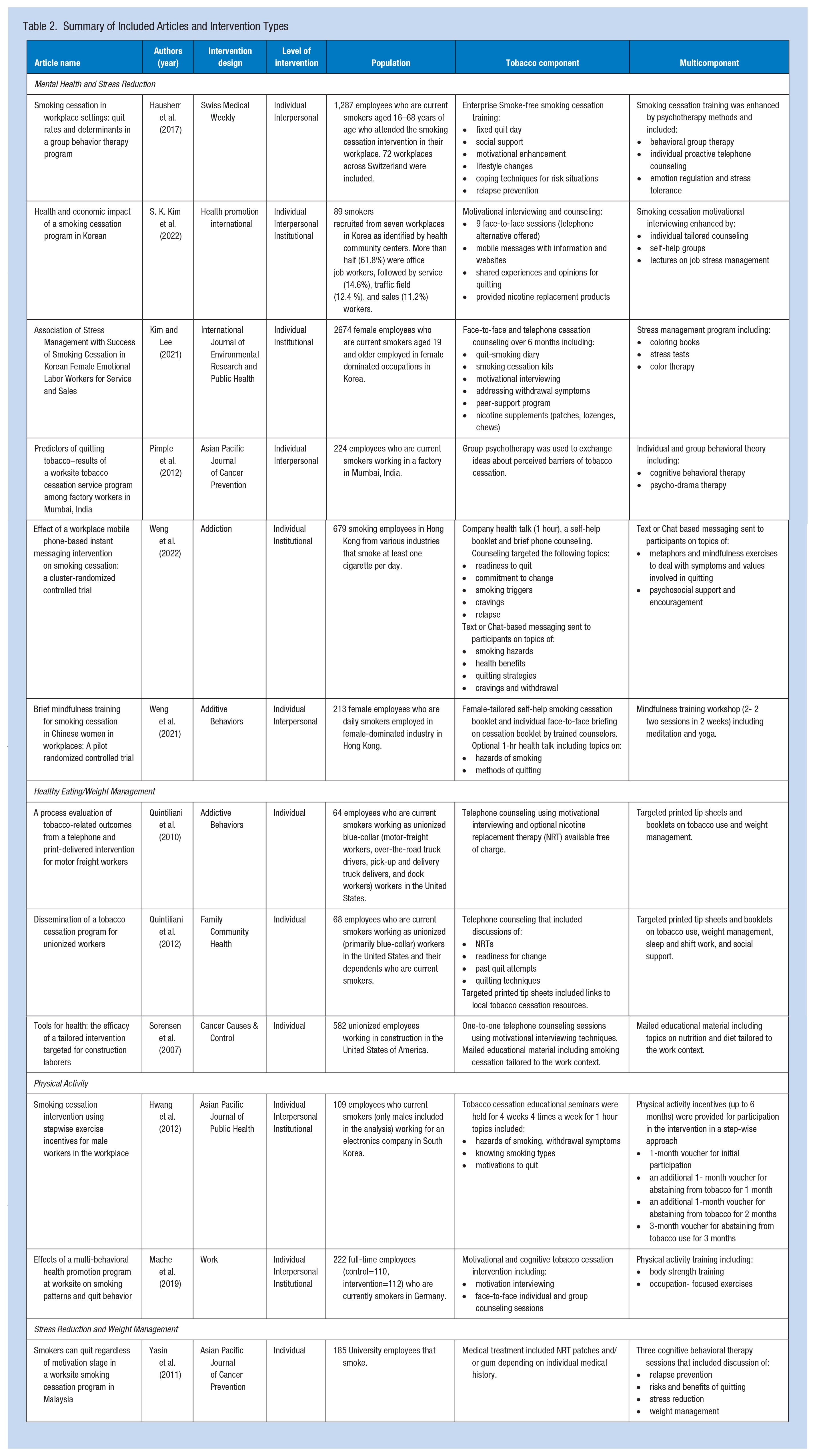
The included studies described interventions implemented in various industry populations. The most common target employee population was blue-collar workers (n=4; Pimple et al., 2012; Quintiliani et al., 2010, 2012; Sorensen et al., 2007). Two studies recruited participants from female-dominant occupations, including service and sales (H. Kim & Lee, 2021), beauty, and retail industries (Weng et al., 2021). One study looked specifically at male workers at an electronics company (Hwang et al., 2012). In addition, one study targeted university employees (Yasin et al., 2011). All four remaining interventions were either implemented in multiple industries (S. K. Kim et al., 2022; Weng et al., 2022) or the industry/occupation of employees was not explicitly stated (Hausherr et al., 2017; Mache et al., 2019).
Tobacco Cessation
The most common tobacco cessation intervention components described were cessation counseling or therapy (H. Kim & Lee, 2021; Pimple et al., 2012; Quintiliani et al., 2010; 2012; Sorensen et al., 2007) and motivational interviewing (H. Kim & Lee, 2021; S. K. Kim et al., 2022; Quintiliani et al., 2012; Sorensen et al., 2007; see Table 2). Three of the workplace interventions also included tobacco cessation health promotion materials such as handouts and booklets (Quintiliani et al., 2012; Sorensen et al., 2007; Weng et al., 2021). Two of the workplace interventions incorporated nicotine replacement therapy free of charge to participants (Quintiliani et al., 2010; Yasin et al., 2011). Workplace tobacco cessation interventions were paired with mental health or stress reduction interventions in six articles (Hausherr et al., 2017; H. Kim & Lee, 2021; S. K. Kim et al., 2022; Pimple et al., 2012; Weng et al., 2021, 2022) and paired with healthy eating or weight management interventions in three articles (Quintiliani et al., 2010; 2012; Sorensen et al., 2007). Two studies integrated tobacco cessation interventions with physical activity (Hwang et al., 2012; Mache et al., 2019). Only one study integrated tobacco cessation interventions with multiple complementary components (i.e., stress reduction and weight management; Yasin et al., 2011).
Mental Health/Stress Reduction
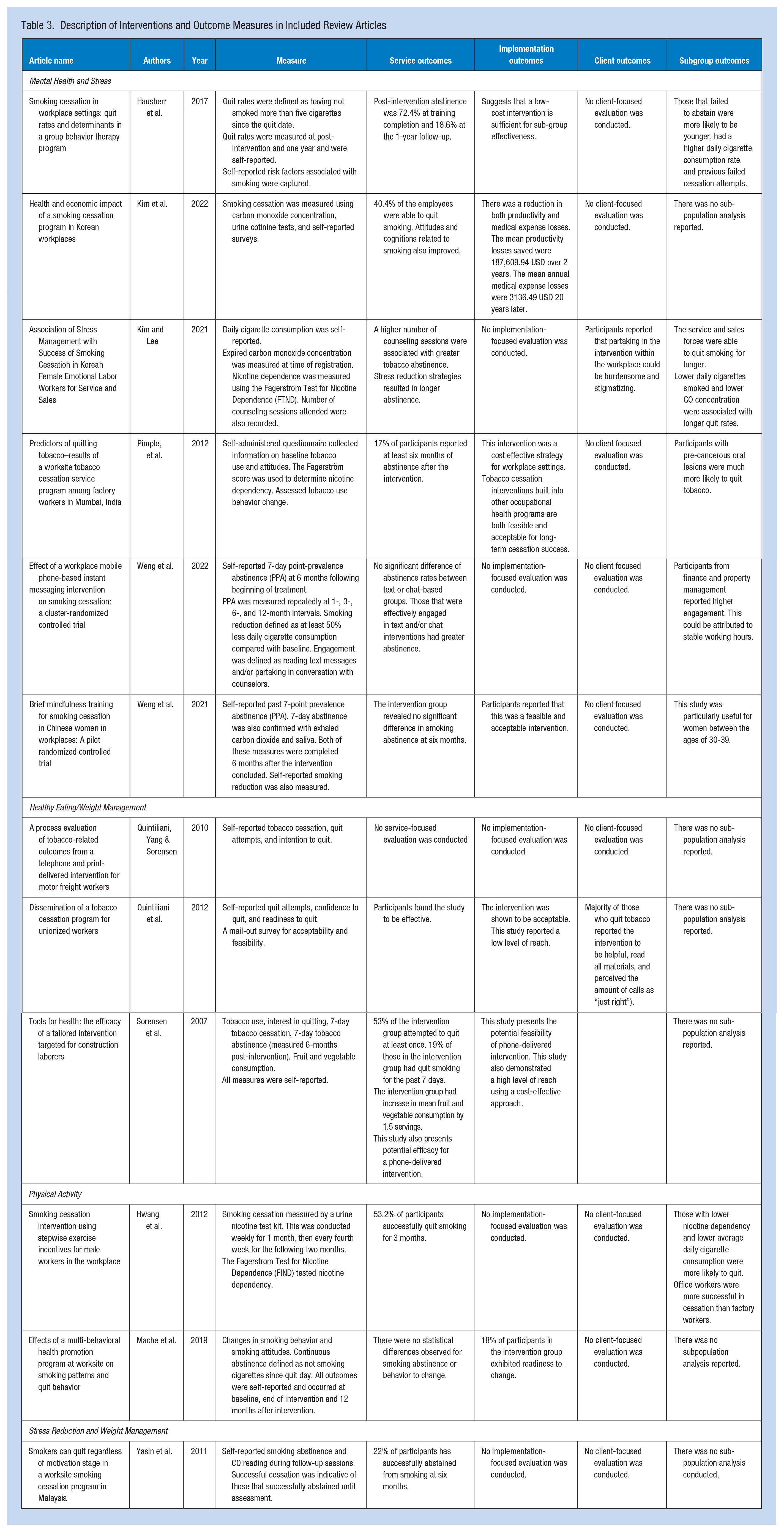
Most of the studies (n = 4; 67%) that intervened with mental health or stress reduction in addition to tobacco cessation used some form of psychotherapy (e.g., group therapy, counseling, or emotion regulation) with varying results (Hausherr et al., 2017; H. Kim & Lee, 2021; S. K. Kim et al., 2022; Pimple et al., 2012; Weng et al., 2022). Pimple et al. (2012) incorporated psychodrama into its intervention design, while Hausherr et al. (2017) incorporated telephone counseling, psychotherapy, and emotion regulation training for all participants. Both Pimple et al. (2012) and Hausherr et al. (2017) found that their interventions were successful with 17% abstinence rates at 6 months and 18% at 1 year, respectively (Table 3). In addition to traditional stress management techniques, Kim and Lee (2021) incorporated coloring books and color therapy into the intervention design for female employees. Weng et al. (2022) and Weng et al. (2021) both integrated unique mindfulness techniques into their tobacco cessation programming. These techniques included yoga and mindfulness messaging via SMS (text) or chat messaging with participants. Weng et al. (2022) reported a 6-month abstinence rate of 18.8% in chat-based participants and 21.6% in text-based participants. Kim and Lee (2021) found that 18.3% of participants in service and sales successfully quit smoking for 4 weeks. Weng et al. (2021) did not report statistically significant service outcomes of smoking abstinence. Finally, Kim et al. (2022) provided lectures on job stress management and implemented self-help groups, reporting that 40.4% of participants successfully quit smoking post-intervention. Furthermore, they reported an increase in productivity and a decrease in medical expenses for the company (S. K. Kim et al., 2022).
Description of Interventions and Outcome Measures in Included Review Articles
Healthy Eating/Weight Management
All studies that combined healthy eating or weight management with tobacco cessation interventions targeted blue-collar workers (Quintiliani et al., 2010, 2012; Sorensen et al., 2007). Furthermore, all the included papers that incorporated healthy eating and/or weight management into the intervention design did so using a combination of telephone counseling and distributing educational materials tailored to resonate with the targeted audiences in the studies. For example, Sorensen et al. (2007) tailored the diet and nutritional information by integrating it into health messaging information that addressed concerns with the work environment and hazardous substances of the construction industry (Sorensen et al., 2007). The researchers reported that the intervention had high levels or participation, leading to a 19% quit rate and an increase in fruit and vegetable consumption by approximately 1.5 daily servings (Sorensen et al., 2007). A series of studies by Quintiliani et al. (2010; 2012), reporting on the same intervention, provided telephone counseling and targeted print sheets to blue-collar workers in the workplace. The intervention resulted in a 7-day quit rate of 30.9% after a 16-week follow-up and high intervention acceptability among participants (Quintiliani et al., 2012). After evaluation, all three articles reported that their interventions were both feasible and relatively low-cost.
Physical Activity
There were two articles that integrated physical activity with workplace tobacco cessation efforts (Hwang et al., 2012; Mache et al., 2019). Mache et al. (2019) offered participants the opportunity to participate in optional physical training sessions with a trainer during the intervention. These sessions focused on body-strengthening techniques. The participants’ smoking cessation rates were compared to those of a control workplace who did not participate in the intervention. At 12 months follow-up, the intervention group's rates of cessation were higher but did not achieve statistical significance when compared with the control group (Mache et al., 2019). Hwang et al. (2012) used a stepwise incentive model for their physical activity intervention, where vouchers for a local fitness center were awarded to participants with smoking cessation success (confirmed via urinary analysis) at various intervals throughout the study. Hwang et al. (2012) reported a 3-month sustained smoking cessation success rate of 53.2%.
Stress Reduction/Weight Management
There was one study that integrated both stress reduction and weight management with the workplace tobacco cessation program. Yasin et al. (2011) offered participants three behavioral therapy sessions covering topics such as relapse prevention, risks and benefits of quitting, stress reduction techniques, and weight management techniques. Yasin et al. (2011) reported a high success rate of 22% smoking abstinence among participants at 6 months post-intervention.
Level of Intervention
All studies included in this review implemented some component of their intervention at the individual level (Table 2). Five studies only implemented activities at the individual level (Quintiliani et al., 2010; Sorensen et al., 2007; Yasin et al., 2011). Common individual-level intervention components across the intervention studies reviewed included counseling sessions (e.g., motivational interviewing, therapy sessions, etc.), educational material or lectures, and stress management materials (e.g., coloring books, self-help books, and mindfulness training).
Half (n=6) of the studies included a component leveraging the interpersonal level (Hausherr et al., 2017; Hwang et al., 2012; S. K. Kim et al., 2022; Mache et al., 2019; Pimple et al., 2012; Weng et al., 2021). Common interpersonal interventions included group counseling and mindfulness sessions, educational classes, and self-help groups. Fewer than half (n = 5) of the interventions targeted the institutional level (Hwang et al., 2012; H. Kim & Lee, 2021; S. K. Kim et al., 2022; Mache et al., 2019; Weng et al., 2022) via flexible participation options (e.g., during working hours, adaptable timetables), incentives, environmental diagnostics, and consulting, and creating a workplace fund. None of the interventions included in this review targeted community or policy levels.
Subpopulation Outcomes
Approximately half of the studies reported intervention outcomes stratified by subpopulations. Studies identified that abstinence and quit rates were lower among younger individuals (Hausherr et al., 2017), heavy smokers, or individuals who had reported previously failed cessation attempts (Hausherr et al., 2017; Hwang et al., 2012). Differences in cessation success rates were also reported among different occupations. Kim and Lee (2021) found that women in sales and services occupations were able to quit for longer time periods than those in other occupations, while Hwang et al. (2012) found that office workers were more successful in abstaining from smoking than factory workers. Similarly, Weng et al. (2022) found that participants from finance and property management were more likely to engage with the intervention and attributed this finding to the stable working hours of the participants. Kim and Lee (2021) found that the women participants with greater social support were more successful in their intervention efforts.
Facilitators
The subpopulation outcomes reported in select studies suggest that tailoring intervention approaches may better meet the needs of different workplace populations. An example of this implementation strategy involves crafting targeted materials for specific subpopulations by highlighting their particular needs, lives, and work experiences within the materials being produced (Quintiliani et al., 2010; 2012; Sorensen et al., 2007; Weng et al., 2021). As an example, Weng et al. (2021) tailored the intervention materials to contain information specific to women, such as health messaging surrounding smoking and pregnancy harms. In addition, Sorensen et al. (2007) created targeted cessation strategies by discussing the home lives of participants during counseling to enhance implementation.
Delivering interventions fully or partially in workplace settings was one of the most widely reported facilitators of equitable access and enhanced participation among sub-populations (Sorensen et al., 2007). For example, Kim and Lee (2021) conducted their intervention during paid working hours, which increased participation rates among employees. Additional facilitators reported in the studies included various language deliveries (Sorensen et al., 2007), time- and material-condensed educational sessions (Weng et al., 2021), integration of intervention methods into existing workplace health and safety programs (Sorensen et al., 2007), and offering multiple intervention platforms, e.g., alternative methods of accessing counseling, such as by telephone versus in-person (H. Kim & Lee, 2021).
Incentives are also effective facilitators for tobacco cessation in workplace interventions (Brand et al., 2018) and must be considered as a way to enhance cessation programming. Five of the included studies offered incentives within their intervention programs (Hwang et al., 2012; H. Kim & Lee, 2021; S. K. Kim et al., 2022; Quintiliani et al., 2010; Yasin et al., 2011). Many of the studies incentivized eligible participants by providing nicotine replacement therapy free of charge during the intervention (H. Kim & Lee, 2021; S. K. Kim et al., 2022; Quintiliani et al., 2010, 2012; Yasin et al., 2011). Hwang et al. (2012) provided a fitness center voucher for all participants who were able to successfully abstain from smoking. Similarly, Kim et al. (2022) paid out successful participants via an operating incentive system. Together, these studies demonstrate that the inclusion of incentives could be a helpful strategy for promoting tobacco cessation (Hwang et al., 2012; Quintiliani et al., 2012; Yasin et al., 2011).
The inclusion of social support during the cessation intervention process was also identified as a facilitator in tobacco cessation intervention designs. For example, Quintiliani et al. (2012) included the dependents of employees within the intervention to increase social support and better integrate cessation methods within the home environment. Kim et al. (2022) organized self-help groups that encouraged participants to share opinions and experiences surrounding cessation, with the aim of strengthening the participants’ social support network. Kim et al. (2022) further recognized that Korean workplace culture tends to emphasize a sense of community and co-worker connection, which may have further facilitated successful cessation outcomes.
Barriers
Social supports, while viewed as a facilitator to some, were viewed as a barrier by others. For example, women emotional labor workers found it burdensome and stigmatizing to have other co-workers aware of their smoking status during an intervention study set in the workplace (H. Kim & Lee, 2021). To avoid unintended consequences, program designers must consider how facilitators and barriers translate across workplace settings and for different employee subpopulations.
Although many of the studies were successful at integrating facilitators into their interventions, several barriers were also noted. Programs that were too lengthy or abstract proved difficult for participants to integrate into daily routines (Weng et al., 2021). In addition, verifying cessation via biochemical tests such as urine, CO, or saliva analysis, despite having strong research validity, may introduce the perception that participants are not trusted. This outcome was especially applicable to workplaces in which drug tests are already commonplace (Quintiliani et al., 2012; Weng et al., 2021).
Discussion
Existing systematic reviews and meta-analyses have shown that multicomponent tobacco cessation interventions are effective in non-workplace settings such as hospitals and communities (Apollonio et al., 2016; Barth et al., 2015; Bock et al., 2019; Prochaska et al., 2008). Results from our scoping review indicate that there is limited evidence of this approach being applied in the workplace setting. The 12 studies we considered implemented multicomponent interventions integrating physical activity, healthy eating and/or weight management, and mental health/stress reduction alongside tobacco cessation interventions. Implementation of multicomponent approaches appears to be feasible in workplace settings and can enhance cessation outcomes (Hwang et al., 2012; H. Kim & Lee, 2021; Quintiliani et al., 2010; 2012; Sorensen et al., 2007). Offering incentives in conjunction with participation in other intervention components further improved cessation efforts (Hwang et al., 2012). However, these types of interventions were delivered in limited types of workplaces and with few targeted subpopulations of employees. Our scoping review findings demonstrate the need to test this approach across a diversity of workplaces to determine whether a multicomponent, multilevel approach improves upon existing workplace tobacco cessation efforts.
This scoping review also suggests that a multicomponent approach offers a unique opportunity to target subgroup populations of employees who are vulnerable to higher smoking rates, such as blue-collar workers (Sorensen et al., 2004; Upson, 2015). Blue-collar workers are important to target as they have a higher smoking prevalence rate alongside lower levels of education and income, which are also associated with poorer dietary practices and nutrition (Barbeau et al., 2004; Lee et al., 2022). Our findings suggest a unique opportunity to further tailor cessation materials in future complementary tobacco cessation designs. Our findings also support tailoring approaches when targeting occupations with inconsistent or nontraditional working hours, such as factory and blue-collar workers, as seen in Quintiliani et al. (2010), Quintiliani et al. (2012), and Sorensen et al. (2007). The result of our review suggests a call to action to innovate multicomponent tobacco cessation programming that effectively targets other priority populations, such as emotional labor workers (H. Kim & Lee, 2021).
Our scoping review findings indicate that workplace tobacco cessation programs, when delivered as multicomponent interventions, have most often been combined with mental health and/or stress reduction programming. The extant literature demonstrates that this approach is essential for mitigating the links between experiencing stress and successfully navigating tobacco cessation. By integrating mental health and stress reduction within intervention designs, there is potential to address existing inequities in tobacco use (Lee et al., 2022; U.S. National Cancer Institute, 2017). However, it is important to note that stress is hypothesized to manifest at the institutional and community levels, where poor psychosocial work environments increase employee stress (Lazarus, 2020; Sorensen et al., 2004). Most of the studies we reviewed that integrated mental health and stress reduction with tobacco cessation focused on the individual level. The onus was placed on the individual to cope with their stress, rather than addressing the occupational and environmental conditions creating the stressors in the first place. Therefore, future innovations aiming to complement tobacco cessation in the workplace with mental health and stress reduction interventions should look beyond the individual level. Promising multicomponent interventions should seek to address structural drivers of employee stresses and occupational safety hazards that could attenuate efforts to maximize the effectiveness and sustainability of tobacco cessation programming.
Few studies explored addressing the interpersonal level (e.g., social support) within intervention design. Intervening at the interpersonal level could enhance the integration of intervention strategies within the lived realities and home lives of participants. For example, Quintiliani et al. (2012) integrated the dependents of participants into the intervention and Kim et al. (2022) designed self-help support groups among participants. However, implementing interpersonal-level interventions with certain employee populations, such as female emotional laborers, may cause stigmatization as an unintended consequence (Kim & Lee, 2021). Employee characteristics must be considered when developing workplace multicomponent tobacco cessation programming at the interpersonal level. For example, future interventions could benefit from implementing tobacco cessation interventions in conjunction with workplace-level social support systems or voluntary participation without public workplace disclosure to minimize risk to the participants.
Despite the interventions being implemented fully or partially in the workplace, only five studies addressed institutional-level intervention components (Hwang et al., 2012, H. Kim & Lee, 2021; S. K. Kim et al., 2022; Mache et al., 2019; Weng et al., 2022). Both individual and institutional tailoring of intervention designs could help increase study effectiveness. Accounting for the lived realities of the unique employee populations in various intervention programming methods allows for greater effectiveness in cessation efforts (Quintiliani et al., 2010; 2012; Sorensen et al., 2007). For example, implementing these programs during paid working hours can increase participation from low-income workers who are known to have higher smoking rates, such as blue-collar workers (Brand et al., 2018). It is necessary that these workplace interventions use complementary components across multiple levels to maximize effectiveness. Failing to do so may explain why some studies did not find significant differences in the results of cessation efforts for experimental versus control groups.
Strengths
This review was conducted using a systematic and rigorous search process by following the PRISMA-ScR (Tricco et al., 2018). This process ensured that our scoping review results were reliable and reproducible. Accordingly, the search question, search terms, and inclusion criteria were established a priori and required no adjustment as the scoping review progressed. In doing so, interrater reliability was maximized when analyzing texts. In addition, all research questions and methods were developed in consultation with a multidisciplinary advisory committee that represented practitioners’ perspectives. To the authors’ knowledge, this scoping review is the first to examine and review literature reporting on multicomponent tobacco cessation interventions delivered within workplace settings.
Limitations
Despite the strengths of this scoping review, some limitations must be considered. First, all articles within this scoping review were published in English, and thus our review may have failed to capture relevant research published in other languages. In addition, the scoping review considered studies conducted between 2001 and 2023. In doing so, some pertinent research may have been missed. However, the time frame was limited to the past 22 years due to a recent expansion of workplace health focus on non-communicable disease risk factors. Prior to 2001, there was limited research focused on workplace health programming to address single modifiable risk factors for cancer, let alone multiple risk factors (Sorensen et al., 2004). Finally, it is necessary to consider potential publication bias. Although gray literature was searched, there is a tendency for nonpositive or nonsignificant findings to go unpublished and may not be captured in this review.
Conclusion
The findings of this scoping review suggest the need to better understand and integrate multiple complementary program components into workplace tobacco cessation efforts and innovations. For practitioners developing new interventions, it is necessary to consider the context of the workplace, the inclusion of interpersonal relationships, and tailoring to unique populations experiencing systemic inequities. Future research should examine the unintended consequences of workplace tobacco cessation intervention programs on stigmatizing current tobacco users and preventing their participation in workplace health promotion initiatives. There is a need to deepen our understanding of both individual-level factors and workplace culture that may influence implementing interventions. Future interventions could use tailored multicomponent approaches that target the whole workplace to both build cohesion among employees and overcome negative associations between certain individuals with tobacco use. Finally, targeting multiple levels of intervention rather than relying solely on individual and interpersonal activities could improve the effectiveness of workplace intervention programs.
Implications for Occupational Health Practice
Our scoping review reveals that multicomponent tobacco cessation interventions, although effective in non-workplace settings, are underutilized in workplace environments. For occupational health practitioners, integrating tobacco cessation with complementary health initiatives—such as stress reduction, physical activity, and healthy eating—may significantly improve outcomes, especially for vulnerable groups like blue-collar workers. The findings emphasize the importance of tailored, multilevel approaches that address both individual behaviors and broader workplace conditions. By considering the unique needs and challenges of diverse employee populations, occupational health practitioners can enhance the effectiveness and inclusivity of workplace health promotion efforts, ultimately supporting sustained tobacco cessation.
In Summary
Combining complementary program components such as physical activity, healthy eating, and mental health with tobacco cessation in a workplace health intervention may enhance cessation outcomes.
All healthy eating intervention designs were implemented in blue-collar workplaces. These workplaces employ individuals who conduct manual labor or perform skilled trades (e.g., motor-freight workers, delivery drivers, dock workers). This demonstrates a need to intervene across other workplaces and populations.
Complementary mental health intervention programming was common, however, only at the individual and interpersonal level. Literature has shown this to be insufficient.For maximum impact, interventions should be implemented across multiple levels of the Social Ecological Model (SEM) to account for the psychosocial and physical work environments of participants.
Tobacco cessation programming must consider the context of the workplace and its employees, leverage inter-personal relationships in the intervention design, tailor programs to the populations within the industry, and conduct a proper evaluation of effectiveness outcomes.
Footnotes
Acknowledgements
We would like to express our gratitude to Marcus Vaska from the Knowledge Resource Service at Alberta Health Services for his valuable contribution to the development and implementation of the search strategy for this scoping review. We would also like to acknowledge and thank the expertise of our advisory committee. Finally, we would like to thank Howie Thomson from Provincial Population and Public Health at Alberta Health Services for his contribution to formatting all article tables.
Author Contributions
C. Baay made substantial contributions to design, analysis and interpretation of the data for the work, contributed to the drafting of the initial manuscript, approved the final manuscript, and is accountable for all aspects of the work.
G. Jessiman-Perreault made substantial contributions to the design and analysis of the work, as well as contributed to the interpretation of the data, drafting of the initial manuscript, approved the final manuscript, and is accountable for all aspects of the work.
A. M. Toohey contributed to the interpretation of the data, made substantial contributions to the drafting of the manuscript, approved the final manuscript, and is accountable for all aspects of the work.
L. K. Allen Scott made substantial contributions to the design of the work, assisted in the interpretation of the data, contributed to the drafting of the initial manuscript, approved the final manuscript, and is accountable for all aspects of the work.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding provided, in whole or in part by Alberta Health. Strategic direction and applied research support provided by the Alberta Health Services (AHS), Cancer Prevention and Screening Innovation (CPSI) team. Provision of funding by Alberta Health does not signify that this project represents the policies or views of Alberta Health.