
Abstract
Background:
The workplace provides a unique opportunity to intervene on tobacco use, by implementing multilevel interventions engaging diverse employees. Using the social ecological model (SEM), this scoping review aimed to synthesize descriptions of multilevel workplace tobacco control programs to create a health equity informed framework for intervention planning.
Methods:
Multiple databases were searched for articles published from January 2010 to December 2020 meeting inclusion criteria (i.e., discussed multilevel tobacco cessation interventions that intervene, target, or incorporate two or more levels of influence, and one of the levels must be the workplace). Articles were screened by two independent researchers and included if they discussed multilevel tobacco cessation interventions that intervened, targeted, or incorporated two or more levels of influence. To integrate the extracted information into the SEM, we utilized the McLeroy et al. model and definitions to describe potential multilevel interventions and their determinants.
Results:
Nine articles were included in this review. No studies intervened across all five levels (individual, interpersonal, institutional, community, and policy), and the most common levels of intervention were individual (e.g., individual counseling), interpersonal (e.g., group therapy), and institutional (e.g., interventions during work hours). Participation rates varied by key social determinants of health (SDOHs) such as age, gender, education and income. Barriers including cost and sustainability influenced successful implementation, while leadership endorsement and accessibility facilitated successful implementation.
Discussion/Application to Practice:
Multilevel interventions targeting at least two SEM levels may reduce persistent health inequities if they address how SDOHs influence individual health behaviors. Employee characteristics impacted the success of tobacco cessation interventions, but more research is needed to understand the barriers and facilitators related to workplace characteristics.
Background
Tobacco use is the leading modifiable risk factor for cancer, linked to the highest proportion and number of cancer cases compared with all other modifiable risk factors (Islami et al., 2018). To address this issue, the World Health Organization (WHO) developed the Framework Convention on Tobacco Control (WHO FCTC), an evidence-based treaty that upholds the right of all people to have the highest standard of health (WHO, 2008). Among its many recommendations to promote tobacco cessation and offer adequate treatment, the WHO FCTC encourages nations to take a settings-based approach to tobacco cessation by designing and implementing tobacco cessation programs in the places individuals live, work, learn, and play (WHO, 2008).
One of the significant challenges to implementing tobacco control programs is related to the higher rates of tobacco smoking among subpopulations experiencing multiple sociocultural disadvantages such as low socioeconomic status (SES), lower educational attainment, higher risk of mental illness, higher prevalence of disability, and histories of homelessness and neighborhood deprivation (Upson, 2015). These inequities extend to lung cancer incidence, where a stepped gradient has been shown according to educational attainment, income, and occupation (Mitra et al., 2015). Inequities in tobacco use and resulting chronic disease burden exist across multiple levels of influence (i.e., individual, interpersonal, institutional, community, and policy factors) interacting with one another to exert a multiplicative influence on individual tobacco use (Kalkhoran et al., 2018).
Leveraging the workplace as a setting presents a unique opportunity to implement health promotion activities for a diverse population, with the potential to reach subsets of the population that are often difficult to engage through traditional means (Goetzel & Ozminkowski, 2008; Burton & World Health Organization, 2010). In addition, workplace health interventions provide access to a large and relatively stable population, have higher participation rates than other settings, allow for peer group support and positive peer pressure, offer access to professional support through occupational health staff, and have a low cost to participate (Cahill & Lancaster, 2014). Despite the potential value of such programs, organizational characteristics and capacities often prevent certain workplaces from implementing these programs. For instance, studies have concluded that small to midsized businesses are significantly less likely to offer health promotion programs (Hannon et al., 2012; Jessiman-Perreault et al., 2020; Linnan et al., 2008; McCoy et al., 2014). Industry and occupation type have also been found to impact the adoption of workplace health promotion programs, with findings suggesting that workplaces with the greatest availability of these types of programs were more likely to be white-collar, indoor office jobs, whereas blue-collar, labor-intensive jobs were much less likely to have access to workplace health promotion programs (Tsai et al., 2019). In the context of tobacco use, this is particularly problematic given the long-established relationship between tobacco use and blue-collar work (Leigh, 1996; Nelson et al., 1994; Smith, 2008). Workplace environments and working conditions have also been shown to impact the success of health promotion activities, such as tobacco cessation programs (Goetzel et al., 2014). Therefore, working conditions contribute significantly to health inequities (Burgard & Lin, 2013), and implementing tobacco cessation programs without addressing interactions between underlying individual and workplace determinants of health may be ineffective or even counterproductive (Schölmerich & Kawachi, 2016; Sorensen et al., 1998). Thus, reducing tobacco use among priority populations requires coordinated and multilevel interventions in settings such as the workplace to address numerous determinants of use and support continued abstinence (Baron et al., 2014).
The social ecological model (SEM) is a conceptual tool that emphasizes the interactions between environmental and social determinants on individual health behaviors (Sallis & Owen, 2015). Social ecological models have become increasingly popular in public health as the field shifts away from a biomedical paradigm that prioritizes individual or interpersonal interventions in favor of increasingly addressing social or structural determinants of health (S. D. Golden et al., 2015; T. L. Golden & Wendel, 2020). The SEM is commonly used in public health for diverse health issues and has also been used by national and international health bodies as a framework to guide health promotion efforts (Blas & Sivasankara, 2010; Leppo et al., 2013).
While multiple researchers contributed to the popularization of SEM in public health, McLeroy and associates (1988) developed one of the most commonly used iterations of the SEM. McLeroy et al. (1988) identified five layers of the SEM: (a) intrapersonal (i.e., individual knowledge, skills, and motivation), (b) interpersonal (i.e., relationships with others), (c) institutional (i.e., policies and procedures of organizations), (d) community (i.e., availability and location of resources within a defined boundary), and (e) policy (i.e., local, provincial, or federal policies and laws). McLeroy et al. (1988) also used the SEM to help identify and craft multilevel interventions, where all levels are understood as determinants of health which can help or hinder individuals’ abilities to modify their behaviors (S. D. Golden & Earp, 2012). The SEM model has been previously utilized by authors such as Kalkhoran et al. (2018) to describe multilevel factors that are associated with smoking initiation and cessation.
The SEM provides context for understanding tobacco interventions and their level of intervention. In the present article, we built on the work of Kalkhoran et al. (2018) and Sorensen et al. (2004) to review multilevel interventions that have been implemented, in part, in the workplace setting and describe health equity considerations to guide the development, implementation, and evaluation of multilevel tobacco control programs.
Rationale
Scoping reviews are best used for charting or mapping evidence and are conducted by researchers with methodological or content expertise. Like a systematic review, they follow a prescribed format to reduce bias, but allow research teams to explore broader questions than a systematic review. To determine priority populations and inform future multilevel tobacco control interventions, it was essential to extract evidence of what tobacco control interventions have been successful for whom and in what contexts. Given that disparities exist at individual and institutional levels, investigation was needed to better understand the impacts of multilevel interventions on tobacco cessation and control. To this end, we conducted a scoping review of published evidence of multilevel tobacco control interventions focused on workplace settings to explore the breadth of research on this topic and inform the development, implementation, and evaluation of future public health interventions focused on the workplace setting (Peters et al., 2020).
Overall, this scoping review aimed to identify and describe the current body of evidence on multilevel workplace tobacco control programs. Specifically, this review focused on three objectives, including to determine (a) which multilevel workplace tobacco control programs have been shown to be effective or ineffective; (b) for whom (i.e., populations or participants) these tobacco control programs have been shown to be effective or ineffective; and (c) the barriers and facilitators associated with implementing multilevel tobacco control programs in the workplace context.
Methods
The scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses–Scoping Review (PRISMA-ScR) checklist (Tricco et al., 2018). The inclusion criteria were defined through population, concept, and context. First, the focal population for intervention was to be, at minimum, employees at a workplace. Second, at the conceptual level, the intervention must have focused on tobacco control, defined as interventions with the primary target of increasing tobacco control rates within a population. Third, also at the conceptual level, the intervention discussed in the included articles must have been multilevel, defined as some form of tobacco control program that targets, intervenes, or incorporates interventions at two or more levels of the SEM. Finally, at the contextual level, the intervention must have been focused in part on workplace tobacco control programs, defined as interventions taking place at the workplace with an employee population.
Additional limits included: (a) exclusion of review articles; (b) exclusion of studies published in languages other than English; (c) exclusion of studies published prior to 2010 to focus on recent workplace tobacco control interventions; and (d) creation of regional restrictions limited only to include publications from Canada, the United States, Europe, Australia, or New Zealand to increase relevance of included studies based on similar economic and demographic factors.
The search was completed by a trained research librarian at Alberta Health Services. The initial search was conducted through the following databases: MEDLINE (Ovid), PsycINFO, Cochrane Library, PubMed, PubMed Central, CINAHL, MEDLINE (Ebsco), and Psychology & Behavioral Sciences Collection. In addition, a search for relevant gray literature was also conducted using Alberta Health Services Insite, Google, Google Scholar, and OAISter. The time frame of the search was January 2010 to December 2020, and the search was completed on December 22, 2020. In addition to this initial search, systematic reviews were hand-searched for relevant references. Details of the search strategy used to search MEDLINE (Ovid) can be found in Supplemental Table 1.
The initial search strategy also included literature that focused on cannabis and marijuana. However, there was a paucity of evidence connecting cannabis use to increased risk of chronic diseases (Jett et al., 2018). Moreover, the workplaces’ role in preventing cannabis use among employees was still unclear and typically focused on concerns around safety rather than chronic disease prevention, as seen with programs targeting tobacco use in the workplace (Howard & Osborne, 2020). Considering this rationale, we excluded articles that focused solely on marijuana or cannabis.
Studies meeting the inclusion criteria were independently reviewed by two reviewers (R.P., N.F.). To ensure consistency between reviewers, a pilot test of title and abstract screening was conducted with 10 articles. Eighty percent agreement was obtained from this pilot test allowing the reviewers to proceed with title, abstract, and full-text screening. Results of independent reviews were compared, and any disagreement was brought to the larger research team (G.J.-P., L.K.A.S.) for discussion and to determine final inclusion. During the selection of sources of evidence processes, the two independent reviewers had an agreement rate of 99% for title and abstract and 89% for full text.
A pilot-tested data extraction table was used to compile information on article characteristics (purpose/objective, population, sample size, setting, methodology), social determinants of health (e.g., gender, age, income, education, occupation), level of intervention (individual, interpersonal, institutional, community, policy), and barriers and facilitators of participation and/or successful outcomes.
Integration Into the SEM
To integrate the information extracted from included articles into the SEM, we utilized the McLeroy et al. (1988) model and definitions to describe potential multilevel interventions, where all levels are understood as determinants of health which can influence the effectiveness of the intervention. We integrated information on the social determinants of health, modifying conditions, and their corresponding workplace interventions across all five SEM levels (i.e., individual, interpersonal, institutional, community, policy). Barriers and facilitators were linked with the multilevel intervention design, acting as mediating mechanisms across the SEM levels. Interventions were classified by level based on the target of the intervention regardless of the level of the outcome measure. Integration into the SEM provides a visual model of how employee characteristics, modifying conditions, and unique barriers and enablers influence intervention design and ultimately the effectiveness and health equity of a multilevel tobacco cessation intervention.
Results
The PRISMA flow diagram (see Figure 1) illustrates the total number of results across all databases searched, as well as numbers after duplicate removal. The search of electronic databases retrieved 141 peer-reviewed articles and two gray literature sources (n = 143). During title and abstract screening, 88 sources were excluded, the majority of which solely focused on the use of marijuana or cannabis. During full-text screening, 46 articles were excluded with reason (as described above), resulting in the final inclusion of nine articles for analysis.
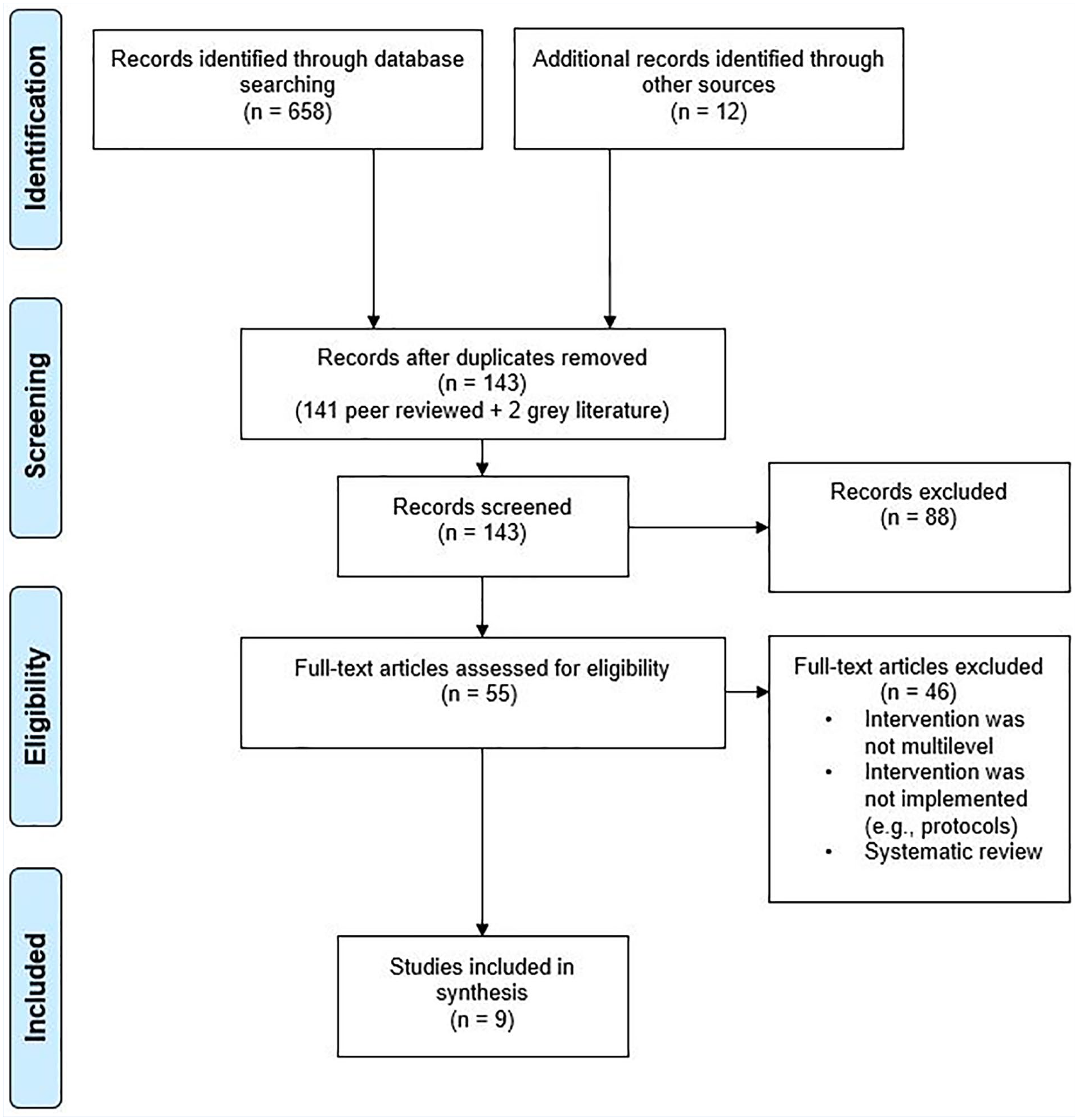
PRISMA statement displaying study selection process for multilevel workplace control interventions scoping review.
Of the nine included studies, five were randomized controlled trials that compared two different forms of intervention (Asfar et al., 2020; Caponnetto et al., 2020; Mache et al., 2019; van den Brand et al., 2018, 2020) and four were cohort studies (Moses et al., 2020; Nieva et al., 2017; Paul et al., 2013; Schult et al., 2016) (Table 1). Follow-up time points ranged from 3 to 12 months, except for Nieva et al. (2017) with a follow-up period of 5 years. This longer follow-up period allowed Nieva et al. (2017) to explore rates of continued tobacco abstinence. Three studies were in the United States (Asfar et al., 2020; Moses et al., 2020; Schult et al., 2016), two studies were in the Netherlands (van den Brand et al., 2018, 2020), and one study each was in Italy (Caponnetto et al., 2020), Germany (Mache et al., 2019), Spain (Nieva et al., 2017), and Australia (Paul et al., 2013).
Characteristics of Included Articles in the Multilevel Workplace Tobacco Control Interventions Scoping Review (n = 9)
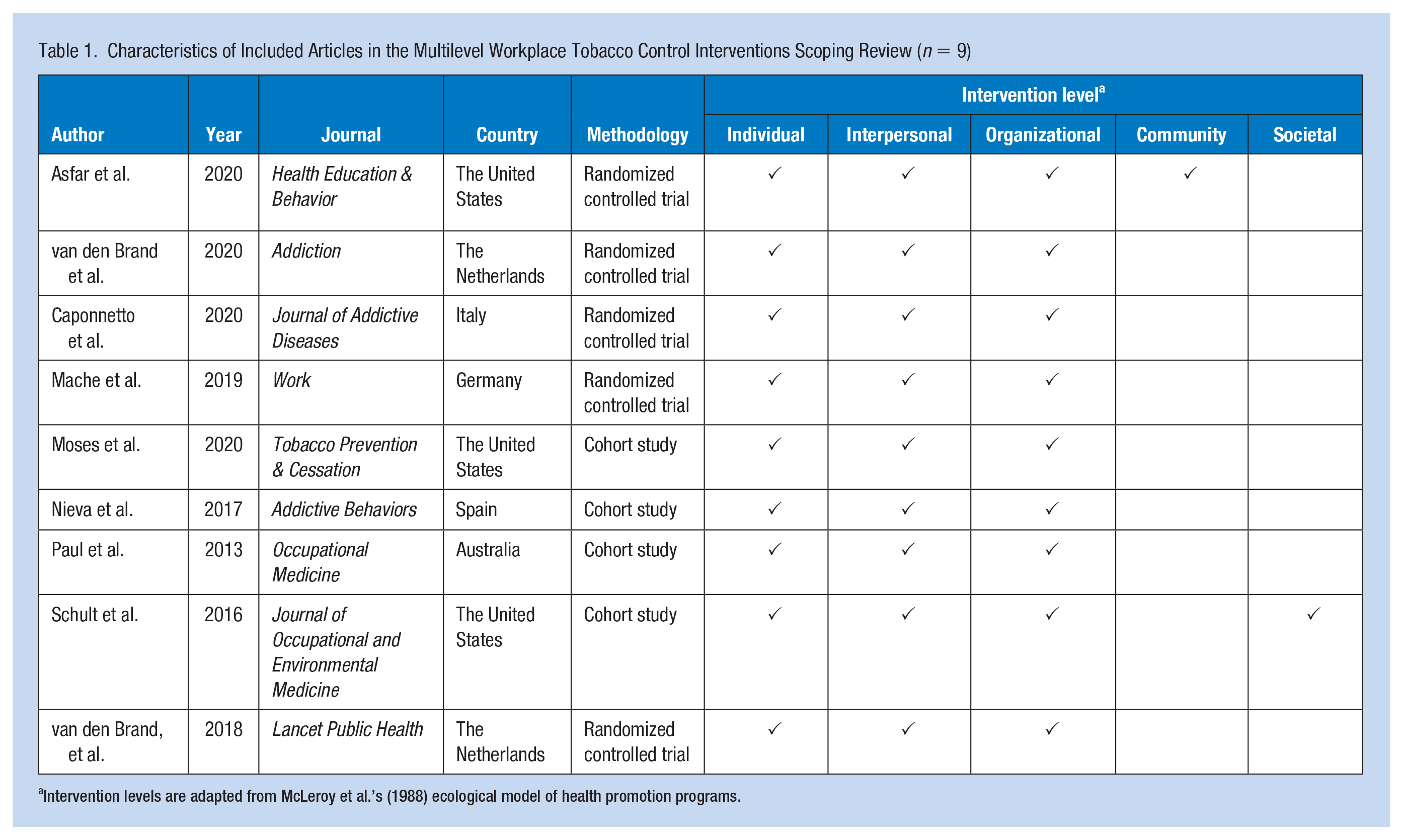
Intervention levels are adapted from McLeroy et al.’s (1988) ecological model of health promotion programs.
Multilevel Workplace Tobacco Control Program Effectiveness
Most studies included interventions that targeted or intervened across three levels of the SEM: the individual, interpersonal, and institutional (Table 2). Most commonly, interventions at the individual level included individual counseling (i.e., motivational interviewing [MI] and goal setting) (Asfar et al., 2020; Caponnetto et al., 2020; Mache et al., 2019; Nieva et al., 2017; Schult et al., 2016). Several of these interventions also paired individual counseling with pharmacological tobacco cessation aids, such as nicotine replacement therapy (NRT) (Asfar et al., 2020; Nieva et al., 2017). Three interventions also included individual-level financial incentives (i.e., direct payment or lower cost health plan) and reported high participation at follow-up (Moses et al., 2020; van den Brand et al., 2018, 2020).
Summary of Levels of Intervention and Intervention Outcomes of Included Articles in the Multilevel Workplace Tobacco Control Interventions Scoping Review
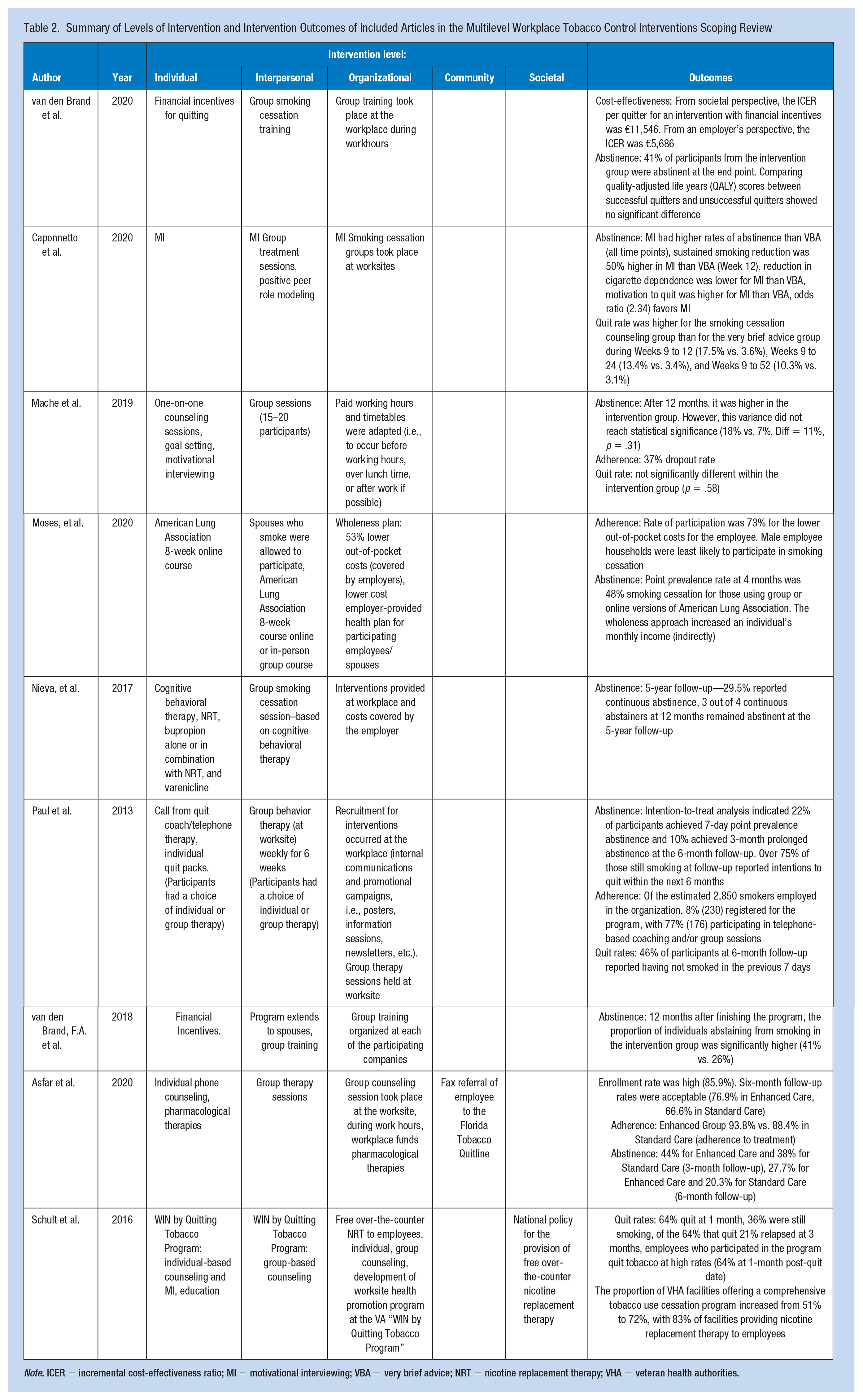
Note. ICER = incremental cost-effectiveness ratio; MI = motivational interviewing; VBA = very brief advice; NRT = nicotine replacement therapy; VHA = veteran health authorities.
Two main approaches were taken at the interpersonal level: group therapy and inclusion of spouses. Four studies included a group therapy component to their intervention (Caponnetto et al., 2020; Mache et al., 2019; Paul et al., 2013; van den Brand et al., 2020). Mache et al. (2019) and Caponnetto et al. (2020) both examined the effectiveness of group tobacco cessation as a mechanism to translate peer role modeling as a positive influence on abstinence, adherence, and quit rates. Second, the inclusion of spouses in the intervention resulted in increased participation among male spouses of female employees (Moses et al., 2020).
Institutional interventions typically included providing company time to attend tobacco cessation programs offered to the individual or the group (Asfar et al., 2020; Caponnetto et al., 2020; Mache et al., 2019; Nieva et al., 2017; Paul et al., 2013; van den Brand et al., 2018, 2020) or covering some cost associated with the program (e.g., the cost of NRTs) (Asfar et al., 2020; Moses et al., 2020; Nieva et al., 2017; Schult et al., 2016). Interestingly, none of the reviewed studies included an institutional intervention that altered any aspect of the workplace environment.
One study included a multilevel intervention that incorporated referral to community services such as local tobacco Quitline (Asfar et al., 2020). One study linked the intervention to a policy-level national policy for free over-the-counter NRTs (Schult et al., 2016), resulting in an increased NRT use across veteran health authorities (VHA) from 51% to 72%.
Impact of Multilevel Workplace Tobacco Control Program on Priority Populations
As part of this review, we examined the influence of SDOH on the effectiveness of the included studies. Information about the SDOH of the individual employee participants was limited, but we were able to present grouped results in Table 3 based on age, gender, education, and income.
Summary of the Impacts of the Interventions on Key Social Determinants of Health From Included Articles in the Multilevel Workplace Tobacco Control Interventions Scoping Review
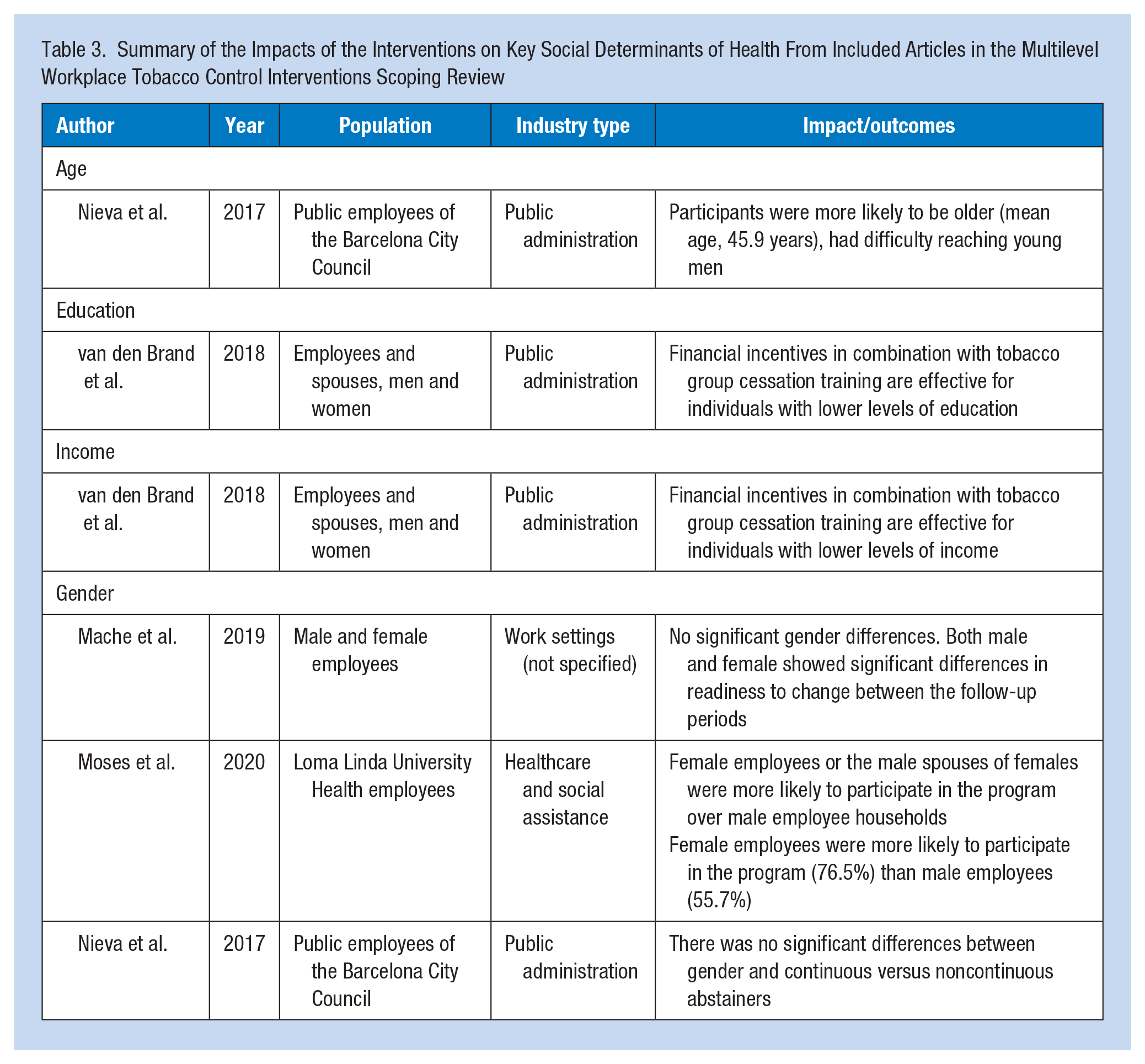
Nieva and colleagues (2017) reported that the individuals most likely to participate in programs were middle-aged (mean age, 45.9 years) men and highlighted how young adult men were a difficult age group to reach, but intervention early on could lead to continued health benefits for the individual. While several other articles reported the mean ages of participants, few articles noted how age influenced the likelihood of participating or likelihood of successful outcomes in the intervention.
Gender was discussed as a significant SDOH in many of the included articles. Moses et al. (2020) emphasized the impact that gender had on extending the smoking cessation program to participants’ spouses (i.e., interpersonal-level intervention) by revealing that female employees were more likely than male employees to refer their spouses to the smoking cessation program. The authors also found that male employees were the least likely to participate, with 55.7% of male employees participating and 76.5% of female employees participating. In contrast, Caponnetto et al. (2020) and Nieva et al. (2017) saw higher rates of participation for male employees. Mache et al. (2019) noted that there were no significant differences in readiness to change between males and females. Similarly, Nieva et al. (2017) saw no significant differences between genders in continuous abstinence.
Finally, one study (van den Brand et al., 2018) suggested that providing financial incentives coupled with group therapy could be an effective smoking cessation strategy for those with lower levels of education and income.
Multilevel Workplace Tobacco Control Program Facilitators and Barriers
Interventions that incorporated financial incentives had high rates of abstinence of 41% to 71% and adherence rates of 73% (Moses et al., 2020; van den Brand et al., 2018, 2020). van den Brand et al. (2020) found that from an employer’s perspective, long-term financial incentives were cost-effective and were particularly helpful in obtaining high participation from employees with lower education and income.
Asfar et al. (2020) and Paul et al. (2013) suggested that incorporating safety managers and wellness coaches into tobacco control interventions (i.e., integrating tobacco control intervention into existing health and safety programs) encouraged the adoption and maintenance of smoking cessation. Asfar et al. (2020) attributed the success of safety managers to the workers having an established and trusting relationship, which was optimal for motivating individuals to quit using tobacco. Caponnetto et al. (2020) also identified the role of positive social relationships as a facilitator in that group treatment had a positive impact on peer influence and motivation to quit.
Another key facilitator suggested by Asfar et al. (2020), van den Brand et al. (2020), Mache et al. (2019), and Paul et al. (2013) was accessibility. These authors emphasized that offering interventions at the workplace during paid work hours enhanced the accessibility of the programs to participants/employees. By offering tobacco cessation programming during work hours, workplace leadership endorsed the tobacco control intervention which also facilitated the success of the program (Paul et al., 2013).
Asfar et al. (2020), Caponnetto et al. (2020), and Paul et al. (2013) also noted that collaboration with company leadership was a key facilitator to obtain leadership buy-in and later their endorsement of the program. Interestingly, Caponnetto et al. (2020) noted that although providing interventions during work time was seen as a facilitator, it was often still difficult to convince employees to attend training at the workplace, which the authors hypothesized could be due to unmeasured factors such as negative peer pressure or individual motivation.
Nieva et al. (2017) highlighted the impacts of mental health as a barrier to smoking cessation, emphasizing that depressive symptoms influenced abstinence and quit rates. Another significant barrier mentioned by Nieva et al. (2017) were the costs associated with continuing the intervention. Nieva et al. (2017) indicated that interventions could be costly for the workplace, and the ongoing expenses may impact whether an employer chose to continue the smoking cessation intervention.
Discussion
With the persistent and growing disparities in commercial tobacco use (Drope et al., 2018; Mitra et al., 2015), there is a need for health promotion practitioners to do things differently. While existing efforts at the individual and policy levels serve to reduce tobacco use overall, targeted approaches that focus on unique social-contextual factors that create inequitable barriers to quitting are required. A multilevel approach has the potential to shift the traditional focus on individual and interpersonal levels to a modern and holistic approach that addresses the social or contextual factors that influence health (S. D. Golden et al., 2015; T. L. Golden & Wendel, 2020). The results from this scoping review provided further support for a multilevel approach as an effective strategy to equitably increase tobacco abstinence, quit rates, and cessation adherence among employed individuals and improve cost-effectiveness in the workplace setting.
To promote knowledge to action, we have taken our synthesis of included studies further and integrated our results into a framework adapted from socio-ecological (Kalkhoran et al., 2018) or social-contextual frameworks (Sorensen et al., 2004) previously described in the workplace tobacco control literature (Figure 2). Incorporating results into existing frameworks enhanced practical application by providing evidence-based examples of multilevel interventions and multilevel barriers and facilitators that need to be addressed to equitably decrease tobacco use in the workplace.
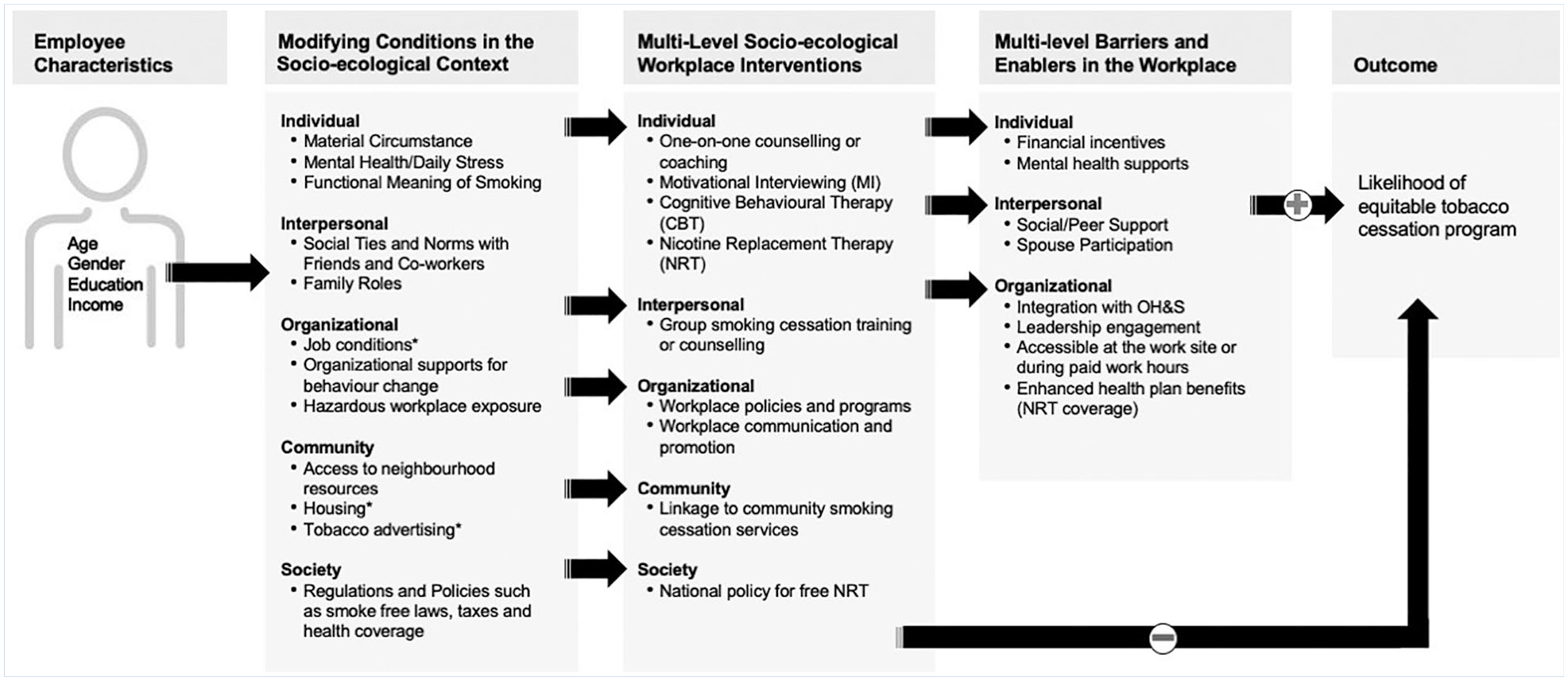
A socio-ecological framework for planning multilevel workplace tobacco control interventions.
Figure 2 demonstrates the complexity of interacting factors that influence workplace tobacco control intervention design, implementation, and uptake. Not all factors presented in Figure 2 need to be understood or incorporated into intervention design for every workplace. However, it is critical that practitioners take the time to unpack the complexity of conditions and factors shown to influence intervention effectiveness for different population groups and types of workplaces. This framework is meant to demonstrate that “one size does not fit all” for workplace tobacco control interventions aiming to reduce persistent and growing inequities.
Understanding employee characteristics is an important first step in multilevel intervention design within the workplace setting that addresses unique barriers of diverse groups of employees leading to increased participation. From our review of the literature, we know that there is variation in participation and effectiveness of smoking control intervention outcomes by age (Nieva et al., 2017), gender (Mache et al., 2019; Moses et al., 2020; Nieva et al., 2017), education, and income (van den Brand et al., 2018). To understand employee characteristics, workplace leaders can work with human resource departments to gather data or develop a targeted strategy to engage with employees who are currently using tobacco.
Next, by linking an understanding of the employee characteristics with factors in the workplace socio-ecological context, intervention planners can select and tailor interventions that will intervene on key modifying conditions (e.g., employee stress, social ties and norms, organizational supports, access to resources). To understand the workplace socio-ecological context, intervention planners need to meaningfully engage with both employees and leaders within the workplace. Planners can then identify and select the core components of the intervention across multiple socio-ecological levels that are best aligned with the unique workplace context.
Effective multilevel workplace interventions should aim to intervene across all socio-ecological levels (although most studies included in this review intervened across three levels). For example, a multilevel intervention may include the following core components: MI and NRT (individual), peer role modeling (interpersonal), employer-provided financial incentives (institutional), linkage to community tobacco cessation services (community), and adherence to or advocacy for policies supporting smoke-free indoor workplaces (policy). What is most important is that the selection of the core multilevel components is rooted upon the deep understanding of employee characteristics and workplace context to increase equitable uptake and effectiveness.
Intervention planners must be aware of potential barriers and facilitators in the workplace context. Examples of potential facilitators from our scoping review included financial incentives (Moses et al., 2020; van den Brand et al., 2018, 2020), integration with occupational health and safety (Asfar et al., 2020; Paul et al., 2013), leadership engagement (Asfar et al., 2020; Caponnetto et al., 2020; Paul et al., 2013), accessibility (Asfar et al., 2020; Caponnetto et al., 2020; Mache et al., 2019; Paul et al., 2013; van den Brand et al., 2020), and social/peer support (Caponnetto et al., 2020). Potential barriers included mental health (especially depressive symptoms) of employees (Nieva et al., 2017) and cost to the employer (influencing sustainability of the intervention) (Nieva et al., 2017). These facilitators and barriers served as areas of focus for creating an environment that is supportive of employee participation and smoking cessation.
This review also serves as a call for additional research and integration of SDOH such as job conditions (particularly those influencing poor mental health among employees) as they were not described in any of the included studies. Importantly, tobacco use is more prevalent among employees who do not feel they are using their skills and have more monotonous jobs conditions (Johansson et al., 1991), and there has been lower success in quitting smoking among employees with higher levels of occupational stress (Green & Johnson, 1990; Radi et al., 2007). As seen in our review, the majority of institutional-level interventions focused on covering the costs associated with program components (e.g., NRTs) or allowing interventions to occur during work hours. None of the reviewed articles incorporated alterations to work conditions that may cause stress or mental health concerns, thus hindering tobacco control efforts. This is an important area to consider for employers and occupational health practitioners when designing multilevel workplace tobacco control programs and may signal the need for tobacco control programs that incorporate multiple components (i.e., tobacco cessation and mental health).
Furthermore, there is a need to incorporate consideration of the workplace context itself. Findings from our review of barriers determined that employers are concerned about the cost of sustaining these tobacco control programs over time. Yet, few of the reviewed articles considered the influence of workplace factors on the success of the intervention under study despite a robust body of knowledge indicating the importance of such factors. Recent research has found that small workplaces often lack the resources (i.e., financial and human) and experience to implement health promotion programming, including those focused on tobacco control (Hannon et al., 2012; Jessiman-Perreault et al., 2020; Linnan et al., 2008; McCoy et al., 2014). Despite this known barrier, articles covered in this scoping review focused on individual financial incentives (Moses et al., 2020; van den Brand et al., 2018; van den Brand et al., 2020), often provided by the workplace, rather than incentives available to workplaces implementing workplace tobacco control programs. While there is evidence that employers can see a positive return on investment for multilevel tobacco cessation programs (Halpern et al., 2007; Javitz et al., 2004), further research is needed to investigate system-level incentives to support the implementation of tobacco-focused workplace interventions.
While this scoping review and proposed planning framework did not provide evidence for every potential intervention in the socio-ecological context, it did provide evidence-based examples of how to unpack the “black box” of how employee characteristics, socio-ecological contextual factors, and workplace barriers and facilitators impact workplace tobacco control intervention effectiveness (Nielsen & Randall, 2012).
This review was conducted following a systematic and established methodological process (i.e., PRISMA-ScR). Following this process was important for ensuring we conducted a transparent and reproducible scoping review. This scoping review began with prior research questions and well-defined inclusion criteria which lead to a high interrater agreement between our two independent reviewers during title and abstract review and full-text review. In addition to the knowledge of the authors, this scoping review was the first of its nature to examine and review the literature on multilevel workplace tobacco control interventions using a health equity lens.
Despite these strengths, there are some limitations that need to be considered when interpreting the results presented in this article. First, considering that the majority of the articles included in this review were obtained from peer-reviewed journals, this review could be subject to publication bias. In an effort to overcome this limitation, we included gray literature in our search, although none was included in the final scoping review. Scoping reviews are also at risk of bias if we were not able to identify all the available data on our topic, which results in the descriptive account of the information being incomplete. To overcome this, we hand-searched and identified systematic reviews (n = 3) to identify additional sources that may have been missed through the electronic search but found no additional articles for inclusion. Second, by applying a time frame limit to this search, (i.e., the last 10 years), older but potentially relevant studies have not been included in this review. While inclusion of literature prior to 2010 could have added value to this review, in light of recent societal calls for tobacco-free workplaces (e.g., the WHO recommended workplaces to implement measures to control tobacco exposure in 2005 [WHO, 2005] but by 2010 only 20% of ratified countries had implemented rules banning tobacco in indoor workplace [Uang et al., 2016]), an inclusion of only articles published after 2010 ensured that we reviewed the most up-to-date and relevant information.
Implications for Occupational Health Practice
This review described evidence-based multilevel core components for tobacco control in the workplace. It also contextualized these potential interventions in a socio-ecological framework that facilitates consideration of what works, for whom, and under what circumstances. Consideration of the ecological influences on employee health and wellbeing should be a part of everyday occupational health and safety practice. The environments that are closest to the employee often have the strongest influence (i.e., peer relationships and the immediate work environment that the employee interacts with on a daily basis), but consideration should always be made to the influences on employee health from outside of the workplace itself. This supports the call for comprehensive and integrated programs that look holistically at employee health and the multiple influences (i.e., the intersection between tobacco use and employee physical and psychological health and safety).
Planning comprehensive and integrated interventions in the workplace setting requires consideration of variability and complexity. Building upon models in Implementation and Dissemination Science (Koh et al., 2018), we suggest the following steps could be followed to promote equity in intervention participation and effectiveness: (a) engage with workplace leaders and workplace health committee representatives to understand the workplace socio-ecological context; (b) work together with human resources, benefit providers, and/or employee assistance programs (EAP) to gain access to data that describe key employee characteristics such as age, gender, income, and education to inform engagement and tailoring of interventions; (c) collaboratively select evidence-based multilevel intervention components dependent on outcomes from Steps (a) and (b) (i.e., NRT, group counseling, workplace-led communication and promotion, and collaboration with community services); (d) work collaboratively to adapt core intervention components to the workplace and employee context to improve health equity of outcomes (i.e., adaptations for shift workers or low-income earners); and (e) be mindful of workplace-specific barriers and facilitators (i.e., time, cost, collaboration between occupational health and safety, and leadership) and work collaboratively to enhance facilitators and overcome barriers.
In Summary
The workplace provides a unique opportunity to intervene on modifiable risk factors such as tobacco use, but workplaces do not exist in a vacuum and multilevel interventions are needed to engage individuals in settings where they live, work, and play to improve rates of smoking cessation.
Multilevel interventions are essential in designing health equity–informed interventions as they recognize how social determinants of health accumulate across settings of the population to impact individual health behaviors, thus creating condition of health inequities.
Implementation of multilevel intervention that targets at least two levels of the social ecological model has the potential to disperse the positive impacts of smoking cessation beyond just the individual (e.g., spousal effects, second-hand smoking exposure reduction).
Future research and health promotion initiatives should investigate the impact of workplace factors (e.g., size, job conditions, and industry) to design interventions that account for these factors that may impact the success of an intervention.
Supplemental Material
sj-docx-1-whs-10.1177_21650799221081265 – Supplemental material for Exploring Multilevel Workplace Tobacco Control Interventions: A Scoping Review
Supplemental material, sj-docx-1-whs-10.1177_21650799221081265 for Exploring Multilevel Workplace Tobacco Control Interventions: A Scoping Review by Reilly Parkinson, Geneviève Jessiman-Perreault, Nicole Frenette and Lisa K. Allen Scott in Workplace Health & Safety
Footnotes
Acknowledgements
We would like to express our gratitude to Marcus Vaska from the Knowledge Resource Service at Alberta Health Services for his valuable contribution to the development and implementation of the search strategy for this scoping review.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding provided, in whole or in part by Alberta Health. Strategic direction and applied research support provided by the Alberta Health Services (AHS), Cancer Prevention and Screening Innovation (CPSI) team. Provision of funding by Alberta Health does not signify that this project represents the policies or views of Alberta Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.